

Rationale and Design of a Wearable Cardiopulmonary Monitoring System for Improving the Efficiency of Critical Care Monitoring

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire for Intensive Care Unit Medical Staff
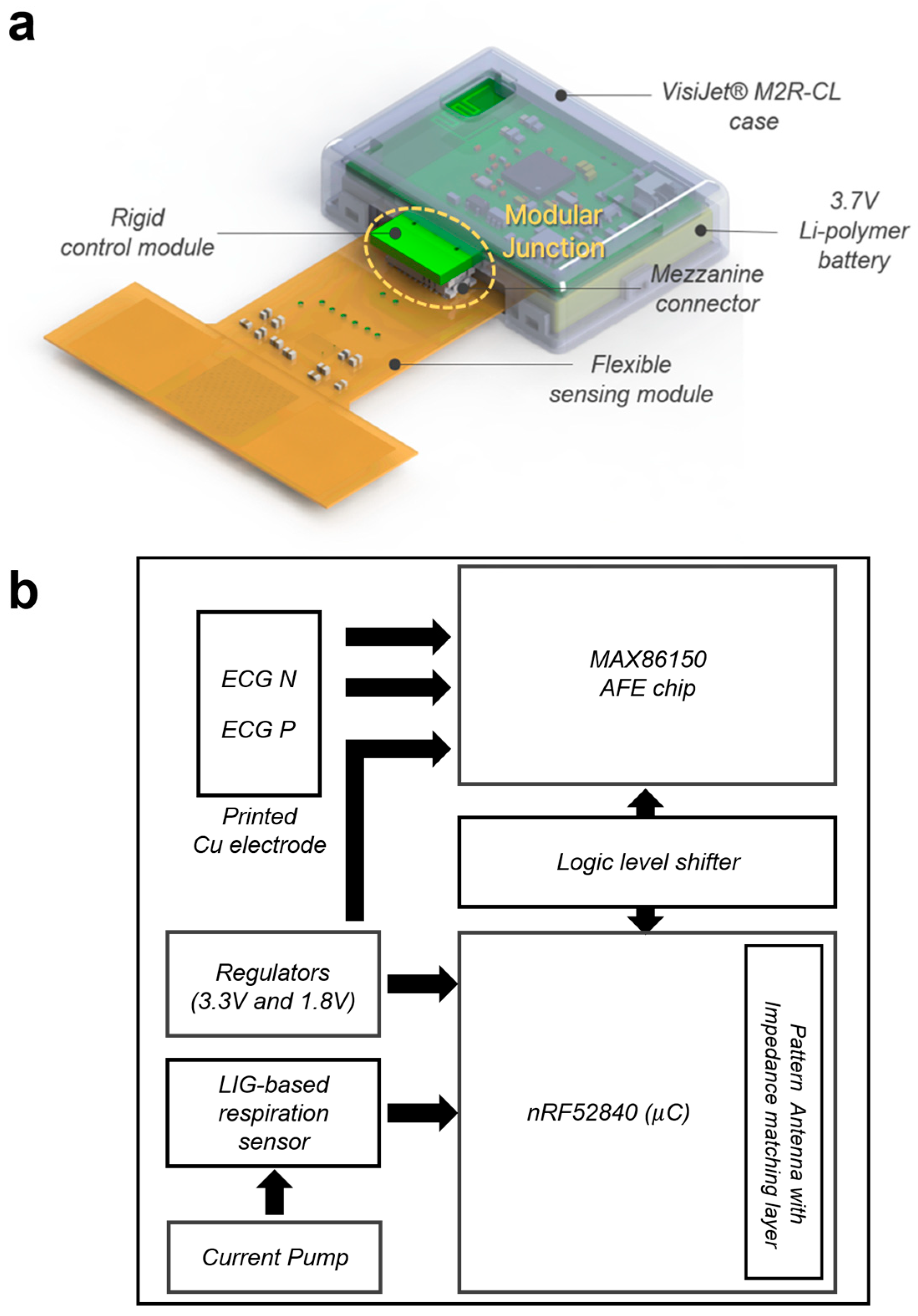
2.3. Developing an Integrated Wearable Cardiopulmonary Device for a Patient Monitoring System
2.4. Data Collection
2.5. Statistical Analysis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kang, S.; Pradana Rachim, V.; Baek, J.H.; Lee, S.Y.; Park, S. A flexible patch-type strain sensor based on polyaniline for continuous monitoring of pulse waves. IEEE Access 2020, 8, 152105–152115. [Google Scholar] [CrossRef]
- Ding, X.; Cao, H.; Zhang, X.; Li, M.; Liu, Y. Large scale triboelectric nanogenerator and self-powered flexible sensor for human sleep monitoring. Sensors 2018, 18, 1713. [Google Scholar] [CrossRef] [PubMed]
- Bariya, M.; Nyein, H.Y.Y.; Javey, A. Wearable sweat sensors. Nat. Electron. 2018, 1, 160–171. [Google Scholar] [CrossRef]
- Yoon, S.; Sim, J.K.; Cho, Y.H. A flexible and wearable human stress monitoring patch. Sci. Rep. 2016, 6, 23468. [Google Scholar] [CrossRef] [PubMed]
- Rachim, V.P.; Lee, J.; Kim, Y.C.; Oh, J.; Jeong, U.; Park, S. A scalable laser-centric fabrication of an epidermal cardiopulmonary patch. Adv. Mater. Technol. 2022, 7, 2200242. [Google Scholar] [CrossRef]
- Liu, Y.; Norton, J.J.S.; Qazi, R.; Zou, Z.; Ammann, K.R.; Liu, H.; Yan, L.; Tran, P.L.; Jang, K.-I.; Lee, J.W.; et al. Epidermal mechano-acoustic sensing electronics for cardiovascular diagnostics and human-machine interfaces. Sci. Adv. 2016, 2, e1601185. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and other Societies on cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention and Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Breteler, M.J.M.; KleinJan, E.J.; Dohmen, D.A.J.; Leenen, L.P.H.; van Hillegersberg, R.; Ruurda, J.P.; van Loon, K.; Blokhuis, T.J.; Kalkman, C.J. Vital signs monitoring with wearable sensors in high-risk surgical patients: A clinical validation study. Anesthesiology 2020, 132, 424–439. [Google Scholar] [CrossRef] [PubMed]
- Downey, C.; Randell, R.; Brown, J.; Jayne, D.G. Continuous versus intermittent vital signs monitoring using a wearable, wireless patch in patients admitted to surgical wards: Pilot cluster randomized controlled trial. J. Med. Internet Res. 2018, 20, e10802. [Google Scholar] [CrossRef]
- Downey, C.L.; Chapman, S.; Randell, R.; Brown, J.M.; Jayne, D.G. The impact of continuous versus intermittent vital signs monitoring in hospitals: A systematic review and narrative synthesis. Int. J. Nurs. Stud. 2018, 84, 19–27. [Google Scholar] [CrossRef]
- Cardona-Morrell, M.; Prgomet, M.; Lake, R.; Nicholson, M.; Harrison, R.; Long, J.; Westbrook, J.; Braithwaite, J.; Hillman, K. Vital signs monitoring and nurse-patient interaction: A qualitative observational study of hospital practice. Int. J. Nurs. Stud. 2016, 56, 9–16. [Google Scholar] [CrossRef]
- Bøgh, N.; Agger, P.; Omann, C.; Skov, M.N.; Laustsen, C.; Wang, T.; Pedersen, M. New device for noninvasive telemetric monitoring of vital signs in healthy and newly operated piglets. J. Am. Assoc. Lab. Anim. Sci. 2020, 59, 90–93. [Google Scholar] [CrossRef]
