

Efficient Computer-Based Method for Adjusting the Stiffness of Subject-Specific 3D-Printed Insoles during Walking


Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Participant Information and Construction of the Insole
2.2. Gait Measurements
2.3. Musculoskeletal Multibody Model
2.4. Finite Element Modelling
2.4.1. Geometries
2.4.2. Material Properties
2.4.3. Mesh
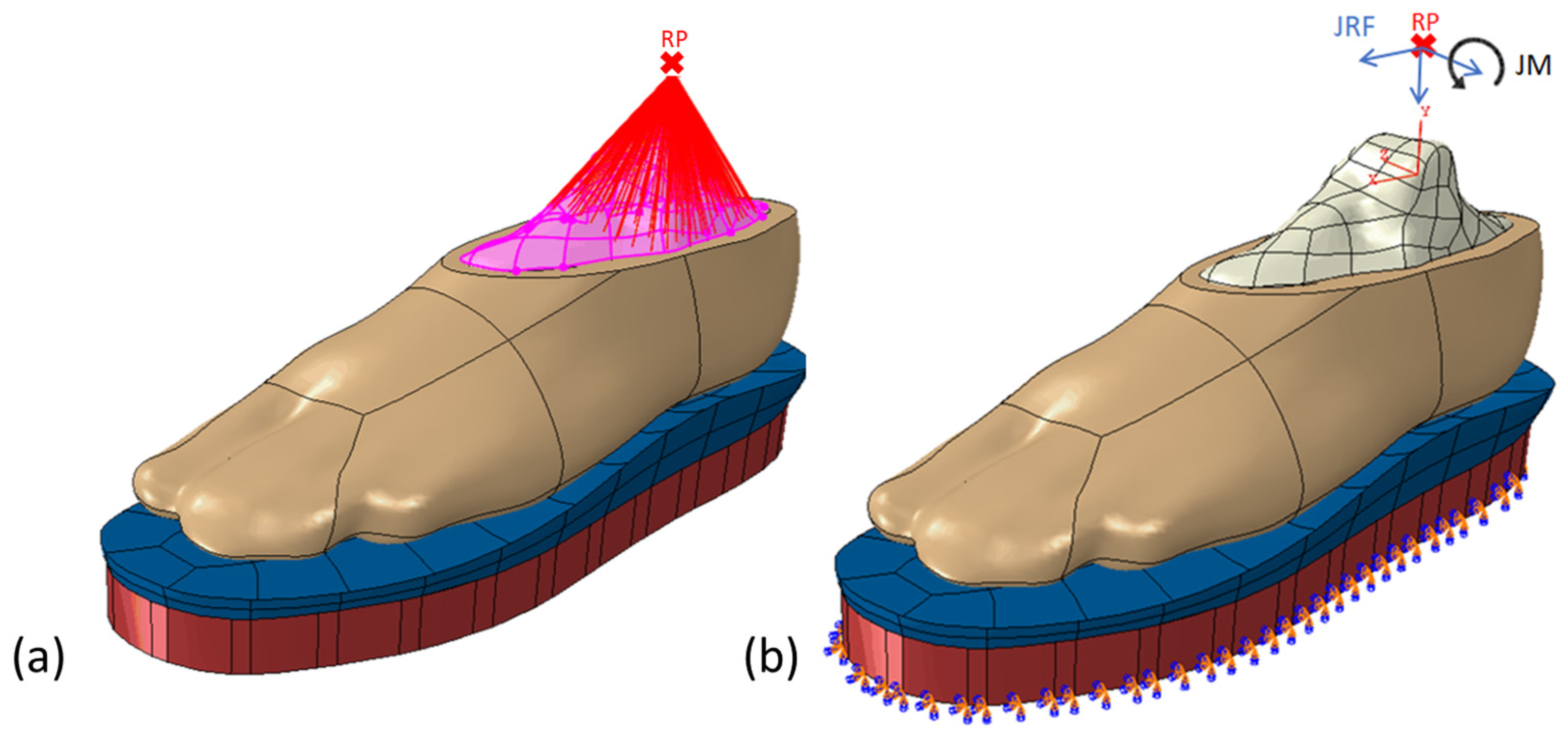
2.4.4. Boundary and Loading Condition
2.4.5. Validation
2.4.6. Parameter Analysis
3. Results
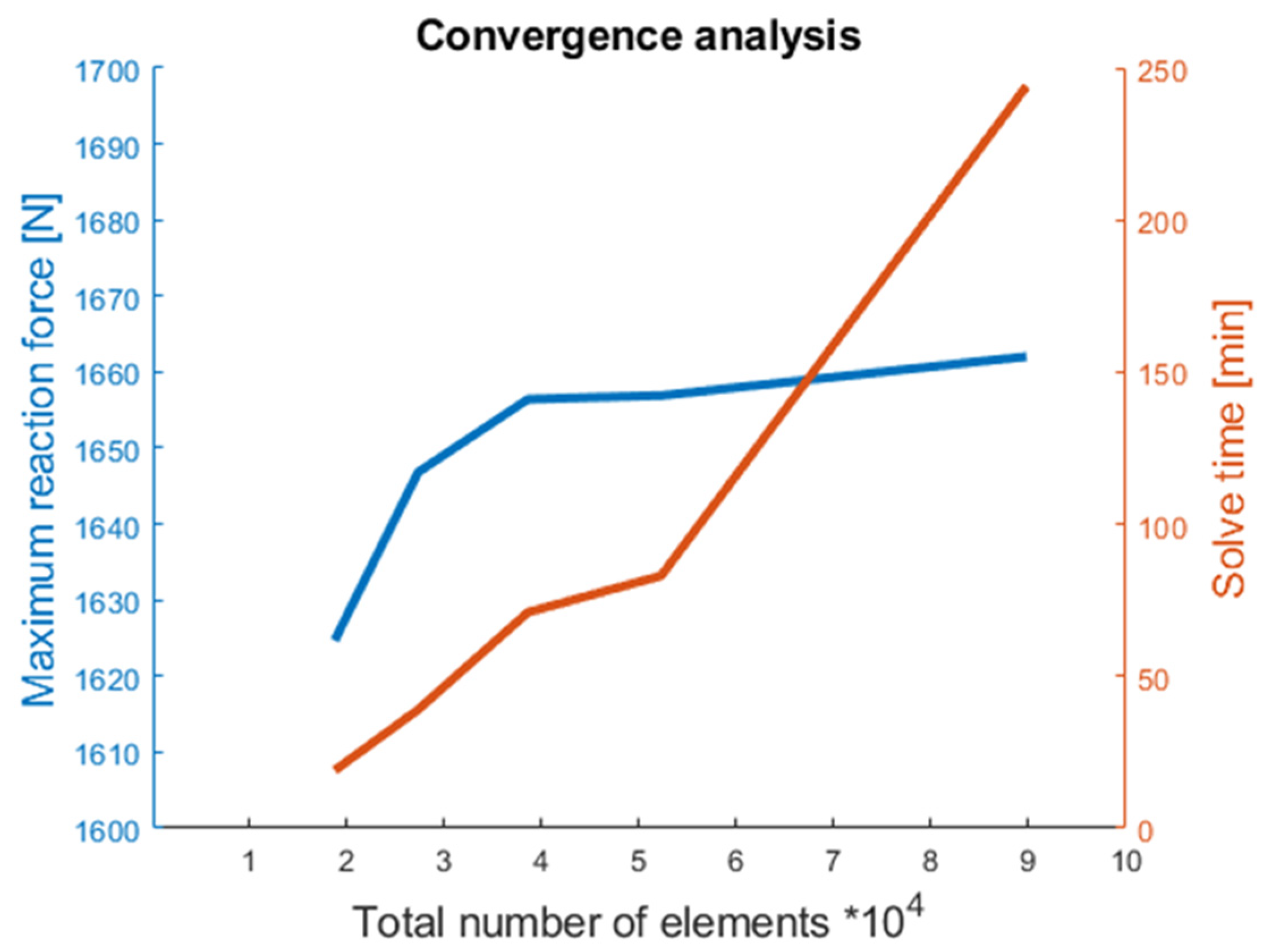
3.1. Convergence Analysis
3.2. Experimental Validation of the FE Model
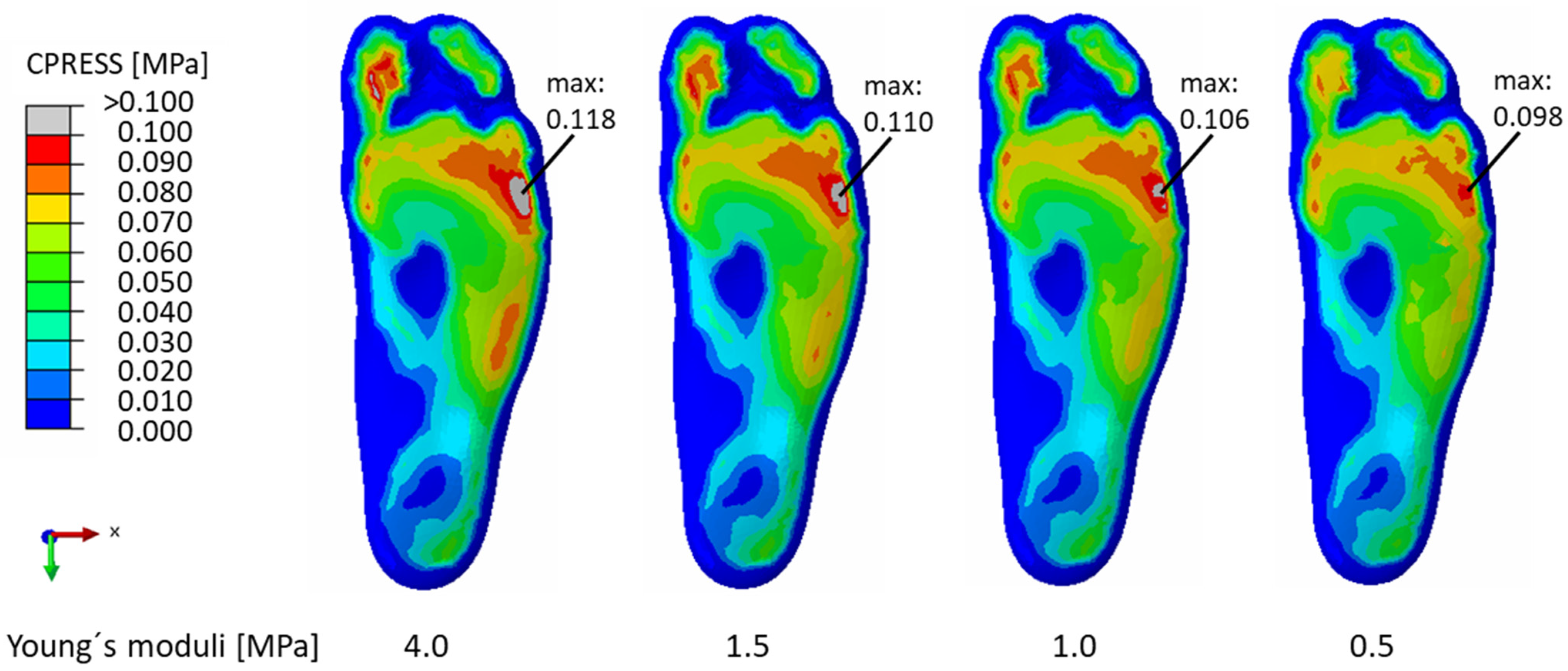
3.3. Parameter Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed. 2021. Available online: https://diabetesatlas.org/data/en/country/77/de.html (accessed on 2 August 2021).
- Zhang, Y.; Lazzarini, P.A.; McPhail, S.M.; van Netten, J.J.; Armstrong, D.G.; Pacella, R.E. Global Disability Burdens of Diabetes-Related Lower-Extremity Complications in 1990 and 2016. Diabetes Care 2020, 43, 964–974. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef] [PubMed]
- Morbach, S.; Müller, E.; Reike, H.; Risse, A.; Rümenapf, G.; Spraul, M. Diabetic Foot Syndrome. Exp. Clin. Endocrinol. Diabetes 2014, 122, 416–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Q.; Lazzarini, P.A.; Gibb, M.; Derhy, P.H.; Kinnear, E.M.; Burn, E.; Graves, N.; Norman, R.E. A cost-effectiveness analysis of optimal care for diabetic foot ulcers in Australia. Int. Wound J. 2016, 14, 616–628. [Google Scholar] [CrossRef]
- Kröger, K.; Berg, C.; Santosa, F.; Malyar, N.; Reinecke, H. Lower Limb Amputation in Germany. Dtsch. Arztebl. Int. 2017, 114, 130–136. [Google Scholar] [CrossRef] [Green Version]
- Norman, G.; Westby, M.J.; Vedhara, K.; Game, F.; Cullum, N.A. Effectiveness of psychosocial interventions for the prevention and treatment of foot ulcers in people with diabetes: A systematic review. Diabet. Med. 2020, 37, 1256–1265. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Swerdlow, M.A.; Armstrong, A.A.; Conte, M.S.; Padula, W.V.; Bus, S.A. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J. Foot Ankle Res. 2020, 13, 16. [Google Scholar] [CrossRef] [Green Version]
- Lazzarini, P.A.; Pacella, R.E.; Armstrong, D.G.; Van Netten, J.J. Diabetes-related lower-extremity complications are a leading cause of the global burden of disability. Diabet. Med. 2018, 35, 1297–1299. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Armstrong, D.G.; Lipsky, B.A. Preventing Foot Ulcers in Patients with Diabetes. JAMA 2005, 293, 217–228. [Google Scholar] [CrossRef]
- Bus, S.A. Priorities in offloading the diabetic foot. Diabetes Metab. Res. Rev. 2012, 28, 54–59. [Google Scholar] [CrossRef]
