
Characteristics of the Contingent Negative Variation during Lower Limb Functional Movement with an Audio-Visual Cue

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Equipment Set Up
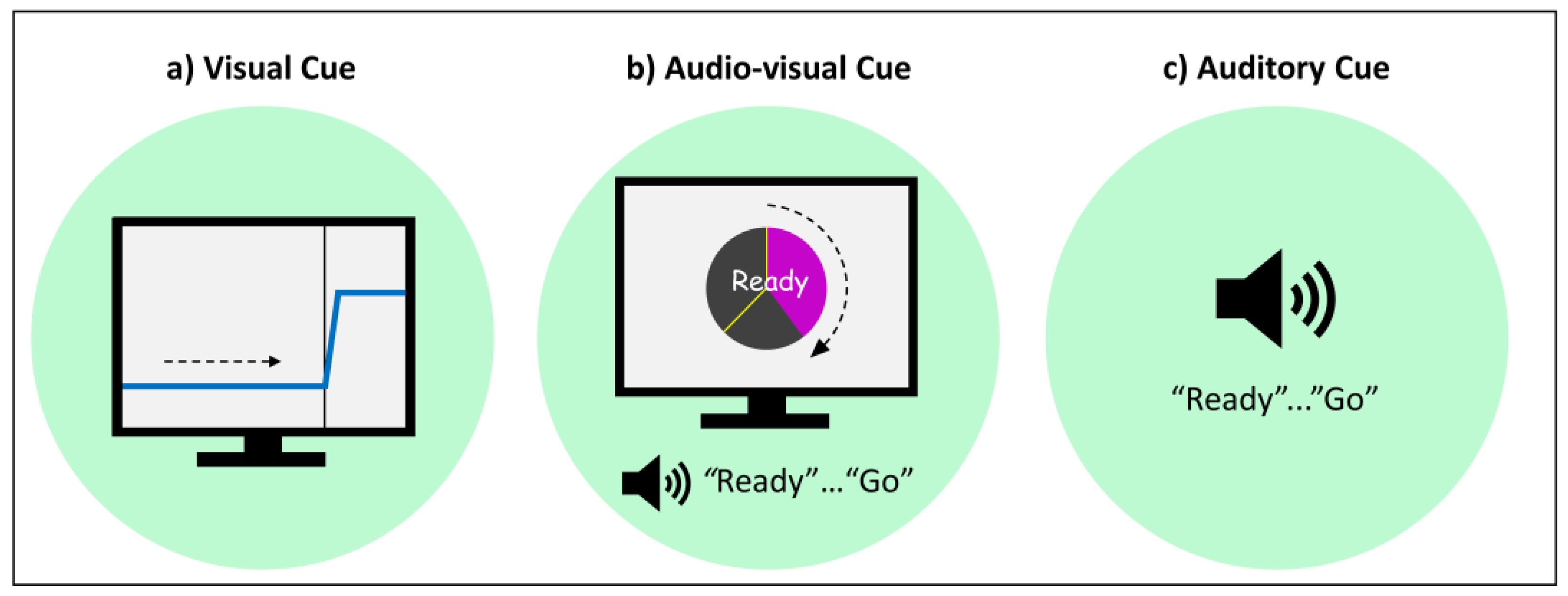
2.3. Movement Cues
2.4. Procedures
2.5. Data Processing
2.5.1. Surrogate Channel
2.5.2. Epoch Extraction
2.6. Data Analysis
3. Results
3.1. Sample
3.2. CNV Characteristics under Different Movement Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walter, W.G.; Cooper, R.; Aldridge, V.J.; McCallum, W.C.; Winter, A.L. Contingent negative variation: An electric sign of sensori-motor association and expectancy in the human brain. Nature 1964, 203, 380–384. [Google Scholar] [CrossRef]
- Shakeel, A.; Navid, M.S.; Anwar, M.N.; Mazhar, S.; Jochumsen, M.; Niazi, I.K. A review of techniques for detection of movement intention using movement-related cortical potentials. Comput. Math. Methods Med. 2015, 2015, 346217. [Google Scholar] [CrossRef] [Green Version]
- Olsen, S.; Alder, G.; Williams, M.; Chambers, S.; Jochumsen, M.; Signal, N.; Rashid, U.; Niazi, I.K.; Taylor, D. Electroencephalographic recording of the movement-related cortical potential in ecologically valid movements: A scoping review. Front. Neurosci. 2021, 15, 721387. [Google Scholar] [CrossRef]
- Monge-Pereira, E.; Molina-Rueda, F.; Rivas-Montero, F.M.; Ibanez, J.; Serrano, J.I.; Alguacil-Diego, I.M.; Miangolarra-Page, J.C. Electroencephalography as a post-stroke assessment method: An updated review. Neurologia 2017, 32, 40–49. [Google Scholar] [CrossRef]
- Osborne, K.J.; Kraus, B.; Lam, P.H.; Vargas, T.; Mittal, V.A. Contingent negative variation blunting and psychomotor dysfunction in schizophrenia: A systematic review. Schizophr. Bull. 2020, 46, 1144–1154. [Google Scholar] [CrossRef]
- Bai, O.; Vorbach, S.; Hallett, M.; Floeter, M.K. Movement-related cortical potentials in primary lateral sclerosis. Ann. Neurol. Off. J. Am. Neurol. Assoc. Child Neurol. Soc. 2006, 59, 682–690. [Google Scholar] [CrossRef]
- Guger, C.; Spataro, R.; Allison, B.Z.; Heilinger, A.; Ortner, R.; Cho, W.; La Bella, V. Complete locked-in and locked-in patients: Command following assessment and communication with vibro-tactile P300 and motor imagery brain-computer interface tools. Front. Neurosci. 2017, 11, 251. [Google Scholar] [CrossRef]
- Bizovicar, N.; Zidar, I.; Koritnik, B.; Zidar, J. Inspiratory- and finger-flexion-related cortical potentials in patients with amyotrophic lateral sclerosis--an exploratory study. Clin. Neurol. Neurosurg. 2012, 114, 455–459. [Google Scholar] [CrossRef]
