
A Digital 3D Retrospective Study Evaluating the Efficacy of Root Control during Orthodontic Treatment with Clear Aligners


Abstract
:1. Introduction
2. Materials and Methods
- -
- orthopantomography,
- -
- TMJ stratigraphy,
- -
- cross sections,
- -
- posteroanterior teleradiography,
- -
- superior and inferior submento-vertex
- -
- virtual reconstruction of right and left masseter muscles.
3. Results
4. Disscussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Simon, M.; Keilig, L.; Schwarze, J.; Jun, B.A.; Bourauel, C. Treatment outcome and efficacy of an aligner technique–regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health 2014, 11, 14–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, T.; Jiang, Y.; Chu, F.; Lu, P.; Tang, G. A cone-beam computed tomographic study evaluating the efficacy of incisor movement with clear aligners: Assessment of incisor pure tipping, controlled tipping, translation, and torque. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Lacruz, R.S.; Bermúdez de Castro, J.M.; Martinón-Torres, M.; O’Higgins, P.; Paine, M.L.; Carbonell, E.; Arsuaga, J.L.; Bromage, T.G. Facial morphogenesis of the earliest europeans. PLoS ONE 2013, 6, e65199. [Google Scholar] [CrossRef] [PubMed]
- Macrì, M.; Festa, F. Three-dimensional evaluation using CBCT of the mandibular asymmetry and the compensation mechanism in a growing patient: A case report. Front. Public Health 2022, 10, 921413. [Google Scholar] [CrossRef] [PubMed]
- Archambault, A.; Major, T.W.; Carey, J.P.; Heo, G.; Badawi, H.; Major, P.W. A comparison of torque expression between stainless steel, titanium molybdenum alloy and copper nickel titanium wires in metallic self-ligating brackets. Angle Orthod. 2010, 80, 884–889. [Google Scholar] [CrossRef]
- Rauch, D.E. Torque and its application to orthodontics. Am. J. Orthod. 1959, 45, 817–830. [Google Scholar] [CrossRef]
- Hemingway, R.; Williams, R.L.; Hunt, J.A.; Rudge, S.J. The influence of bracket type on the force delivery of Ni-Ti archwires. Eur. J. Orthod. 2001, 23, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Elhaddaoui, R.; Qoraich, H.S.; Bahije, L.; Zaoui, F. Orthodontic aligners and root resorption: A systematic review. Int. Orthod. 2017, 15, 1–12. [Google Scholar] [CrossRef]
