
Influence of Thermal and Mechanical Load Cycling on Fracture Resistance of Premolars Filled with Calcium Silicate Sealer

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size
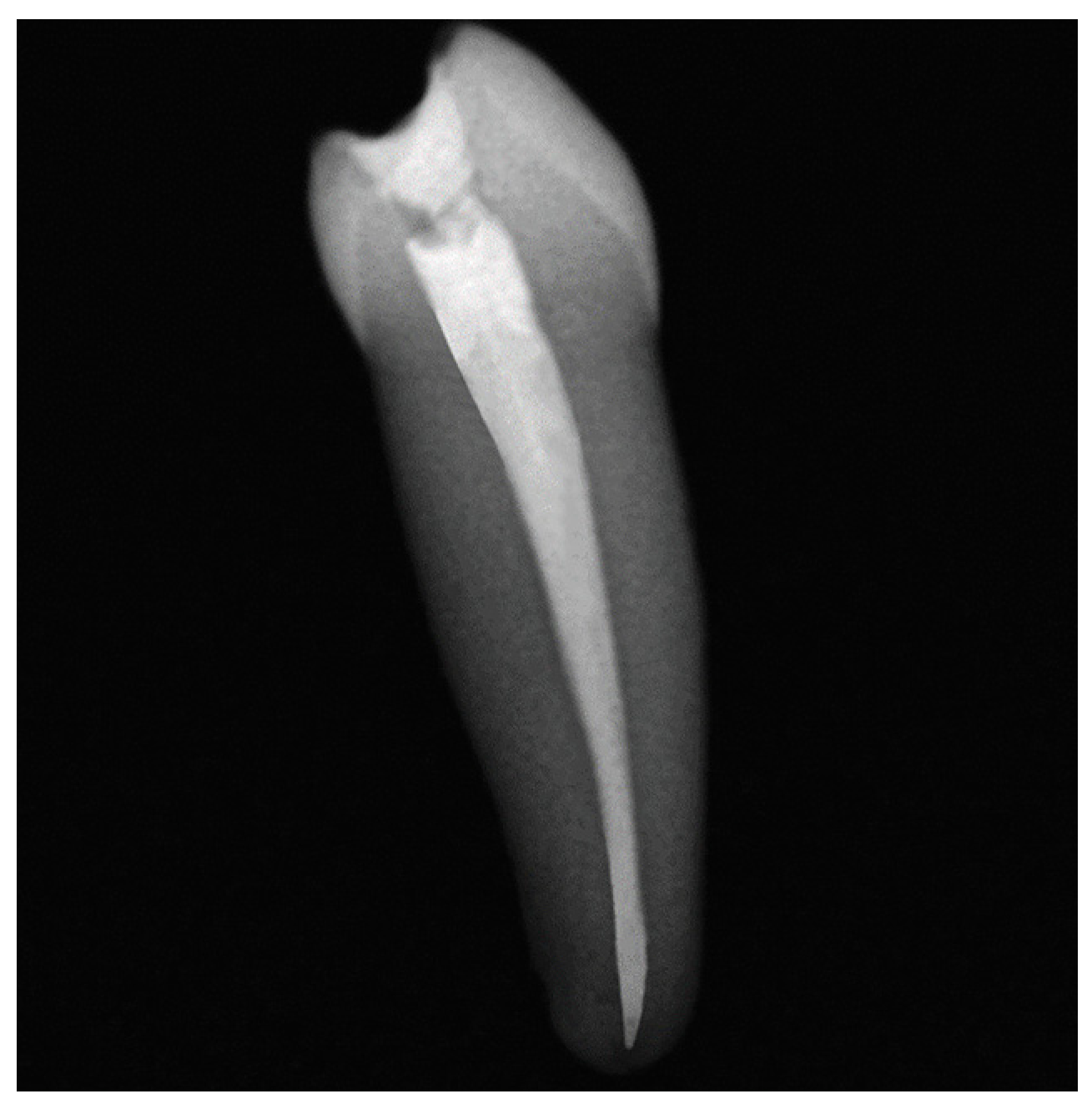
2.2. Specimen Preparation
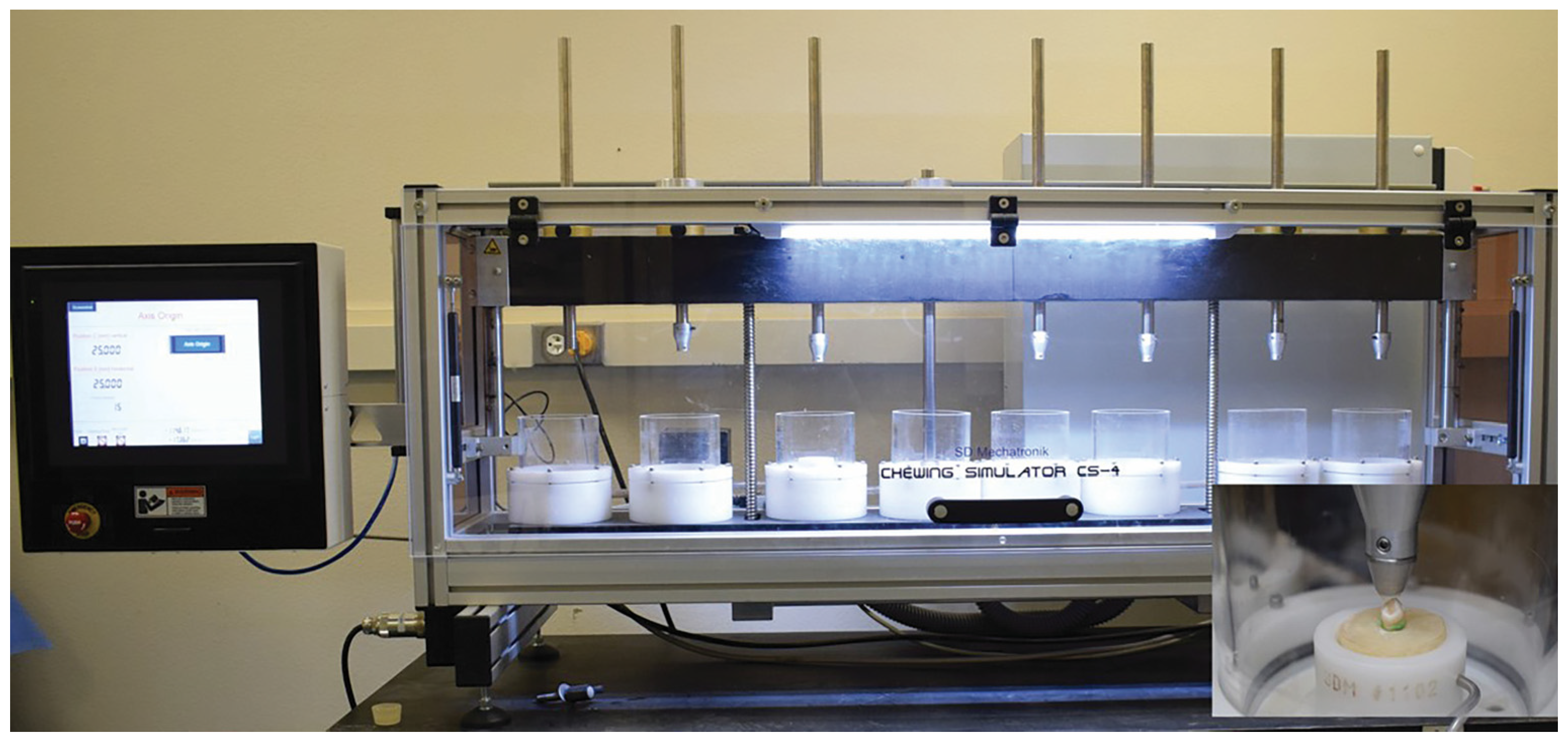
2.3. Thermomechanical Cycling
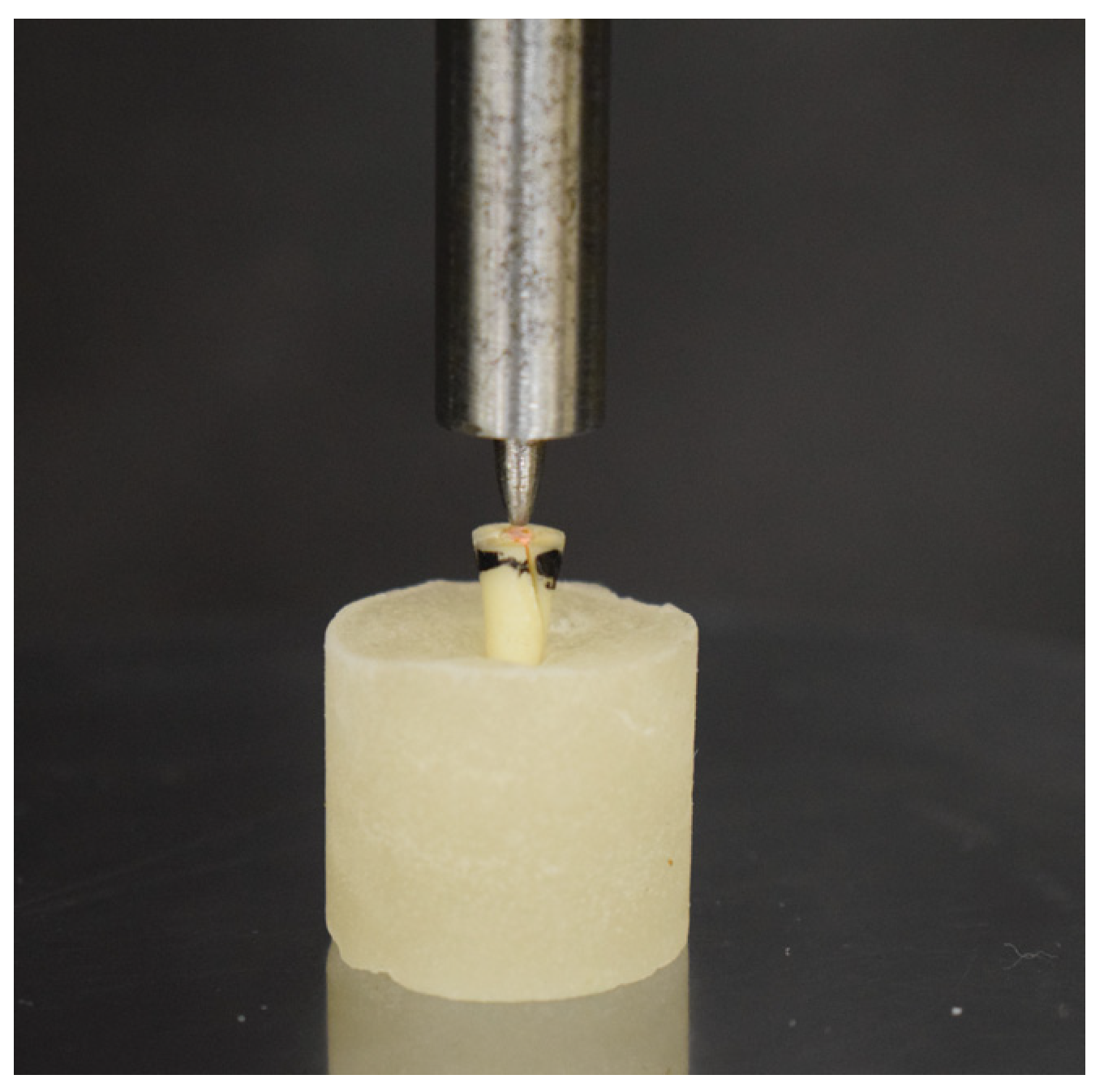
2.4. Fracture Test
2.5. Statistical Analysis
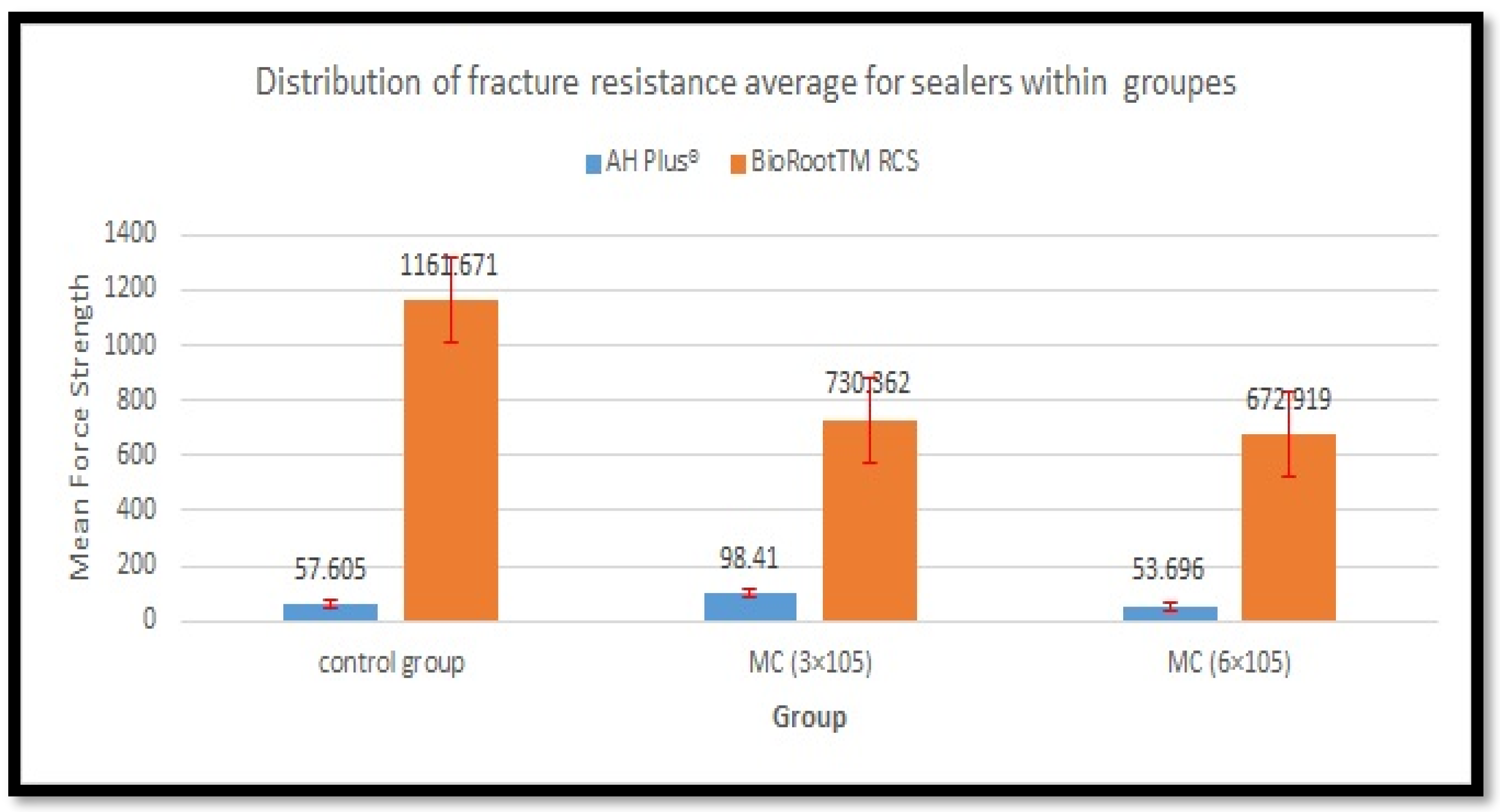
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Uzunoglu, E.; Aktemur, S.; Uyanik, M.O.; Durmaz, V.; Nagas, E. Effect of Ethylenediaminetetraacetic Acid on Root Fracture with Respect to Concentration at Different Time Exposures. J. Endod. 2012, 38, 1110–1113. [Google Scholar] [CrossRef]
- Al-Omiri, M.K.; Mahmoud, A.A.; Rayyan, M.R.; Abu-Hammad, O. Fracture Resistance of Teeth Restored with Post-Retained Restorations: An Overview. J. Endod. 2010, 36, 1439–1449. [Google Scholar] [CrossRef]
- Mikrogeorgis, G.; Eirinaki, E.; Kapralos, V.; Koutroulis, A.; Lyroudia, K.; Pitas, I. Diagnosis of Vertical Root Fractures in Endodontically Treated Teeth Utilising Digital Subtraction Radiography: A Case Series Report. Aust. Endod. J. 2018, 44, 286–291. [Google Scholar] [CrossRef]
- Seo, D.-G.; Yi, Y.-A.; Shin, S.-J.; Park, J.-W. Analysis of Factors Associated with Cracked Teeth. J. Endod. 2012, 38, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, K.; Ito, K.; Kuroda, M.; Sugihara, N. Prevalence of Vertical Root Fracture as the Reason for Tooth Extraction in Dental Clinics. Clin. Oral Investig. 2015, 19, 1405–1409. [Google Scholar] [CrossRef]
- Almasri, M. Assessment of Extracting Molars and Premolars after Root Canal Treatment: A Retrospective Study. Saudi Dent. J. 2019, 31, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Lertchirakarn, V.; Palamara, J.E.; Messer, H.H. Patterns of Vertical Root Fracture: Factors Affecting Stress Distribution in the Root Canal. J. Endod. 2003, 29, 523–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghoddusi, J.; Bagherpour, A.; Mahmudabadi, F.; Forghani, M.; Sarmad, M. Residual Dentin Thickness of Bifurcated Maxillary Premolars Following Two Post Space Preparation Methods. Iran. Endod. J. 2013, 8, 94. [Google Scholar]
