
The Relationship between Gait Velocity and Walking Pattern in Hemiplegic Patients
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Sample
2.3. Assessment
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Keenan, M.A.; Perry, J.; Jordan, C. Factors affecting balance and ambulation following stroke. Clin. Orthop. Relat. Res. 1984, 182, 165–171. [Google Scholar] [CrossRef]
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Pollock, A.; Baer, G.; Campbell, P.; Choo, P.L.; Forster, A.; Morris, J.; Pomeroy, V.M.; Langhorne, P. Physical rehabilitation approaches for the recovery of function and mobility following stroke. Cochrane Database Syst. Rev. 2014, 2014, CD001920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, D.H.; Sanderson, M.; Hayes, S.; Johnson, L.; Kramer, S.; Carter, D.D.; Jarvis, H.; Brazzelli, M.; E Mead, G. Physical fitness training for stroke patients. Cochrane Database Syst. Rev. 2020, 2020, CD003316. [Google Scholar] [CrossRef] [Green Version]
- Saunders, D.H.; Greig, C.A.; Mead, G.E. Physical Activity and Exercise After Stroke: Review of multiple meaningful benefits. Stroke 2014, 45, 3742–3747. [Google Scholar] [CrossRef] [Green Version]
- Calugi, S.; Taricco, M.; Rucci, P.; Fugazzaro, S.; Stuart, M.; Dallolio, L.; Pillastrini, P.; Fantini, M.P. Effectiveness of adaptive physical< activity combined with therapeutic patient education in stroke survivors at twelve months: A non-randomized parallel group study. Eur. J. Phys. Rehabil. Med. 2016, 52, 72–80. [Google Scholar]
- Wonsetler, E.C.; Bowden, M.G. A systematic review of mechanisms of gait speed change post-stroke. Part 2: Exercise capacity, muscle activation, kinetics, and kinematics. Top. Stroke Rehabil. 2017, 24, 394–403. [Google Scholar] [CrossRef]
- Wang, Y.; Mukaino, M.; Ohtsuka, K.; Otaka, Y.; Tanikawa, H.; Matsuda, F.; Tsuchiyama, K.; Yamada, J.; Saitoh, E. Gait characteristics of post-stroke hemiparetic patients with different walking speeds. Int. J. Rehabil. Res. 2020, 43, 69–75. [Google Scholar] [CrossRef]
- Wonsetler, E.C.; Bowden, M.G. A systematic review of mechanisms of gait speed change post-stroke. Part 1: Spatiotemporal parameters and asymmetry ratios. Top. Stroke Rehabil. 2017, 24, 435–446. [Google Scholar] [CrossRef]
- Iosa, M.; Benedetti, M.G.; Antonucci, G.; Paolucci, S.; Morone, G. Artificial Neural Network Detects Hip Muscle Forces as Determinant for Harmonic Walking in People after Stroke. Sensors 2022, 22, 1374. [Google Scholar] [CrossRef]
- Cleland, B.; Madhavan, S. Changes in Walking Speed After High-Intensity Treadmill Training Are Independent of Changes in Spatiotemporal Symmetry After Stroke. Front. Neurol. 2021, 12, 647338. [Google Scholar] [CrossRef]
- Matsuzawa, Y.; Miyazaki, T.; Takeshita, Y.; Higashi, N.; Hayashi, H.; Araki, S.; Nakatsuji, S.; Fukunaga, S.; Kawada, M.; Kiyama, R. Effect of Leg Extension Angle on Knee Flexion Angle during Swing Phase in Post-Stroke Gait. Medicina 2021, 57, 1222. [Google Scholar] [CrossRef]
- Wist, S.; Clivaz, J.; Sattelmayer, K.M. Muscle strengthening for hemiparesis after stroke: A meta-analysis. Ann. Phys. Rehabil. Med. 2016, 59, 114–124. [Google Scholar] [CrossRef]
- Haruyama, K.; Kawakami, M.; Okada, K.; Okuyama, K.; Tsuzuki, K.; Liu, M. Pelvis-Toe Distance: 3-Dimensional Gait Characteristics of Functional Limb Shortening in Hemiparetic Stroke. Sensors 2021, 21, 5417. [Google Scholar] [CrossRef]
- Kerrigan, D.C.; Frates, E.P.; Rogan, S.; Riley, P.O. Hip Hiking and Circumduction. Am. J. Phys. Med. Rehabil. 2000, 79, 247–252. [Google Scholar] [CrossRef]
