Perspectives and Challenges in Robotic Neurorehabilitation

 ,
,  ,
, 
 and
and
Abstract
:1. Introduction
2. An Overview of Robotic Devices for Neurorehabilitation
2.1. Robotic Neurorehabilitation for the Upper Limb
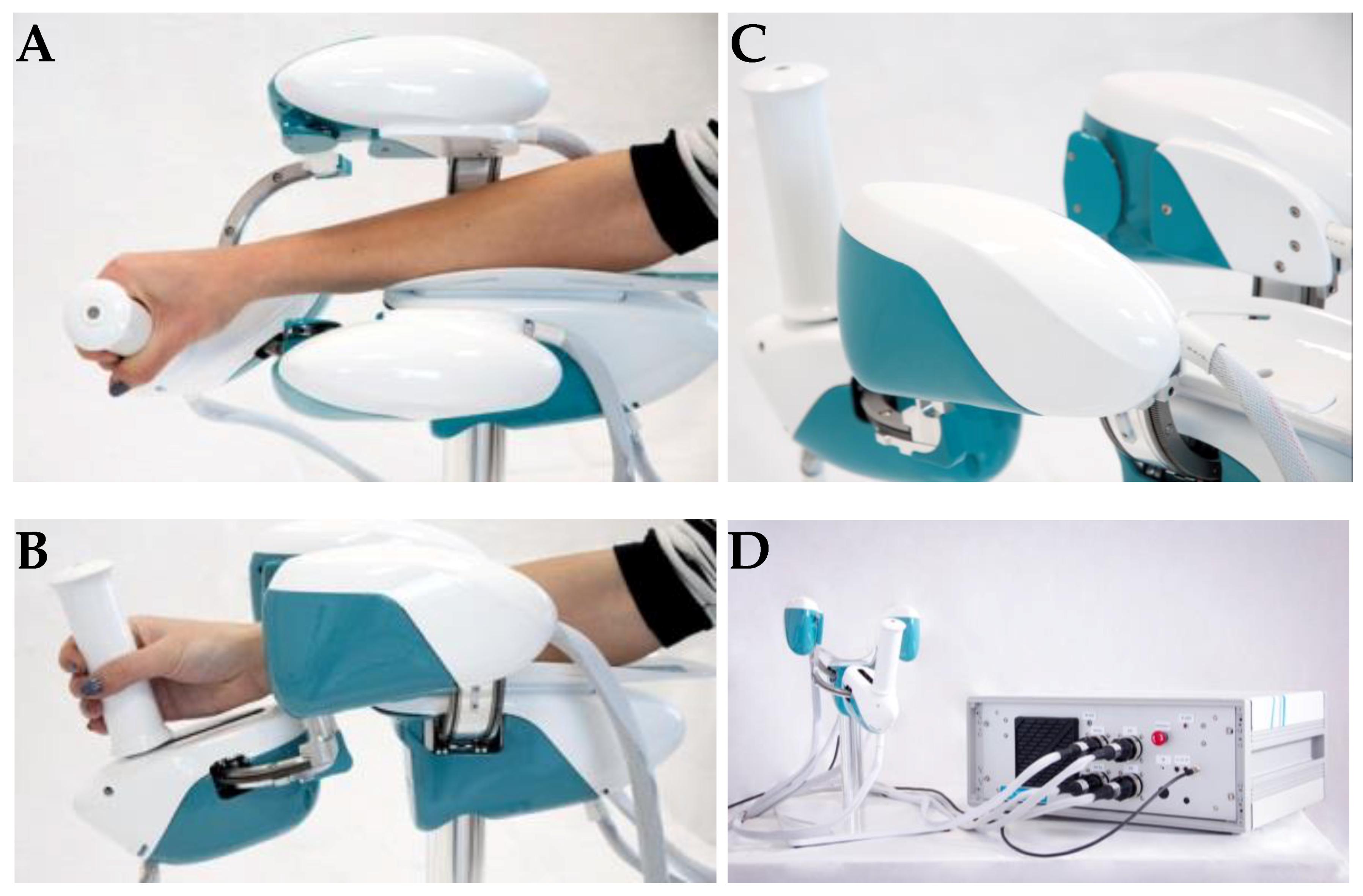
End-Effector Device for Wrist Rehabilitation: WristBot
2.2. Robotic Neurorehabilitation for the Lower Limb
Modular Exoskeleton for Gait Assistance: Twin
3. Current Trends of Robot-Aided Neurorehabilitation
3.1. Rehabilitative Training
3.1.1. Advances in Motor Control for Robotic Neurorehabilitation
3.1.2. Robotic Neurorehabilitation Coupled to Brain Computer Interfaces
3.2. Multimodal Assessment of Recovery
3.2.1. Clinical Scales
3.2.2. Quantitative Assessment of the Sensorimotor Performance
3.2.3. Neural and Muscular Correlates of the Sensorimotor Performance
4. Further Considerations and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hatem, S.M.; Saussez, G.; della Faille, M.; Prist, V.; Zhang, X.; Dispa, D.; Bleyenheuft, Y. Rehabilitation of motor function after stroke: A multiple systematic review focused on techniques to stimulate upper extremity recovery. Front. Hum. Neurosci. 2016, 10, 442. [Google Scholar] [CrossRef] [PubMed]
- Broeks, J.G.; Lankhorst, G.J.; Rumping, K.; Prevo, A.J.H. The long-term outcome of arm function after stroke: Results of a follow-up study. Disabil. Rehabil. 1999, 21, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Coderre, A.M.; Zeid, A.A.; Dukelow, S.P.; Demmer, M.J.; Moore, K.D.; Demers, M.J.; Bretzke, H.; Herter, T.M.; Glasgow, J.I.; Norman, K.E. Assessment of upper-limb sensorimotor function of subacute stroke patients using visually guided reaching. Neurorehabil. Neural Repair 2010, 24, 528–541. [Google Scholar] [CrossRef] [PubMed]
- Winward, C.E.; Halligan, P.W.; Wade, D.T. Current practice and clinical relevance of somatosensory assessment after stroke. Clin. Rehabil. 1999, 13, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Lang, C.E.; Bland, M.D.; Bailey, R.R.; Schaefer, S.Y.; Birkenmeier, R.L. Assessment of upper extremity impairment, function, and activity after stroke: Foundations for clinical decision making. J. Hand Ther. 2013, 26, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Lang, C.E.; Beebe, J.A. Relating movement control at 9 upper extremity segments to loss of hand function in people with chronic hemiparesis. Neurorehabil. Neural Repair 2007, 21, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Meng, W.; Liu, Q.; Zhou, Z.; Ai, Q.; Sheng, B.; Xie, S. Recent development of mechanisms and control strategies for robot-assisted lower limb rehabilitation. Mechatronics 2015, 31, 132–145. [Google Scholar] [CrossRef]
- Zhang, X.; Yue, Z.; Wang, J. Robotics in Lower-Limb Rehabilitation after Stroke. Behav. Neurol. 2017, 2017, 13. [Google Scholar] [CrossRef] [PubMed]
- Wolbrecht, E.T.; Chan, V.; Le, V.; Cramer, S.C.; Reinkensmeyer, D.J.; Bobrow, J.E. Real-time computer modeling of weakness following stroke optimizes robotic assistance for movement therapy. In Proceedings of the 2007 3rd International IEEE/EMBS Conference on Neural Engineering, Kohala Coast, HI, USA, 2–5 May 2007; pp. 152–158. [Google Scholar]
- Casadio, M.; Sanguineti, V. Learning, retention, and slacking: A model of the dynamics of recovery in robot therapy. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 20, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Lambercy, O.; Dovat, L.; Gassert, R.; Burdet, E.; Teo, C.L.; Milner, T. A haptic knob for rehabilitation of hand function. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Stienen, A.H.A.; Hekman, E.E.G.; Van der Helm, F.C.T.; Prange, G.B.; Jannink, M.J.A.; Aalsma, A.M.M.; Van der Kooij, H. Dampace: Dynamic force-coordination trainer for the upper extremities. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007. [Google Scholar]
- Johnson, M.J.; Van der Loos, H.F.M.; Burgar, C.G.; Shor, P.; Leifer, L.J. Design and evaluation of Driver’s SEAT: A car steering simulation environment for upper limb stroke therapy. Robotica 2003, 21, 13–23. [Google Scholar] [CrossRef]
- Proietti, T.; Crocher, V.; Roby-Brami, A.; Jarrasse, N. Upper-Limb Robotic Exoskeletons for Neurorehabilitation: A Review on Control Strategies. IEEE Rev. Biomed. Eng. 2016, 9, 4–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guidali, M.; Duschau-Wicke, A.; Broggi, S.; Klamroth-Marganska, V.; Nef, T.; Riener, R. A robotic system to train activities of daily living in a virtual environment. Med. Biol. Eng. Comput. 2011, 49, 1213–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdollahi, F.; Lazarro, E.D.C.; Listenberger, M.; Kenyon, R.V.; Kovic, M.; Bogey, R.A.; Hedeker, D.; Jovanovic, B.D.; Patton, J.L. Error Augmentation Enhancing Arm Recovery in Individuals With Chronic Stroke: A Randomized Crossover Design. Neurorehabil. Neural Repair 2014, 28, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Patton, J.L.; Stoykov, M.E.; Kovic, M.; Mussa-Ivaldi, F.A. Evaluation of robotic training forces that either enhance or reduce error in chronic hemiparetic stroke survivors. Exp. Brain Res. 2006, 168, 368–383. [Google Scholar] [CrossRef] [PubMed]
- Marchal-Crespo, L.; Reinkensmeyer, D.J. Review of control strategies for robotic movement training after neurologic injury. J. NeuroEng. Rehabil. 2009, 6, 20. [Google Scholar] [CrossRef]
- Posteraro, F.; Mazzoleni, S.; Aliboni, S.; Cesqui, B.; Battaglia, A.; Dario, P.; Micera, S. Robot-mediated therapy for paretic upper limb of chronic patients following neurological injury. J. Rehabil. Med. 2009, 41, 976–980. [Google Scholar] [CrossRef] [Green Version]
- Squeri, V.; Masia, L.; Giannoni, P.; Sandini, G.; Morasso, P. Wrist rehabilitation in chronic stroke patients by means of adaptive, progressive robot-aided therapy. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 22, 312–325. [Google Scholar] [CrossRef]
- Lum, P.S.; Burgar, C.G.; Shor, P.C.; Majmundar, M.; Van der Loos, M. Robot-assisted movement training compared with conventional therapy techniques for the rehabilitation of upper-limb motor function after stroke. Arch. Phys. Med. Rehabil. 2002, 83, 952–959. [Google Scholar] [CrossRef] [Green Version]
- Riener, R.; Nef, T.; Colombo, G. Robot-aided neurorehabilitation of the upper extremities. Med. Biol. Eng. Comput. 2005, 43, 2–10. [Google Scholar] [CrossRef] [Green Version]
- Shadmehr, R.; Mussa-Ivaldi, F.A. Adaptive representation of dynamics during learning of a motor task. J. Neurosci. 1994, 14, 3208–3224. [Google Scholar] [CrossRef] [PubMed]
- Klamroth-Marganska, V.; Blanco, J.; Campen, K.; Curt, A.; Dietz, V.; Ettlin, T.; Felder, M.; Fellinghauer, B.; Guidali, M.; Kollmar, A.; et al. Three-dimensional, task-specific robot therapy of the arm after stroke: A multicentre, parallel-group randomised trial. Lancet Neurol. 2014, 13, 159–166. [Google Scholar] [CrossRef]
- Gassert, R.; Dietz, V. Rehabilitation robots for the treatment of sensorimotor deficits: A neurophysiological perspective. J. NeuroEng. Rehabil. 2018, 15, 46. [Google Scholar] [CrossRef] [PubMed]
- Krebs, H.I.; Ferraro, M.; Buerger, S.P.; Newbery, M.J.; Makiyama, A.; Sandmann, M.; Lynch, D.; Volpe, B.T.; Hogan, N. Rehabilitation robotics: Pilot trial of a spatial extension for MIT-Manus. J. NeuroEng. Rehabil. 2004, 1, 5. [Google Scholar] [CrossRef] [PubMed]
- Reinkensmeyer, D.J.; Kahn, L.E.; Averbuch, M.; McKenna-Cole, A.; Schmit, B.D.; Rymer, W.Z. Understanding and treating arm movement impairment after chronic brain injury: Progress with the ARM guide. J. Rehabil. Res. Dev. 2000, 37, 653–662. [Google Scholar] [PubMed]
- Coote, S.; Murphy, B.; Harwin, W.; Stokes, E. The effect of the GENTLE/s robot-mediated therapy system on arm function after stroke. Clin. Rehabil. 2008, 22, 395–405. [Google Scholar] [CrossRef] [Green Version]