- Bus, S.A.; van Deursen, R.; Armstrong, D.G.; Lewis, J.E.A.; Caravaggi, C.F.; Cavanagh, P.R.; on behalf of the International Working Group on the Diabetic Foot (IWGDF). Footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in patients with diabetes: A systematic review. Diabetes Metab. Res. Rev. 2016, 32, 99–118. [Google Scholar] [CrossRef] [Green Version]
- Bus, S.A.; Lavery, L.A.; Monteiro-Soares, M.; Rasmussen, A.; Raspovic, A.; Sacco, I.C.; van Netten, J.J.; on behalf of the International Working Group on the Diabetic Foot. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36, e3269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collings, R.; Freeman, J.; Latour, J.M.; Paton, J. Footwear and insole design features for offloading the diabetic at risk foot—A systematic review and meta-analyses. Endocrinol. Diabetes Metab. 2020, 4, e00132. [Google Scholar] [CrossRef] [Green Version]
- Jeffcoate, W.J.; Harding, K.G. Diabetic foot ulcers. Lancet 2003, 361, 1545–1551. [Google Scholar] [CrossRef]
- Rizzo, L.; Tedeschi, A.; Fallani, E.; Coppelli, A.; Vallini, V.; Iacopi, E.; Piaggesi, A. Custom-Made Orthesis and Shoes in a Structured Follow-Up Program Reduces the Incidence of Neuropathic Ulcers in High-Risk Diabetic Foot Patients. Int. J. Low. Extrem. Wounds 2012, 11, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Schaper, N.C.; Van Netten, J.J.; Apelqvist, J.; Bus, S.A.; Hinchliffe, R.J.; Lipsky, B.A.; IWGDF Editorial Board. Practical Guidelines on the prevention and management of diabetic foot disease (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. S1), e3266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Netten, J.J.; Price, P.E.; Lavery, L.A.; Monteiro-Soares, M.; Rasmussen, A.; Jubiz, Y.; Bus, S.A.; on behalf of the International Working Group on the Diabetic Foot (IWGDF). Prevention of foot ulcers in the at-risk patient with diabetes: A systematic review. Diabetes Metab. Res. Rev. 2016, 32, 84–98. [Google Scholar] [CrossRef] [Green Version]
- Davia-Aracil, M.; Hinojo-Pérez, J.J.; Jimeno-Morenilla, A.; Mora-Mora, H. 3D printing of functional anatomical insoles. Comput. Ind. 2018, 95, 38–53. [Google Scholar] [CrossRef] [Green Version]
- Hellstrand, S.; Sundberg, L.; Karlsson, J.; Zügner, R.; Tranberg, R.; Tang, U.H. Measuring sustainability in healthcare: An analysis of two systems providing insoles to patients with diabetes. Environ. Dev. Sustain. 2020, 23, 6987–7001. [Google Scholar] [CrossRef]
- Paton, J.S.; Stenhouse, E.A.; Bruce, G.; Zahra, D.; Jones, R.B. A comparison of customised and prefabricated insoles to reduce risk factors for neuropathic diabetic foot ulceration: A participant-blinded randomised controlled trial. J. Foot Ankle Res. 2012, 5, 31. [Google Scholar] [CrossRef] [Green Version]
