1. Introduction
Creating an access cavity to reach the complex root canal anatomy is the first important step in non-surgical endodontic procedures. Obtaining information about the complex composition of the root canal system is imperative to comply with the principles to be followed during traditional and conservative access cavity preparation and to find solutions to the problems encountered [
1]. The main goal of endodontic procedures is to adequately shape, clean, and obturate the root canal system to prevent apical periodontitis [
2].
Recently, different designs of minimally invasive root canal access cavities have been proposed to remove as little tissue as possible to achieve the goal of root canal treatment. The goal of this concept is to increase the resistance of the tooth to cracks and fractures after root canal treatment by maximally preserving the healthy structure of the tooth during the preparation of the access cavity [
3]. However, the smaller the access cavity, the more difficult the visibility and disinfection of the root canal system become, and the more difficult it can be to find, shape, clean, and obturate the root canals. At the same time, poor visibility because of the small access cavity may increase the risk of iatrogenic complications, which may affect treatment outcomes [
4].
Lately, technological developments have brought innovations in the field of endodontics, such as new-generation rotary systems, magnification and lighting systems, and cone beam computed tomography (CBCT), that provide clinicians convenience during treatment. Using these technologies allows endodontic procedures to preserve healthy dental tissues more and prevent the loss of teeth [
5].
Traditional access cavity (TAC) preparation aims to provide direct access to the root canal system. Direct access helps to increase biomechanical efficiency and prohibits errors that may occur in various treatment stages [
6]. In contrast, dental tissue removed during TAC preparation can reduce the resistance of teeth to fracture under occlusal forces [
7,
8]. Current developments recommend choosing the access cavity design that preserves more dentin and brings the endodontic-restorative relationship to an ideal state in terms of the preservation of tooth structure [
9].
One of the most common causes of root canal treatment failure is reported to be the significant loss of dental tissue due to untreated caries and fractures of endodontically treated teeth [
10]; this is also directly related to the amount of tissue lost and specific cavity configurations [
11].
Conservative access cavity (CAC) preparation requires a dynamic approach that follows a conservative dental tissue removal procedure from the beginning of the procedure, which is expanded until adequate vision is achieved, rather than a predetermined access cavity form. This approach involves partial roof removal of the pulp chamber to protect the pulp horns, accompanied by cavity walls that are slightly concave and beveled towards the occlusal surface. This design aims to visualize the floor of the pulp chamber and all root canal openings from different angles [
12], which means that clinicians can visualize the pulp chamber and floor by changing the angle of the mirror, though not at the same angle [
13].
The minimally invasive endodontic concept, in addition to the differences in the access cavity, uses endodontic files with smaller tapers and innovative designs that aim to minimize the removal of tooth tissue [
14].
Two different Ni–Ti instrument systems were used in this study. The first is One Reci (OR) (MicroMega, Besançon, France). This file is a recently released single-file system that works with a reciprocating motion. OR files undergo a heat treatment (C-wire) aimed at increasing the instrument’s flexibility and ability of the file to stay at the center of the canal. Its variable off-center section, which begins as a triple helix and gradually turns into an S-shape towards the body, together with a deep groove, provides more space for debris removal in the coronal direction, giving it good cutting efficiency. This system completes the cutting action by rotating 170° counterclockwise and 60° clockwise [
15]. The files of this system consist of 20.04, 25.04, 25.06, 35.04 and 45.04. The other file system used in this study is ProTaper Ultimate (PU) (Dentsply Sirona, 2021). The ProTaper rotary file system was introduced in 2001, evolved into ProTaper Universal (PTU) in 2006, and then progressed to ProTaper Gold (PTG) in 2014. The ProTaper system is known for its ability to precisely prepare both anatomically complex and simple canals while offering a simple workflow. PU by Dentsply Sirona is a more advanced version of PTU and PTG and has a similar working principle as previous ProTaper generations. The manufacturer claims that PU offers additional advantages by showing increased elasticity and greater resistance to cyclic fatigue. According to the manufacturer’s instructions, the files of this system should be used at a constant speed of 400 rpm and with torque values of 4–5.2 Ncm. In this system, SX(020.003v), S1(016.002v), S2(020.004v), F1(020.007v), F2(025.008v), F3(030.009v), FX(035.012v), FXL(050.010v) files are available. SX, FX, and FXL files are auxiliary files in this system and were not used in this study [
16].