- Li, Y.; Deng, S.; Mei, L.; Li, Z.; Zhang, X.; Yang, C.; Li, Y. Prevalence and severity of apical root resorption during orthodontic treatment with clear aligners and fixed appliances: A cone beam computed tomography study. Prog. Orthod. 2020, 21, 1. [Google Scholar] [CrossRef] [Green Version]
- Krieger, E.; Drechsler, T.; Schmidtmann, I.; Jacobs, C.; Haag, S.; Wehrbein, H. Apical root resorption during orthodontic treatment with aligners? A retrospective radiometric study. Head Face Med. 2013, 9, 21. [Google Scholar] [CrossRef]
- Iglesias-Linares, A.; Sonnenberg, B.; Solano, B.; Yañez-Vico, R.M.; Solano, E.; Lindauer, S.J.; Flores-Mir, C. Orthodontically induced external apical root resorption in patients treated with fixed appliances vs removable aligners. Angle Orthod. 2017, 87, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lascala, C.A.; Panella, J.; Marques, M.M. Analysis of the accuracy of linear measurements obtained by cone beam computed tomography (CBCT-NewTom). Dentomaxillofac. Radiol. 2004, 33, 291–294. [Google Scholar] [CrossRef]
- Dudic, A.; Giannopoulou, C.; Martinez, M.; Montet, X.; Kiliaridis, S. Diagnostic accuracy of digitized periapical radiographs validated against micro-computed tomography scanning in evaluating orthodontically induced apical root resorption. Eur. J. Oral Sci. 2008, 116, 467–472. [Google Scholar] [CrossRef]
- Lund, H.; Gröndahl, K.; Gröndahl, H. Cone beam computed tomography for assessment of root length and marginal bone level during orthodontic treatment. Angle Orthod. 2010, 80, 466–473. [Google Scholar] [CrossRef] [Green Version]
- Ren, H.; Chen, J.; Deng, F.; Zheng, L.; Liu, X.; Dong, Y. Comparison of cone-beam computed tomography and periapical radiography for detecting simulated apical root resorption. Angle Orthod. 2013, 83, 189–195. [Google Scholar] [CrossRef] [Green Version]
- Festa, F.; Rotelli, C.; Scarano, A.; Navarra, R.; Caulo, M.; Macrì, M. Functional Magnetic Resonance Connectivity in Patients with Temporomadibular Joint Disorders. Front. Neurol. 2021, 12, 629211. [Google Scholar] [CrossRef]