- Behforootan, S.; Chatzistergos, P.; Naemi, R.; Chockalingam, N. Finite element modelling of the foot for clinical application: A systematic review. Med. Eng. Phys. 2017, 39, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Telfer, S.; Erdemir, A.; Woodburn, J.; Cavanagh, P.R. What Has Finite Element Analysis Taught Us about Diabetic Foot Disease and Its Management? A Systematic Review. PLoS ONE 2014, 9, e109994. [Google Scholar] [CrossRef]
- Actis, R.L.; Ventura, L.B.; Lott, D.J.; Smith, K.E.; Commean, P.K.; Hastings, M.; Mueller, M.J. Multi-plug insole design to reduce peak plantar pressure on the diabetic foot during walking. Med. Biol. Eng. Comput. 2008, 46, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Erdemir, A.; Saucerman, J.J.; Lemmon, D.; Loppnow, B.; Turso, B.; Ulbrecht, J.S.; Cavanagh, P.R. Local plantar pressure relief in therapeutic footwear: Design guidelines from finite element models. J. Biomech. 2005, 38, 1798–1806. [Google Scholar] [CrossRef]
- Goske, S.; Erdemir, A.; Petre, M.; Budhabhatti, S.; Cavanagh, P.R. Reduction of plantar heel pressures: Insole design using finite element analysis. J. Biomech. 2006, 39, 2363–2370. [Google Scholar] [CrossRef] [PubMed]
- Cheung, J.T.-M.; Zhang, M. Parametric design of pressure-relieving foot orthosis using statistics-based finite element method. Med. Eng. Phys. 2008, 30, 269–277. [Google Scholar] [CrossRef]
- Ghazali, M.; Ren, X.; Rajabi, A.; Zamri, W.; Mustafah, N.M.; Ni, J. Finite Element Analysis of Cushioned Diabetic Footwear Using Ethylene Vinyl Acetate Polymer. Polymers 2021, 13, 2261. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.D.; Li, J.S.; Lake, M.J.; Zeng, Y.J.; Ren, J.; Li, Z.-Y. Image-based midsole insert design and the material effects on heel plantar pressure distribution during simulated walking loads. Comput. Methods Biomech. Biomed. Eng. 2011, 14, 747–753. [Google Scholar] [CrossRef]
- Gu, Y.D.; Ren, X.J.; Li, J.S.; Lake, M.J.; Zhang, Q.Y.; Zeng, Y.J. Computer simulation of stress distribution in the metatarsals at different inversion landing angles using the finite element method. Int. Orthop. 2010, 34, 669–676. [Google Scholar] [CrossRef] [Green Version]
- Nouman, M.; Dissaneewate, T.; Chong, D.; Chatpun, S. Effects of Custom-Made Insole Materials on Frictional Stress and Contact Pressure in Diabetic Foot with Neuropathy: Results from a Finite Element Analysis. Appl. Sci. 2021, 11, 3412. [Google Scholar] [CrossRef]
- Peng, Y.; Wong, D.W.-C.; Chen, T.L.-W.; Wang, Y.; Zhang, G.; Yan, F.; Zhang, M. Influence of arch support heights on the internal foot mechanics of flatfoot during walking: A muscle-driven finite element analysis. Comput. Biol. Med. 2021, 132, 104355. [Google Scholar] [CrossRef] [PubMed]
