
Analysis of Factors Associated with Charcot Neuroarthropathy following Pancreatic Transplantation

 , , and
, , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Immunosuppressive Protocol
2.3. Patient Characteristics and Other Relevant Data
2.4. Nerve Conduction Velocity Study
2.5. Perception Threshold Test
2.6. Bone Mineral Density Test
2.7. CN Diagnosis and Treatment
2.8. Ethical Considerations
2.9. Statistical Analysis
3. Results
3.1. Background Characteristics of All Patients
3.2. The Cumulative Incidence of CN
3.3. Background of Characteristics of Patients with CN
3.4. The Neurological Examination Results
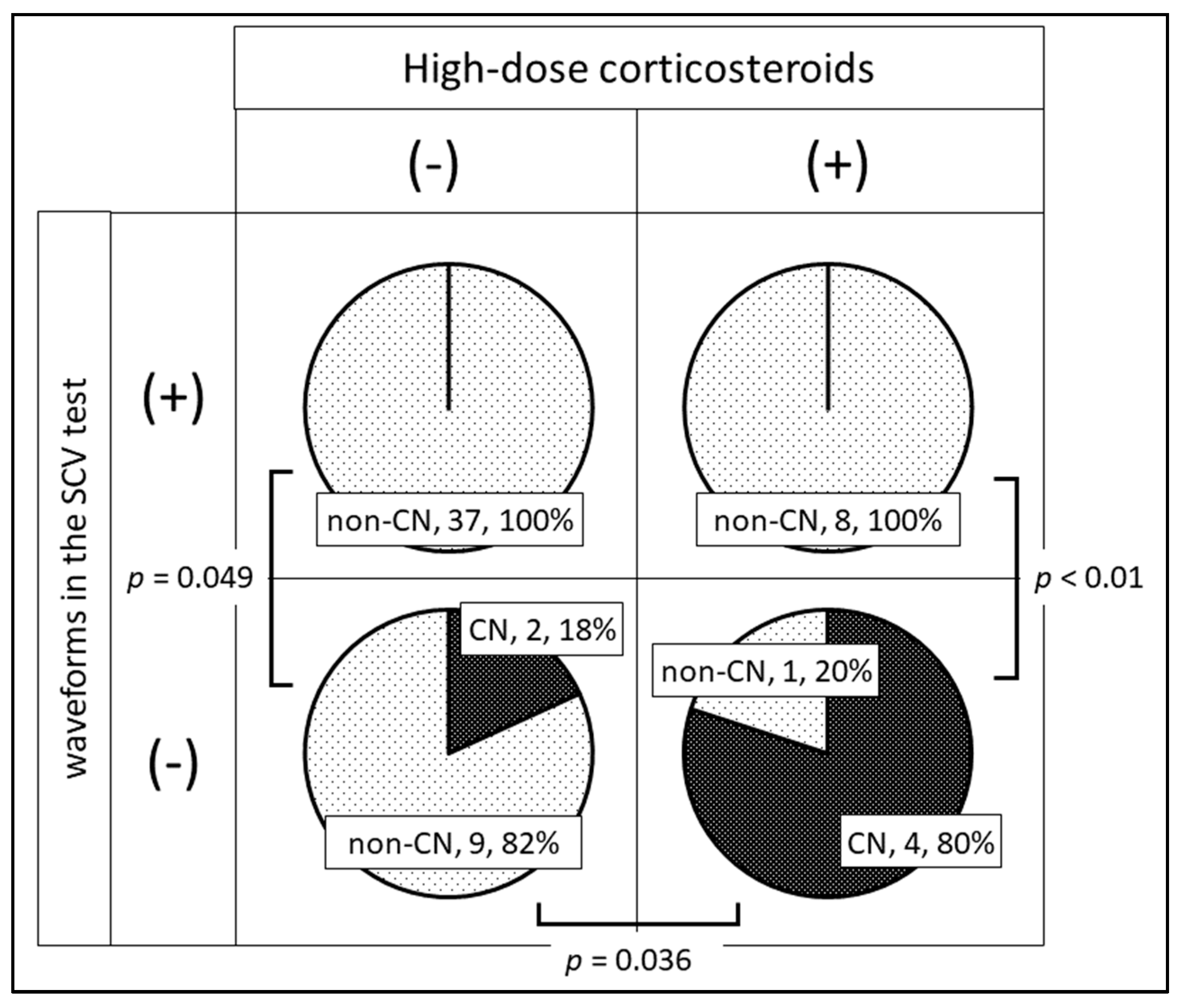
3.5. Severe Peripheral Neuropathy and CN Development
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gruessner, R.W.; Sutherland, D.E.; Gruessne, A.C. Mortality assessment for pancreas transplants. Am. J. Transplant. 2004, 4, 2018–2026. [Google Scholar]
- Ito, T.; Kenmochi, T.; Aida, N.; Matsushima, H.; Kurihara, K.; Ishihara, T.; Shintani, A.; Asaoka, T.; Ito, T. Impact of pancreas transplantation on patient survival: An analysis of the Japanese pancreas transplant registry. J. Clin. Med. 2020, 9, 2134. [Google Scholar] [CrossRef] [PubMed]
- Albers, J.W.; Herman, W.H.; Pop-Busui, R.; Feldman, E.; Martin, C.; Cleary, P.; Waberski, B.; Lachin, J.; Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Effect of prior intensive insulin treatment during the Diabetes Control and Complications Trial (DCCT) on peripheral neuropathy in type 1 diabetes during the Epidemiology of Diabetes Interventions and Complications (EDIC) Study. Diabetes Care 2010, 33, 1090–1096. [Google Scholar] [CrossRef] [Green Version]
- Dardari, D.; Schuldiner, S.; Julien, C.-A.; Van, G.H.; M’Bemba, J.; Bourgeon, M.; Sultan, A.; Lepeut, M.; Grandperret-Vauthier, S.; Baudoux, F.; et al. Trends in the relation between hyperglycemia correction and active Charcot neuroarthropathy: Results from the EPICHAR study. BMJ Open Diabetes Res. Care 2022, 10, e002380. [Google Scholar] [CrossRef] [PubMed]
- Dardari, D.; Dardari, R. Why the Risk of Developing Neuroarthropathy Is Higher After Simultaneous Kidney and Pancreatic Transplantation Compared to Kidney Transplantation Only: The Role of Euglycemia. Ann. Transplant. 2021, 26, e928449. [Google Scholar] [CrossRef]
- Papanas, N.; Maltezos, E. Etiology, pathophysiology, and classifications of the diabetic Charcot Foot. Diabet. Foot Ankle 2013, 4. [Google Scholar] [CrossRef]