- Poncette, A.S.; Wunderlich, M.M.; Spies, C.; Heeren, P.; Vorderwülbecke, G.; Salgado, E.; Kastrup, M.; Feufel, M.; Balzer, F. Patient monitoring alarms in an intensive care unit: Observational study with do-it-yourself instructions. J. Med. Internet Res. 2021, 23, e26494. [Google Scholar] [CrossRef]
- Asadi, N.; Salmani, F.; Asgari, N.; Salmani, M. Alarm fatigue and moral distress in ICU nurses in COVID-19 pandemic. BMC Nurs. 2022, 21, 125. [Google Scholar] [CrossRef]
- Akturan, S.; Güner, Y.; Tuncel, B.; Üçüncüoğlu, M.; Kurt, T. Evaluation of alarm fatigue of nurses working in the COVID-19 Intensive Care Service: A mixed methods study. J. Clin. Nurs. 2022, 31, 2654–2662. [Google Scholar] [CrossRef]
- Sun, B.; McCay, R.N.; Goswami, S.; Xu, Y.; Zhang, C.; Ling, Y.; Lin, J.; Yan, Z. Gas-Permeable, Multifunctional On-Skin Electronics Based on Laser-Induced Porous Graphene and Sugar-Templated Elastomer Sponges. Adv. Mater. 2018, 30, e1804327. [Google Scholar] [CrossRef]
- Yang, X.; Wang, S.; Liu, M.; Li, L.; Zhao, Y.; Wang, Y.; Bai, Y.; Lu, Q.; Xiong, Z.; Feng, S.; et al. All-Nanofiber-Based Janus Epidermal Electrode with Directional Sweat Permeability for Artifact-Free Biopotential Monitoring. Small 2022, 18, 2106477. [Google Scholar] [CrossRef]
- Zhou, W.; Yao, S.; Wang, H.; Du, Q.; Ma, Y.; Zhu, Y. Gas-Permeable, Ultrathin, Stretchable Epidermal Electronics with Porous Electrodes. ACS Nano 2020, 14, 5798–5805. [Google Scholar] [CrossRef]
- Chowdhury, M.E.H.; Khandakar, A.; Alzoubi, K.; Mansoor, S.; MTahir, A.; Reaz, M.B.I.; Al-Emadi, N. Real-Time Smart-Digital Stethoscope System for Heart Diseases Monitoring. Sensors 2019, 19, 2781. [Google Scholar] [CrossRef]
- Nakamura, Y.; Matsuda, Y.; Arakawa, Y.; Yasumoto, K. WaistonBelt X: A Belt-Type Wearable Device with Sensing and Intervention toward Health Behavior Change. Sensors 2019, 19, 4600. [Google Scholar] [CrossRef]
- Roudjane, M.; Bellemare-Rousseau, S.; Drouin, E.; Bélanger-Huot, B.; Dugas, M.; Miled, A.; Messaddeq, Y. Smart T-Shirt Based on Wireless Communication Spiral Fiber Sensor Array for Real-Time Breath Monitoring: Validation of the Technology. IEEE Sens. J. 2020, 20, 10841–10850. [Google Scholar] [CrossRef]
- Tscholl, D.W.; Handschin, L.; Rössler, J.; Weiss, M.; Spahn, D.R.; Nöthiger, C.B. It’s not you, it’s the design—Common problems with patient monitoring reported by anesthesiologists: A mixed qualitative and quantitative study. BMC Anesthesiol. 2019, 19, 87. [Google Scholar] [CrossRef]
- Lubitz, S.A.; Faranesh, A.Z.; Atlas, S.J.; McManus, D.D.; Singer, D.E.; Pagoto, S.; Pantelopoulos, A.; Foulkes, A.S. Rationale and design of a large population study to validate software for the assessment of atrial fibrillation from data acquired by a consumer tracker or smartwatch: The Fitbit heart study. Am. Heart J. 2021, 238, 16–26. [Google Scholar] [CrossRef]
- Rush, B.; Celi, L.A.; Stone, D.J. Applying machine learning to continuously monitored physiological data. J. Clin. Monit. Comput. 2019, 33, 887–893. [Google Scholar] [CrossRef]
