Probability of Abnormal Indoor Air Exposure Categories Compared with Occupants’ Symptoms, Health Information, and Psychosocial Work Environment

Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
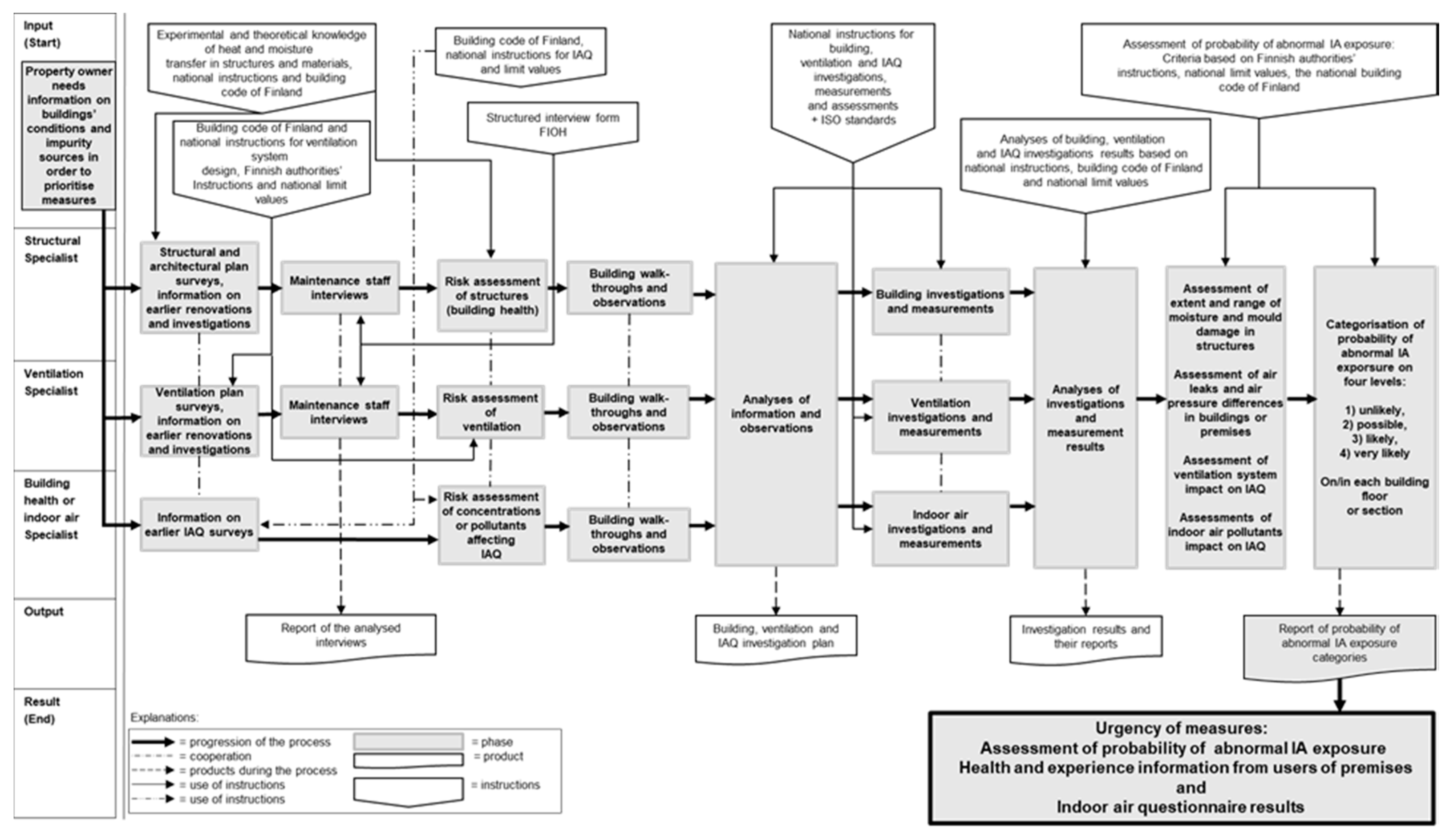
2.2. Assessment of Probability of Abnormal IA Exposure
2.3. Employees’ Experiences of Indoor Air Quality and Psychosocial Work Environment
2.4. Group-Level Information from Occupational Health Services and Multiprofessional Indoor Air Group
2.5. Statistical Analyses
3. Results
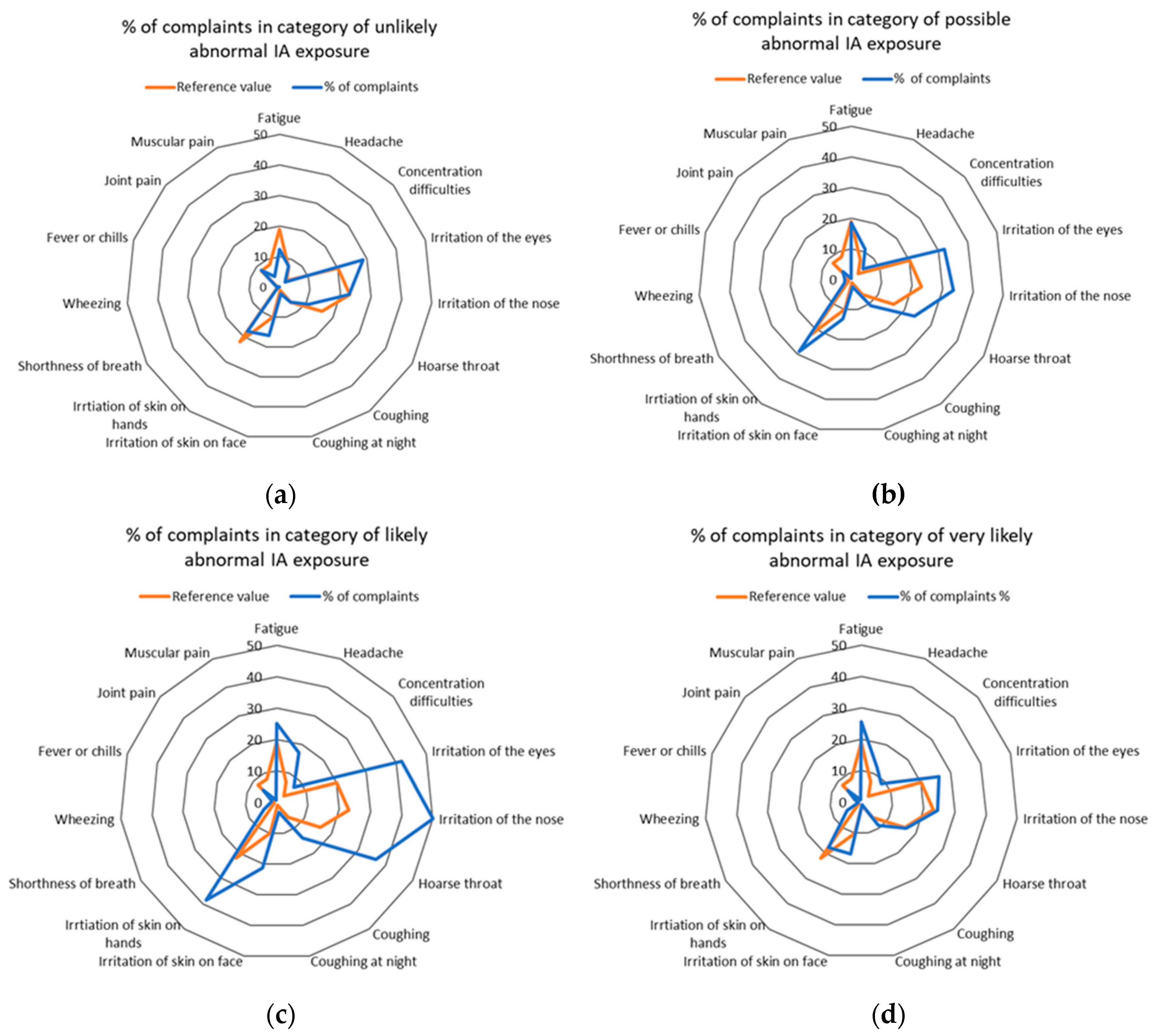
Probability of Abnormal IA Exposure and Employees’ Experience
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| FIOH | Finnish Institute of Occupational Health |
| IA | Indoor air |
| IAQ | Indoor air quality |
| OHS | Occupational health service |
| PAH | Polycyclic aromatic hydrocarbon |
| VOC | Volatile organic compound |
References
- Frontczak, M.; Wargocki, P. Literature survey on how different factors influence human comfort in indoor environments. Build. Environ. 2011, 46, 922–937. [Google Scholar] [CrossRef]
- WHO. Dampness and Mould—Who Guidelines for Indoor Air Quality; World Health Organisation: Geneva, Switzerland, 2009. [Google Scholar]
- Lappalainen, S.; Lahtinen, M.; Palomaki, E.; Korhonen, P.; Niemelä, R.; Reijula, K. Comprehensive procedure for solving indoor environment problems. In Proceedings of the NAM Nordic Work Environment Meeting, Espoo, Finland, 31 August–2 September 2009; p. 93. [Google Scholar]