- Feragalli, B.; Rampado, O.; Abate, C.; Macrì, M.; Festa, F.; Stromei, F.; Caputi, S.; Guglielmi, G. Cone beam computed tomography for dental and maxillofacial imaging: Technique improvement and low-dose protocols. Radiol. Med. 2017, 122, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Nucera, R.; Ciancio, E.; Maino, G.; Barbera, S.; Imbesi, E.; Bellocchio, A.M. Evaluation of bone depth, cortical bone, and mucosa thickness of palatal posterior supra-alveolar insertion site for miniscrew placement. Prog. Orthod. 2022, 23, 18. [Google Scholar] [CrossRef] [PubMed]
- Macrì, M.; Toniato, E.; Murmura, G.; Varvara, G.; Festa, F. Midpalatal Suture Density as a Function of Sex and Growth-Pattern-Related Variability via CBCT Evaluations of 392 Adolescents Treated with a Rapid Maxillary Expander Appliance. Appl. Sci. 2022, 12, 2221. [Google Scholar] [CrossRef]
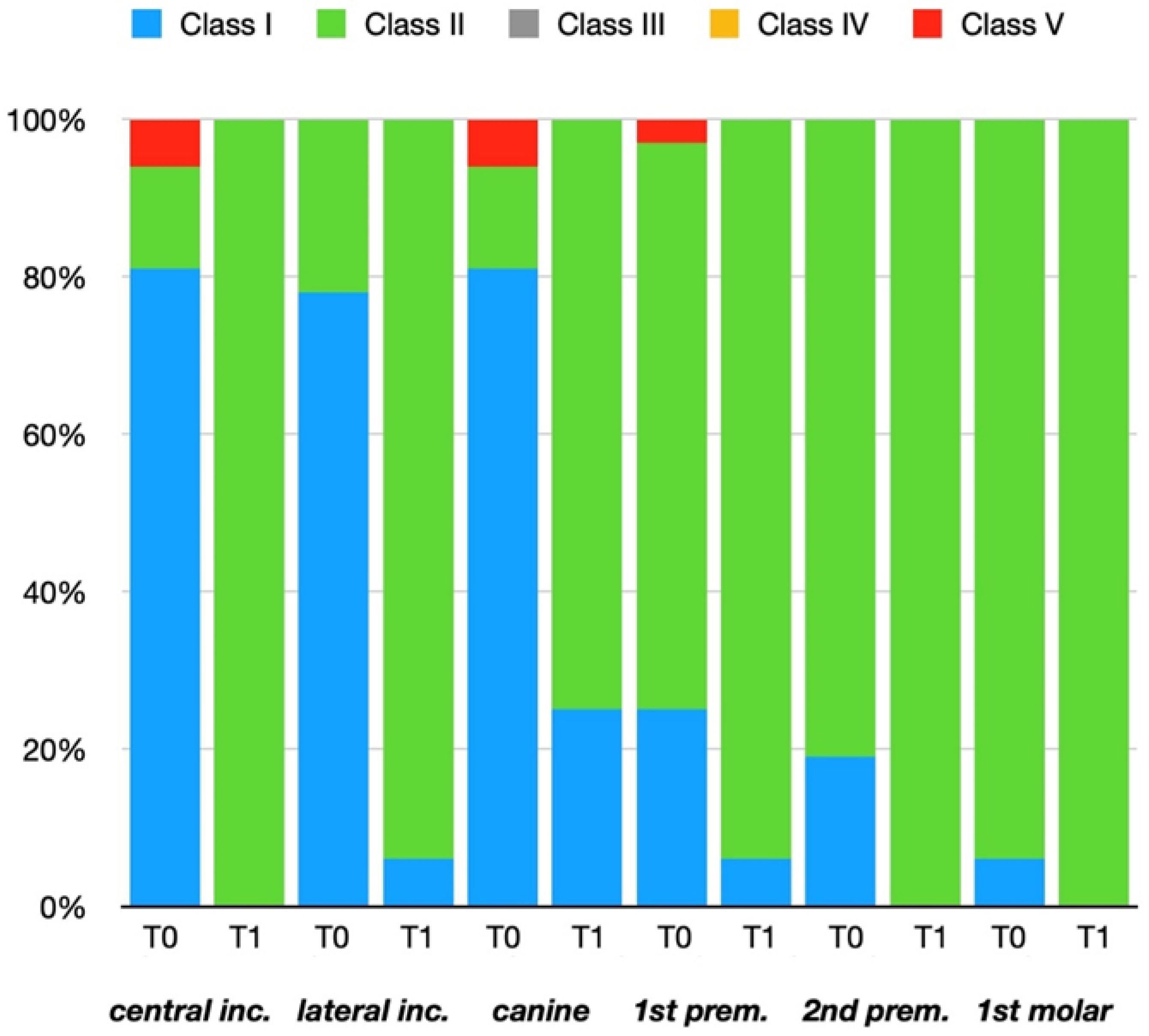
- Kan, J.Y.; Roe, P.; Rungcharassaeng, K.; Patel, R.D.; Waki, T.; Lozada, J.L. Classification of sagittal root position in relation to the anterior maxillary osseous housing for immediate implant placement: A cone beam computed tomography study. Int. J. Oral Maxillofac. Implant. 2011, 26, 873–876. [Google Scholar]
- Aman, C.; Azevedo, B.; Bednar, E.; Chandiramami, S.; German, D.; Nicholson, E.; Nicholson, K.; Scarfe, W.C. Apical root resorption during orthodontic treatment with clear aligners: A retrospective study using cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Tong, H.; Enciso, R.; Van Elslande, D.; Major, P.W.; Sameshima, G.T. A new method to measure mesiodistal angulation and faciolingual inclination of each whole tooth with volumetric cone-beam computed tomography images. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Guo, J. Efficiency of upper arch expansion with the Invisalign system. Angle Orthod. 2020, 90, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houle, J.P.; Piedade, L.; Todescan, R., Jr.; Pinheiro, F.H. The predictability of transverse changes with Invisalign. Angle Orthod. 