- Su, S.; Mo, Z.; Guo, J.; Fan, Y. The Effect of Arch Height and Material Hardness of Personalized Insole on Correction and Tissues of Flatfoot. J. Healthc. Eng. 2017, 2017, 8614341. [Google Scholar] [CrossRef] [Green Version]
- Tang, L.; Wang, L.; Bao, W.; Zhu, S.; Li, D.; Zhao, N.; Liu, C. Functional gradient structural design of customized diabetic insoles. J. Mech. Behav. Biomed. Mater. 2019, 94, 279–287. [Google Scholar] [CrossRef]
- Cheung, J.T.-M.; Zhang, M. A 3-dimensional finite element model of the human foot and ankle for insole design. Arch. Phys. Med. Rehabil. 2005, 86, 353–358. [Google Scholar] [CrossRef]
- Akrami, M.; Qian, Z.; Zou, Z.; Howard, D.; Nester, C.J.; Ren, L. Subject-specific finite element modelling of the human foot complex during walking: Sensitivity analysis of material properties, boundary and loading conditions. Biomech. Model. Mechanobiol. 2018, 17, 559–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarton, A.; Guiotto, A.; Malaquias, T.; Spolaor, F.; Sinigaglia, G.; Cobelli, C.; Jonkers, I.; Sawacha, Z. A methodological framework for detecting ulcers’ risk in diabetic foot subjects by combining gait analysis, a new musculoskeletal foot model and a foot finite element model. Gait Posture 2018, 60, 279–285. [Google Scholar] [CrossRef]
- Morales-Orcajo, E.; Souza, T.R.; Bayod, J.; Casas, E.B.D.L. Non-linear finite element model to assess the effect of tendon forces on the foot-ankle complex. Med. Eng. Phys. 2017, 49, 71–78. [Google Scholar] [CrossRef]
- Tsung, B.Y.S.; Zhang, M.; Mak, A.F.T.; Wong, M.W.N. Effectiveness of insoles on plantar pressure redistribution. J. Rehabil. Res. Dev. 2004, 41, 767–774. [Google Scholar] [CrossRef] [Green Version]
- Ren, X.; Lutter, C.; Kebbach, M.; Bruhn, S.; Bader, R.; Tischer, T. Lower extremity joint compensatory effects during the first recovery step following slipping and stumbling perturbations in young and older subjects. BMC Geriatr. 2022, 22, 656. [Google Scholar] [CrossRef]
- Ren, X.; Lutter, C.; Kebbach, M.; Bruhn, S.; Yang, Q.; Bader, R.; Tischer, T. Compensatory Responses During Slip-Induced Perturbation in Patients with Knee Osteoarthritis Compared with Healthy Older Adults: An Increased Risk of Falls? Front. Bioeng. Biotechnol. 2022, 10, 893840. [Google Scholar] [CrossRef] [PubMed]