- Rosati, G.; Gallina, P.; Masiero, S. Design, implementation and clinical tests of a wire-based robot for neurorehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 560–569. [Google Scholar] [CrossRef] [PubMed]
- Ellis, M.D.; Sukal-Moulton, T.M.; Dewald, J.P. Impairment-based 3-D robotic intervention improves upper extremity work area in chronic stroke: Targeting abnormal joint torque coupling with progressive shoulder abduction loading. IEEE Trans. Robot. 2009, 25, 549–555. [Google Scholar] [CrossRef]
- Lum, P.S.; Burgar, C.G.; Van der Loos, M.; Shor, P.C. MIME robotic device for upper-limb neurorehabilitation in subacute stroke subjects: A follow-up study. J. Rehabil. Res. Dev. 2006, 43, 631. [Google Scholar] [CrossRef]
- Hesse, S.; Schulte-Tigges, G.; Konrad, M.; Bardeleben, A.; Werner, C. Robot-assisted arm trainer for the passive and active practice of bilateral forearm and wrist movements in hemiparetic subjects. Arch. Phys. Med. Rehabil. 2003, 84, 915–920. [Google Scholar] [CrossRef]
- Hogan, N.; Krebs, H.I.; Charnnarong, J.; Srikrishna, P.; Sharon, A. MIT-MANUS: A workstation for manual therapy and training. I. In Proceedings of the IEEE International Workshop on Robot and Human Communication, Okyo, Japan, 12 June 1992; pp. 161–165. [Google Scholar]
- Frascarelli, F.; Masia, L.; Di Rosa, G.; Cappa, P.; Petrarca, M.; Castelli, E.; Krebs, H. The impact of robotic rehabilitation in children with acquired or congenital movement disorders. Eur. J. Phys. Rehabil. Med. 2009, 45, 135–141. [Google Scholar] [PubMed]
- Fasoli, S.E.; Fragala-Pinkham, M.; Hughes, R.; Hogan, N.; Stein, J.; Krebs, H.I. Upper limb robot-assisted therapy: A new option for children with hemiplegia. Technol. Disabil. 2010, 22, 193–198. [Google Scholar] [CrossRef]
- Hidler, J.; Nichols, D.; Pelliccio, M.; Brady, K. Advances in the understanding and treatment of stroke impairment using robotic devices. Top. Stroke Rehabil. 2005, 12, 22–35. [Google Scholar] [CrossRef] [PubMed]
- Kahn, L.E.; Zygman, M.L.; Rymer, W.Z.; Reinkensmeyer, D.J. Robot-assisted reaching exercise promotes arm movement recovery in chronic hemiparetic stroke: A randomized controlled pilot study. J. NeuroEng. Rehabil. 2006, 3, 12. [Google Scholar] [CrossRef] [PubMed]
- Amirabdollahian, F.; Loureiro, R.; Gradwell, E.; Collin, C.; Harwin, W.; Johnson, G. Multivariate analysis of the Fugl-Meyer outcome measures assessing the effectiveness of GENTLE/S robot-mediated stroke therapy. J. NeuroEng. Rehabil. 2007, 4, 4. [Google Scholar] [CrossRef]
- van der Linde, R.Q.; Lammertse, P. HapticMaster–a generic force controlled robot for human interaction. Ind. Robot. Int. J. 2003, 30, 515–524. [Google Scholar] [CrossRef]
- Masiero, S.; Poli, P.; Armani, M.; Ferlini, G.; Rizzello, R.; Rosati, G. Robotic upper limb rehabilitation after acute stroke by NeReBot: Evaluation of treatment costs. BioMed Res. Int. 2014, 2014, 5. [Google Scholar]
- Sukal, T.M.; Ellis, M.D.; Dewald, J.P. Shoulder abduction-induced reductions in reaching work area following hemiparetic stroke: Neuroscientific implications. Exp. Brain Res. 2007, 183, 215–223. [Google Scholar] [CrossRef]
- Lum, P.S.; Burgar, C.G.; Shor, P.C. Evidence for improved muscle activation patterns after retraining of reaching movements with the MIME robotic system in subjects with post-stroke hemiparesis. IEEE Trans. Neural Syst. Rehabil. Eng. 2004, 12, 186–194. [Google Scholar] [CrossRef]
- Casadio, M.; Sanguineti, V.; Morasso, P.G.; Arrichiello, V. Braccio di Ferro: A new haptic workstation for neuromotor rehabilitation. Technol. Health Care 2006, 14, 123–142. [Google Scholar]
- Squeri, V.; Vergaro, E.; Brichetto, G.; Casadio, M.; Morasso, P.G.; Solaro, C.; Sanguineti, V. Adaptive robot training in the rehabilitation of incoordination in Multiple Sclerosis: A pilot study. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; pp. 364–370. [Google Scholar]
- De Santis, D.; Zenzeri, J.; Casadio, M.; Masia, L.; Riva, A.; Morasso, P.; Squeri, V. Robot-assisted training of the kinesthetic sense: Enhancing proprioception after stroke. Front. Hum. Neurosci. 2015, 8, 1037. [Google Scholar] [CrossRef] [PubMed]
- Masia, L.; Casadio, M.; Giannoni, P.; Sandini, G.; Morasso, P. Performance adaptive training control strategy for recovering wrist movements in stroke patients: A preliminary, feasibility study. J. NeuroEng. Rehabil. 2009, 6, 44. [Google Scholar] [CrossRef] [PubMed]
- Marini, F.; Hughes, C.M.L.; Squeri, V.; Doglio, L.; Moretti, P.; Morasso, P.; Masia, L. Robotic wrist training after stroke: Adaptive modulation of assistance in pediatric rehabilitation. Robot. Auton. Syst. 2017, 91, 169–178. [Google Scholar] [CrossRef]
- Marini, F.; Cappello, L.; Squeri, V.; Morasso, P.; Moretti, P.; Riva, A.; Doglio, L.; Masia, L. Online Modulation of Assistance in Robot Aided Wrist Rehabilitation A Pilot Study on a Subject Affected by Dystonia. In Proceedings of the 2014 IEEE Haptics Symposium (HAPTICS), Houston, TX, USA, 23–26 February 2014; pp. 153–158. [Google Scholar]
- Gopura, R.A.R.C.; Kiguchi, K.; Li, Y. SUEFUL-7: A 7DOF upper-limb exoskeleton robot with muscle-model-oriented EMG-based control. In Proceedings of the 2009 IEEE/RSJ International Conference on Intelligent Robots and Systems, St. Louis, MO, USA, 10–15 October 2009; pp. 1126–1131. [Google Scholar]
- Nef, T.; Guidali, M.; Riener, R. ARMin III–arm therapy exoskeleton with an ergonomic shoulder actuation. Appl. Bionics Biomech. 2009, 6, 127–142. [Google Scholar] [CrossRef]
- Perry, J.C.; Rosen, J.; Burns, S. Upper-limb powered exoskeleton design. IEEE/ASME Trans. Mechatron. 2007, 12, 408–417. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Wei, R.; Perez, M.; Shepard, B.; Koeneman, E.; Koeneman, J.; He, J. RUPERT: An exoskeleton robot for assisting rehabilitation of arm functions. In Proceedings of the 2008 Virtual Rehabilitation, Vancouver, BC, Canada, 25–27 August 2008; pp. 163–167. [Google Scholar]
- Rehmat, N.; Zuo, J.; Meng, W.; Liu, Q.; Xie, S.Q.; Liang, H. Upper limb rehabilitation using robotic exoskeleton systems: A systematic review. Int. J. Intell. Robot. Appl. 2018, 2, 283–295. [Google Scholar] [CrossRef]
- Frisoli, A.; Rocchi, F.; Marcheschi, S.; Dettori, A.; Salsedo, F.; Bergamasco, M. A new force-feedback arm exoskeleton for haptic interaction in virtual environments. In Proceedings of the 1st Joint Eurohaptics Conference and Symposium on Haptic Interfaces for Virtual Environment and Teleoperator Systems World Haptics Conference, Pisa, Italy, 18–20 March 2005; pp. 195–201. [Google Scholar]
- Reinkensmeyer, D.J.; Wolbrecht, E.T.; Chan, V.; Chou, C.; Cramer, S.C.; Bobrow, J.E. Comparison of 3D, assist-as-needed robotic arm/hand movement training provided with Pneu-WREX to conventional table top therapy following chronic stroke. Am. J. Phys. Med. Rehabil. Assoc. Acad. Physiatr. 2012, 91, S232. [Google Scholar] [CrossRef]
- Ren, Y.; Park, H.-S.; Zhang, L.-Q. Developing a whole-arm exoskeleton robot with hand opening and closing mechanism for upper limb stroke rehabilitation. In Proceedings of the 2009 IEEE International Conference on Rehabilitation Robotics, Kyoto, Japan, 23–26 June 2009; pp. 761–765. [Google Scholar]
- Nef, T.; Mihelj, M.; Kiefer, G.; Perndl, C.; Muller, R.; Riener, R. ARMin-Exoskeleton for arm therapy in stroke patients. In Proceedings of the 2007 IEEE 10th international conference on rehabilitation robotics, Noordwijk, The Netherlands, 13–15 June 2007; pp. 68–74. [Google Scholar]
- Nef, T.; Mihelj, M.; Riener, R. ARMin: A robot for patient-cooperative arm therapy. Med. Biol. Eng. Comput. 2007, 45, 887–900. [Google Scholar] [CrossRef]
- Huang, J.; Tu, X.; He, J. Design and evaluation of the RUPERT wearable upper extremity exoskeleton robot for clinical and in-home therapies. IEEE Trans. Syst. Man Cybern. Syst. 2015, 46, 926–935. [Google Scholar] [CrossRef]