- Peters, S.; Ivanova, T.D.; Lakhani, B.; Boyd, L.A.; Staines, W.R.; Handy, T.C.; Garland, S.J. Symmetry of cortical planning for initiating stepping in sub-acute stroke. Clin. Neurophysiol. 2018, 129, 787–796. [Google Scholar] [CrossRef]
- Jochumsen, M.; Shafique, M.; Hassan, A.; Niazi, I.K. Movement intention detection in adolescents with cerebral palsy from single-trial EEG. J. Neural Eng. 2018, 15, 066030. [Google Scholar] [CrossRef] [Green Version]
- Bae, S.H.; Lee, J.H.; Oh, K.A.; Kim, K.Y. The effects of kinesio taping on potential in chronic low back pain patients anticipatory postural control and cerebral cortex. J. Phys. Ther. Sci. 2013, 25, 1367–1371. [Google Scholar] [CrossRef] [Green Version]
- Jochumsen, M.; Niazi, I.K.; Mrachacz-Kersting, N.; Jiang, N.; Farina, D.; Dremstrup, K. Comparison of spatial filters and features for the detection and classification of movement-related cortical potentials in healthy individuals and stroke patients. J. Neural Eng. 2015, 12, 056003. [Google Scholar] [CrossRef]
- Mrachacz-Kersting, N.; Stevenson, A.J.T.; Jorgensen, H.R.M.; Severinsen, K.E.; Aliakbaryhosseinabadi, S.; Jiang, N.; Farina, D. Brain state-dependent stimulation boosts functional recovery following stroke. Ann. Neurol. 2019, 85, 84–95. [Google Scholar] [CrossRef]
- Millan, J.D.; Rupp, R.; Muller-Putz, G.R.; Murray-Smith, R.; Giugliemma, C.; Tangermann, M.; Vidaurre, C.; Cincotti, F.; Kubler, A.; Leeb, R.; et al. Combining brain-computer interfaces and assistive technologies: State-of-the-art and challenges. Front. Neurosci. 2010, 4, 161. [Google Scholar] [CrossRef]
- Guo, F.; Wang, J.Y.; Sun, Y.J.; Yang, A.L.; Zhang, R.H. Movement-related cortical potentials during muscle fatigue induced by upper limb submaximal isometric contractions. Neuroreport 2014, 25, 1136–1143. [Google Scholar] [CrossRef]
- Aliakbaryhosseinabadi, S.; Kostic, V.; Pavlovic, A.; Radovanovic, S.; Nlandu Kamavuako, E.; Jiang, N.; Petrini, L.; Dremstrup, K.; Farina, D.; Mrachacz-Kersting, N. Influence of attention alternation on movement-related cortical potentials in healthy individuals and stroke patients. Clin. Neurophysiol. 2017, 128, 165–175. [Google Scholar] [CrossRef] [Green Version]
- do Nascimento, O.F.; Nielsen, K.D.; Voigt, M. Relationship between plantar-flexor torque generation and the magnitude of the movement-related potentials. Exp. Brain Res. 2005, 160, 154–165. [Google Scholar] [CrossRef]
- Olsen, S.; Signal, N.; Niazi, I.K.; Rashid, U.; Alder, G.; Mawston, G.; Nedergaard, R.W.; Jochumsen, M.; Taylor, D. Peripheral electrical stimulation paired with movement-related cortical potentials improves isometric muscle strength and voluntary activation following stroke. Front. Hum. Neurosci. 2020, 14, 156. [Google Scholar] [CrossRef]