This study aims to compare the shaping efficiency of the One Reci and ProTaper Ultimate Ni–Ti instrument systems using micro-CT in traditional and conservative endodontic access cavities approached in extracted mandibular molar teeth. In this respect, the study is novel due to the comparison of two different endodontic access cavities with two different Ni–Ti systems.
2. Materials and Methods
2.1. Sample Size Determination and Power Calculation
After ethics committee approval (protocol no. 18/02), the sample size was estimated based on studies that compared TACs and CACs [
17,
18]. Fixed effects one-way ANOVA was selected from the F tests family and ran in G*Power 3.1 software (Henrick Heine-Universität, Düsseldorf, Germany). Accordingly, for an analysis with α = 0.05 and 80% power, at least 10 teeth were allocated for each of the experimental groups as the ideal size required to observe significant differences. A total of 60 extracted mandibular molar teeth were selected for the experiments, and 15 samples/groups were used to compensate for possible sample loss.
2.2. Sample Selection
Sample selection was carried out with a dental operation microscope (Leica M320, Wetzlar, Germany) under 10× magnification. The first and second mandibular molar teeth were included in this study. The teeth were extracted due to periodontal diseases. Teeth with fractures, cracks, and caries on the root surface in the examination were excluded from the study. Additionally, teeth with root canal curvatures of more than 35° according to the Schilder technique were not included in the study. To ensure standardization in all samples, the root canal curvature was selected to be less than 35°. After the samples were kept in 2.5% NaOCl for 24 h, hard and soft tissue residues on the root surfaces were removed with the help of a periodontal curette. The teeth were numbered according to the study groups and stored at 4 °C and in 0.1% thymol solution until the experiment.
2.3. Micro-CT Scans
To conduct the first micro-CT scan before access cavity and root canal preparation, the samples were fixed on the turntable of the micro-CT device and scanned with the X-ray source of the device at 80 kVp, 125 mA, 26.7 μm pixel size, and 0.2 rotation. The images obtained after the scan were transferred to the NRecon software (ver. 1.6.10.4, Bruker X-ray, Kontich, Belgium). A total of 1800 two-dimensional sections were obtained from each sample. For the reconstruction, the ring artifact correction was fixed to 7, and the smoothing parameter was set to 3. The beam hardening artifact correction was set to 38%. Contrast settings were kept between 0 and 0.05 for all the samples. Examples of images obtained from micro-CT scanning before cavity and root canal preparation are given in
Figure 1.
Figure 1 shows the results of the first micro-CT scan. In this scan, teeth were examined regarding fractures, cracks, caries, and radii of curvature to avoid missing possible errors in the dental operating microscope. Samples from micro-CT scanning were placed in silicone molds (Express XT, 3M ESPE, Neuss, Germany) with root tips visible to stabilize and isolate them from the environment during access cavity preparation. The experimental groups were formed according to the type of access cavity and the Ni–Ti file system to be used, as shown in
Figure 2.
Figure 2 shows the four groups and the study design. Two different micro-CT scans were carried out for the control and analysis of all groups. The samples used in the study were randomly assigned to four main groups (
n = 15). Of the randomly selected teeth, the groups were as follows: Group 1 included traditional access cavity and root canal preparation using One Reci(TAC-OR) (
n = 15); Group 2 included traditional access cavity and root canal preparation using ProTaper Ultimate (TAC-PU) (
n = 15); group 3 included conservative access cavity and root canal preparation using One Reci (CAC-OR) (
n = 15); and Group 4 included conservative access cavity and root canal preparation using ProTaper Ultimate (CAC-PU) (
n = 15). All specimens were removed from the silicone molds after cavity and root canal preparations and placed in the holder platform of the micro-CT. The second scans were repeated with the same parameters used in the first scans.