- Van den Bogert, A.J.; Geijtenbeek, T.; Even-Zohar, O.; Steenbrink, F.; Hardin, E.C. A real-time system for biomechanical analysis of human movement and muscle function. Med. Biol. Eng. Comput. 2013, 51, 1069–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carbone, V.; Fluit, R.; Pellikaan, P.; van der Krogt, M.M.; Janssen, D.; Damsgaard, M.; Vigneron, L.; Feilkas, T.; Koopman, H.F.J.M.; Verdonschot, N. TLEM 2.0—A comprehensive musculoskeletal geometry dataset for subject-specific modeling of lower extremity. J. Biomech. 2015, 48, 734–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damsgaard, M.; Rasmussen, J.; Christensen, S.T.; Surma, E.; de Zee, M. Analysis of musculoskeletal systems in the AnyBody Modeling System. Simul. Model. Pract. Theory 2006, 14, 1100–1111. [Google Scholar] [CrossRef]
- Andersen, M.S. Introduction to musculoskeletal modelling. In Computational Modelling of Biomechanics and Biotribology in the Musculoskeletal System; Elsevier: Amsterdam, The Netherlands, 2021; pp. 41–80. [Google Scholar]
- Qian, Z.; Ren, L.; Ding, Y.; Hutchinson, J.R.; Ren, L. A Dynamic Finite Element Analysis of Human Foot Complex in the Sagittal Plane during Level Walking. PLoS ONE 2013, 8, e79424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, L.; Jones, R.K.; Howard, D. Whole body inverse dynamics over a complete gait cycle based only on measured kinematics. J. Biomech. 2008, 41, 2750–2759. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Kluess, D.; Souffrant, R.; Mittelmeier, W.; Wree, A.; Schmitz, K.-P.; Bader, R. A convenient approach for finite-element-analyses of orthopaedic implants in bone contact: Modeling and experimental validation. Comput. Methods Programs Biomed. 2009, 95, 23–30. [Google Scholar] [CrossRef]
- ASTM D 3574-17; D20 Committee. Standard Test Methods for Flexible Cellular Materials Slab, Bonded, and Molded Urethane Foams. ASTM International: West Conshohocken, PA, USA, 2017. [Google Scholar]
- Häfele, P.; Issler, L.; Ruoß, H. Festigkeitslehre—Grundlagen, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2003. [Google Scholar]
- Nakamura, S.; Crowninshield, R.D.; Cooper, R.R. An Analysis of Soft Tissue Loading in the Foot—A Preliminary Report; Bulletin of Prosthetics Research: Washington, DC, USA, 1981. [Google Scholar]
- Xu, Y.-X.; Juang, J.-Y. Measurement of Nonlinear Poisson’s Ratio of Thermoplastic Polyurethanes under Cyclic Softening Using 2D Digital Image Correlation. Polymers 2021, 13, 1498. [Google Scholar] [CrossRef]
- Lewis, G. Finite element analysis of a model of a therapeutic shoe: Effect of material selection for the outsole. Bio-Med. Mater. Eng. 2003, 13, 75–81. [Google Scholar]
- Lemmon, D.; Shiang, T.; Hashmi, A.; Ulbrecht, J.S.; Cavanagh, P.R. The effect of insoles in therapeutic footwear—A finite element approach. J. Biomech. 1997, 30, 615–620. [Google Scholar] [CrossRef]
- Chen, W.-M.; Lee, T.; Lee, P.V.S.; Lee, J.W.; Lee, S.-J. Effects of internal stress concentrations in plantar soft-tissue—A preliminary three-dimensional finite element analysis. Med. Eng. Phys. 2010, 32, 324–331. [Google Scholar] [CrossRef]