- Chantelau, E.; Onvlee, G.J. Charcot foot in diabetes: Farewell to neurotrophic theory. Horm. Metab. Res. 2006, 38, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Christensen, T.M.; Bülow, J.; Simonsen, L.; Holstein, P.; Svendsen, O. Bone mineral density in diabetes mellitus patients with and without a Charcot foot. Clin. Physiol. Funct. Imaging 2010, 30, 130–134. [Google Scholar] [PubMed]
- Ergen, F.B.; Sanverdi, S.E.; Oznur, A. Charcot foot in diabetes and an update on imaging. Diabet. Foot Ankle 2013, 4. [Google Scholar] [CrossRef] [Green Version]
- Matricali, G.A.; Bammens, B.; Kuypers, D.; Flour, M.; Mathieu, C. High rate of Charcot foot attacks early after simultaneous pancreas-kidney transplantation. Transplantation 2007, 83, 245–246. [Google Scholar] [CrossRef]
- Rangel, É.B.; Sá, J.R.; Gomes, S.A.; Carvalho, A.; Melaragno, C.; Gonzalez, A.; Linhares, M.; Medina-Pestana, J. Charcot neuroarthropathy after simultaneous pancreas-kidney transplant. Transplantation 2012, 94, 642–645. [Google Scholar] [CrossRef] [PubMed]
- García, B.F.; Kuypers, D.R.; Matricali, G.A. Charcot neuroarthropathy after simultaneous pancreas-kidney transplantation: Risk factors, prevalence, and outcome. Clin. Transplant. 2015, 29, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Boggi, U.; Vistoli, F.; Andres, A.; Arbogast, H.P.; Badet, L.; Baronti, W.; Bartlett, S.T.; Benedetti, E.; Branchereau, J.; Burke, G.W.; et al. First World Consensus Conference on pancreas transplantation: Part II-recommendations. Am. J. Transplant. 2021, 21, 17–59. [Google Scholar] [CrossRef] [PubMed]
- Cosman, F.; de Beur, S.J.; LeBoff, M.S. National Osteoporosis Foundation. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos. Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013, 48, 452–458. [Google Scholar]
- Dyck, P.J.; Kratz, K.M.; Karnes, J.L.; Litchy, W.J.; Klein, R.; Pach, J.M.; Wilson, D.M.; O’Brien, P.C.; Melton, L.J., 3rd; Service, F.J. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: The Rochester Diabetic Neuropathy Study. Neurology 1993, 43, 817–824. [Google Scholar] [CrossRef]
- Feldman, E.L.; Callaghan, B.C.; Pop-Busui, R. Diabetic neuropathy. Nat. Rev. Dis. Primers 2019, 5, 42. [Google Scholar] [CrossRef]
- Callaghan, B.C.; Little, A.A.; Feldman, E.L.; Hughes, R.A.C. Enhanced glucose control for preventing and treating diabetic neuropathy. Cochrane Database Syst. Rev. 2012, 6, CD007543. [Google Scholar]