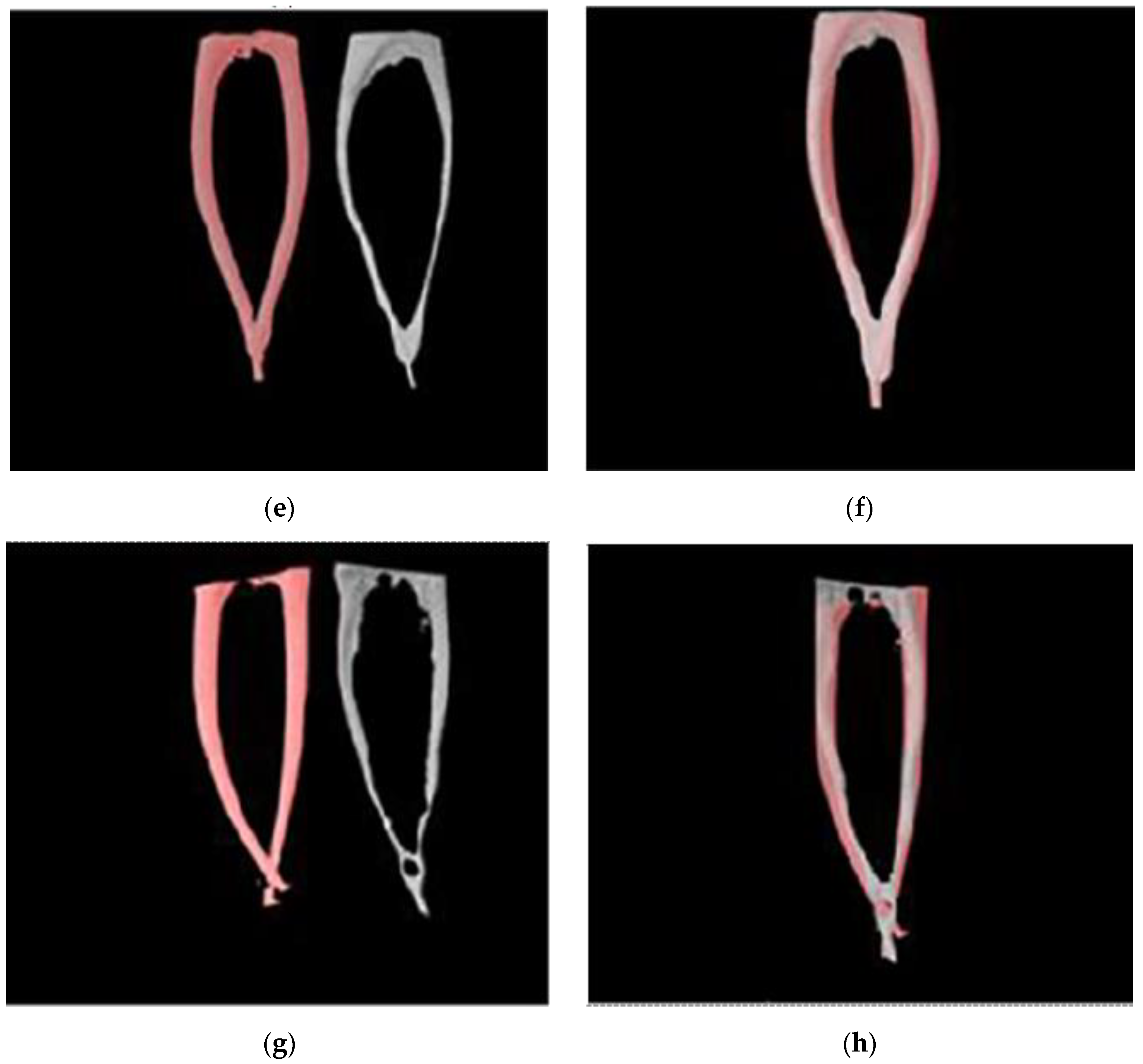
Figure 3 shows examples of images obtained after the second scan.
The images obtained after micro-CT scanning of traditional and conservative access cavities are shown in
Figure 3.
Figure 3 shows the differences between the access cavities of the two different methods.