- Faller, A.; Schünke, M.; Schünke, G. Der Körper des Menschen: Einführung in Bau und Funktion; 4 Poster mit Übersichten Skelett, Gefäße, Nerven, Muskeln, 16., überarb. Aufl.; Georg Thieme Verlag KG: Stuttgart, Germany, 2012. [Google Scholar]
- Mandolini, M.; Brunzini, A.; Manieri, S.; Germani, M. Foot plantar pressure offloading: How to select the right material for a custom-made insole. In DS 87-1 Proceedings of the 21st International Conference on Engineering Design (ICED 17) Vol 1: Resource Sensitive Design, Design Research Applications and Case Studies, Vancouver, BC, Canada, 21–25 August 2017; Universitŕ Politecnica delle Marche: Ancona, Italy, 2017; pp. 469–478. [Google Scholar]
- Bus, S.A.; Zwaferink, J.B.; Dahmen, R.; Busch-Westbroek, T. State of the art design protocol for custom made footwear for people with diabetes and peripheral neuropathy. Diabetes Metab. Res. Rev. 2020, 36, e3237. [Google Scholar] [CrossRef]
- Bocanegra, M.; López, J.; Vidal-Lesso, A.; Tobar, A.; Vallejo, R. Numerical Assessment of the Structural Effects of Relative Sliding between Tissues in a Finite Element Model of the Foot. Mathematics 2021, 9, 1719. [Google Scholar] [CrossRef]
- Telfer, S.; Erdemir, A.; Woodburn, J.; Cavanagh, P.R. Simplified versus geometrically accurate models of forefoot anatomy to predict plantar pressures: A finite element study. J. Biomech. 2016, 49, 289–294. [Google Scholar] [CrossRef]
- Perry, J. Ganganalyse: Norm und Pathologie des Gehens, 1st ed.; Urban & Fischer: München, Germany, 2003. [Google Scholar]
- Dai, X.-Q.; Li, Y.; Zhang, M.; Cheung, J.T.-M. Effect of sock on biomechanical responses of foot during walking. Clin. Biomech. 2006, 21, 314–321. [Google Scholar] [CrossRef]
- Guiotto, A.; Sawacha, Z.; Guarneri, G.; Avogaro, A.; Cobelli, C. 3D finite element model of the diabetic neuropathic foot: A gait analysis driven approach. J. Biomech. 2014, 47, 3064–3071. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wong, D.W.-C.; Zhang, M. Computational Models of the Foot and Ankle for Pathomechanics and Clinical Applications: A Review. Ann. Biomed. Eng. 2016, 44, 213–221. [Google Scholar] [CrossRef]
- Spirka, T.A.; Erdemir, A.; Spaulding, S.E.; Yamane, A.; Telfer, S.; Cavanagh, P.R. Simple finite element models for use in the design of therapeutic footwear. J. Biomech. 2014, 47, 2948–2955. [Google Scholar] [CrossRef] [Green Version]