- Frisoli, A.; Chisari, C.; Sotgiu, E.; Procopio, C.; Fontana, M.; Rossi, B.; Bergamasco, M. Rehabilitation training and evaluation with the L-EXOS in chronic stroke. In Proceedings of the International Conference on Smart Homes and Health Telematics, Singapore, 10–12 July 2018; pp. 242–245. [Google Scholar]
- Byl, N.N.; Abrams, G.M.; Pitsch, E.; Fedulow, I.; Kim, H.; Simkins, M.; Nagarajan, S.; Rosen, J. Chronic stroke survivors achieve comparable outcomes following virtual task specific repetitive training guided by a wearable robotic orthosis (UL-EXO7) and actual task specific repetitive training guided by a physical therapist. J. Hand Ther. 2013, 26, 343–352. [Google Scholar] [CrossRef]
- Kim, H.; Miller, L.M.; Fedulow, I.; Simkins, M.; Abrams, G.M.; Byl, N.; Rosen, J. Kinematic data analysis for post-stroke patients following bilateral versus unilateral rehabilitation with an upper limb wearable robotic system. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 21, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Wolbrecht, E.T.; Leavitt, J.; Reinkensmeyer, D.J.; Bobrow, J.E. Control of a pneumatic orthosis for upper extremity stroke rehabilitation. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 2687–2693. [Google Scholar]
- Park, H.-S.; Ren, Y.; Zhang, L.-Q. IntelliArm: An exoskeleton for diagnosis and treatment of patients with neurological impairments. In Proceedings of the 2008 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, Scottsdale, AZ, USA, 19–22 October 2008; pp. 109–114. [Google Scholar]
- Milot, M.-H.; Spencer, S.J.; Chan, V.; Allington, J.P.; Klein, J.; Chou, C.; Bobrow, J.E.; Cramer, S.C.; Reinkensmeyer, D.J. A crossover pilot study evaluating the functional outcomes of two different types of robotic movement training in chronic stroke survivors using the arm exoskeleton BONES. J. NeuroEng. Rehabil. 2013, 10, 112. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, R.C.; Harwin, W.S. Reach & grasp therapy: Design and control of a 9-DOF robotic neuro-rehabilitation system. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; pp. 757–763. [Google Scholar]
- Fazekas, G.; Horvath, M.; Troznai, T.; Toth, A. Robot-mediated upper limb physiotherapy for patients with spastic hemiparesis: A preliminary study. J. Rehabil. Med. 2007, 39, 580–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Housman, S.J.; Le, V.; Rahman, T.; Sanchez, R.J.; Reinkensmeyer, D.J. Arm-training with T-WREX after chronic stroke: Preliminary results of a randomized controlled trial. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; pp. 562–568. [Google Scholar]
- Colomer, C.; Baldovi, A.; Torromé, S.; Navarro, M.; Moliner, B.; Ferri, J.; Noé, E. Efficacy of Armeo® Spring during the chronic phase of stroke. Study in mild to moderate cases of hemiparesis. Neurologia 2013, 28, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Jarrasse, N.; Proietti, T.; Crocher, V.; Robertson, J.; Sahbani, A.; Morel, G.; Roby-Brami, A. Robotic exoskeletons: A perspective for the rehabilitation of arm coordination in stroke patients. Front. Hum. Neurosci 2014, 8, 947. [Google Scholar] [CrossRef] [PubMed]
- Maclean, N.; Pound, P.; Wolfe, C.; Rudd, A. Qualitative analysis of stroke patients’ motivation for rehabilitation. BMJ 2000, 321, 1051–1054. [Google Scholar] [CrossRef]
- Fazekas, G.; Tavaszi, I. The future role of robots in neuro-rehabilitation. Expert Rev. Neurother. 2019, 19, 471–473. [Google Scholar] [CrossRef]
- Morales, R.; Badesa, F.J.; Garcia-Aracil, N.; Sabater, J.M.; Perez-Vidal, C. Pneumatic robotic systems for upper limb rehabilitation. Med. Biol. Eng. Comput. 2011, 49, 1145–1156. [Google Scholar] [CrossRef]
- Song, Z.B.; Guo, S.X.; Pang, M.Y.; Zhang, S.Y.; Xiao, N.; Gao, B.F.; Shi, L.W. Implementation of Resistance Training Using an Upper-Limb Exoskeleton Rehabilitation Device for Elbow Joint. J. Med. Biol. Eng. 2014, 34, 188–196. [Google Scholar] [CrossRef]
- Hogan, N. Impedance Control—An Approach to Manipulation 1. Theory. J. Dyn. Syst. Meas. Control 1985, 107, 1–7. [Google Scholar] [CrossRef]
- Rahman, M.H.; Saad, M.; Kenne, J.P.; Archambault, P.S. Control of an Exoskeleton Robot Arm with Sliding Mode Exponential Reaching Law. Int. J. Control Autom. 2013, 11, 92–104. [Google Scholar] [CrossRef]
- Kiguchi, K.; Quan, Q. Muscle-Model-Oriented EMG-Based Control of an Upper-Limb Power-Assist Exoskeleton with a Neuro-Fuzzy Modifier. In Proceedings of the 2008 IEEE International Conference on Fuzzy Systems, Hong Kong, China, 1–6 June 2008; pp. 1181–1186. [Google Scholar]
- Buchanan, T.S.; Lloyd, D.G.; Manal, K.; Besier, T.F. Neuromusculoskeletal modeling: Estimation of muscle forces and joint moments and movements from measurements of neural command. J. Appl. Biomech. 2004, 20, 367–395. [Google Scholar] [CrossRef] [PubMed]
- Blank, A.; O’Malley, M.K.; Francisco, G.E.; Contreras-Vidal, J.L. A Pre-Clinical Framework for Neural Control of a Therapeutic Upper-Limb Exoskeleton. In Proceedings of the 2013 6th International IEEE/EMBS Conference on Neural Engineering (NER), San Diego, CA, USA, 6–8 November 2013; pp. 1159–1162. [Google Scholar]
- Lauretti, C.; Cordella, F.; Ciancio, A.L.; Trigili, E.; Catalan, J.M.; Badesa, F.J.; Crea, S.; Pagliara, S.M.; Sterzi, S.; Vitiello, N. Learning by demonstration for motion planning of upper-limb exoskeletons. Front. Neurorobot. 2018, 12, 5. [Google Scholar] [CrossRef] [PubMed]
- Guidali, M.; Schmiedeskamp, M.; Klamroth, V.; Riener, R. Assessment and training of synergies with an arm rehabilitation robot. In Proceedings of the 2009 IEEE 11th International Conference on Rehabilitation Robotics, Kyoto, Japan, 23–26 June 2009; pp. 899–903. [Google Scholar]
- Masia, L.; Casadio, M.; Sandini, G.; Morasso, P. Eye-hand coordination during dynamic visuomotor rotations. PLoS ONE 2009, 4, e7004. [Google Scholar] [CrossRef] [PubMed]
- Semprini, M.; Laffranchi, M.; Sanguineti, V.; Avanzino, L.; De Icco, R.; De Michieli, L.; Chiappalone, M. Technological approaches for neurorehabilitation: From robotic devices to brain stimulation and beyond. Front. Neurol. 2018, 9, 212. [Google Scholar] [CrossRef] [PubMed]
- Hesse, S.; Uhlenbrock, D. A mechanized gait trainer for restoration of gait. J. Rehabil. Res. Dev. 2000, 37, 701–708. [Google Scholar]
- Schmidt, H.; Hesse, S.; Bernhardt, R.; Krüger, J. HapticWalker—A novel haptic foot device. ACM Trans. Appl. Percept. 2005, 2, 166–180. [Google Scholar] [CrossRef]
- Hesse, S.; Waldner, A.; Tomelleri, C. Innovative gait robot for the repetitive practice of floor walking and stair climbing up and down in stroke patients. J. NeuroEng. Rehabil. 2010, 7, 30. [Google Scholar] [CrossRef]
- Schmidt, H.; Werner, C.; Bernhardt, R.; Hesse, S.; Krüger, J. Gait rehabilitation machines based on programmable footplates. J. NeuroEng. Rehabil. 2007, 4, 2. [Google Scholar] [CrossRef]
- Squeri, V.; De Luca, A.; Cella, A.; Vallone, F.; Siri, G.; Zigoura, E.; Giorgeschi, A.; Tavella, E.; Puntoni, M.; Avella, M. Robotic evaluation of fall risk in older people: Results on trunk parameters in static and dynamic balance conditions by hunova robot. Ann. Phys. Rehabil. Med. 2018, 61, e339. [Google Scholar] [CrossRef]
- Girone, M.; Burdea, G.; Bouzit, M.; Popescu, V.; Deutsch, J.E. A Stewart platform-based system for ankle telerehabilitation. Auton. Robot. 2001, 10, 203–212. [Google Scholar] [CrossRef]
- Zhang, M.; Davies, T.C.; Xie, S. Effectiveness of robot-assisted therapy on ankle rehabilitation–a systematic review. J. NeuroEng. Rehabil. 2013, 10, 30. [Google Scholar] [CrossRef]
- Saglia, J.A.; Tsagarakis, N.G.; Dai, J.S.; Caldwell, D.G. A high-performance redundantly actuated parallel mechanism for ankle rehabilitation. Int. J. Robot. Res. 2009, 28, 1216–1227. [Google Scholar] [CrossRef]