- Han, C.; Song, Y.; Lim, H.S.; Tae, Y.; Jang, J.-H.; Lee, B.T.; Lee, Y.; Bae, W.; Yoon, D. Automated detection of acute myocardial infarction using asynchronous electrocardiogram signals-preview of implementing artificial intelligence with multichannel electrocardiographs obtained from smartwatches: Retrospective study. J. Med. Internet Res. 2021, 23, e31129. [Google Scholar] [CrossRef]
- Yoon, S.; Kim, T.; Roh, T.; Chang, H.; Hwang, S.Y.; Yoon, H.; Shin, T.G.; Sim, M.S.; Jo, I.J.; Cha, W.C. Twelve-lead electrocardiogram acquisition with a patchy-type wireless device in ambulance transport: Simulation-based randomized controlled trial. JMIR MHealth UHealth 2021, 9, e24142. [Google Scholar] [CrossRef]
- Morgado Areia, C.; Santos, M.; Vollam, S.; Pimentel, M.; Young, L.; Roman, C.; Ede, J.; Piper, P.; King, E.; Gustafson, O.; et al. A Chest patch for continuous vital sign monitoring: Clinical validation study during movement and controlled hypoxia. J. Med. Internet Res. 2021, 23, e27547. [Google Scholar] [CrossRef]
- Gardner, M.; Randhawa, S.; Malouf, G.; Reynolds, K. A wearable ballistocardiography device for estimating heart rate during positive airway pressure therapy: Investigational study among the general population. JMIR Cardio 2021, 5, e26259. [Google Scholar] [CrossRef]
- Nazir, S.; Pateau, V.; Bert, J.; Clement, J.; Fayad, H.; L’Her, E.; Visvikis, D. Surface imaging for real-time patient respiratory function assessment in intensive care. Med. Phys. 2021, 48, 142–155. [Google Scholar] [CrossRef]
- Khunlertkit, A.; Carayon, P. Contributions of tele-intensive care unit (Tele-ICU) technology to quality of care and patient safety. J. Crit. Care 2013, 28, 315.e1–315.e12. [Google Scholar] [CrossRef]
- Ha, T.; Tran, J.; Liu, S.; Jang, H.; Jeong, H.; Mitbander, R.; Huh, H.; Qiu, Y.; Duong, J.; Wang, R.L.; et al. A chest-laminated ultrathin and stretchable e-tattoo for the measurement of electrocardiogram, seismocardiogram, and cardiac time intervals. Adv. Sci. 2019, 6, 1900290. [Google Scholar] [CrossRef]
- Poncette, A.S.; Spies, C.; Mosch, L.; Schieler, M.; Weber-Carstens, S.; Krampe, H.; Balzer, F. Clinical Requirements of Future Patient Monitoring in the Intensive Care Unit: Qualitative Study. JMIR Med. Inform. 2019, 7, e13064. [Google Scholar] [CrossRef]
- Shahidul Islam, M.; Islam, M.T.; Almutairi, A.F.; Beng, G.K.; Misran, N.; Amin, N. Monitoring of the Human Body Signal through the Internet of Things (IoT) Based LoRa Wireless Network System. Appl. Sci. 2019, 9, 1884. [Google Scholar] [CrossRef]
- Sanfilippo, F.; Pettersen, K.Y. A sensor fusion wearable health-monitoring system with haptic feedback. In Proceedings of the 2015 11th International Conference on Innovations in Information Technology (IIT), Dubai, United Arab Emirates, 1–3 November 2015; pp. 262–266. [Google Scholar] [CrossRef]
- Ren, Y.; Sun, X.; Liu, J. Advances in Liquid Metal-Enabled Flexible and Wearable Sensors. Micromachines 2020, 11, 200. [Google Scholar] [CrossRef]
- Okutani, C.; Yokota, T.; Someya, T. Interconnected Heat-Press-Treated Gold Nanomesh Conductors for Wearable Sensors. ACS Appl. Nano Mater. 2020, 3, 200. [Google Scholar] [CrossRef]