- Smets, Y.F.; de Fijter, J.W.; Ringers, J.; Lemkes, H.H.; Hamdy, N.A. Long-term follow-up study on bone mineral density and fractures after simultaneous pancreas-kidney transplantation. Kidney Int. 2004, 66, 2070–2076. [Google Scholar]
- Pereira, S.; Pedroso, S.; Martins, L.; Santos, P.; Almeida, M.; Freitas, C.; Dias, L.; Dores, J.; Almeida, R.; Henriques, A.C.; et al. Bone mineral density after simultaneous kidney-pancreas transplantation: Four years follow-up of 57 recipients. Transplant. Proc. 2010, 42, 555–557. [Google Scholar] [CrossRef] [PubMed]
- Rocha, A.; Martins, L.S.; Malheiro, J.; Dores, J.; Santos, C.; Henriques, C. Changes in bone mineral density following long-term simultaneous pancreas-kidney transplantation. J. Bone Miner. Metab. 2016, 34, 209–215. [Google Scholar] [CrossRef]
- Sewing, L.; Potasso, L.; Baumann, S.; Schenk, D.; Gazozcu, F.; Lippuner, K.; Kraenzlin, M.; Zysset, P.; Meier, C. Bone microarchitecture and strength in long-standing type 1 diabetes. J. Bone Miner. Res. 2022, 37, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, A.; Cinnirella, M.; Bayfield, J.; Watson, C.J.E.; Oniscu, G.C.; Draper, H.; Tomson, C.R.V.; Ravanan, R.; Johnson, R.J.; Forsythe, J.; et al. Changes in quality of life, health status and other patient-reported outcomes following simultaneous pancreas and kidney transplantation (SPKT): A quantitative and qualitative analysis within a UK-wide programme. Transpl. Int. 2020, 33, 1230–1243. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Kenmochi, T.; Maruyama, M.; Saigo, K.; Akutsu, N.; Iwashita, C.; Otsuki, K.; Miyazaki, M. Evaluation of quality of life after simultaneous pancreas and kidney transplantation from living donors using short form 36. Transplant. Proc. 2008, 40, 2565–2567. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 61) | Patients with CN (n = 6) | Patients without CN (n = 55) | p-Value | |
|---|---|---|---|---|
| Age at Tx | 44 [29–65] | 38.5 [29–57] | 44 [31–65] | 0.42 |
| Sex (male, %) | 23 (37.7) | 1 (16.7) | 22 (44.0) | 0.40 |
| BMI (Kg/m2) | 19.9 [15.5–28.4] | 19.8 [18.1–22.8] | 20.2 [15.5–28.4] | 0.98 |
| Duration of DM (years) | 28.5 [16.8–53.1] | 22.7 [18.7–36.6] | 29.2 [16.8–53.1] | 0.20 |
| Duration of HD (years) | 3.7 [0–19.2] | 5.0 [0.4–11.3] | 3.6 [0–19.2] | 0.55 |
| Procedure (%) | 0.22 | |||
| PTA | 2 (3.3) | 1 (16.7) | 1 (1.8) | |
| PAK | 9 (14.8) | 0 (0) | 9 (16.4) | |
| SPK | 50 (82.0) | 5 (83.3) | 45 (81.8) | |
| Induction drug dose (%) | 1.0 | |||
| Basiliximab | 53 (86.9) | 6 (100) | 47 (85.5) | |
| Thymoglobulin | 8 (13.1) | 0 (0) | 8 (14.5) | |