- Lahtinen, M.; Huuhtanen, P.; Kahkonen, E.; Reijula, K. Psychosocial dimensions of solving an indoor air problem. Indoor Air 2002, 12, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Salonen, H.; Lappalainen, S.; Riuttala, H.; Tossavainen, A.; Pasanen, P.; Reijula, K. Man-made vitreous fibers in office buildings in the helsinki area. J. Occup. Environ. Hyg. 2009, 6, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Sundell, J.; Levin, H.; Nazaroff, W.W.; Cain, W.S.; Fisk, W.J.; Grimsrud, D.T.; Gyntelberg, F.; Li, Y.; Persily, A.K.; Pickering, A.C.; et al. Ventilation rates and health: Multidisciplinary review of the scientific literature. Indoor Air 2011, 21, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Wolkoff, P.; Wilkins, C.K.; Clausen, P.A.; Nielsen, G.D. Organic compounds in office environments—Sensory irritation, odor, measurements and the role of reactive chemistry. Indoor Air 2006, 16, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Airaksinen, M.; Pasanen, P.; Kurnitski, J.; Seppänen, O. Microbial contamination of indoor air due to leakages from crawl space: A field study. Indoor Air 2004, 14, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Nevalainen, A.; Täubel, M.; Hyvärinen, A. Indoor fungi: Companions and contaminants. Indoor Air 2015, 25, 125–156. [Google Scholar] [CrossRef]
- Nordström, K.; Norbäck, D.; Akselsson, R. Effect of air humidification on the sick building syndrome and perceived indoor air quality in hospitals: A four month longitudinal study. Occup. Environ. Med. 1994, 51, 683–688. [Google Scholar] [CrossRef]
- Mendell, M.J.; Kumagai, K. Observation-based metrics for residential dampness and mold with dose–response relationships to health: A review. Indoor Air 2017, 27, 506–517. [Google Scholar] [CrossRef]
- Hellgren, U.-M.; Hyvärinen, M.; Holopainen, R.; Reijula, K. Perceived indoor air quality, air-related symptoms and ventilation in finnish hospitals. Int. J. Occup. Med. Environ. Health 2011, 24, 48–56. [Google Scholar] [CrossRef]