- Myers, A.C.; Huang, H.; Zhu, Y. Wearable silver nanowire dry electrodes for electrophysiological sensing. RSC Adv. 2015, 5, 1848–1854. [Google Scholar] [CrossRef]
- Huang, L.; Su, J.; Song, Y.; Ye, R. Laser-induced graphene: En route to smart sensing. Nanomicro. Lett. 2020, 12, 157. [Google Scholar] [CrossRef]
- Ye, R.; James, D.K.; Tour, J.M. Laser-induced graphene: From discovery to translation. Adv. Mater. 2019, 31, e1803621. [Google Scholar] [CrossRef]
- Ye, R.; James, D.K.; Tour, J.M. Laser-induced graphene. Acc. Chem. Res. 2018, 51, 1609–1620. [Google Scholar] [CrossRef]
- Yi, M.; Shen, Z. A review on mechanical exfoliation for the scalable production of graphene. J. Mater. Chem. A 2015, 3, 11700–11715. [Google Scholar] [CrossRef]
- Parvez, K.; Yang, S.; Feng, X.; Müllen, K. Exfoliation of graphene via wet chemical routes. Synth. Met. 2015, 210, 123–132. [Google Scholar] [CrossRef]
- Jeerapan, I.; Poorahong, S. Review—Flexible and stretchable electrochemical sensing systems: Materials, energy sources, and integrations. J. Electrochem. Soc. 2020, 167, 037573. [Google Scholar] [CrossRef]
- Choi, J.; Ahmed, B.; Gutierrez-Osuna, R. Development and evaluation of an ambulatory stress monitor based on wearable sensors. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 279–286. [Google Scholar] [CrossRef]
- Meziane, N.; Webster, J.G.; Attari, M.; Nimunkar, A.J. Dry electrodes for electrocardiography. Physiol. Meas. 2013, 34, R47–R69. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Jang, S.G.; Moon, S.; Kim, J.; Park, H.K.; Kim, H.S.; Park, S.; Jeong, U. Air-permeable waterproofing electrocardiogram patch to monitor full-day activities for multiple days. Adv. Healthc. Mater 2022, 11, e2102703. [Google Scholar] [CrossRef]
- Chen, Y.H.; De Beeck, M.O.; Vanderheyden, L.; Carrette, E.; Mihajlović, V.; Vanstreels, K.; Grundlehner, B.; Gadeyne, S.; Boon, P.; Van Hoof, C. Soft, comfortable polymer dry electrodes for high quality ECG and EEG recording. Sensors 2014, 14, 23758–23780. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Yamamoto, D.; Takada, M.; Naito, H.; Arie, T.; Akita, S.; Takei, K. Efficient skin temperature sensor and stable gel-less sticky ECG sensor for a wearable flexible healthcare patch. Adv. Healthc. Mater. 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Hwang, Y.M.; Sung, M.K.; Kim, S.O. Impact of de novo tachyarrhythmias in patients with prior acute coronary syndrome. Medicine 2022, 101, e29685. [Google Scholar] [CrossRef]
- Orvin, K.; Eisen, A.; Goldenberg, I.; Gottlieb, S.; Kornowski, R.; Matetzky, S.; Golovchiner, G.; Kuznietz, J.; Gavrielov-Yusim, N.; Segev, A.; et al. Outcome of contemporary acute coronary syndrome complicated by ventricular tachyarrhythmias. Europace 2016, 18, 219–226. [Google Scholar] [CrossRef]
- Holden, J.; Fernie, G.R.; Soto, M. An assessment of a system to monitor the activity of patients in a rehabilitation programme. Prosthet. Orthot. Int. 1979, 3, 99–102. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Conventional | Proposed | |
|---|---|---|
| Weight | Bulky (~tens of kilograms) | Lightweight (~5 g) |
| Portability | Hard (non-portable) | Easy |