- Johnson, M.E.; Stewart, G.P.; Nielsen, C.J.; Hatton, J.F. Evaluation of Root Reinforcement of Endodontically Treated Teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2000, 90, 360–364. [Google Scholar] [CrossRef]
- Gulsahi, K.; Cehreli, Z.; Kuraner, T.; Dagli, F. Sealer Area Associated with Cold Lateral Condensation of Gutta-percha and Warm Coated Carrier Filling Systems in Canals Prepared with Various Rotary NiTi Systems. Int. Endod. J. 2007, 40, 275–281. [Google Scholar] [CrossRef]
- Ribeiro, F.C.; Souza-Gabriel, A.E.; Marchesan, M.A.; Alfredo, E.; Silva-Sousa, Y.T.C.; Sousa-Neto, M.D. Influence of Different Endodontic Filling Materials on Root Fracture Susceptibility. J. Dent. 2008, 36, 69–73. [Google Scholar] [CrossRef]
- Lin, G.S.S.; Ghani, N.R.N.A.; Noorani, T.Y.; Kamarudin, A. Apical Sealing Ability of Different Endodontic Sealers Using Glucose Penetration Test: A Standardized Methodological Approach. Cumhur. Dent. J. 2020, 23, 79–87. [Google Scholar] [CrossRef]
- Lee, S.-J.; Monsef, M.; Torabinejad, M. Sealing Ability of a Mineral Trioxide Aggregate for Repair of Lateral Root Perforations. J. Endod. 1993, 19, 541–544. [Google Scholar] [CrossRef]
- Neelakantan, P.; Subbarao, C.; Subbarao, C.V.; De-Deus, G.; Zehnder, M. The Impact of Root Dentine Conditioning on Sealing Ability and Push-out Bond Strength of an Epoxy Resin Root Canal Sealer. Int. Endod. J. 2011, 44, 491–498. [Google Scholar] [CrossRef] [Green Version]
- Hergt, A.; Wiegand, A.; Hülsmann, M.; Rödig, T. AH Plus Root Canal Sealer–an Updated Literature. Endod. Pract. Today 2015, 9, 245–265. [Google Scholar]