- Cruz, T.H.; Lewek, M.D.; Dhaher, Y.Y. Biomechanical impairments and gait adaptations post-stroke: Multi-factorial associations. J. Biomech. 2009, 42, 1673–1677. [Google Scholar] [CrossRef] [Green Version]
- Perry, J.; Burnfield, J. Section Three: Pathological Gait. In Gait Analysis: Normal and Pathological Function, 2nd ed.; SLACK Incorporated: West Deptford, NJ, USA, 2010; pp. 256, 260, 267, 339. [Google Scholar]
- Gould, D.; Kelly, D.; Goldstone, L.; Gammon, J. Examining the validity of pressure ulcer risk assessment scales: Developing and using illustrated patient simulations to collect the data INFORMATION POINT: Visual Analogue Scale. J. Clin. Nurs. 2001, 10, 697–706. [Google Scholar] [CrossRef]
- Boonstra, A.M.; Preuper, H.R.S.; Reneman, M.F.; Posthumus, J.B.; Stewart, R.E. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int. J. Rehabil. Res. 2008, 31, 165–169. [Google Scholar] [CrossRef] [Green Version]
- Demeurisse, G.; Demol, O.; Robaye, E. Motor evaluation in vascular hemiplegia. Eur. Neurol. 1980, 19, 382–389. [Google Scholar] [CrossRef]
- Medical Research Council. Aids to the Investigation of Peripheral Nerve Injuries; HMSO: London, UK, 1942. [Google Scholar]
- Fayazi, M.; Dehkordi, S.N.; Dadgoo, M.; Salehi, M. Test-retest reliability of Motricity Index strength assessments for lower extremity in post stroke hemiparesis. Med. J. Islam. Repub. Iran 2012, 26, 27–30. [Google Scholar]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef] [PubMed]
- E Kasner, S. Clinical interpretation and use of stroke scales. Lancet Neurol. 2006, 5, 603–612. [Google Scholar] [CrossRef]
- Quinn, T.J.; Dawson, J.; Walters, M.R.; Lees, K.R. Functional Outcome Measures in Contemporary Stroke Trials. Int. J. Stroke 2009, 4, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Hsueh, I.-P.; Lee, M.M.; Hsieh, C.-L. Psychometric characteristics of the Barthel activities of daily living index in stroke patients. J. Formos. Med. Assoc. 2001, 100, 526–532. [Google Scholar] [PubMed]
- Lincoln, N.B.; Gladman, J. The Extended Activities of Daily Living scale: A further validation. Disabil. Rehabil. 1992, 14, 41–43. [Google Scholar] [CrossRef]
- Sarker, S.-J.; Rudd, A.G.; Douiri, A.; Wolfe, C.D. Comparison of 2 Extended Activities of Daily Living Scales with the Barthel Index and Predictors of Their Outcomes. Stroke 2012, 43, 1362–1369. [Google Scholar] [CrossRef] [Green Version]
- Green, J.; Young, J. A test-retest reliability study of the Barthel Index, the Rivermead Mobility Index, the Nottingham extended Activities of Daily Living Scale and the Frenchay Activities Index in stroke patients. Disabil. Rehabil. 2001, 23, 670–676. [Google Scholar] [CrossRef]
- Leardini, A.; Sawacha, Z.; Paolini, G.; Ingrosso, S.; Nativo, R.; Benedetti, M.G. A new anatomically based protocol for gait analysis in children. Gait Posture 2007, 26, 560–571. [Google Scholar] [CrossRef]
- Wu, G.; Cavanagh, P.R. ISB recommendations for standardization in the reporting of kinematic data. J. Biomech. 1995, 28, 1257–1261. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Cappozzo, A.; Catani, F.; Della Croce, U.; Leardini, A. Position and orientation in space of bones during movement: Anatomical frame definition and determination. Clin. Biomech. 1995, 10, 171–178. [Google Scholar] [CrossRef]