- Saglia, J.A.; De Luca, A.; Squeri, V.; Ciaccia, L.; Sanfilippo, C.; Ungaro, S.; De Michieli, L. Design, Development and Clinical Results of a Novel Total-Body Rehabilitation Robot: Hunova®. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; pp. 417–422. [Google Scholar]
- Werner, C.; Von Frankenberg, S.; Treig, T.; Konrad, M.; Hesse, S. Treadmill training with partial body weight support and an electromechanical gait trainer for restoration of gait in subacute stroke patients: A randomized crossover study. Stroke 2002, 33, 2895–2901. [Google Scholar] [CrossRef]
- Mehrholz, J.; Pohl, M. Electromechanical-assisted gait training after stroke: A systematic review comparing end-effector and exoskeleton devices. J. Rehabil. Med. 2012, 44, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Gandolfi, M.; Geroin, C.; Picelli, A.; Munari, D.; Waldner, A.; Tamburin, S.; Marchioretto, F.; Smania, N. Robot-assisted vs. sensory integration training in treating gait and balance dysfunctions in patients with multiple sclerosis: A randomized controlled trial. Front. Hum. Neurosci. 2014, 8, 318. [Google Scholar] [CrossRef]
- Picelli, A.; Melotti, C.; Origano, F.; Waldner, A.; Fiaschi, A.; Santilli, V.; Smania, N. Robot-assisted gait training in patients with Parkinson disease: A randomized controlled trial. Neurorehabil. Neural Repair 2012, 26, 353–361. [Google Scholar] [CrossRef]
- Smania, N.; Bonetti, P.; Gandolfi, M.; Cosentino, A.; Waldner, A.; Hesse, S.; Werner, C.; Bisoffi, G.; Geroin, C.; Munari, D. Improved gait after repetitive locomotor training in children with cerebral palsy. Am. J. Phys. Med. Rehabil 2011, 90, 137–149. [Google Scholar] [CrossRef]
- Taglione, E.; Catitti, P.; D’Angelo, M.; Squeri, V.; Saglia, J.; Sanfilippo, C.; De Michieli, L. Proprioceptive and motor training using the high performance robotic device hunova: Protocol of a randomized, controlled trial in patients with lower limb post-traumatic conditions. Ann. Phys. Rehabil. Med. 2018, 61, e497–e498. [Google Scholar] [CrossRef]
- Jezernik, S.; Colombo, G.; Keller, T.; Frueh, H.; Morari, M. Robotic orthosis lokomat: A rehabilitation and research tool. Neuromodul. Technol. Neural Interface 2003, 6, 108–115. [Google Scholar] [CrossRef]
- Freivogel, S.; Mehrholz, J.; Husak-Sotomayor, T.; Schmalohr, D. Gait training with the newly developed ‘LokoHelp’-system is feasible for non-ambulatory patients after stroke, spinal cord and brain injury. A feasibility study. Brain Inj. 2008, 22, 625–632. [Google Scholar] [CrossRef]
- Veneman, J.F.; Kruidhof, R.; Hekman, E.E.; Ekkelenkamp, R.; Van Asseldonk, E.H.; Van Der Kooij, H. Design and evaluation of the LOPES exoskeleton robot for interactive gait rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 379–386. [Google Scholar] [CrossRef]
- Banala, S.K.; Agrawal, S.K.; Scholz, J.P. Active Leg Exoskeleton (ALEX) for Gait Rehabilitation of Motor-Impaired Patients. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; pp. 401–407. [Google Scholar]
- Kolakowsky-Hayner, S.A.; Crew, J.; Moran, S.; Shah, A. Safety and feasibility of using the EksoTM bionic exoskeleton to aid ambulation after spinal cord injury. J. Spine 2013, 4. [Google Scholar] [CrossRef]
- Zeilig, G.; Weingarden, H.; Zwecker, M.; Dudkiewicz, I.; Bloch, A.; Esquenazi, A. Safety and tolerance of the ReWalk™ exoskeleton suit for ambulation by people with complete spinal cord injury: A pilot study. J. Spinal Cord Med. 2012, 35, 96–101. [Google Scholar] [CrossRef]
- Farris, R.J.; Quintero, H.A.; Murray, S.A.; Ha, K.H.; Hartigan, C.; Goldfarb, M. A preliminary assessment of legged mobility provided by a lower limb exoskeleton for persons with paraplegia. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 22, 482–490. [Google Scholar] [CrossRef]
- Kotov, S.; Lijdvoy, V.; Sekirin, A.; Petrushanskaya, K.; Pismennaya, E. The efficacy of the exoskeleton ExoAtlet to restore walking in patients with multiple sclerosis. Zhurnal Nevrol. Psikhiatrii Im. SS Korsakova 2017, 117, 41–47. [Google Scholar] [CrossRef]
- He, Y.; Eguren, D.; Azorín, J.M.; Grossman, R.G.; Luu, T.P.; Contreras-Vidal, J.L. Brain–machine interfaces for controlling lower-limb powered robotic systems. J. Neural Eng. 2018, 15, 021004. [Google Scholar] [CrossRef]
- Louie, D.R.; Eng, J.J. Powered robotic exoskeletons in post-stroke rehabilitation of gait: A scoping review. J. NeuroEng. Rehabil. 2016, 13, 53. [Google Scholar] [CrossRef]
- Kazerooni, H.; Steger, R.; Huang, L. Hybrid control of the Berkeley lower extremity exoskeleton (BLEEX). Int. J. Robot. Res. 2006, 25, 561–573. [Google Scholar] [CrossRef]
- Bastian, A.J. Understanding sensorimotor adaptation and learning for rehabilitation. Curr. Opin. Neurol. 2008, 21, 628. [Google Scholar] [CrossRef]
- Huang, V.S.; Krakauer, J.W. Robotic neurorehabilitation: A computational motor learning perspective. J. NeuroEng. Rehabil. 2009, 6, 5. [Google Scholar] [CrossRef]
- Duschau-Wicke, A.; von Zitzewitz, J.; Caprez, A.; Lunenburger, L.; Riener, R. Path control: A method for patient-cooperative robot-aided gait rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2009, 18, 38–48. [Google Scholar] [CrossRef]
- Wu, H.G.; Miyamoto, Y.R.; Castro, L.N.G.; Ölveczky, B.P.; Smith, M.A. Temporal structure of motor variability is dynamically regulated and predicts motor learning ability. Nat. Neurosci. 2014, 17, 312. [Google Scholar] [CrossRef]
- Duschau-Wicke, A.; Caprez, A.; Riener, R. Patient-cooperative control increases active participation of individuals with SCI during robot-aided gait training. J. NeuroEng. Rehabil. 2010, 7, 43. [Google Scholar] [CrossRef]
- Grazi, L.; Crea, S.; Parri, A.; Molino Lova, R.; Micera, S.; Vitiello, N. Gastrocnemius myoelectric control of a robotic hip exoskeleton can reduce the user’s lower-limb muscle activities at push off. Front. Neurosci. 2018, 12, 71. [Google Scholar] [CrossRef]
- Kawamoto, H.; Taal, S.; Niniss, H.; Hayashi, T.; Kamibayashi, K.; Eguchi, K.; Sankai, Y. Voluntary motion support control of Robot Suit HAL triggered by bioelectrical signal for hemiplegia. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 462–466. [Google Scholar]
- Westlake, K.P.; Patten, C. Pilot study of Lokomat versus manual-assisted treadmill training for locomotor recovery post-stroke. J. NeuroEng. Rehabil. 2009, 6, 18. [Google Scholar] [CrossRef]
- Nam, K.Y.; Kim, H.J.; Kwon, B.S.; Park, J.-W.; Lee, H.J.; Yoo, A. Robot-assisted gait training (Lokomat) improves walking function and activity in people with spinal cord injury: A systematic review. J. NeuroEng. Rehabil. 2017, 14, 24. [Google Scholar] [CrossRef]
- Lo, A.C.; Chang, V.C.; Gianfrancesco, M.A.; Friedman, J.H.; Patterson, T.S.; Benedicto, D.F. Reduction of freezing of gait in Parkinson’s disease by repetitive robot-assisted treadmill training: A pilot study. J. NeuroEng. Rehabil. 2010, 7, 51. [Google Scholar] [CrossRef]
- Lo, A.C.; Triche, E.W. Improving gait in multiple sclerosis using robot-assisted, body weight supported treadmill training. Neurorehabil. Neural Repair 2008, 22, 661–671. [Google Scholar] [CrossRef]
- Borggraefe, I.; Schaefer, J.S.; Klaiber, M.; Dabrowski, E.; Ammann-Reiffer, C.; Knecht, B.; Berweck, S.; Heinen, F.; Meyer-Heim, A. Robotic-assisted treadmill therapy improves walking and standing performance in children and adolescents with cerebral palsy. Eur. J. Paediatr. Neurol. 2010, 14, 496–502. [Google Scholar] [CrossRef]
- Esquenazi, A.; Lee, S.; Wikoff, A.; Packel, A.; Toczylowski, T.; Feeley, J. A Comparison of Locomotor Therapy Interventions: Partial-Body Weight− Supported Treadmill, Lokomat, and G-EO Training in People With Traumatic Brain Injury. PMR 2017, 9, 839–846. [Google Scholar] [CrossRef]
- Van Asseldonk, E.H.; van der Kooij, H. Robot-aided gait training with LOPES. In Neurorehabilitation Technology; Springer: Berlin, Germany, 2016; pp. 461–481. [Google Scholar]