2017, 87, 19–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.J.; He, L.; Guo, H.M.; Tian, J.; Bai, Y.X.; Li, S. Integrated three-dimensional digital assessment of accuracy of anterior tooth movement using clear aligners. Korean J. Orthod. 2015, 45, 275–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macrì, M.; Murmura, G.; Varvara, G.; Traini, T.; Festa, F. Clinical Performances and Biological Features of Clear Aligners Materials in Orthodontics. Front. Mater. 2022, 9, 819121. [Google Scholar] [CrossRef]
- Schupp, W.; Haubrich, J.; Neumann, I. Class II correction with the Invisalign system. J. Clin. Orthod. 2010, 44, 28–35. [Google Scholar] [PubMed]
- Hahn, W.; Zapf, A.; Dathe, H.; Fialka-Fricke, J.; Fricke-Zech, S.; Gruber, R.; Kubein-Meesenburg, D.; Sadat-Khonsari, R. Torquing an upper central incisor with aligners-acting forces and biomechanical principles. Eur. J. Orthod. 2010, 32, 607–613. [Google Scholar] [CrossRef] [Green Version]
- Castroflorio, T.; Garino, F.; Lazzaro, A.; Debernardi, C. Upper-incisor root control with Invisalign appliances. J. Clin. Orthod. 2013, 47, 346–351. [Google Scholar]
- Morina, E.; Eliades, T.; Pandis, N.; Jäger, A.; Bourauel, C. Torque expression of self-ligating brackets compared with conventional metallic, ceramic, and plastic brackets. Eur. J. Orthod. 2008, 30, 233–238. [Google Scholar] [CrossRef] [Green Version]
- Hennessy, J.; Garvey, T.; Al-Awadhi, E.A. A randomized clinical trial comparing mandibular incisor proclination produced by fixed labial appliances and clear aligners. Angle Orthod. 2016, 86, 706–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sfondrini, M.F.; Gandini, P.; Castroflorio, T.; Garino, F.; Mergati, L.; D’Anca, K.; Trovati, F.; Scribante, A. Buccolingual inclination control of upper central incisors of aligners: A comparison with conventional and self-ligating brackets. Biomed. Res. Int. 2018, 2018, 9341821. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Shao, J.; Li, S.; Al-Balaa, M.; Xia, L.; Li, H.; Hua, X. Volumetric cone-beam computed tomography evaluation and risk factor analysis of external apical root resorption with clear aligner therapy. Angle Orthod. 