- Mrachacz-Kersting, N.; Jiang, N.; Stevenson, A.J.T.; Niazi, I.K.; Kostic, V.; Pavlovic, A.; Radovanovic, S.; Djuric-Jovicic, M.; Agosta, F.; Dremstrup, K.; et al. Efficient neuroplasticity induction in chronic stroke patients by an associative brain-computer interface. J. Neurophysiol. 2016, 115, 1410–1421. [Google Scholar] [CrossRef] [Green Version]
- Niazi, I.K.; Mrachacz-Kersting, N.; Jiang, N.; Demstrup, K.; Farina, D. Peripheral electrical stimulation triggered by self-paced detection of motor intention enhances motor evoked potentials. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 20, 595–604. [Google Scholar] [CrossRef]
- Mrachacz-Kersting, N.; Kristensen, S.R.; Niazi, I.K.; Farina, D. Precise temporal association between cortical potentials evoked by motor imagination and afference induces cortical plasticity. J. Physiol. 2012, 590, 1669–1682. [Google Scholar] [CrossRef] [Green Version]
- Niazi, I.K.; Navid, M.S.; Rashid, U.; Amjad, I.; Olsen, S.; Haavik, H.; Alder, G.; Kumari, N.; Signal, N.; Taylor, D.; et al. Associative cued asynchronous BCI induces cortical plasticity in stroke patients. Ann. Clin. Transl. Neurol. 2022, 9, 722–733. [Google Scholar] [CrossRef]
- Suchomel, T.J.; Nimphius, S.; Bellon, C.R.; Stone, M.H. The importance of muscular strength: Training considerations. Sports Med. 2018, 48, 765–785. [Google Scholar] [CrossRef]
- Luker, J.; Lynch, E.; Bernhardsson, S.; Bennett, L.; Bernhardt, J. Stroke survivors’ experiences of physical rehabilitation: A systematic review of qualitative studies. Arch. Phys. Med. Rehabil. 2015, 96, 1698–1708.e10. [Google Scholar] [CrossRef]
- Scrivener, K.; Dorsch, S.; McCluskey, A.; Schurr, K.; Graham, P.L.; Cao, Z.; Shepherd, R.; Tyson, S. Bobath therapy is inferior to task-specific training and not superior to other interventions in improving lower limb activities after stroke: A systematic review. J. Physiother. 2020, 66, 225–235. [Google Scholar] [CrossRef]
- Olsen, S. Rewiring the Brain after Stroke. A Novel Neuromodulatory Intervention to Improve Neuromuscular Control; Auckland University of Technology: Auckland, New Zealand, 2019. [Google Scholar]
- Callaghan Innovation. C Prize Finalist’s Journal: Rehabilitation Innovation Team; Callaghan Innovation: Auckland, New Zealand, 2017. Available online: https://www.callaghaninnovation.govt.nz/sites/all/files/cprize-2017-team-notebooks-web.pdf (accessed on 8 November 2022).