- Fleerkotte, B.M.; Koopman, B.; Buurke, J.H.; van Asseldonk, E.H.; van der Kooij, H.; Rietman, J.S. The effect of impedance-controlled robotic gait training on walking ability and quality in individuals with chronic incomplete spinal cord injury: An explorative study. J. NeuroEng. Rehabil. 2014, 11, 26. [Google Scholar] [CrossRef]
- Banala, S.K.; Kim, S.H.; Agrawal, S.K.; Scholz, J.P. Robot assisted gait training with active leg exoskeleton (ALEX). In Proceedings of the 2008 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, Scottsdale, AZ, USA, 19–22 October 2008; pp. 653–658. [Google Scholar]
- Baunsgaard, C.B.; Nissen, U.V.; Brust, A.K.; Frotzler, A.; Ribeill, C.; Kalke, Y.-B.; León, N.; Gómez, B.; Samuelsson, K.; Antepohl, W. Gait training after spinal cord injury: Safety, feasibility and gait function following 8 weeks of training with the exoskeletons from Ekso Bionics. Spinal Cord 2018, 56, 106. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Naro, A.; Russo, M.; Bramanti, P.; Carioti, L.; Balletta, T.; Buda, A.; Manuli, A.; Filoni, S.; Bramanti, A. Shaping neuroplasticity by using powered exoskeletons in patients with stroke: A randomized clinical trial. J. NeuroEng. Rehabil. 2018, 15, 35. [Google Scholar] [CrossRef]
- Molteni, F.; Gasperini, G.; Gaffuri, M.; Colombo, M.; Giovanzana, C.; Lorenzon, C.; Farina, N.; Cannaviello, G.; Scarano, S.; Proserpio, D. Wearable robotic exoskeleton for overground gait training in sub-acute and chronic hemiparetic stroke patients: Preliminary results. Eur. J. Phys. Rehabil. Med. 2017, 53, 676–684. [Google Scholar]
- Benson, I.; Hart, K.; Tussler, D.; van Middendorp, J.J. Lower-limb exoskeletons for individuals with chronic spinal cord injury: Findings from a feasibility study. Clin. Rehabil. 2016, 30, 73–84. [Google Scholar] [CrossRef]
- Esquenazi, A.; Talaty, M.; Packel, A.; Saulino, M. The ReWalk powered exoskeleton to restore ambulatory function to individuals with thoracic-level motor-complete spinal cord injury. Am. J. Phys. Rehabil. Med. 2012, 91, 911–921. [Google Scholar] [CrossRef]
- Kozlowski, A.J.; Fabian, M.; Lad, D.; Delgado, A.D. Feasibility and safety of a powered exoskeleton for assisted walking for persons with multiple sclerosis: A single-group preliminary study. Arch. Phys. Med. Rehabil. 2017, 98, 1300–1307. [Google Scholar] [CrossRef]
- Hartigan, C.; Kandilakis, C.; Dalley, S.; Clausen, M.; Wilson, E.; Morrison, S.; Etheridge, S.; Farris, R. Mobility outcomes following five training sessions with a powered exoskeleton. Top. Spinal Cord Inj. Rehabil. 2015, 21, 93–99. [Google Scholar] [CrossRef]
- Murray, S.A.; Ha, K.H.; Goldfarb, M. An assistive controller for a lower-limb exoskeleton for rehabilitation after stroke, and preliminary assessment thereof. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 4083–4086. [Google Scholar]
- Laffranchi, M.; Semprini, M.; Manzan, E.; Cerruti, G.; Vassallo, C.; De Giuseppe, S.; Maludrottu, S.; Succi, A.; Chiappalone, M.; Gruppioni, E.; et al. A Novel Lower Limb Exoskeleton and new Neurorehabilitation-based Application Scenarios. In Proceedings of the 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC’18), Honolulu, HI, USA, 17–21 July 2018. [Google Scholar]
- Nilsson, A.; Vreede, K.S.; Häglund, V.; Kawamoto, H.; Sankai, Y.; Borg, J. Gait training early after stroke with a new exoskeleton–the hybrid assistive limb: A study of safety and feasibility. J. NeuroEng. Rehabil. 2014, 11, 92. [Google Scholar] [CrossRef]
- Wall, A.; Borg, J.; Palmcrantz, S. Clinical application of the Hybrid Assistive Limb (HAL) for gait training—A systematic review. Front. Syst. Neurosci. 2015, 9, 48. [Google Scholar] [CrossRef]
- Kubota, S.; Nakata, Y.; Eguchi, K.; Kawamoto, H.; Kamibayashi, K.; Sakane, M.; Sankai, Y.; Ochiai, N. Feasibility of rehabilitation training with a newly developed wearable robot for patients with limited mobility. Arch. Phys. Med. Rehabil. 2013, 94, 1080–1087. [Google Scholar] [CrossRef]
- Fitts, P.M.; Peterson, J.R. Information capacity of discrete motor responses. J. Exp. Psychol. 1964, 67, 103. [Google Scholar] [CrossRef]
- Ranganathan, R.; Newell, K.M. Changing up the routine: Intervention-induced variability in motor learning. Exerc. Sport Sci. Rev. 2013, 41, 64–70. [Google Scholar] [CrossRef]
- Cardis, M.; Casadio, M.; Ranganathan, R. High variability impairs motor learning regardless of whether it affects task performance. J. Neurophysiol. 2017, 119, 39–48. [Google Scholar] [CrossRef]
- Stefan, K.; Cohen, L.G.; Duque, J.; Mazzocchio, R.; Celnik, P.; Sawaki, L.; Ungerleider, L.; Classen, J. Formation of a motor memory by action observation. J. Neurosci. 2005, 25, 9339–9346. [Google Scholar] [CrossRef]
- Mattar, A.A.; Gribble, P.L. Motor learning by observing. Neuron 2005, 46, 153–160. [Google Scholar] [CrossRef]
- Hayes, S.J.; Elliott, D.; Bennett, S.J. General motor representations are developed during action-observation. Exp. Brain Res. 2010, 204, 199–206. [Google Scholar] [CrossRef]
- Hodges, N.J.; Williams, A.M.; Hayes, S.J.; Breslin, G. What is modelled during observational learning? J. Sports Sci. 2007, 25, 531–545. [Google Scholar] [CrossRef]
- Cuppone, A.V.; Semprini, M.; Konczak, J. Consolidation of human somatosensory memory during motor learning. Behav. Brain Res. 2018, 347, 184–192. [Google Scholar] [CrossRef]
- Ostry, D.J.; Gribble, P.L. Sensory plasticity in human motor learning. Trends Neurosci. 2016, 39, 114–123. [Google Scholar] [CrossRef]
- Cuppone, A.V.; Squeri, V.; Semprini, M.; Masia, L.; Konczak, J. Robot-assisted proprioceptive training with added vibro-tactile feedback enhances somatosensory and motor performance. PLoS ONE 2016, 11, e0164511. [Google Scholar] [CrossRef]
- Reinkensmeyer, D.J.; Burdet, E.; Casadio, M.; Krakauer, J.W.; Kwakkel, G.; Lang, C.E.; Swinnen, S.P.; Ward, N.S.; Schweighofer, N. Computational neurorehabilitation: Modeling plasticity and learning to predict recovery. J. NeuroEng. Rehabil. 2016, 13, 42. [Google Scholar] [CrossRef]
- Han, C.E.; Arbib, M.A.; Schweighofer, N. Stroke rehabilitation reaches a threshold. PLoS Comput. Biol. 2008, 4, e1000133. [Google Scholar] [CrossRef]
- Reinkensmeyer, D.J.; Guigon, E.; Maier, M.A. A computational model of use-dependent motor recovery following a stroke: Optimizing corticospinal activations via reinforcement learning can explain residual capacity and other strength recovery dynamics. Neural Netw. 2012, 29, 60–69. [Google Scholar] [CrossRef]
- Zenzeri, J.; De Santis, D.; Morasso, P. Strategy switching in the stabilization of unstable dynamics. PLoS ONE 2014, 9, e99087. [Google Scholar] [CrossRef]
- Loram, I.D.; Lakie, M.; Gawthrop, P.J. Visual control of stable and unstable loads: What is the feedback delay and extent of linear time-invariant control? J. Physiol. 2009, 587, 1343–1365. [Google Scholar] [CrossRef]
- Burdet, E.; Osu, R.; Franklin, D.W.; Milner, T.E.; Kawato, M. The central nervous system stabilizes unstable dynamics by learning optimal impedance. Nature 2001, 414, 446. [Google Scholar] [CrossRef]
- Goršič, M.; Cikajlo, I.; Novak, D. Competitive and cooperative arm rehabilitation games played by a patient and unimpaired person: Effects on motivation and exercise intensity. J. NeuroEng. Rehabil. 2017, 14, 23. [Google Scholar] [CrossRef]
- Novak, D.; Nagle, A.; Keller, U.; Riener, R. Increasing motivation in robot-aided arm rehabilitation with competitive and cooperative gameplay. J. NeuroEng. Rehabil. 2014, 11, 64. [Google Scholar] [CrossRef]
- Galofaro, E.; Morasso, P.; Zenzeri, J. Improving motor skill transfer during dyadic robot training through the modulation of the expert role. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17-20 July 2017; pp. 78–83. [Google Scholar]