2021, 91, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Pastro, J.D.V.; Nogueira, A.C.A.; Salvatore de Freitas, K.M.; Valarelli, F.P.; Cançado, R.H.; de Oliveira, R.C.G.; de Oliveira, R.C.G. Factors associated to apical root resorption after orthodontic treatment. Open Dent. J. 2018, 12, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, D.J.; Willes, M.G.; Sameshima, G.T. A finite element model of apical force distribution from orthodontic tooth movement. Angle Orthod. 2001, 71, 127–131. [Google Scholar] [CrossRef]
- Lund, H.; Gröndahl, K.; Hansen, K.; Gröndahl, H.G. Apical root resorption during orthodontic treatment. A prospective study using cone beam CT. Angle Orthod. 2012, 82, 480–487. [Google Scholar] [CrossRef] [Green Version]
- Eissa, O.; Carlyle, T.; El-Bialy, T. Evaluation of root length following treatment with clear aligners and two different fixed orthodontic appliances. A pilot study. J. Orthod. Sci. 2018, 7, 11. [Google Scholar] [CrossRef]
- Dudic, A.; Giannopoulou, C.; Leuzinger, M.; Kiliaridis, S. Detection of apical root resorption after orthodontic treatment by using panoramic radiography and cone-beam computed tomography of super-high resolution. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 434–437. [Google Scholar] [CrossRef]
- American Academy of Oral and Maxillofacial Radiology. Clinical recommendations regarding use of cone beam computed tomography in orthodontics. [corrected]. Position statement by the American Academy of Oral and Maxillofacial Radiology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 238–257. [Google Scholar] [CrossRef] [Green Version]
- Yeung, A.W.; Jacobs, R.; Bornstein, M.M. Novel low-dose protocols using cone beam computed tomography in dental medicine: A review focusing on indications, limitations, and future possibilities. Clin. Oral Investig. 2019, 23, 2573–2581. [Google Scholar] [CrossRef]