- Natali, A.N.; Forestiero, A.; Carniel, E.L.; Pavan, P.G.; Dal Zovo, C. Investigation of foot plantar pressure: Experimental and numerical analysis. Med. Biol. Eng. Comput. 2010, 48, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Petre, M.; Erdemir, A.; Panoskaltsis, V.P.; Spirka, T.A.; Cavanagh, P.R. Optimization of Nonlinear Hyperelastic Coefficients for Foot Tissues Using a Magnetic Resonance Imaging Deformation Experiment. J. Biomech. Eng. 2013, 135, 61001–61012. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Chen, Z.; Jin, Z. (Eds.) Computational Modelling of Biomechanics and Biotribology in the Musculoskeletal System: Biomaterials and Tissues, 2nd ed.; Woodhead Publishing: Duxford, UK, 2021. [Google Scholar]
- Chen, W.-M.; Lee, S.-J.; Lee, P.V.S. Plantar pressure relief under the metatarsal heads—Therapeutic insole design using three-dimensional finite element model of the foot. J. Biomech. 2015, 48, 659–665. [Google Scholar] [CrossRef]
- Kwan, R.L.-C.; Zheng, Y.-P.; Cheing, G.L.-Y. The effect of aging on the biomechanical properties of plantar soft tissues. Clin. Biomech. 2010, 25, 601–605. [Google Scholar] [CrossRef]
- Gefen, A. Plantar soft tissue loading under the medial metatarsals in the standing diabetic foot. Med. Eng. Phys. 2003, 25, 491–499. [Google Scholar] [CrossRef]
- Sert, E.; Öchsner, A.; Hitzler, L.; Werner, E.; Merkel, M. Additive manufacturing: A review of the influence of building orientation and post heat treatment on the mechanical properties of aluminium Alloys. In State of the Art and Future Trends in Material Modelling; Altenbach, H., Öchsner, A., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 349–366. [Google Scholar]
- Scarton, A.; Aerts, W.; Guiotto, A.; Sawacha, Z.; Jonkers, I.; Sloten, J.V.; Cobelli, C. Gait analysis driven finite element simulations: Towards the use of opensim output as boundary condition. Gait Posture 2015, 42, S75. [Google Scholar] [CrossRef]
- Peng, Y.; Wong, D.W.-C.; Wang, Y.; Chen, T.L.-W.; Tan, Q.; Chen, Z.; Jin, Z.; Zhang, M. Immediate Effects of Medially Posted Insoles on Lower Limb Joint Contact Forces in Adult Acquired Flatfoot: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 2226. [Google Scholar] [CrossRef] [Green Version]
- Price, M.A.; LaPrè, A.K.; Johnson, R.T.; Umberger, B.R.; Sup, F.C. A model-based motion capture marker location refinement approach using inverse kinematics from dynamic trials. Int. J. Numer. Methods Biomed. Eng. 2020, 36, e3283. [Google Scholar] [CrossRef] [PubMed]
- Kluess, D.; Hurschler, C.; Voigt, C.; Hölzer, A.; Stoffel, M. Einsatzgebiete der numerischen Simulation in der muskuloskelettalen Forschung und ihre Bedeutung für die Orthopädische Chirurgie. Orthopade 2013, 42, 220–231. [Google Scholar] [CrossRef] [PubMed]
- Kunze, M.; Schaller, A.; Steinke, H.; Scholz, R.; Voigt, C. Combined multi-body and finite element investigation of the effect of the seat height on acetabular implant stability during the activity of getting up. Comput. Methods Programs Biomed. 2012, 105, 175–182. [Google Scholar] [CrossRef]