- McMichen, F.; Pearson, G.; Rahbaran, S.; Gulabivala, K. A Comparative Study of Selected Physical Properties of Five Root-canal Sealers. Int. Endod. J. 2003, 36, 629–635. [Google Scholar] [CrossRef]
- Azar, N.G.; Heidari, M.; Bahrami, Z.S.; Shokri, F. In Vitro Cytotoxicity of a New Epoxy Resin Root Canal Sealer. J. Endod. 2000, 26, 462–465. [Google Scholar] [CrossRef] [PubMed]
- Antunovic, M.; Vukmanovic, L.; Budimir, A.; Kabil, E.; Anic, I.; Bago, I. Evaluation of Sealing Ability of Four Bioceramic Root Canal Sealers and an Epoxy Resin-Based Sealer: An in Vitro Study. Saudi Endod. J. 2021, 11, 66. [Google Scholar]
- Prüllage, R.-K.; Urban, K.; Schäfer, E.; Dammaschke, T. Material Properties of a Tricalcium Silicate–Containing, a Mineral Trioxide Aggregate–Containing, and an Epoxy Resin–Based Root Canal Sealer. J. Endod. 2016, 42, 1784–1788. [Google Scholar] [CrossRef]
- Guneser, M.B.; Akman, M.; Kolcu, İ.B.; Eldeniz, A.U. Fracture Resistance of Roots Obturated with a Novel Calcium Silicate-Based Endodontic Sealer (BioRoot RCS). J. Adhes. Sci. Technol. 2016, 30, 2420–2428. [Google Scholar] [CrossRef]
- Siboni, F.; Taddei, P.; Zamparini, F.; Prati, C.; Gandolfi, M.G. Properties of BioRoot RCS, a Tricalcium Silicate Endodontic Sealer Modified with Povidone and Polycarboxylate. Int. Endod. J. 2017, 50, e120–e136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, D.-G.; Lee, D.; Kim, Y.-M.; Song, D.; Kim, S.-Y. Biocompatibility and Mineralization Activity of Three Calcium Silicate-Based Root Canal Sealers Compared to Conventional Resin-Based Sealer in Human Dental Pulp Stem Cells. Materials 2019, 12, 2482. [Google Scholar] [CrossRef] [Green Version]
- Sterzenbach, G.; Rosentritt, M.; Frankenberger, R.; Paris, S.; Naumann, M. Loading Standardization of Postendodontic Restorations in Vitro: Impact of Restorative Stage, Static Loading, and Dynamic Loading. Oper. Dent. 2012, 37, 71–79. [Google Scholar] [CrossRef] [Green Version]