- Alder, G.; Signal, N.; Vandal, A.C.; Olsen, S.; Jochumsen, M.; Niazi, I.K.; Taylor, D. Investigating the intervention parameters of endogenous paired associative stimulation (ePAS). Brain Sci. 2021, 11, 224. [Google Scholar] [CrossRef]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial eeg dynamics including independent component analysis. J. Neurosci. Methods 2004, 134, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Calderon, J.; Luck, S.J. ERPLAB: An open-source toolbox for the analysis of event-related potentials. Front. Hum. Neurosci. 2014, 8, 213. [Google Scholar] [CrossRef] [Green Version]
- Rashid, U.; Niazi, I.K.; Signal, N.; Taylor, D. An EEG experimental study evaluating the performance of Texas Instruments ADS1299. Sensors 2018, 18, 3721. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, A.S.; Schlink, B.R.; Hairston, W.D.; König, P.; Ferris, D.P. Proposing metrics for benchmarking novel EEG technologies towards real-world measurements. Front. Hum. Neurosci. 2016, 10, 188. [Google Scholar] [CrossRef] [Green Version]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Degerman, A.; Rinne, T.; Pekkola, J.; Autti, T.; Jaaskelainen, I.P.; Sams, M.; Alho, K. Human brain activity associated with audiovisual perception and attention. Neuroimage 2007, 34, 1683–1691. [Google Scholar] [CrossRef]