2.4. Specimen Preparation
Access cavity preparations were made with a dental operating microscope (Leica M320, Wetzlar, Germany) under 6.4× magnification. Following the principles for traditional access cavities [
19], the specimens in Group 1 and Group 2 were accessed from the central fossa with a number 14 diamond round bur. The cavity walls were then paralleled with a number 12 diamond fissure bar to allow direct access of files to the coronal third of the canal.
Conservative access cavity preparation was performed following the principles previously described in the studies of Clark and Khademi [
13]. Cavity preparation of the specimens in Group 3 and Group 4 was started slightly mesial to the central fossa using the number 12 diamond round bur. The cavity walls were made slightly parallel with the diamond fissure burr numbered 11. Organic tissue residues and calcifications in the pulp chamber were removed with the help of ultrasonic tips.
After the cavity preparations of all specimens, to determine the working length in the mesio-buccal and mesio-lingual canals, a #10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) was inserted and advanced until it could be visible through the apical foramen. By measuring this length and subtracting 1 mm from that, the working length was determined for each canal and recorded. Then, the canal preparation process was carried out using an endodontic motor (Changzhou Eighteenth Medical Technology Co., Ltd., Changzhou, China). According to the determined working lengths of the samples belonging to Group 1 and Group 3, a glide path was created with a One G file (MicroMega, Besançon, France) using 300 rpm speed and 1.2 Ncm torque value. Each canal was then rinsed using 2 mL of 2.5% NaOCl. After this step, the preparation was made according to the manufacturer’s instructions using the OR 25/06 file up to the working length with 170° counterclockwise and 60° clockwise motion.
In Group 2 and Group 4, the samples were prepared using PU according to the manufacturer’s instructions with S1 and S2 files and F1 and F2 files, respectively. During the preparation procedures, the root canals were rinsed with 2 mL of 2.5% NaOCl at each file. Final irrigation was carried out with 5 mL of distilled water. All these procedures were performed by a single operator.
2.5. Image Processing
Images before and after instrumentation were repositioned in all three planes of space using the DataViewer software (ver. 1.5.6.2; Bruker X-ray, Kontich, Belgium). These images were imported into CTAn software (ver. 1.20.3.0; Bruker X-ray, Kontich, Belgium) and DataViewer to calculate canal volume, surface area, non-instrumented area, transportation, STL model preparation, and the thickness of the dentin in the danger zone.
Changes in volume and surface area were determined by subtracting the values before and after instrumentation using the CTAn software. The software was used to determine the region of interest (ROI). Furthermore, by adjusting the values of brightness and opacity, it is possible to remove “unwanted” voxels before calculating the final volume of the pulp and the canal cavity. Therefore, the software allows to obtain the desired volume, and the changes in volume and surface area can be compared between pre- and post-instrumentation [
20]. CTVol software (ver. 2.3.2.0; Bruker X-ray, Kontich, Belgium) was used for the visualization of the STL models. The STL models were obtained with CTAn software by selecting the ROIs that include the root canals and adjusting the threshold to select the air in the canal for the preparation of the models.
The percentage of the non-instrumented area was calculated according to the study by Arias et al. [
20] calculated using CTAn software as the percentage of the number of static voxel surfaces to the total number of surface voxels from the fitted 3D model before and after root canal preparation.
Canal transportation, the shortest distances from the orifice to the root tip before and after instrumentation, were measured in the mesial and distal directions using the DataViewer software. Then, using these data, the amount of transportation was obtained for each canal with the formula
This formula was previously used in the study of Rover et al. [
18]. In this formula, m1 represents the shortest distance from the mesial border of the root to the non-instrumented mesial margin, m2 represents the shortest distance from the mesial border of the root to the mesial margin of the instrumented canal, d1 represents the shortest distance from the distal border of the root to the non-instrumented distal margin, and d2 represents the shortest distance from the distal border of the root to the distal margin of the instrumented canal.
A value for canal transportation equal to 0 means no transportation. If the transportation value is negative, it indicates transportation in the distal direction, and if it is positive, it indicates mesial transportation. In
Figure 4, images from the DataViewer software, where the measurement of the transportation amount is made, are displayed.
Figure 4 shows the measurement of the transportation. The transportation was measured using the Dataviewer software. In
Figure 4, red lines show the shortest distances between borders and margins.