- Ou, K.; Chang, C.; Chang, W.; Lin, C.; Chang, K.; Huang, H. Effect of Damping Properties on Fracture Resistance of Root Filled Premolar Teeth: A Dynamic Finite Element Analysis. Int. Endod. J. 2009, 42, 694–704. [Google Scholar] [CrossRef] [PubMed]
- Att, W.; Kurun, S.; Gerds, T.; Strub, J.R. Fracture Resistance of Single-Tooth Implant-Supported All-Ceramic Restorations: An in Vitro Study. J. Prosthet. Dent. 2006, 95, 111–116. [Google Scholar] [CrossRef]
- Baldissara, P.; Zicari, F.; Valandro, L.F.; Scotti, R. Effect of Root Canal Treatments on Quartz Fiber Posts Bonding to Root Dentin. J. Endod. 2006, 32, 985–988. [Google Scholar] [CrossRef]
- Habib, S.R.; Alotaibi, A.; Al Hazza, N.; Allam, Y.; AlGhazi, M. Two-Body Wear Behavior of Human Enamel versus Monolithic Zirconia, Lithium Disilicate, Ceramometal and Composite Resin. J. Adv. Prosthodont. 2019, 11, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Tay, F.R.; Loushine, R.J.; Monticelli, F.; Weller, R.N.; Breschi, L.; Ferrari, M.; Pashley, D.H. Effectiveness of Resin-Coated Gutta-Percha Cones and a Dual-Cured, Hydrophilic Methacrylate Resin-Based Sealer in Obturating Root Canals. J. Endod. 2005, 31, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Lam, P.P.; Palamara, J.E.; Messer, H.H. Fracture Strength of Tooth Roots Following Canal Preparation by Hand and Rotary Instrumentation. J. Endod. 2005, 31, 529–532. [Google Scholar] [CrossRef] [PubMed]
- Trope, M.; Ray Jr, H.L. Resistance to Fracture of Endodontically Treated Roots. Oral Surg. Oral Med. Oral Pathol. 1992, 73, 99–102. [Google Scholar] [CrossRef]
- Demiriz, L.; Bodrumlu, E.H. Fracture Resistance of Simulated Incomplete Vertical Fractured Teeth Treated with Different Bioceramic Based Root Canal Sealers. Int. J. Appl. Dent. Sci. 2018, 4, 25–30. [Google Scholar]
- Arola, D. Fatigue Testing of Biomaterials and Their Interfaces. Dent. Mater. 2017, 33, 367–381. [Google Scholar] [CrossRef]
- da Silva, G.R.; da Silva, N.R.; Soares, P.V.; Costa, A.R.; Fernandes-Neto, A.J.; Soares, C.J. Influence of Different Load Application Devices on Fracture Resistance of Restored Premolars. Braz. Dent. J. 2012, 23, 484–489. [Google Scholar] [CrossRef] [Green Version]