- Redlich, C.; Sparer, J.; Cullen, M.R. Sick-building syndrome. Lancet 1997, 349, 1013–1016. [Google Scholar] [CrossRef]
- Schneider, T. Dust and fibers as a cause of indoor environment problems. Scand. J. Work. Environ. Health 2008, 33, 10–17. [Google Scholar]
- Milton, D.K.; Glencross, P.M.; Walters, M.D. Risk of sick leave associated with outdoor air supply rate, humidification, and occupant complaints. Indoor Air 2000, 10, 212. [Google Scholar] [CrossRef] [PubMed]
- Cox-Ganser, J.; Rao, C.; Park, J.; Schumpert, J.; Kreiss, K. Asthma and respiratory symptoms in hospital workers related to dampness and biological contaminants. Indoor Air 2009, 19, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Mendell, M.; Brennan, T.; Lee, H.; Odom, J.D.; Offerman, F.J.; Turk, B.H.; Wallingford, K.M.; Diamond, R.C.; Fisk, W.J. Causes and prevention of symptom complaints in office buildings. Facilities 2006, 24, 436–444. [Google Scholar] [CrossRef]
- Sauni, R.; Verbeek, J.H.; Uitti, J.; Jauhiainen, M.; Kreiss, K.; Sigsgaard, T. Remediating buildings damaged by dampness and mould for preventing or reducing respiratory tract symptoms, infections and asthma. Cochrane Database Syst. Rev. 2015, 76, 1. [Google Scholar] [CrossRef] [PubMed]
- Wargocki, P.; Lagercrantz, L.; Witterseh, T.; Sundell, J.; Wyon, D.P.; Fanger, P.O. Subjective perceptions, symptom intensity and performance: A comparison of two independent studies, both changing similarly the pollution load of an office. Indoor Air 2002, 12, 74. [Google Scholar] [CrossRef]