| Everolimus (%) | 13 (21.3) | 1 (16.7) | 12 (21.8) | 1.0 |
| MMF (%) | 56 (91.8) | 6 (100) | 50 (90.9) | 1.0 |
| Pre-Tx HbA1c (%) | 7.3 [4.9–9.8] | 8.8 [7.3–9.8] | 7.1 [4.9–9.8] | <0.001 |
| HbA1c at 1M (%) | 5.5 [4.3–6.9] | 5.6 [5.0–6.9] | 5.6 [4.3–6.9] | 0.84 |
| Rejection (%) | 10 (16.4) | 2 (33.3) | 8 (14.5) | 0.25 |
| High-dose steroid dose (%) | 12 (19.7) | 4 (66.7) | 9 (16.4) | 0.015 |
| Additional steroid dose (mg) | 1892.8 [0–6000] | 937.5 [0–3075] | 2987.5 [312.5–6000] | 0.16 |
| Patients with CN (N = 6) | Patients without CN (N = 55) | p-Value | |
|---|---|---|---|
| Autonomic nerve study | |||
| CVR-R (%) | 0.90 [0.43–1.55] | 1.07 [0.36–4.79] | 0.79 |
| Nerve conduction study | |||
| Motor nerve velocity test (tibial) | |||
| Total disappearance (%) | 0/6 (0) | 1/55 (1.8) | 1.0 |
| Velocity (m/s) | 32.7 [26.0–36.0] | 37.0 [21.0–45.0] | 0.014 |
| Amplitude (mV) | 1.29 [0.4–8.02] | 10.8 [0.15–28.11] | 0.001 |
| F wave (n = 60) | |||
| Total disappearance (%) | 3/6 (50.0) | 4/54 (7.3) | 0.025 |
| Latency (s) | 58.3 [51.3–64.4] | 53.2 [45.1–72.9] | 0.19 |
| Sensory nerve velocity test (sural) | |||
| Total disappearance (%) | 6/6 (100) | 10/55 (18.2) | <0.001 |
| Velocity (m/s) | - | 40.5 [30.0–50.4] | |
| Amplitude (mV) | - | 0.004 [0.001–16.5] | |
| Current perception threshold (n = 45) | |||
| 5 Hz | |||
| >160 (%) | 3/3 | 3/42 | 0.020 |
| 250 Hz | |||
| >260 (%) | 3/3 | 4/42 | 0.033 |
| 2000 Hz | |||
| >550 (%) | 3/3 | 7/42 | 0.095 |
| Bone density test (femur) (n = 52) | |||
| T-score | 0.78 | ||
| −1.0< | 0/4 (0) | 6/48 (12.5) | |
| −2.5<, <−1.0 | 2/4 (50.0) | 26/48 (54.2) | |
| <−2.5 | 2/4 (50.0) | 16/48 (33.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aida, N.; Ito, T.; Kurihara, K.; Hiratsuka, I.; Shibata, M.; Suzuki, A.; Kenmochi, T. Analysis of Factors Associated with Charcot Neuroarthropathy following Pancreatic Transplantation. Appl. Sci. 2023, 13, 2670. https://doi.org/10.3390/app13042670
Aida N, Ito T, Kurihara K, Hiratsuka I, Shibata M, Suzuki A, Kenmochi T. Analysis of Factors Associated with Charcot Neuroarthropathy following Pancreatic Transplantation. Applied Sciences. 2023; 13(4):2670. https://doi.org/10.3390/app13042670
Chicago/Turabian StyleAida, Naohiro, Taihei Ito, Kei Kurihara, Izumi Hiratsuka, Megumi Shibata, Atsushi Suzuki, and Takashi Kenmochi. 2023. "Analysis of Factors Associated with Charcot Neuroarthropathy following Pancreatic Transplantation" Applied Sciences 13, no. 4: 2670. https://doi.org/10.3390/app13042670