- Georgiev, Z.; Kovacevska, I.; Sotirovska-Ivkovska, A.; Zabokova-Bilbilova, E.; Dimova, C. Methods of Deciduous Dental Pulp Research. Int. Dent. J. 2013, 63, 151–153. [Google Scholar]
- Lima, V.P.; Machado, J.B.; Zhang, Y.; Loomans, B.A.; Moraes, R.R. Laboratory Methods to Simulate the Mechanical Degradation of Resin Composite Restorations. Dent. Mater. 2022, 38, 214–229. [Google Scholar] [CrossRef]
- Nawafleh, N.; Hatamleh, M.; Elshiyab, S.; Mack, F. Lithium Disilicate Restorations Fatigue Testing Parameters: A Systematic Review. J. Prosthodont. 2016, 25, 116–126. [Google Scholar] [CrossRef]
- Yusufoglu, S.İ.; Akman, M.; Akbulut, M.B.; Eldeniz, A.Ü. Fracture Resistance of Roots Enlarged with Various Rotary Systems and Obturated with Different Sealers. J. Dent. Res. Dent. Clin. Dent. Prospect. 2019, 13, 215. [Google Scholar] [CrossRef] [Green Version]
- Viapiana, R.; Moinzadeh, A.T.; Camilleri, L.; Wesselink, P.R.; Tanomaru Filho, M.; Camilleri, J. Porosity and Sealing Ability of Root Fillings with Gutta-percha and BioRoot RCS or AH Plus Sealers. Evaluation by Three Ex Vivo Methods. Int. Endod. J. 2016, 49, 774–782. [Google Scholar] [CrossRef]
- Al-Hiyasat, A.S.; Alfirjani, S.A. The Effect of Obturation Techniques on the Push-out Bond Strength of a Premixed Bioceramic Root Canal Sealer. J. Dent. 2019, 89, 103169. [Google Scholar] [CrossRef]
- Moinzadeh, A.T.; Zerbst, W.; Boutsioukis, C.; Shemesh, H.; Zaslansky, P. Porosity Distribution in Root Canals Filled with Gutta Percha and Calcium Silicate Cement. Dent. Mater. 2015, 31, 1100–1108. [Google Scholar] [CrossRef]
- Pişkin, B.; Aydın, B.; Sarıkanat, M. The Effect of Spreader Size on Fracture Resistance of Maxillary Incisor Roots. Int. Endod. J. 2008, 41, 54–59. [Google Scholar] [CrossRef]