- Cheng, Y.; Gao, J.; Fang, S.; Wang, W.; Ma, Y.; Jin, Z. Torque movement of the upper anterior teeth using a clear aligner in cases of extraction: A finite element study. Prog. Orthod. 2022, 23, 26. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tooth | Measurements T0 (n°) | Measurements T1 (n°) | Tot. Measurements (n°) |
|---|---|---|---|
| Central incisor | 56 | 56 | 112 |
| Lateral incisor | 56 | 56 | 112 |
| Canine | 56 | 56 | 112 |
| First premolar | 56 | 56 | 112 |
| Second premolar | 56 | 56 | 112 |
| First molar | 56 | 56 | 112 |
| From central incisor to first molar | 336 | 336 | 672 |
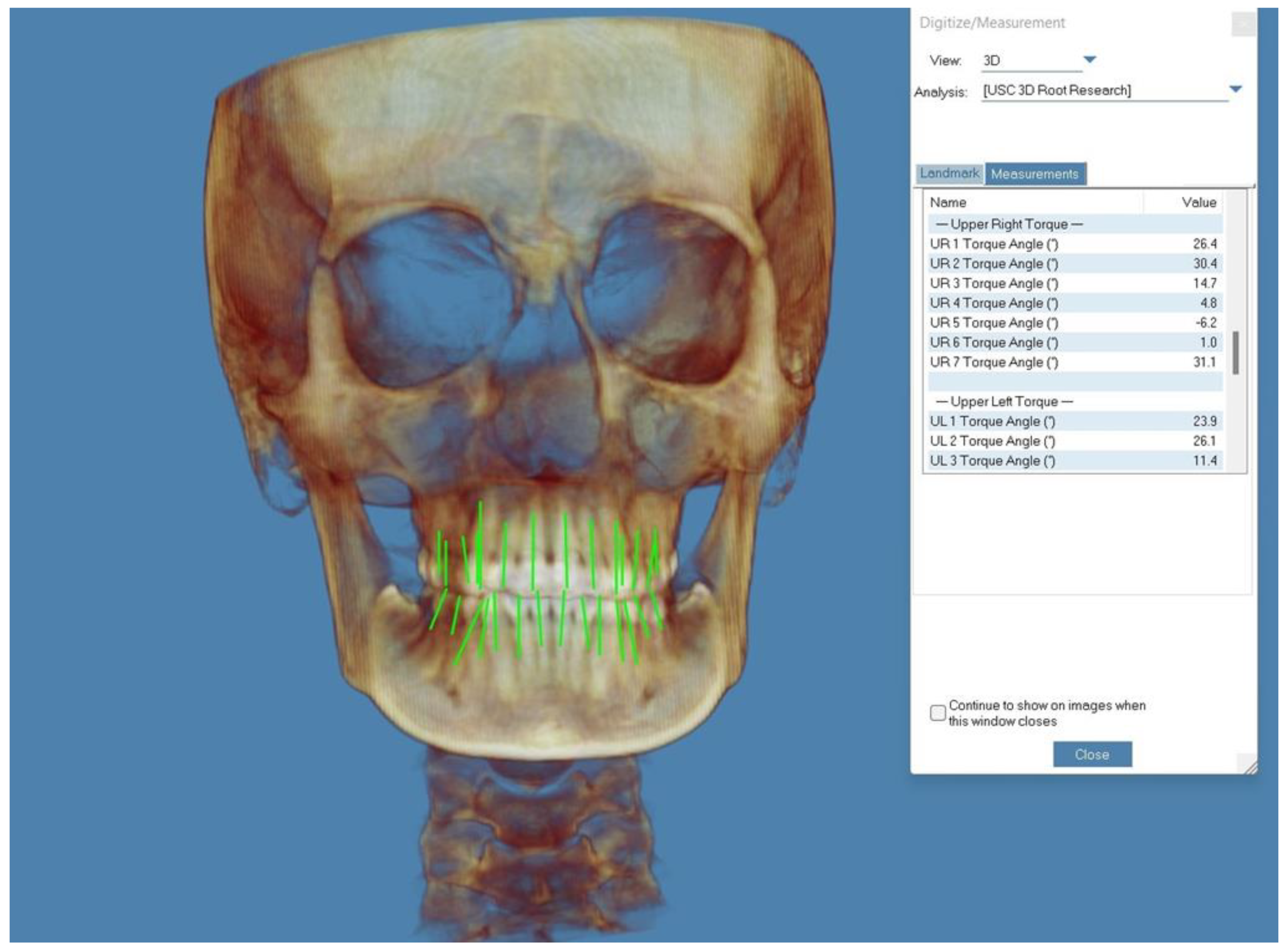
| Tooth | Torque Variation (°) (Mean ± SD) | Range (°) | Torque Variation (%) (Mean ± SD) | Range (%) | Tp | Confidence Interval | p-Value |
|---|---|---|---|---|---|---|---|
| Central incisor | 3.26 ± 1.95 | 9.50–0.10 | 22.82 ± 12.62 | 66.66–1.20 | 12.49 | 3.78–2.74 | * |
| Lateral incisor | 2.57 ± 1.86 | 7.50–0.40 | 17.74 ± 9.09 | 48.68–7.03 | 10.31 | 3.07–2.07 | * |
| Canine | 1.53 ± 0.89 | 3.90–0 | 14.38 ± 6.52 | 32.05–0 | 12.84 | 1.77–1.29 | * |
| First premolar | 0.53 ± 0.36 | 1.10–0 | 8.59 ± 6.27 | 20.75–0 | 8.24 | 0.65–0.39 | * |
| Second premolar | 0.02 ± 0.07 | 0.20–−0.20 | 0.25 ± 0.91 | 2.74–−2.70 | 1.53 | 0.04–0 | NS |
| First molar | 0.01 ± 0.05 | 0.10–−0.20 | 0.15 ± 0.73 | 1.49–−2.70 | 1.28 | 0.03–0 | NS |
| Tooth | Torque Variation (°) (Mean ± SD) | Range (°) | Torque Variation (%) (Mean ± SD) | Range (%) | Tp | Confidence Interval | p-Value |
|---|---|---|---|---|---|---|---|
| Central incisor | 2.97 ± 2.53 | 9.00–0.20 | 22.63 ± 11.58 | 67.92–3.17 | 8.78 | 3.65–2.29 | * |
| Lateral incisor | 2.07 ± 2.16 | 8.10–0 | 12.95 ± 11.09 | 54.69–0 | 7.15 | 2.65–1.49 | * |
| Canine | 0.94 ± 0.95 | 3.40–0 | 7.82 ± 8.16 | 33.33–0 | 7.43 | 1.19–0.69 | * |
| First premolar | 0.18 ± 0.13 | 0.50–0 | 1.92 ± 1.67 | 6.25–0 | 7.67 | 0.26–0.13 | * |
| Second premolar | 0.02 ± 0.07 | 0.10–−0.20 | 0.18 ± 0.79 | 1.41–−2.47 | 1.31 | 0.04–0 | NS |
| First molar | 0.02 ± 0.06 | 0.10–−0.10 | 0.21 ± 0.84 | 1.30–−1.43 | 1.65 | 0.04–0 | NS |
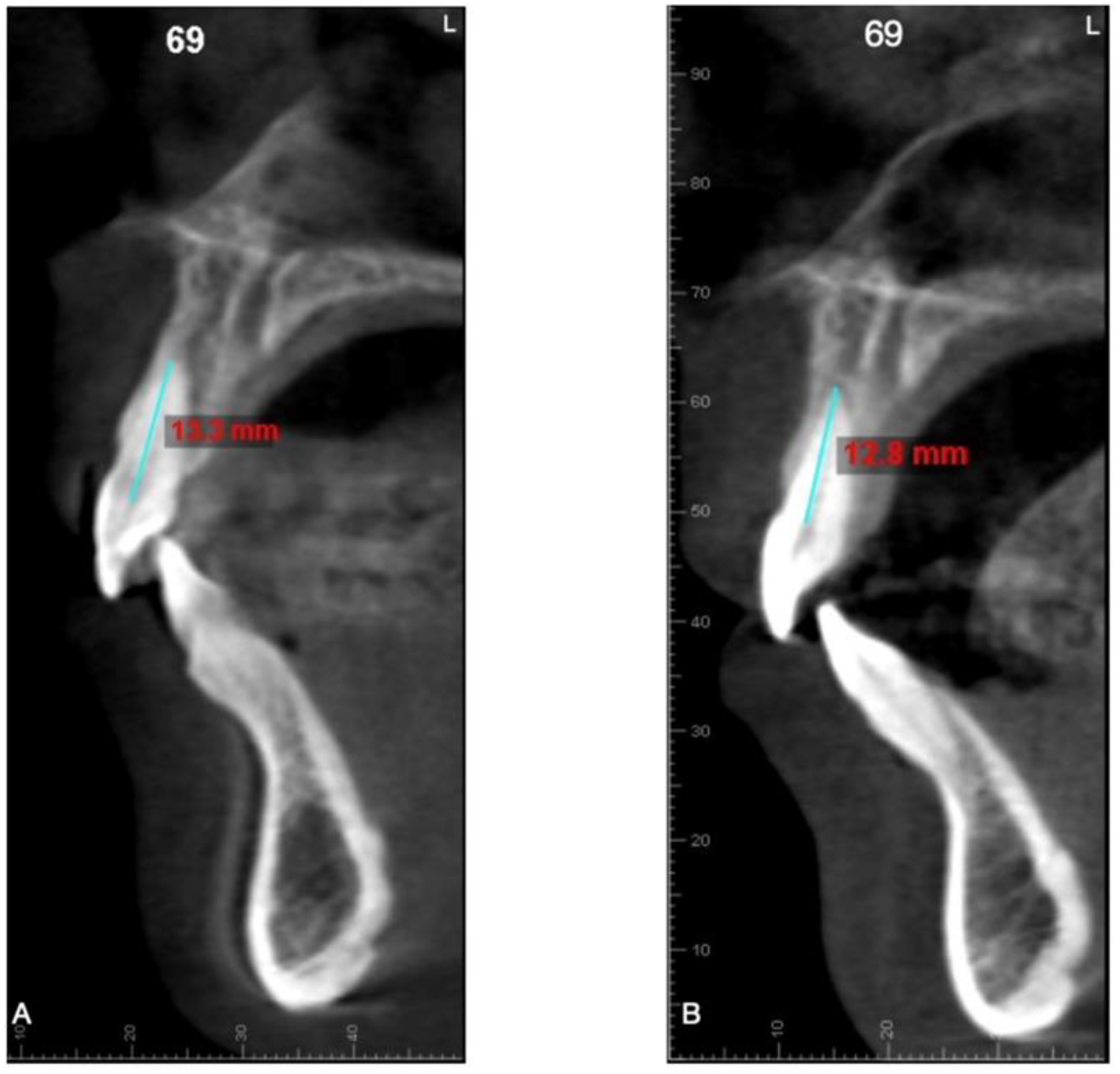
| Tooth | Changes in Root Length (mm) (Mean ± SD) | Range (mm) | Changes in Root Length (%) (Mean ± SD) | Range (%) | Tp | Confidence Interval | p-Value |