- Euler, M.J.; Niermeyer, M.A.; Suchy, Y. Neurocognitive and neurophysiological correlates of motor planning during familiar and novel contexts. Neuropsychology 2016, 30, 109–119. [Google Scholar] [CrossRef]
- de Morree, H.M.; Klein, C.; Marcora, S.M. Perception of effort reflects central motor command during movement execution. Psychophysiology 2012, 49, 1242–1253. [Google Scholar] [CrossRef]
- Reiser, J.E.; Wascher, E.; Rinkenauer, G.; Arnau, S. Cognitive-motor interference in the wild: Assessing the effects of movement complexity on task switching using mobile EEG. Eur. J. Neurosci. 2020, 54, 8175–8195. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
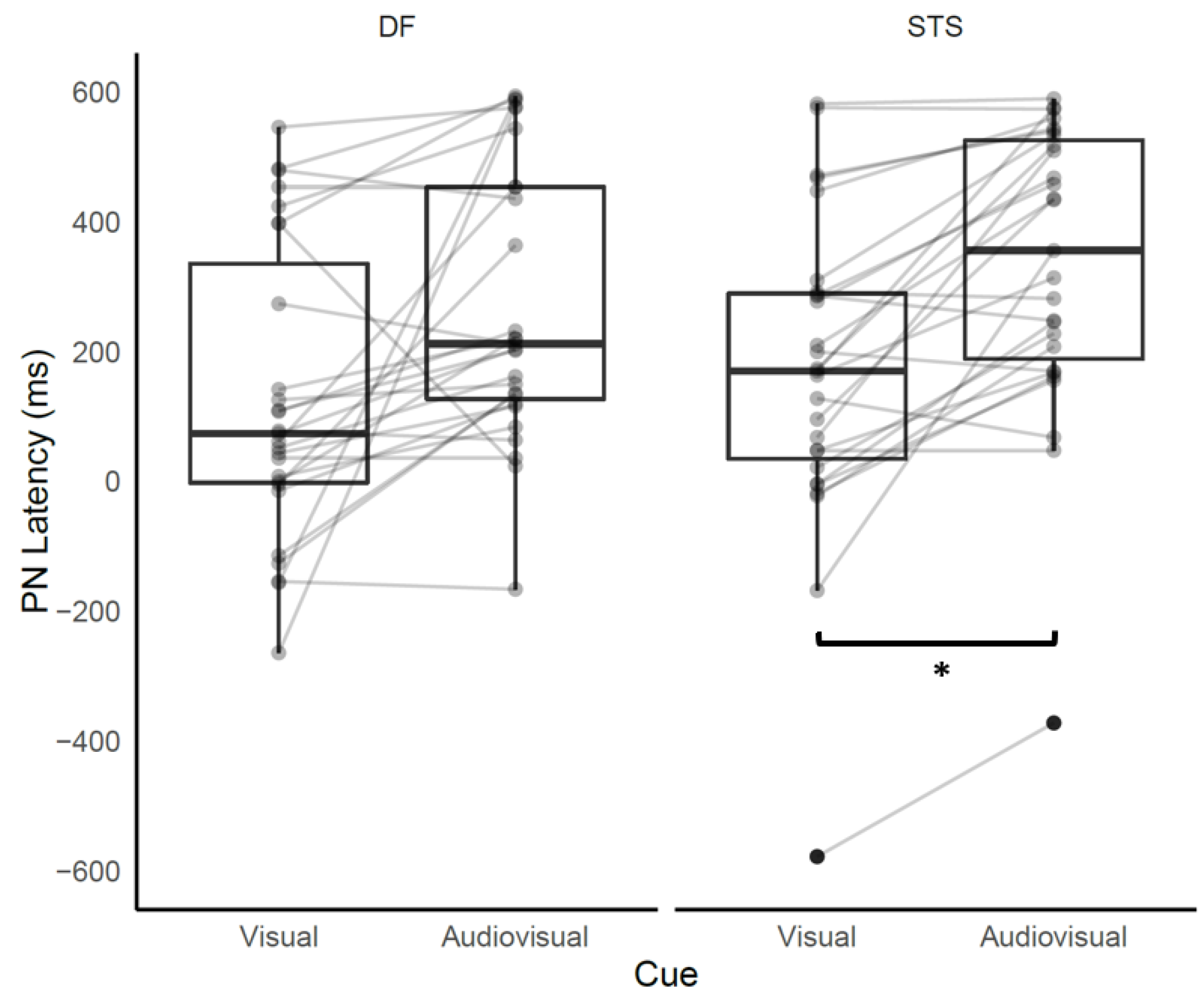
| Movement Condition | Group Mean (SD) ms | Post-Hoc Tests | Estimated Difference Mean (95% CI) |
|---|---|---|---|
| DFvisual | 128 (226) | ||
| DFaudiovisual | 271 (214) | DFaudiovisual – DFvisual | 143 (−8, 294) |
| DFauditory | 205 (336) | ||
| STSvisual | 168 (244) | ||
| STSaudiovisual | 334 (223) | STSaudiovisual – STSvisual | 166 (15, 317) * |
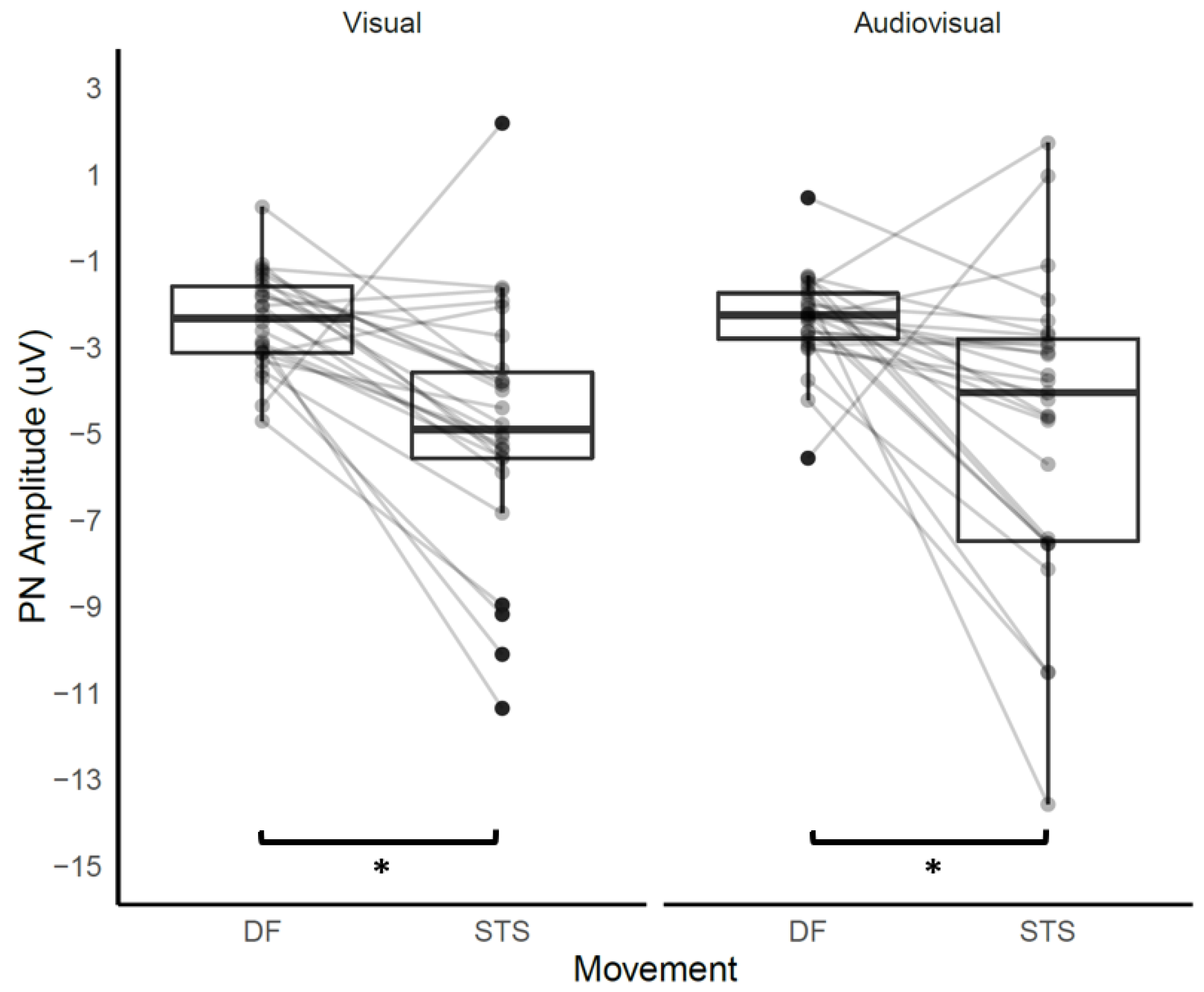
| Movement Condition | Group Mean (SD) µV | Post-Hoc Test | Estimated Difference Mean (95% CI) |