- Özyürek, T.; Ülker, Ö.; Demiryürek, E.Ö.; Yılmaz, F. The Effects of Endodontic Access Cavity Preparation Design on the Fracture Strength of Endodontically Treated Teeth: Traditional versus Conservative Preparation. J. Endod. 2018, 44, 800–805. [Google Scholar] [CrossRef]
- Sagsen, B.; Er, O.; Kahraman, Y.; Akdogan, G. Resistance to Fracture of Roots Filled with Three Different Techniques. Int. Endod. J. 2007, 40, 31–35. [Google Scholar] [CrossRef]
- Bonessio, N.; Arias, A.; Lomiento, G.; Peters, O.A. Effect of Root Canal Treatment Procedures with a Novel Rotary Nickel Titanium Instrument (TRUShape) on Stress in Mandibular Molars: A Comparative Finite Element Analysis. Odontology 2017, 105, 54–61. [Google Scholar] [CrossRef]
- Xie, C.; Han, Y.; Zhao, X.-Y.; Wang, Z.-Y.; He, H.-M. Microtensile Bond Strength of One-and Two-Step Self-Etching Adhesives on Sclerotic Dentin: The Effects of Thermocycling. Oper. Dent. 2010, 35, 547–555. [Google Scholar] [CrossRef] [Green Version]
- Soros, C.; Zinelis, S.; Lambrianidis, T.; Palaghias, G. Spreader Load Required for Vertical Root Fracture during Lateral Compaction Ex Vivo: Evaluation of Periodontal Simulation and Fracture Load Information. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 106, e64–e70. [Google Scholar] [CrossRef]
- Ausiello, P.; Ciaramella, S.; Martorelli, M.; Lanzotti, A.; Zarone, F.; Watts, D.C.; Gloria, A. Mechanical Behavior of Endodontically Restored Canine Teeth: Effects of Ferrule, Post Material and Shape. Dent. Mater. 2017, 33, 1466–1472. [Google Scholar] [CrossRef] [Green Version]
- Rippe, M.P.; Santini, M.F.; Bier, C.A.S.; Borges, A.L.S.; Valandro, L.F. Root Canal Filling: Fracture Strength of Fiber-Reinforced Composite-Restored Roots and Finite Element Analysis. Braz. Dent. J. 2013, 24, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Ulusoy, Ö. Fracture Resistance of Roots with Simulated Internal Resorption Defects and Obturated Using Different Hybrid Techniques. J. Dent. Sci. 2017, 12, 121–125. [Google Scholar] [CrossRef] [Green Version]