- Avila Mireles, E.J.; Zenzeri, J.; Squeri, V.; Morasso, P.; De Santis, D. Skill learning and skill transfer mediated by cooperative haptic interaction. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 832–843. [Google Scholar] [CrossRef]
- Birbaumer, N. Breaking the silence: Brain–computer interfaces (BCI) for communication and motor control. Psychophysiology 2006, 43, 517–532. [Google Scholar] [CrossRef]
- Wolpaw, J.R.; Birbaumer, N.; McFarland, D.J.; Pfurtscheller, G.; Vaughan, T.M. Brain–computer interfaces for communication and control. Clin. Neurophysiol. 2002, 113, 767–791. [Google Scholar] [CrossRef]
- Ganguly, K.; Carmena, J.M. Emergence of a stable cortical map for neuroprosthetic control. PLoS Biol. 2009, 7, e1000153. [Google Scholar] [CrossRef]
- Venkatakrishnan, A.; Francisco, G.E.; Contreras-Vidal, J.L. Applications of brain–machine interface systems in stroke recovery and rehabilitation. Curr. Phys. Med. Rehabil. Rep. 2014, 2, 93–105. [Google Scholar] [CrossRef]
- Biasiucci, A.; Leeb, R.; Iturrate, I.; Perdikis, S.; Al-Khodairy, A.; Corbet, T.; Schnider, A.; Schmidlin, T.; Zhang, H.; Bassolino, M. Brain-actuated functional electrical stimulation elicits lasting arm motor recovery after stroke. Nat. Commun. 2018, 9, 2421. [Google Scholar] [CrossRef]
- Luu, T.P.; Nakagome, S.; He, Y.; Contreras-Vidal, J.L. Real-time EEG-based brain-computer interface to a virtual avatar enhances cortical involvement in human treadmill walking. Sci. Rep. 2017, 7, 8895. [Google Scholar] [CrossRef]
- Ramos-Murguialday, A.; Khanna, P.; Sarasola-sanz, A.; Irastorza-Landa, N.; Klein, J.; Jung, J.H.; Garzo, A.; Santisteban, L.; Chueca, C.; Lopez-larraz, E.; et al. A novel implantable hybrid brain-machine-interface (BMI) for motor rehabilitation in stroke patients. In Proceedings of the 2019 9th International IEEE/EMBS Conference on Neural Engineering (NER), San Francisco, CA, USA, 20–23 March 2019. [Google Scholar]
- Maggioni, S.; Melendez-Calderon, A.; van Asseldonk, E.; Klamroth-Marganska, V.; Lünenburger, L.; Riener, R.; van der Kooij, H. Robot-aided assessment of lower extremity functions: A review. J. NeuroEng. Rehabil. 2016, 13, 72. [Google Scholar] [CrossRef]
- Cerasa, A.; Pignolo, L.; Gramigna, V.; Serra, S.; Olivadese, G.; Roccca, F.; Perrotta, P.; Dolce, G.; Quattrone, A.; Tonin, P. Exoskeleton-robot assisted therapy in stroke patients: A lesion mapping study. Front. Neuroinform. 2018, 12, 44. [Google Scholar] [CrossRef]
- Sczesny-Kaiser, M.; Höffken, O.; Lissek, S.; Lenz, M.; Schlaffke, L.; Nicolas, V.; Meindl, R.; Aach, M.; Sankai, Y.; Schildhauer, T.A. Neurorehabilitation in chronic paraplegic patients with the HAL® exoskeleton–preliminary electrophysiological and fMRI data of a pilot study. In Converging Clinical and Engineering Research on Neurorehabilitation; Springer: Berlin, Germany, 2013; pp. 611–615. [Google Scholar]
- Várkuti, B.; Guan, C.; Pan, Y.; Phua, K.S.; Ang, K.K.; Kuah, C.W.K.; Chua, K.; Ang, B.T.; Birbaumer, N.; Sitaram, R. Resting state changes in functional connectivity correlate with movement recovery for BCI and robot-assisted upper-extremity training after stroke. Neurorehabil. Neural Repair 2013, 27, 53–62. [Google Scholar] [CrossRef]
- DeMatteo, C.; Law, M.; Russell, D.; Pollock, N.; Rosenbaum, P.; Walter, S. The reliability and validity of the Quality of Upper Extremity Skills Test. Phys. Occup. Ther. Pediatr. 1993, 13, 1–18. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Smith, M.B. Interrater Reliability of a Modified Ashworth Scale of Muscle Spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef]
- Duncan, P.W.; Propst, M.; Nelson, S.G. Reliability of the Fugl-Meyer Assessment of Sensorimotor Recovery Following Cerebrovascular Accident. Phys. Ther. 1983, 63, 1606–1610. [Google Scholar] [CrossRef]
- Randall, M.; Carlin, J.B.; Chondros, P.; Reddihough, D. Reliability of the Melbourne Assessment of Unilateral Upper Limb Function. Dev. Med. Child Neurol. 2001, 43, 761–767. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult norms for the Box and Block Test of manual dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef]
- Lincoln, N.; Jackson, J.; Adams, S. Reliability and revision of the Nottingham Sensory Assessment for stroke patients. Physiotherapy 1998, 84, 358–365. [Google Scholar] [CrossRef]
- Winward, C.E.; Halligan, P.W.; Wade, D.T. The Rivermead Assessment of Somatosensory Performance (RASP): Standardization and reliability data. Clin. Rehabil. 2002, 16, 523–533. [Google Scholar] [CrossRef]
- Lephart, S.M.; Warner, J.J.; Borsa, P.A.; Fu, F.H. Proprioception of the shoulder joint in healthy, unstable, and surgically repaired shoulders. J. Shoulder Elb. Surg. 1994, 3, 371–380. [Google Scholar] [CrossRef]
- Lephart, S.M.; Kocher, M.S.; Fu, F.H.; Borsa, P.A.; Harner, C.D. Proprioception following anterior cruciate ligament reconstruction. J. Sport Rehabil. 1992, 1, 188–196. [Google Scholar] [CrossRef]
- Gilman, S. Joint position sense and vibration sense: Anatomical organisation and assessment. J. Neurol. Neurosurg. Psychiatry 2002, 73, 473–477. [Google Scholar] [CrossRef]
- Mong, Y.; Teo, T.W.; Ng, S.S. 5-repetition sit-to-stand test in subjects with chronic stroke: Reliability and validity. Arch. Phys. Med. Rehabil. 2010, 91, 407–413. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Watson, M.J. Refining the ten-metre walking test for use with neurologically impaired people. Physiotherapy 2002, 88, 386–397. [Google Scholar] [CrossRef]
- Lanska, D.J.; Goetz, C.G. Romberg’s sign: Development, adoption, and adaptation in the 19th century. Neurology 2000, 55, 1201–1206. [Google Scholar] [CrossRef]
- Blum, L.; Korner-Bitensky, N. Usefulness of the Berg Balance Scale in stroke rehabilitation: A systematic review. Phys. Ther. 2008, 88, 559–566. [Google Scholar] [CrossRef]
- Barnes, M.P.; Dobkin, B.H.; Bogousslavsky, J. Recovery after Stroke; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Maulden, S.A.; Gassaway, J.; Horn, S.D.; Smout, R.J.; DeJong, G. Timing of initiation of rehabilitation after stroke. Arch. Phys. Med. Rehabil. 2005, 86, 34–40. [Google Scholar] [CrossRef]
- Feigenson, J.S.; McDowell, F.H.; Meese, P.; McCarthy, M.L.; Greenberg, S.D. Factors influencing outcome and length of stay in a stroke rehabilitation unit. Part 1. Analysis of 248 unscreened patients--medical and functional prognostic indicators. Stroke 1977, 8, 651–656. [Google Scholar] [CrossRef]
- Dukelow, S.P.; Herter, T.M.; Moore, K.D.; Demers, M.J.; Glasgow, J.I.; Bagg, S.D.; Norman, K.E.; Scott, S.H. Quantitative assessment of limb position sense following stroke. Neurorehabil. Neural Repair 2010, 24, 178–187. [Google Scholar] [CrossRef]
- Lunenburger, L.; Colombo, G.; Riener, R.; Dietz, V. Clinical assessments performed during robotic rehabilitation by the gait training robot Lokomat. In Proceedings of the 9th International Conference on Rehabilitation Robotics (ICORR 2005), Chicago, IL, USA, 28 June–1 July 2005; pp. 345–348. [Google Scholar]
- Debert, C.T.; Herter, T.M.; Scott, S.H.; Dukelow, S. Robotic assessment of sensorimotor deficits after traumatic brain injury. J. Neurol. Phys. Ther. 2012, 36, 58–67. [Google Scholar] [CrossRef]
- Zarrugh, M.Y.; Todd, F.N.; Ralston, H.J. Optimization of energy expenditure during level walking. Eur. J. Appl. Physiol. Occup. Physiol. 1974, 33, 293–306. [Google Scholar] [CrossRef]
- Waters, R.L.; Mulroy, S. The energy expenditure of normal and pathologic gait. Gait Posture 1999, 9, 207–231. [Google Scholar] [CrossRef]
- Quinlivan, B.T.; Lee, S.; Malcolm, P.; Rossi, D.M.; Grimmer, M.; Siviy, C.; Karavas, N.; Wagner, D.; Asbeck, A.; Galiana, I.; et al. Assistance magnitude versus metabolic cost reductions for a tethered multiarticular soft exosuit. Sci. Robot. 2017, 2, eaah4416. [Google Scholar] [CrossRef]