|---|---|---|---|---|---|---|---|
| Central incisor | −0.43 ± 0.27 | −1.10–0.10 | −3.27 ± 2.07 | −8.53–0.76 | 8.92 | 0.53–0.33 | * |
| Lateral incisor | −0.53 ± 0.38 | −1.50–0.10 | −4.03 ± 2.82 | −10.79–0.78 | 7.88 | 0.66–0.39 | * |
| Canine | −0.14 ± 0.13 | −0.60–0 | −0.83 ± 0.75 | −3.57–0 | 6.28 | 0.19–0.09 | * |
| First premolar | −0.08 ± 0.66 | −0.30–0 | −0.56 ± 0.42 | −2.20–0 | 8.31 | 0.11–0.10 | * |
| Second premolar | −0.003 ± 0.02 | −0.10–0 | −0.02 ± 0.13 | −0.70–0 | 1 | 0.004–0 | NS |
| First molar | −0.003 ± 0.01 | −0.10–0 | −0.02 ± 0.12 | −0.68–0 | 1 | 0.004–0 | NS |
| Tooth | Changes in Root Length (mm) (Mean ± SD) | Range (mm) | Changes in Root Length (%) (Mean ± SD) | Range (%) | Tp | Confidence Interval | p-Value |
|---|---|---|---|---|---|---|---|
| Central incisor | −0.20 ± 0.28 | −0.80–0 | −1.58 ± 1.77 | −6.20–0 | 4.98 | 0.28–0.12 | * |
| Lateral incisor | −0.09 ± 0.11 | −0.50–0 | −0.67 ± 0.79 | −3.60–0 | 4.71 | 0.13–0.05 | * |
| Canine | −0.08 ± 0.07 | −0.20–0 | −0.50 ± 0.41 | −1.31–0 | 6.70 | 0.10–0.05 | * |
| First premolar | −0.003 ± 0.01 | −0.10–0 | −0.02 ± 0.13 | −0.71–0 | 1 | 0.004–0 | NS |
| Second premolar | −0.003 ± 0.02 | −0.10–0 | −0.02 ± 0.13 | −0.75–0 | 1 | 0.004–0 | NS |
| First molar | −0.003 ± 0.02 | −0.10–0 | −0.03 ± 0.14 | −0.80–0 | 1 | 0.004–0 | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macrì, M.; Medori, S.; Varvara, G.; Festa, F. A Digital 3D Retrospective Study Evaluating the Efficacy of Root Control during Orthodontic Treatment with Clear Aligners. Appl. Sci. 2023, 13, 1540. https://doi.org/10.3390/app13031540
Macrì M, Medori S, Varvara G, Festa F. A Digital 3D Retrospective Study Evaluating the Efficacy of Root Control during Orthodontic Treatment with Clear Aligners. Applied Sciences. 2023; 13(3):1540. https://doi.org/10.3390/app13031540
Chicago/Turabian StyleMacrì, Monica, Silvia Medori, Giuseppe Varvara, and Felice Festa. 2023. "A Digital 3D Retrospective Study Evaluating the Efficacy of Root Control during Orthodontic Treatment with Clear Aligners" Applied Sciences 13, no. 3: 1540. https://doi.org/10.3390/app13031540