- Nagpal, A.; Annapoorna, B.M.; Prashanth, M.B.; Prashanth, N.T.; Singla, M.; Deepak, B.S.; Singh, A.; Tavane, P.N. A Comparative Evaluation of the Vertical Root Fracture Resistance of Endodontically Treated Teeth Using Different Root Canal Sealers: An in Vitro Study. J. Contemp. Dent. Pract. 2012, 13, 351–355. [Google Scholar]
- Saba, A.A.; Al-Zaka, I.M. Fracture Resistance of Endodontically Treated Teeth Obturated with Different Root Canal Sealers (in Vitro Study). J. Contemp. Dent. Pract. 2019, 65, 1567–1575. [Google Scholar] [CrossRef] [Green Version]
- Osiri, S.; Banomyong, D.; Sattabanasuk, V.; Yanpiset, K. Root Reinforcement after Obturation with Calcium Silicate–Based Sealer and Modified Gutta-Percha Cone. J. Endod. 2018, 44, 1843–1848. [Google Scholar] [CrossRef] [PubMed]
- Khalil, I.; Naaman, A.; Camilleri, J. Properties of Tricalcium Silicate Sealers. J. Endod. 2016, 42, 1529–1535. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Li, Z.; Peng, B. Assessment of a New Root Canal Sealer’s Apical Sealing Ability. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, e79–e82. [Google Scholar] [CrossRef]
- Chakraborty, J.; Basu, D. Bioceramics—A New Era. Trans. Indian Ceram. Soc. 2005, 64, 171–192. [Google Scholar] [CrossRef]
- Duarte, M.A.H.; Marciano, M.A.; Vivan, R.R.; Tanomaru Filho, M.; Tanomaru, J.M.G.; Camilleri, J. Tricalcium Silicate-Based Cements: Properties and Modifications. Braz. Oral Res. 2018, 32, e70. [Google Scholar] [CrossRef] [Green Version]
- Cirstea, A.C.; Gheorghita, L.M.; Diaconu, O.A.; Bataiosu, M.; Georgescu, R.V.; Dascalu, I.T. Bioceramic-Based Root Canal Sealers: A Review. Rom. J. Oral Rehabil. 2020, 12, 48–54. [Google Scholar]
- Shetty, S.; Kahler, B. Alkaline Material Effects on Roots of Teeth. Materials 2017, 10, 1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resende, L.M.; Rached-Junior, F.J.A.; Versiani, M.A.; Souza-Gabriel, A.E.; Miranda, C.E.S.; Silva-Sousa, Y.T.C.; Sousa Neto, M.D. de A Comparative Study of Physicochemical Properties of AH Plus, Epiphany, and Epiphany SE Root Canal Sealers. Int. Endod. J. 2009, 42, 785–793. [Google Scholar] [CrossRef]