- Brauer, C.; Mikkelsen, S. The influence of individual and contextual psychosocial work factors on the perception of the indoor environment at work: A multilevel analysis. Int. Arch. Occup. Environ. Health 2010, 83, 639–651. [Google Scholar] [CrossRef]
- Magnavita, N. Work-related symptoms in indoor environments: A puzzling problem for the occupational physician. Int. Arch. Occup. Environ. Health 2015, 88, 185–196. [Google Scholar] [CrossRef]
- Finell, E.; Haverinen-Shaughnessy, U.; Tolvanen, A.; Laaksonen, S.; Karvonen, S.; Sund, R.; Saaristo, V.; Luopa, P.; Ståhl, T.; Putus, T.; et al. The associations of indoor environment and psychosocial factors on the subjective evaluation of indoor air quality among lower secondary school students: A multilevel analysis. Indoor Air 2017, 27, 329–337. [Google Scholar] [CrossRef]
- Lahtinen, M.; Lappalainen, S.; Reijula, K. Multiprofessional teams resolving indoor-air problems-emphasis on the psychosocial perspective. Scand. J. Work. Environ. Health 2008, 34, 30–34. [Google Scholar]
- Carrer, P.; Wolkoff, P. Assessment of indoor air quality problems in office-like environments: Role of occupational health services. Int. J. Environ. Res. Public Health 2018, 15, 741. [Google Scholar] [CrossRef] [PubMed]
- Tähtinen, K.; Lappalainen, S.; Karvala, K.; Remes, J.; Salonen, H. Association between four-level categorisation of indoor exposure and perceived indoor air quality. Int. J. Environ. Res. Public Health 2018, 15, 679. [Google Scholar] [CrossRef] [PubMed]
- Finnish Ministry of the Environment, Department of Built Environment. D2 the National Building Code of Finland, Health. Indoor Climate and Ventilation of Buildings, Regulations and Guidelines; Department of Built Environment: Helsinki, Finland, 2012.