To measure the thickness of dentin in the danger zone area after canal preparation, sections were created from the images obtained from DataViewer software. In these slices, the thickness of the canal wall was measured in the axial plane. To assess changes in dentin thickness, the shortest distance from the instrumented and non-instrumented canal inner wall to the corresponding outer wall of the canal was measured. Radii of curvature were measured for all the samples, and the mean value for this measurement was 6.52 ± 1.49 mm using the method from Schafer et al.’s study [
21]. All images were evaluated and measured by a single observer with 12 years of Micro-CT experience, and all measurements were made twice by the same observer.
2.6. Statistical Analysis
Statistical analyses were performed using SPSS software (ver. 20.0.1; SPSS Inc., Chicago, IL, USA). The normality of the data distribution was obtained by the Kolmogorov–Smirnov test, and its homogeneity was obtained by the Levene test. The data showed a normal distribution. Two-way analysis of ANOVA was used to statistically compare the means of the changes in the canal volume and surface area of the groups, as well as values for the danger zone, transportation, and non-instrumented area. Post hoc analyses were performed with Tukey and Bonferroni tests. In all analyses, p ≤ 0.05 was taken to indicate statistical significance.
3. Results
There was no statistically significant difference between the groups in terms of volume change after root canal preparation in the mesio-buccal and mesio-lingual canals (
p > 0.05). The use of OR or PU did not affect volume change (
p > 0.05).
Table 1 shows the values for volume change, surface area change, non-instrumented area change and danger zone change after canal preparation of the mesio-buccal and mesio-lingual canals.
There was no statistical difference between the groups in terms of changes in the surface area of the mesio-buccal and mesio-lingual canals after root canal preparation (
p > 0.05). The use of OR or PU did not affect the change in surface area (
p > 0.05).
Table 1 shows the values of the surface area change after root canal preparation of the mesio-buccal and mesio-lingual canals.
The non-instrumented area in the TAC-OR group was 11.82 ± 0.25% in the mesio-buccal canal and 11.69 ± 0.15% in the mesio-lingual canal, respectively, and in the TAC-PU group, values of 11.76 ± 0.17% in the mesio-buccal canal and 11.44 ± 0.18% in the mesio-lingual canal were found. In the CAC-OR group, the non-instrumented area in the mesio-buccal canal was 16.08 ± 0.46%, and in the mesio-lingual canal, this value was 16.76 ± 0.14%; in the CAC-PU group, the non-instrumented area in the mesio-buccal canal was 15.41 ± 0.31%, and this value in the mesio-lingual canal was 15.55 ± 0.08%. The percentage of non-instrumented areas post-instrumentation in the mesio-buccal and mesio-lingual canals between the groups and the percentage of non-instrumented areas was statistically higher in specimens with a CAC compared to TAC groups (
p < 0.05). The use of OR or PU did not affect the percentage of the non-instrumented area (
p > 0.05).
Table 1 shows the percentage values of the non-instrumented areas of the mesio-buccal and mesio-lingual canals post-instrumentation.
There was no statistical difference between the groups in terms of the thickness of the dentin in the danger zone after root canal preparation in the mesio-buccal and mesio-lingual canals (
p > 0.05). The use of OR or PU did not affect the thickness of the dentin in the danger zone (
p > 0.05).
Table 1 shows the numerical values of the thickness of dentin in the danger zone after root canal preparation of the mesio-buccal and mesio-lingual canals.
In
Figure 5, the STL images obtained by micro-CT pre- and post-instrumentation were presented to all groups in the study, as well as the images obtained by superimposing these images.
Regardless of the file system used, more canal transportation was observed in the CAC groups at a distance of 2 mm, 5 mm, and 8 mm from the apical region (
p < 0.05). The use of OR or PU did not affect canal transportation (
p > 0.05). In
Table 2, the mean transportation values of the mesio-buccal canals at a distance of 2 mm, 5 mm, and 8 mm from the apical region are given.
Table 2 shows statistically significant differences between the CAC and TAC groups without the effect of the PU and OR subgroups in terms of transportation in all measured distances from the apical region in the mesiobuccal canals.