- Gordon, D.F.N.; Henderson, G.; Vijayakumar, S. Effectively Quantifying the Performance of Lower-Limb Exoskeletons Over a Range of Walking Conditions. Front. Robot. AI 2018, 5. [Google Scholar] [CrossRef] [Green Version]
- Rich, C.; Ponsler, B.; Holroyd, A.; Sidner, C.L. Recognizing Engagement in Human-Robot Interaction. In Proceedings of the 5th ACM/IEEE International Conference on Human-Robot Interaction (HRI), Osaka, Japan, 2–5 March 2010; pp. 375–382. [Google Scholar]
- Sandini, G.; Mohan, V.; Sciutti, A.; Morasso, P. Social Cognition for Human-Robot Symbiosis-Challenges and Building Blocks. Front. Neurorobot. 2018, 12, 34. [Google Scholar] [CrossRef]
- Drejing, K.; Thill, S.; Hemeren, P. Engagement: A Traceable Motivational Concept in Human-Robot Interaction. In Proceedings of the 2015 International Conference on Affective Computing and Intelligent Interaction (ACII), Xi’an, China, 21–24 September 2015; pp. 956–961. [Google Scholar]
- Cornforth, D.J.; Koenig, A.; Riener, R.; August, K.; Khandoker, A.H.; Karmakar, C.; Palaniswami, M.; Jelinek, H.F. The role of serious games in robot exoskeleton-assisted rehabilitation of stroke patients. In Serious Games Analytics; Springer: Cham, Switzerland, 2015; pp. 233–254. [Google Scholar]
- He, B.; Sohrabpour, A.; Brown, E.; Liu, Z. Electrophysiological source imaging: A noninvasive window to brain dynamics. Annu. Rev. Biomed. Eng. 2018, 20, 171–196. [Google Scholar] [CrossRef]
- Liu, Q.; Farahibozorg, S.; Porcaro, C.; Wenderoth, N.; Mantini, D. Detecting large-scale networks in the human brain using high-density electroencephalography. Hum. Brain Mapp. 2017, 38, 4631–4643. [Google Scholar] [CrossRef] [Green Version]
- Seeber, M.; Cantonas, L.-M.; Hoevels, M.; Sesia, T.; Visser-Vandewalle, V.; Michel, C.M. Subcortical electrophysiological activity is detectable with high-density EEG source imaging. Nat. Commun. 2019, 10, 753. [Google Scholar] [CrossRef]
- Comani, S.; Velluto, L.; Schinaia, L.; Cerroni, G.; Serio, A.; Buzzelli, S.; Sorbi, S.; Guarnieri, B. Monitoring neuro-motor recovery from stroke with high-resolution EEG, robotics and virtual reality: A proof of concept. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 1106–1116. [Google Scholar] [CrossRef]
- Formaggio, E.; Masiero, S.; Bosco, A.; Izzi, F.; Piccione, F.; Del Felice, A. Quantitative EEG evaluation during robot-assisted foot movement. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 25, 1633–1640. [Google Scholar] [CrossRef]
- Gandolfi, M.; Formaggio, E.; Geroin, C.; Storti, S.F.; Boscolo Galazzo, I.; Bortolami, M.; Saltuari, L.; Picelli, A.; Waldner, A.; Manganotti, P. Quantification of upper limb motor recovery and EEG power changes after robot-assisted bilateral arm training in chronic stroke patients: A prospective pilot study. Neural Plast. 2018, 2018, 8105480. [Google Scholar] [CrossRef]
- Caliandro, P.; Vecchio, F.; Miraglia, F.; Reale, G.; Della Marca, G.; La Torre, G.; Lacidogna, G.; Iacovelli, C.; Padua, L.; Bramanti, P. Small-world characteristics of cortical connectivity changes in acute stroke. Neurorehabil. Neural Repair 2017, 31, 81–94. [Google Scholar] [CrossRef]
- Fornito, A.; Zalesky, A.; Breakspear, M. The connectomics of brain disorders. Nat. Rev. Neurosci. 2015, 16, 159. [Google Scholar] [CrossRef]
- Lenne, B.; Blanc, J.-L.; Nandrino, J.-L.; Gallois, P.; Hautecæur, P.; Pezard, L. Decrease of mutual information in brain electrical activity of patients with relapsing-remitting multiple sclerosis. Behav. Neurol. 2013, 27, 201–212. [Google Scholar] [CrossRef]
- Wang, L.; Yu, C.; Chen, H.; Qin, W.; He, Y.; Fan, F.; Zhang, Y.; Wang, M.; Li, K.; Zang, Y. Dynamic functional reorganization of the motor execution network after stroke. Brain 2010, 133, 1224–1238. [Google Scholar] [CrossRef] [Green Version]
- Vahdat, S.; Darainy, M.; Thiel, A.; Ostry, D.J. A single session of robot-controlled proprioceptive training modulates functional connectivity of sensory motor networks and improves reaching accuracy in chronic stroke. Neurorehabil. Neural Repair 2019, 33, 70–81. [Google Scholar] [CrossRef]
- Carter, A.R.; Shulman, G.L.; Corbetta, M. Why use a connectivity-based approach to study stroke and recovery of function? Neuroimage 2012, 62, 2271–2280. [Google Scholar] [CrossRef] [Green Version]
- Faivre, A.; Rico, A.; Zaaraoui, W.; Crespy, L.; Reuter, F.; Wybrecht, D.; Soulier, E.; Malikova, I.; Confort-Gouny, S.; Cozzone, P.J. Assessing brain connectivity at rest is clinically relevant in early multiple sclerosis. Mult. Scler. J. 2012, 18, 1251–1258. [Google Scholar] [CrossRef]
- Wu, J.; Quinlan, E.B.; Dodakian, L.; McKenzie, A.; Kathuria, N.; Zhou, R.J.; Augsburger, R.; See, J.; Le, V.H.; Srinivasan, R. Connectivity measures are robust biomarkers of cortical function and plasticity after stroke. Brain 2015, 138, 2359–2369. [Google Scholar] [CrossRef] [Green Version]
- Faiman, I.; Pizzamiglio, S.; Turner, D.L. Resting-state functional connectivity predicts the ability to adapt arm reaching in a robot-mediated force field. Neuroimage 2018, 174, 494–503. [Google Scholar] [CrossRef]
- Meyer, T.; Peters, J.; Zander, T.O.; Schölkopf, B.; Grosse-Wentrup, M. Predicting motor learning performance from electroencephalographic data. J. NeuroEng. Rehabil. 2014, 11, 24. [Google Scholar] [CrossRef]
- Cole, D.M.; Smith, S.M.; Beckmann, C.F. Advances and pitfalls in the analysis and interpretation of resting-state FMRI data. Front. Syst. Neurosci. 2010, 4, 8. [Google Scholar] [CrossRef] [Green Version]
- Cesqui, B.; Tropea, P.; Micera, S.; Krebs, H.I. EMG-based pattern recognition approach in post stroke robot-aided rehabilitation: A feasibility study. J. NeuroEng. Rehabil. 2013, 10, 75. [Google Scholar] [CrossRef]
- Cheung, V.C.; Turolla, A.; Agostini, M.; Silvoni, S.; Bennis, C.; Kasi, P.; Paganoni, S.; Bonato, P.; Bizzi, E. Muscle synergy patterns as physiological markers of motor cortical damage. Proc. Natl. Acad. Sci. USA 2012, 109, 14652–14656. [Google Scholar] [CrossRef] [Green Version]
- Semprini, M.; Cuppone, A.V.; Delis, I.; Squeri, V.; Panzeri, S.; Konczak, J. Biofeedback signals for robotic rehabilitation: Assessment of wrist muscle activation patterns in healthy humans. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 25, 883–892. [Google Scholar] [CrossRef]
- Delis, I.; Panzeri, S.; Pozzo, T.; Berret, B. A unifying model of concurrent spatial and temporal modularity in muscle activity. J. Neurophysiol. 2013, 111, 675–693. [Google Scholar] [CrossRef]
- Liu, W.; Waller, S.M.; Kepple, T.; Whitall, J. Compensatory arm reaching strategies after stroke: Induced position analysis. J. Rehabil. Res. Dev. 2013, 50, 71. [Google Scholar] [CrossRef]
- Belfatto, A.; Scano, A.; Chiavenna, A.; Mastropietro, A.; Mrakic-Sposta, S.; Pittaccio, S.; Molinari Tosatti, L.; Molteni, F.; Rizzo, G. A Multiparameter Approach to Evaluate Post-Stroke Patients: An Application on Robotic Rehabilitation. Appl. Sci. 2018, 8, 2248. [Google Scholar] [CrossRef]
- Lamers, I.; Feys, P.; Swinnen, E. Robot-assisted rehabilitation in multiple sclerosis: Overview of approaches, clinical outcomes, and perspectives. In Rehabilitation Robotics; Elsevier: Amsterdam, The Netherlands, 2018; pp. 253–266. [Google Scholar]
- Young, A.J.; Ferris, D.P. State of the art and future directions for lower limb robotic exoskeletons. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 25, 171–182. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| End-Effector Name and Main Reference | Classification | Actuators | Targeted DOFs | Training Modality | Type of Disease |
|---|---|---|---|---|---|
| MIT Manus [33] | Planar manipulandum | Electric | Shoulder; Elbow | Passive; Active; Active Assistive | Stroke [26]; ABI [34]; CP [35] |