- Andersson, K. Epidemiological approach to indoor air problems. Indoor Air 1998, 8, 32–39. [Google Scholar] [CrossRef]
- Hellgren, U.-M.; Palomaki, E.; Lahtinen, M.; Riuttala, H.; Reijula, K. Complaints and symptoms among hospital staff in relation to indoor air and the condition and need for repairs in hospital buildings. Scand. J. Work Environ. Health 2008, 34, 58–63. [Google Scholar]
- Reijula, K.; Sundman-Digert, C. Assessment of indoor air problems at work with a questionnaire. Occup. Environ. Med. 2004, 61, 33–38. [Google Scholar] [PubMed]
- Elo, A.-L.; Leppänen, A.; Jahkola, A. Validity of a single-item measure of stress symptoms. Scand. J. Work Environ. Health 2003, 29, 444–451. [Google Scholar] [CrossRef] [Green Version]
- Tähtinen, K.; Lappalainen, S.; Karvala, K.; Salonen, H. A comprehensive approach to evaluating the urgency of iaq measures. In Proceedings of the 15th Conference of the International Society of Indoor Air Quality & Climate (ISIAQ), Philadelphia, PA, USA, 22–27 July 2018. [Google Scholar]
- Lahtinen, M.; Sundman-Digert, C.; Reijula, K. Psychosocial work environment and indoor air problems: A questionnaire as a means of problem diagnosis. Occup. Environ. Med. 2004, 61, 143. [Google Scholar] [CrossRef]
- Bakke, J.; Moen, B.; Wieslander, G.; Norbäck, D. Gender and the physical and psychosocial work environments are related to indoor air symptoms. J. Occup. Environ. Med. 2007, 49, 641–650. [Google Scholar] [CrossRef]
- Finell, E.; Seppälä, T. Indoor air problems and experiences of injustice in the workplace: A quantitative and a qualitative study. Indoor Air 2018, 28, 125–134. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Categories | Main Criteria for Assessing Probability of Abnormal IA Exposure in Buildings. |
|---|---|
| Unlikely | No moisture or mould damage in structures. No air leaks from or through damaged structures. Ventilation system can be controlled by indoor pressure difference from the building envelope. Room acoustic materials and ventilation system have no man-made vitreous fibres (MMVF) sources. Indoor air quality corresponds to national reference values and guidelines set for the premises. |
| Possible | Mould-damaged structure type is not widespread in building and repairs are easily definable (less than 1 m2). A few or single air leaks from or through damaged structures or from surrounding premises. Room acoustic materials or ventilation system have MMVF sources and fibres may end up in the indoor air or on surfaces.1 Concrete floor has extensive moisture, which can cause water vapour damage to permeable floor coating (emissions).1 Indoor air quality does not correspond to national reference values or the guidelines set for the premises, and an indoor air impurity source has been identified.1 |