In
Table 3, the mean transportation values at distances of 2 mm, 5 mm, and 8 mm from the apical region of the mesio-lingual canals are given.
Table 3 shows statistically significant differences between the CAC and TAC groups without the effect of the PU and OR subgroups in terms of transportation in all measured distances from the apical region in the mesiolingual canals.
4. Discussion
In endodontic procedures, minimally invasive access cavity approaches, minimally invasive instrumentation and shaping, activation and agitation of irrigation solutions with different methods, and pressureless canal filling methods are all used for minimally invasive treatment purposes [
22,
23]. Many studies in the literature have emphasized the importance of preserving healthy tooth structure, especially pericervical dentin, using conservative endodontic cavities [
13,
17,
24,
25]. In agreement with the results of this study, Volster et al. revealed that CAC preserved more healthy dentin and pericervical dentin in comparison with TAC after root canal preparation using Wave One Gold and TruNatomy files [
25]. Pericervical dentin is dentin located 4 mm coronal and 4 mm apical to the cementoenamel junction. Preservation of pericervical dentin, especially in the molar area, plays a critical role in the longstanding optimal functioning of the teeth [
24].
Ni–Ti instrument systems, which increase shaping efficiency and shorten the working time, have created a revolutionary change by raising endodontic treatments to a new level. Two different Ni–Ti systems were used in this study. Due to the findings of Bergmans et al. [
26], the files used in studies must have similar apical diameters and tapers to compare morpho-geometric changes after root canal preparation. Parallel to this, in the present study, root canal preparations with OR and PU were made by selecting files with 25 apical diameters and similar tapers. OR and PU are files that have been introduced to the market by manufacturers for minimally invasive root canal shaping purposes and were therefore used in this study.
At the time this manuscript was written, a single study on OR was found in the literature review. Kharouf et al. [
15] evaluated the amount of debris extruding apically after root canal preparation with OR in curved canals.
Today, reciprocation is presented as a safe and viable alternative to traditional continuous rotational motion. In addition, previous studies have reported that systems operating with reciprocal motion have a 0.13–0.26% lower incidence of fracture than systems with rotation [
27,
28]. On the other hand, there are two main topics for which the reciprocal movement is criticized. The first is that reciprocating instruments are more likely to promote the development or propagation of dentinal microcracks than conventional fully rotating rotary systems, while the other is likely to cause debris accumulation during preparation and the extrusion of debris from the apex [
29].
In the present study, no significant difference was found in terms of volume change in the samples as a result of the preparation made with OR and PU in teeth with traditional and conservative access cavities (
p > 0.05). According to this result, the type of access cavity does not have any effect on the volume change as in the study of Barbosa et al. [
30]. Rover et al. did not find any effect of traditional and conservative access cavities on volume change after canal preparation in a similar study on upper molars [
18]. According to these results, the nature of a cavity as a traditional or conservative access cavity does not affect the volume change in the root canals because of root canal preparation and agrees with the results obtained in this study.
No statistically significant difference was found among groups in terms of the change in surface area (
p > 0.05). From the perspective of the two different types of access cavities prepared, this result agrees with Dos Santos Miranda et al.’s results obtained by investigating the effects of traditional and ultraconservative access cavities on the shaping of mandibular central teeth [
31]. Additionally, Lima et al. evaluated the shaping efficiency of two different rotating and reciprocating files in traditional and ultraconservative cavities of mandibular molars. Similarly, no effect of different cavity types and files on the surface area change was found in this study either [
14]. As a result of root canal shaping with OR and PU, no effect of the Ni–Ti file system used was found on the surface area change regardless of endodontic access cavity type (
p > 0.05). The preparation was carried out by selecting files with similar apical diameters and similar tapers in both systems. Therefore, the morphological and geometrical changes in the root canals were similar.
A statistically significant difference was found between the groups in terms of non-instrumented area (
p <0.05). This difference arose independently of the Ni–Ti instrument system used. This result is in agreement with the results of the study obtained by Lima et al. [
14]. In a separate similar study, Krishan et al. emphasized that conservative access cavities remain more non-instrumented than traditional access cavities [
32]. The reason for this result may be that the files cannot provide a completely straight-line entrance to the root canals in CAC groups and touch more cavity and canal walls until they reach the apex. The Ni–Ti instrument system used in the aforementioned studies, similar to this study, did not affect the non-instrumented area.