| ARM (Assisted Rehabilitation and Measurement) Guide [27] | “Trombone-like” device, as defined in [36] | Electric | Shoulder; Elbow | Passive; Active; Active Assistive; Active Resistive | Stroke [37] |
| GENTLE/s [38] | End-point manipulator | Electric/Haptic Master [39] | Shoulder; Elbow; Wrist | Passive; Active; Active Assistive | Stroke [28] |
| NeReBot (Neurorehabilitation Robot) [29] | Wire-driven robot | Electric | Shoulder; Elbow; Wrist | Passive; Active | Stroke [40] |
| ACT3D (Arm Coordination Training Robot) [30] | Planar manipulandum | Electric | Shoulder; Elbow | Passive; Active | Stroke [41] |
| MIME (Mirror Image Motion Enabler) [31] | Bimanual manipulandum | Electric | Shoulder; Elbow | Passive; Active assistive (unimanual and bimanual); Active Resistive | Stroke [42] |
| Bi-Manu-Track [32] | Bimanual manipulandum | Electric | Forearm; Wrist | Passive; Passive-Mirrored; Active Resistive | Stroke [21] |
| Braccio di Ferro [43] | Planar manipulandum | Electric | Shoulder; Elbow | Passive; Active; Active Assistive; Active Resistive | MS [44]; Stroke [45] |
| Wristbot [46] | End-point manipulator | Electric | Wrist | Passive; Active; Active Assistive; Active Resistive | Stroke [20,47]; Dystonia [48] |
| Exoskeleton Name and Main Reference | Actuators | Actuated DOFs | Training Modality | Trigger Event for Movement initiation | Type of Disease |
|---|---|---|---|---|---|
| SUEFUL7 [49] | Electric | Shoulder vertical and horizontal flex./ext.; shoulder internal/external rot.; elbow flex./ext.; forearm sup./pron.; wrist flex./ext.; and wrist radial/ulnar dev. | Active; Passive | Supra-threshold surface EMG activity | - |
| ARMin III [50] | Electric | Shoulder joint in three DOFs; elbow flex./ext.; lower arm pron./sup.; and wrist flex./ext. | Active; Passive; Active Assistive | Assist-as-needed strategy based on performance | Stroke [57]; SCI [58]; other diseases [58] |
| CADEN [51] | Electric (Brushed motors—Cable drive) | Shoulder flex./ext.; abd./add.; internal/external rot.; elbow flex./ext.; forearm sup./pron.; wrist flex./ext.; and radial/ulnar dev. | Active; Passive | - | - |
| RUPERT [52] | Pneumatic | Shoulder flex./ext.; humeral internal/external rot.; elbow flex./ext.; forearm pron./sup.; and wrist flex./ext. | Passive | Movement trajectory and amount of forces exerted | Stroke [59] |
| L-Exos [54] | Electric | Shoulder abd./add.; elbow flex./ext.; wrist pron./sup. | Active; Passive | - | Stroke [60] |
| UL-Exo7 [51] | Electric | Shoulder flex./ext.; shoulder abd./add.; shoulder internal–external rot.; elbow flex./ext.; forearm rot.; wrist flex./ext.; and wrist radial–ulnar dev. | Passive; Active; Active Assistive | Based on the target location and current end-effector position | Stroke [61,62] |
| Pneu-Wrex [63] | Pneumatic | Forward/backward clavicle rot.; shoulder flex./ext.; shoulder horizontal abd./add.; and elbow flex./ext. | Passive; Active; Active Assistive | Assistance-as-needed strategy based on performance | Stroke [55] |
| IntelliArm [64] | Electric | Shoulder abd./add.; flex./ext.: internal/external rot.; elbow flex./ext., and forearm sup./pron.; wrist flex./ext.; hand open/grasp at MCP and thumb joints. | Passive; Active; Active Assistive; Active Resistive | Time elapsed | - |
| BONES [65] | Pneumatic | Shoulder abd./add.; flex./ext.; internal/external rot.; elbow flex./ext. | Passive; Active; Active Assistive | Assist-as-needed strategy based on performance | Stroke [65] |
| End-Effector Name and Main Reference | Classification | Actuators | Actuated DOFs | Training Modality | Type of Disease |
|---|---|---|---|---|---|
| Gait Trainer [84] | Footplate-based | Electric and Mechanical (ropes for controlling COM displacement in vertical and horizontal plane) | Movable footplates allowing for feet movement in the sagittal plane (walking on a flat surface); COM vertical direction; COM horizontal direction | Passive; Active | Stroke [93,94] *; MS [95]; Parkinson [96]; CP [97] |
| Haptic Walker [85] | Footplate-based | Electric | Freely programmable footplates allowing for feet movements in a 3D space. Simulation of complex movements (climbing) | Passive; Active | - |
| G-EO Systems [86] | Footplate-based | Electric | Freely programmable footplates allowing for walking and climbing | Active Assistive | Stroke [86] |
| Hunova [91] | Platform-based | Electric | Ankle Dors./Plant.; Ankle Inv./Evers.; Sagittal plane pelvis rot.; Frontal plane pelvis rot. | Passive; Active; Active Assistive; Active Resistive | Elderly [88]; work-related injuries [98] |
| Rutgers Ankle [89] | Platform-based | Pneumatic | Three ankle translations; Ankle Dors./Plant.; Ankle Inv./Evers.; Ankle Internal and External rot. | Passive; Active; Active Resistive | Stroke, musculo-skeletal ankle injuries, CP [90] ** |
| Exoskeleton Name and Main Reference | Classification | Actuators | Actuated DOFs | Training Modality | Trigger Event for Movement Initiation | Type of Disease |
|---|---|---|---|---|---|---|
| Lokomat [99] | Treadmill-based | Electric | Hip flex./ext. (×2); Knee flex./ext. (×2) | Passive; Active Assistive | - | Stroke [117]; SCI [118]; Parkinson [119]; MS [120]; CP [121]; TBI [122] * |
| LokoHelp [100] | Treadmill-based | Treadmill drive | Levers mounted on the treadmill allowing for the two legs two DOFs movement | Passive; Active Assistive | - | Stroke, SCI, TBI [100] |
| LOPES [101] | Treadmill-based | Series elastic actuator | Pelvis horizontal translation; Hip flex./ext. (×2); Hip abd./add. (×2); Knee flex./ext. (×2) | Passive (robot-in-charge mode) Active (patient-in charge mode) | - | Stroke [123]; SCI [124] |
| ALEX [102] | Treadmill-based | Electric | Pelvis lateral translation; Pelvis vertical translation; Vertical-axis pelvis rotation; Hip flex./ext. (×2); Hip abd./add. (×2); Knee flex./ext. (×2); Ankle dors./plant. (×2) | Active | - | Stroke [125] |
| Ekso [103] | Overground-walking | Electric | Hip flex./ext. (×2); Knee flex./ext. (×2) | Active; Active Assistive; Active Resistive | Trunk inclination and weight shift; (antero-lateral or lateral movement) or joystick button push | SCI [126]; Stroke [127,128] |
| Rewalk [104] | Overground-walking | Electric | Hip flex./ext. (×2); Knee flex./ext. (×2) | Passive (ReWalk 6.0); Active Assistive (Rewalk 2.0) | Trunk inclination and weight shift | SCI [129,130]; MS [131] |
| Indego Therapy [105] | Overground-walking | Electric | Hip flex./ext. (×2); Knee flex./ext. (×2) | Passive; Active; Active Assistive | Forward movement of hip and trunk (vibro-tactile feedback, Motion+ mode) or hip movement (Therapy+ mode) | SCI [132]; Stroke [133] |
| Twin [83,134] | Overground-walking | Electric | Hip flex./ext. (×2); Knee flex./ext. (×2) | Passive; Active Assistive (under development) | Trunk inclination associated with acoustic feedback | - |
| HAL [116] | Overground-walking | Electric | Hip flex./ext. (×2); Knee flex./ext. (×2) | Active Assistive | Supra-threshold surface EMG activity | Stroke [135]; SCI and other diseases [136,137]; |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iandolo, R.; Marini, F.; Semprini, M.; Laffranchi, M.; Mugnosso, M.; Cherif, A.; De Michieli, L.; Chiappalone, M.; Zenzeri, J. Perspectives and Challenges in Robotic Neurorehabilitation. Appl. Sci. 2019, 9, 3183. https://doi.org/10.3390/app9153183
Iandolo R, Marini F, Semprini M, Laffranchi M, Mugnosso M, Cherif A, De Michieli L, Chiappalone M, Zenzeri J. Perspectives and Challenges in Robotic Neurorehabilitation. Applied Sciences. 2019; 9(15):3183. https://doi.org/10.3390/app9153183
Chicago/Turabian StyleIandolo, Riccardo, Francesca Marini, Marianna Semprini, Matteo Laffranchi, Maddalena Mugnosso, Amel Cherif, Lorenzo De Michieli, Michela Chiappalone, and Jacopo Zenzeri. 2019. "Perspectives and Challenges in Robotic Neurorehabilitation" Applied Sciences 9, no. 15: 3183. https://doi.org/10.3390/app9153183