| Likely | Building or premises have widespread mould-damaged structure. Repairs are significant and affect a large part of the (one) structure of the building or premises, e.g., whole base floor structure. There is recurrent damage in the type of structure. Air leaks from or through damaged structures or from surrounding premises and moisture or mould-damaged materials are regular and recurrent in the structure, occasionally there is negative pressure in the premises and/or air-tightness is risky. Indoor air quality does not correspond to national reference values or the guidelines set for the premises, and an indoor air impurity source has been identified.1 Creosote has been used in the structure and air leaks into the indoor air from the structure. There is also a notable smell of creosote (e.g., naphthalene) in the indoor air.1 |
| Very likely | The building or premises has a great deal of extensive mould damage in several structures. The extent of repairs is significant and affects several structures in the building or premises e.g., whole façade and whole base floor. There is recurrent damage in the type of the structures. Air leaks from or through damaged structures are regular and recurrent, negative pressure is significant in the premises and/or air-tightness is very risky. Indoor air quality does not correspond to national reference values or the guidelines set for the premises, and an indoor air impurity source has been identified.1 Creosote has been used in the structures and air leaks into the indoor air from the structures. In addition, concentrations of polycyclic aromatic hydrocarbons (PAH) or separate components exceed the set national values and guidelines.1 Dust sample tests have found asbestos fibres in the premises, and the pollution source has been defined.1 Indoor radon concentrations exceed the set national values and guidelines (400 Bq/m3 [26]).1 |
| Assessed Probability of Abnormal IA Exposure on/in Building Floors or Sections (n = 95) | Lifespan of Ventilation System Had Been Exceeded n (%) | Insufficient Ventilation n (%) | MMVF (Man-Made Vitreous Fibres) Source in Ventilation System n (%) | Moisture Problem in Ventilation System n (%) |
|---|---|---|---|---|
| Unlikely (n = 7) | 7 (100) | 3 (43) | 3 (43) | 0 (0) |
| Possible (n = 39) | 23 (59) | 22 (56) | 12 (31) | 6 (15) |
| Likely (n = 37) | 26 (70) | 24 (65) | 26 (70) | 15 (41) |
| Very likely (n = 12) | 10 (83) | 9 (75) | 9 (75) | 1 (8) |
| Variable (Weekly Symptoms) | Unlikely 1 n = 2 (p-Value) | Possible 2 n = 16 (p-Value) | Likely 3 n = 18 (p-Value) | Very Likely 4 n = 4 |
|---|---|---|---|---|
| Fatigue | 1 vs. 2 (0.673) | 2 vs. 3 (0.220) | 3 vs. 4 (0.609) | |
| 1 vs. 3 (0.257) | 2 vs. 4 (0.570) | |||
| 1 vs. 4 (0.355) | ||||
| Headache | 1 vs. 2 (0.778) | 2 vs. 3 (0.157) | 3 vs. 4 (0.481) | |
| 1 vs. 3 (0.208) | 2 vs. 4 (0.777) | |||
| 1 vs. 4 (0.643) | ||||
| Concentration difficulties | 1 vs. 2 (0.672) | 2 vs. 3 (0.233) | 3 vs. 4 (1.000) | |
| 1 vs. 3 (0.165) | 2 vs. 4 (0.507) | |||
| 1 vs. 4 (0.064) | ||||
| Irritation of the eyes | 1 vs. 2 (0.888) | 2 vs. 3 (0.262) | 3 vs. 4 (0.125) | |
| 1 vs. 3 (0.378) | 2 vs. 4 (0.777) | |||
| 1 vs. 4 (0.814) | ||||
| Irritation of the nose | 1 vs. 2 (0.779) | 2 vs. 3 (0.073) | 3 vs. 4 (0.061) | |
| 1 vs. 3 (0.130) | 2 vs. 4 (0.925) | |||
| 1 vs. 4 (0.643) | ||||
| Hoarse, dry throat | 1 vs. 2 (0.399) | 2 vs. 3 (0.101) | 3 vs. 4 (0.061) | |
| 1 vs. 3 (0.130) | 2 vs. 4 (0.508) | |||
| 1 vs. 4 (1.000) | ||||
| Coughing | 1 vs. 2 (0.481) | 2 vs. 3 (0.147) | 3 vs. 4 (0.287) | |
| 1 vs. 3 (0.378) | 2 vs. 4 (0.636) | |||