| Presence of cables | Yes | No |
| Integrity | No | Yes (single device mounted on the chest) |
| Synchronization of signals | Hard (signals are obtained from separate devices) | Easy |
| Survey for ICU Medical Staff | Strongly Agree | Agree | Neutral | Disagree | Strongly Disagree |
|---|---|---|---|---|---|
| Awareness of ICU monitoring equipment currently in use | |||||
| I think the current ICU monitoring equipment is optimized for patients and medical staff. | |||||
| It is convenient to use the current ICU monitoring equipment. | |||||
| I am satisfied with the current ICU monitoring system; there is nothing to supplement. | |||||
| The inconvenience of the currently used ICU monitoring equipment | |||||
| There are many unnecessary alarms (device noise, false alarms, incorrect settings, and so on). | |||||
| Many cables are connected to the sensor, which is inconvenient when applied. | |||||
| Interlocking or compatibility with other devices is difficult (ventilator, DC device, and EMR linkage). | |||||
| It is difficult to use patient monitoring equipment (it takes learning time, responding to alarms is inconvenient, and so on). | |||||
| I hope that ICU monitoring equipment will be improved as follows. | |||||
| Using a wireless sensor (without cable) | |||||
| Unnecessary alarms are reduced. | |||||
| In-hospital remote monitoring system (mobile phone/tablet PC) | |||||
| Other ideas? | |||||
| What are your thoughts on using new digital equipment to make ICU monitoring more straightforward and accurate? | |||||
| I want to try it as soon as possible. | |||||
| I would like to apply new equipment more slowly (skilled use seems complicated). | |||||
| New digital equipment is unlikely to be trusted yet. | |||||
| Survey for ICU Medical Staff | Strongly Agree | Agree | Neutral | Disagree | Strongly Disagree |
|---|---|---|---|---|---|
| Ease of use of the proposed device | |||||
| The overall system was easy to use. | |||||
| The user interface of the system was intuitive and easy to understand. | |||||
| It was easy to learn how to use the system. | |||||
| It was easy to attach/detach the device. | |||||
| Effectiveness and satisfaction | |||||
| The usage of the system reduced the workload and fatigue. | |||||
| The usage of the system was time-efficient. | |||||
| I would use the system again. | |||||
| I would recommend the system to other medical staff. | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Hwang, Y.-M.; Park, S.-M. Rationale and Design of a Wearable Cardiopulmonary Monitoring System for Improving the Efficiency of Critical Care Monitoring. Appl. Sci. 2023, 13, 13101. https://doi.org/10.3390/app132413101
Lee J, Hwang Y-M, Park S-M. Rationale and Design of a Wearable Cardiopulmonary Monitoring System for Improving the Efficiency of Critical Care Monitoring. Applied Sciences. 2023; 13(24):13101. https://doi.org/10.3390/app132413101
Chicago/Turabian StyleLee, Jina, You-Mi Hwang, and Sung-Min Park. 2023. "Rationale and Design of a Wearable Cardiopulmonary Monitoring System for Improving the Efficiency of Critical Care Monitoring" Applied Sciences 13, no. 24: 13101. https://doi.org/10.3390/app132413101