- Halloran, J.P.; Ackermann, M.; Erdemir, A.; Bogert, A.J.V.D. Concurrent musculoskeletal dynamics and finite element analysis predicts altered gait patterns to reduce foot tissue loading. J. Biomech. 2010, 43, 2810–2815. [Google Scholar] [CrossRef] [Green Version]
- Eckardt, A.; Lobmann, R. Der Diabetische Fuß; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Kunz, J.; Studer, M. Druck-Elastizitätsmodul über Shore-A-Härte ermitteln. Kunststoffe 2006, 96, 92–94. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Young’s Modulus [MPa] | Poisson Ratio | References | |
|---|---|---|---|
| Bone | 7300 | 0.30 | Nakamura et al. [52] |
| Insole | 4.0 | 0.48 | Xu and Juang [53] |
| Shoe sole | 1000 | 0.42 | Lewis [54] |
| C10 | C01 | C20 | C11 | C02 | D1 | D2 |
|---|---|---|---|---|---|---|
| 0.08556 | −0.05841 | 0.039 | −0.02319 | 0.00851 | 3.65273 | 0 |
| High Point Ground Reaction Force | Low Point Ground Reaction Force | |
|---|---|---|
| JM—Dorsiflexion [Nmm] | 24,002.00 | 53,192.00 |
| JRF—Medio (−)/Lateral (+) [N] | −38.20 | 2.28 |
| JRF—Anterior (−)/Posterior (+) [N] | 86.42 | −24.19 |
| JRF—Proximal (−)/Distal (+) [N] | 704.68 | 577.78 |
| Mesh | Element Size [mm] | Total Number of Elements | Total Number of Nodes | Maximal Reaction Force [N] | Percentage Deviation to the Finest Mesh [%] | Computation Time [min] |
|---|---|---|---|---|---|---|
| 1 | 9 | 18,696 | 23,144 | 1624.7 | −1.9 | 19 |
| 2 | 8 | 27,272 | 33,997 | 1646.8 | −0.9 | 39 |
| 3 | 7 | 38,553 | 47,035 | 1656.4 | −0.3 | 71 |
| 4 | 6 | 51,702 | 60,775 | 1656.9 | −0.3 | 83 |
| 5 | 5 | 89,761 | 104,405 | 1662.0 | - | 244 |
| Percentage Reduction in Peak Plantar Pressure [%] | |||
|---|---|---|---|
| Area | 1.5 MPa | 1.0 MPa | 0.5 MPa |
| Heel | −8.16 | −13.01 | −22.96 |
| Lateral Midfoot | −4.44 | −8.15 | −16.30 |
| Lateral Forefoot | −6.78 | −10.17 | −16.95 |
| Toe | −11.30 | −17.39 | −26.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geiger, F.; Kebbach, M.; Vogel, D.; Weissmann, V.; Bader, R. Efficient Computer-Based Method for Adjusting the Stiffness of Subject-Specific 3D-Printed Insoles during Walking. Appl. Sci. 2023, 13, 3854. https://doi.org/10.3390/app13063854
Geiger F, Kebbach M, Vogel D, Weissmann V, Bader R. Efficient Computer-Based Method for Adjusting the Stiffness of Subject-Specific 3D-Printed Insoles during Walking. Applied Sciences. 2023; 13(6):3854. https://doi.org/10.3390/app13063854
Chicago/Turabian StyleGeiger, Franziska, Maeruan Kebbach, Danny Vogel, Volker Weissmann, and Rainer Bader. 2023. "Efficient Computer-Based Method for Adjusting the Stiffness of Subject-Specific 3D-Printed Insoles during Walking" Applied Sciences 13, no. 6: 3854. https://doi.org/10.3390/app13063854