| 1 vs. 4 (0.355) | ||||
| Coughing at night | 1 vs. 2 (0.941) | 2 vs. 3 (0.652) | 3 vs. 4 (0.237) | |
| 1 vs. 3 (0.792) | 2 vs. 4 (0.289) | |||
| 1 vs. 4 (0.411) | ||||
| Irritation of skin on face | 1 vs. 2 (0.260) | 2 vs. 3 (0.133) | 3 vs. 4 (0.551) | |
| 1 vs. 3 (1.000) | 2 vs. 4 (0.508) | |||
| 1 vs. 4 (1.000) | ||||
| Irritation of skin on hands | 1 vs. 2 (0.888) | 2 vs. 3 (0.152) | 3 vs. 4 (0.349) | |
| 1 vs. 3 (0.378) | 2 vs. 4 (0.705) | |||
| 1 vs. 4 (1.000) | ||||
| Shortness of breath | 1 vs. 2 (0.562) | 2 vs. 3 (0.508) | 3 vs. 4 (0.663) | |
| 1 vs. 3 (0.509) | 2 vs. 4 (0.502) | |||
| 1 vs. 4 (0.355) | ||||
| Wheezing | 1 vs. 2 (0.374) | 2 vs. 3 (0.342) | 3 vs. 4 (0.275) | |
| 1 vs. 3 (0.178) | 2 vs. 4 (0.600) | |||
| 1 vs. 4 (0.480) | ||||
| Fever or chills | 1 vs. 2 (0.352) | 2 vs. 3 (0.308) | 3 vs. 4 (1.000) | |
| 1 vs. 3 (0.736) | 2 vs. 4 (0.562) | |||
| 1 vs. 4 (0.623) | ||||
| Muscular pain | 1 vs. 2 (1.000) | 2 vs. 3 (0.161) | 3 vs. 4 (0.932) | |
| 1 vs. 3 (0.44) | 2 vs. 4 (0.298) | |||
| 1 vs. 4 (1.000) | ||||
| Joint pain | 1 vs. 2 (0.324) | 2 vs. 3 (0.283) | 3 vs. 4 (0.898) | |
| 1 vs. 3 (0.900) | 2 vs. 4 (0.570) | |||
| 1 vs. 4 (0.643) | ||||
| Other work environment- | 1 vs. 2 (0.176) | 2 vs. 3 (0.099) | 3 vs. 4 (0.831) | |
| related symptoms | 1 vs. 3 (0.074) | 2 vs. 4 (0.288) | ||
| 1 vs. 4 (0.060) |
| Question on Psychosocial Work Environment | Unlikely n = 61 (%) | Possible n = 619 (%) | Likely n = 763 (%) | Very Likely n = 118 (%) | FIOH’s Reference Value % |
|---|---|---|---|---|---|
| Do you regard your work as interesting and stimulating? | |||||
| Yes, often | 52 (88.1) | 540 (87.5) | 684 (89.9) | 102 (86.4) | 82 |
| Yes, sometimes | 7 (11.9) | 66 (10.7) | 61 (8.0) | 11 (9.3) | 16 |
| No, seldom or rarely | 0 (0) | 11 (1.8) | 16 (2.0) | 5 (4.2) | 0 |
| Do you have too much work? | |||||
| Yes, often | 12 (20.7) | 95 (15.5) | 98 (12.9) | 15 (12.7) | 20 |
| Yes, sometimes | 36 (62.1) | 360 (58.7) | 489 (64.4) | 71 (60.2) | 64 |
| No, seldom or rarely | 10 (17.2) | 158 (25.8) | 172 (22.7) | 32 (27.1) | 16 |
| Do you have opportunities to influence your working conditions? | |||||
| Yes, often | 38 (32.8) | 120 (19.5) | 161 (21.2) | 38 (32.8) | 21 |
| Yes, sometimes | 61 (52.6) | 335 (54.3) | 379 (49.9) | 61 (52.6) | 51 |
| No, seldom or rarely | 17 (14.7) | 162 (26.3) | 220 (29.0) | 17 (14.7) | 28 |
| Do your fellow workers help you with work-related problems? | |||||
| Yes, often | 33 (55.9) | 463 (75.2) | 569 (74.8) | 83 (70.3) | 79 |
| Yes, sometimes | 24 (40.7) | 129 (20.9) | 171 (22.5) | 28 (23.7) | 19 |
| No, seldom or rarely | 2 (3) | 24 (3.9) | 21 (2.8) | 7 (5.9) | 2 |
| Do you feel stress? | |||||
| Quite a lot or very much | 15 (26.3) | 92 (15.1) | 105 (15.0) | 16 (14.0) | 10 |
| Some | 12 (21.1) | 181 (29.7) | 243 (32.4) | 40 (35.1) | 28 |
| Not at all or just a little | 30 (52.6) | 337 (55.2) | 403 (53.7) | 58 (50.9) | 63 |
| IAQ-Related Health Information | Unlikely n = 2 (%) | Possible n = 16 (%) | Likely n = 20 (%) | Very likely n = 5 (%) |
|---|---|---|---|---|
| Some employees have new asthma or aggravation of previous asthma 1 | ||||
| Yes | 2 (100) | 5 (31) | 5 (25) | 3 (60) |