|---|---|---|---|
| DFvisual | 1.24 (18.83) | ||
| STSvisual | −2.33 (13.27) | STSvisual − DFvisual | 2.44 (1.31, 3.58) ** |
| DFaudiovisual | −2.35 (1.09) | ||
| STSaudiovisual | −4.75 (3.47) | STSaudiovisual − DFaudiovisual | 2.40 (1.29, 3.52) ** |
| DFauditory | −2.25 (2.11) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olsen, S.; Alder, G.; Rashid, U.; Ghani, U.; Boulle, N.; Signal, N.; Taylor, D.; Niazi, I.K. Characteristics of the Contingent Negative Variation during Lower Limb Functional Movement with an Audio-Visual Cue. Appl. Sci. 2023, 13, 2621. https://doi.org/10.3390/app13042621
Olsen S, Alder G, Rashid U, Ghani U, Boulle N, Signal N, Taylor D, Niazi IK. Characteristics of the Contingent Negative Variation during Lower Limb Functional Movement with an Audio-Visual Cue. Applied Sciences. 2023; 13(4):2621. https://doi.org/10.3390/app13042621
Chicago/Turabian StyleOlsen, Sharon, Gemma Alder, Usman Rashid, Usman Ghani, Nadia Boulle, Nada Signal, Denise Taylor, and Imran Khan Niazi. 2023. "Characteristics of the Contingent Negative Variation during Lower Limb Functional Movement with an Audio-Visual Cue" Applied Sciences 13, no. 4: 2621. https://doi.org/10.3390/app13042621