- Atmeh, A.R.; Chong, E.Z.; Richard, G.; Festy, F.; Watson, T.F. Dentin-Cement Interfacial Interaction: Calcium Silicates and Polyalkenoates. J. Dent. Res. 2012, 91, 454–459. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Manufacturers | Composition |
|---|---|---|
| AH Plus | Dentsply-De Trey, Constance, Germany | Paste A: diepoxide, calcium tungstate, zirconium oxide, aerosil, pigment (Fe oxide) |
| Paste B: 1-adamantane amine | ||
| BioRoot RCS | Septodont, St. Maur-des-Fossés, France | Powder: tricalcium silicate, zirconium oxide and povidone |
| Liquid: aqueous solution of calcium chloride and polycarboxylate |
| Sealer | Control Group | MC (3 × 105) | MC (6 × 105) | p-Value |
|---|---|---|---|---|
| AH Plus | 57.605 ± 15.207 A,a | 98.41 ± 19.335 A,b | 53.696 ± 24.082 A,a | 0.000 |
| BioRoot RCS | 1161.671 ± 214.948 B,a | 730.362 ± 133.296 B,b | 672.919 ± 131.109 B,b | 0.000 |
| T-test p-value | 0.000 | 0.000 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smran, A.; Abdullah, M.; Ahmad, N.A.; AL-Maflehi, N.; Samran, A. Influence of Thermal and Mechanical Load Cycling on Fracture Resistance of Premolars Filled with Calcium Silicate Sealer. Appl. Sci. 2023, 13, 4388. https://doi.org/10.3390/app13074388
Smran A, Abdullah M, Ahmad NA, AL-Maflehi N, Samran A. Influence of Thermal and Mechanical Load Cycling on Fracture Resistance of Premolars Filled with Calcium Silicate Sealer. Applied Sciences. 2023; 13(7):4388. https://doi.org/10.3390/app13074388
Chicago/Turabian StyleSmran, Ahlam, Mariam Abdullah, Norasmatul Akma Ahmad, Nassr AL-Maflehi, and Abdulaziz Samran. 2023. "Influence of Thermal and Mechanical Load Cycling on Fracture Resistance of Premolars Filled with Calcium Silicate Sealer" Applied Sciences 13, no. 7: 4388. https://doi.org/10.3390/app13074388