Non-instrumented areas of the canal walls obtained by micro-CT analysis were observed, especially in the apical region and isthmus areas. However, these areas may contain pulp tissue, bacteria, and dentin residues. These data show that studies should continue to make irrigation and shaping protocols more effective [
33]. In a minimally invasive treatment, the amount of non-instrumented area should be disinfected using complementary cleaning methods, not by increasing the taper of the Ni–Ti instrument used [
34]. Thus, unnecessary dentin is not removed from the middle and coronal parts of the root canal, and the resistance of the endodontically treated teeth against root fractures is increased [
35]. The percentage of unprepared areas is significantly reduced with the increase in the instrumentation size from 25 to 40, regardless of the system used. However, this situation may conflict with minimally invasive treatment principles, and by utilization of a modern system with a regressive taper, pericervical dentin can be preserved without compromising it [
36].
One of the major points of mechanical damage as a result of excessive instrumentation in an already slim dentin wall under normal conditions is that it can lead to failure of root canal treatment [
37]. Abou-Rass et al. stated in their study that such damage may cause perforations in the middle section of the root. This section is known as the danger zone and is located in the distal area of the mesial roots of mandibular molars. Additionally, the safety zone was defined as the mesial area of the mesial root with a thicker dentin layer [
38]. The safety zone is usually minimally instrumented with endodontic instruments. In this study, no significant difference was found between the groups in terms of the thickness of the danger zone (
p > 0.05). This result is consistent with the results of Peng et al.’s study on the danger zone [
39]. In other words, these results demonstrate the reliability of both systems when preparing mesial root canals of mandibular molars because neither system excessively removed the dentin in the furcation area.
Canal transportation equals the deflection (in millimeters) of the root canal from its original axis after root canal preparation in comparison to before preparation [
40]. Wu et al. showed that canal transportation of >0.3 mm causes adverse effects on root canal obturation [
41]. In accordance with this, the canal transportation values obtained in all sections for all the groups in the present study were <0.3. In this study, canal transportation values were measured for all groups at distances of 2 mm, 5 mm, and 8 mm from the apical foramen. As a result of these measurements, a statistically significant difference was found among the groups in terms of canal transportation (
p < 0.05). According to these results, regardless of the Ni–Ti instrument system used, more transportation was observed in the CAC-OR and CAC-PU groups compared to the TAC-OR and TAC-PU groups at all levels where the canal transportation value was measured. This result was in line with Rover et al.’s study, which compared the effects of traditional and conservative access cavities on shaping efficiency and transportation values in upper molars [
18]. In another similar study, Lima et al. reported that access cavities with an ultraconservative approach in mandibular teeth cause more transportation than traditional cavities. The reason for obtaining these results is due to the presence of coronal interferences of access cavities with conservative and ultraconservative approaches, which causes the instruments to not provide a straight entry into the canals and results in an uneven force distribution [
17,
42]. In contrast, in Peng et al.’s study on the shaping efficiency of traditional and conservative access cavities and the preservation of dentin tissue in mandibular and upper molar teeth, no significant difference was found in terms of transportation post-instrumentation with WaveOne Gold in the two different access cavities evaluated [
39]. Additionally, Kadhim et al. revealed that transportation and centering ability were not statistically affected by traditional versus conservative access cavities [
43].
For conservative access cavities, the use of 3D imaging technology, an operating microscope, a good light source and illumination, ultrasonic tips, irrigation activation methods, and the use of new-generation Ni–Ti rotary instrument systems were found to minimize the negative effects on clinical procedures related to root canal treatment.
Within the limitations of this in vitro study, the effects of TACs and CACs on the shaping efficiencies of two different Ni–Ti instrument systems were evaluated using micro-CT. In this regard, future experiments should be encouraged with larger sample sizes, the use of irrigation activation methods, the incorporation of different shaping tools with fewer expansion angles, and over long-term clinical studies.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}