| No | 0 (0) | 10 (63) | 14 (70) | 2 (40) |
| No information | 0 (0) | 1 (6) | 1 (5) | 0 (0) |
| Some employees have changed work premises or work places due to IAQ-related symptoms 1 | ||||
| Yes | 1 (50) | 4 (25) | 4 (20) | 2 (40) |
| No | 1 (50) | 11 (69) | 16 (80) | 3 (60) |
| No information | 0 (0) | 1 (6) | 0 (0) | 0 (0) |
| The amount of employee contacts with OHS due to IAQ-related issues has increased 1 | ||||
| Yes | 2 (100) | 5 (31) | 10 (50) | 3 (60) |
| No | 0 (0) | 10 (63) | 10 (50) | 2 (40) |
| No information | 0 (0) | 1 (6) | 0 (0) | 0 (0) |
| The amount of sickness absence due to respiratory symptoms has increased 1 | ||||
| Yes | 1 (50) | 4 (25) | 8 (40) | 1 (20) |
| No | 0 (0) | 7 (44) | 11 (55) | 3 (60) |
| No information | 1 (50) | 5 (31) | 1 (5) | 1 (20) |
| Perceived Work Environment-Related Symptoms Weekly | Respondents N = 1558 n | Technical Lifespan of Ventilation System Had Been Exceeded | Moisture Problem in Ventilation System | MMVF Source in Ventilation System | Insufficient Ventilation or Ventilation System Did Not Match Purposes of Facilities |
|---|---|---|---|---|---|
| Fatigue | 532 | NS | NS | 0.005 | NS |
| Headache | 266 | 0.035 | NS | 0.002 | NS |
| Concentration difficulties | 164 | 0.049 | NS | 0.005 | NS |
| Irritation of the eyes | 559 | 0.014 | NS | 0.006 | NS |
| Irritation of the nose | 656 | 0.003 | NS | 0.001 | NS |
| Hoarse, dry throat | 475 | 0.001 | NS | 0.001 | 0.025 |
| Coughing | 225 | 0.016 | NS | 0.022 | NS |
| Coughing at night | 50 | 0.008 | NS | NS | NS |
| Irritation of skin on face | 373 | NS | NS | NS | NS |
| Irritation of skin on hands | 508 | 0.035 | NS | 0.003 | NS |
| Shortness of breath | 64 | 0.045 | NS | NS | NS |
| Wheezing | 32 | 0.001 | NS | NS | 0.044 |
| Fever or chills | 42 | NS | NS | NS | NS |
| Muscular pain | 160 | 0.027 | NS | 0.003 | NS |
| Joint pain | 193 | 0.039 | NS | NS | NS |
| Other work environment-related symptoms | 75 | 0.005 | NS | 0.001 | 0.027 |
| Estimated Duration of IAQ Problems: Number of Cases | Unlikely (n = 2) | Possible (n = 16) | Likely (n = 18) | Very Likely (n = 4) |
|---|---|---|---|---|
| No IAQ problems | 1 | 7 | 6 | 0 |
| Duration of IAQ problems less than a year | 0 | 2 | 4 | 0 |
| Duration of IAQ problems one year or more | 1 | 7 | 8 | 4 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tähtinen, K.; Lappalainen, S.; Karvala, K.; Lahtinen, M.; Salonen, H. Probability of Abnormal Indoor Air Exposure Categories Compared with Occupants’ Symptoms, Health Information, and Psychosocial Work Environment. Appl. Sci. 2019, 9, 99. https://doi.org/10.3390/app9010099
Tähtinen K, Lappalainen S, Karvala K, Lahtinen M, Salonen H. Probability of Abnormal Indoor Air Exposure Categories Compared with Occupants’ Symptoms, Health Information, and Psychosocial Work Environment. Applied Sciences. 2019; 9(1):99. https://doi.org/10.3390/app9010099
Chicago/Turabian StyleTähtinen, Katja, Sanna Lappalainen, Kirsi Karvala, Marjaana Lahtinen, and Heidi Salonen. 2019. "Probability of Abnormal Indoor Air Exposure Categories Compared with Occupants’ Symptoms, Health Information, and Psychosocial Work Environment" Applied Sciences 9, no. 1: 99. https://doi.org/10.3390/app9010099