- Vive, S.; Elam, C.; Bunketorp-Käll, L. Comfortable and Maximum Gait Speed in Individuals with Chronic Stroke and Community-Dwelling Controls. J. Stroke Cerebrovasc. Dis. 2021, 30, 106023. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, L.R.; de Menezes, K.K.P.; Scianni, A.A.; Faria-Fortini, I.; Teixeira-Salmela, L.F. Deficits in motor coordination of the paretic lower limb limit the ability to immediately increase walking speed in individuals with chronic stroke. Braz. J. Phys. Ther. 2019, 24, 496–502. [Google Scholar] [CrossRef]
- Patterson, K.K.; Nadkarni, N.K.; Black, S.E.; McIlroy, W.E. Gait symmetry and velocity differ in their relationship to age. Gait Posture 2012, 35, 590–594. [Google Scholar] [CrossRef] [Green Version]
- Mizuta, N.; Hasui, N.; Nakatani, T.; Takamura, Y.; Fujii, S.; Tsutsumi, M.; Taguchi, J.; Morioka, S. Walking characteristics including mild motor paralysis and slow walking speed in post-stroke patients. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Menezes, K.K.; Nascimento, L.R.; Faria, C.; Avelino, P.R.; A Scianni, A.; Polese, J.C.; Faria-Fortini, I.; Teixeira-Salmela, L.F. Deficits in motor coordination of the paretic lower limb best explained activity limitations after stroke. Physiother. Theory Pr. 2018, 36, 417–423. [Google Scholar] [CrossRef]
- Sánchez, N.; Acosta, A.M.; Lopez-Rosado, R.; Stienen, A.H.A.; Dewald, J.P.A. Lower Extremity Motor Impairments in Ambulatory Chronic Hemiparetic Stroke: Evidence for Lower Extremity Weakness and Abnormal Muscle and Joint Torque Coupling Patterns. Neurorehabilit. Neural Repair 2017, 31, 814–826. [Google Scholar] [CrossRef]
- Kwan, M.S.-M.; Hassett, L.M.; Ada, L.; Canning, C.G. Relationship between lower limb coordination and walking speed after stroke: An observational study. Braz. J. Phys. Ther. 2018, 23, 527–531. [Google Scholar] [CrossRef]
- Hiba, S.; Raphael, Z.; Jonathan, B.; Nicolas, R.; Pauline, G. Co-contraction around the knee and the ankle joints during post-stroke gait. Eur. J. Phys. Rehabil. Med. 2018, 54, 380–387. [Google Scholar] [CrossRef]
- Mentiplay, B.F.; Williams, G.; Tan, D.; Adair, B.; Pua, Y.-H.; Bok, C.W.; Bower, K.J.; Cole, M.H.; Ng, Y.S.; Lim, L.S.; et al. Gait Velocity and Joint Power Generation After Stroke. Am. J. Phys. Med. Rehabil. 2018, 98, 841–849. [Google Scholar] [CrossRef]
- Aguiar, L.T.; Camargo, L.B.A.; Estarlino, L.D.; Teixeira-Salmela, L.F.; Faria, C.D.C.D.M. Strength of the lower limb and trunk muscles is associated with gait speed in individuals with sub-acute stroke: A cross-sectional study. Braz. J. Phys. Ther. 2018, 22, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Dorsch, S.; Ada, L.; Canning, C.G.; Al-Zharani, M.; Dean, C. The Strength of the Ankle Dorsiflexors Has a Significant Contribution to Walking Speed in People Who Can Walk Independently After Stroke: An Observational Study. Arch. Phys. Med. Rehabil. 2012, 93, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Lee, B.J.; Joo, N.-Y.; Park, D. The parameters of gait analysis related to ambulatory and balance functions in hemiplegic stroke patients: A gait analysis study. BMC Neurol. 2021, 21, 1–8. [Google Scholar] [CrossRef]
- Wing, K.; Lynskey, J.; Bosch, P.R. Walking Speed in Stroke Survivors: Considerations for Clinical Practice. Top. Geriatr. Rehabil. 2012, 28, 113–121. [Google Scholar] [CrossRef]
- Stuart, M.; Dromerick, A.W.; Macko, R.; Benvenuti, F.; Beamer, B.; Sorkin, J.; Chard, S.; Weinrich, M. Adaptive Physical Activity for Stroke: An Early-Stage Randomized Controlled Trial in the United States. Neurorehabilit. Neural Repair 2019, 33, 668–680. [Google Scholar] [CrossRef]


{kind=link}
| Age | 69.7 (SD 7.1) |
| Sex (M:F) | 17:13 |
| BMI | 28.8 (SD 5.2) |
| Paretic side (R:L) | 10:20 |
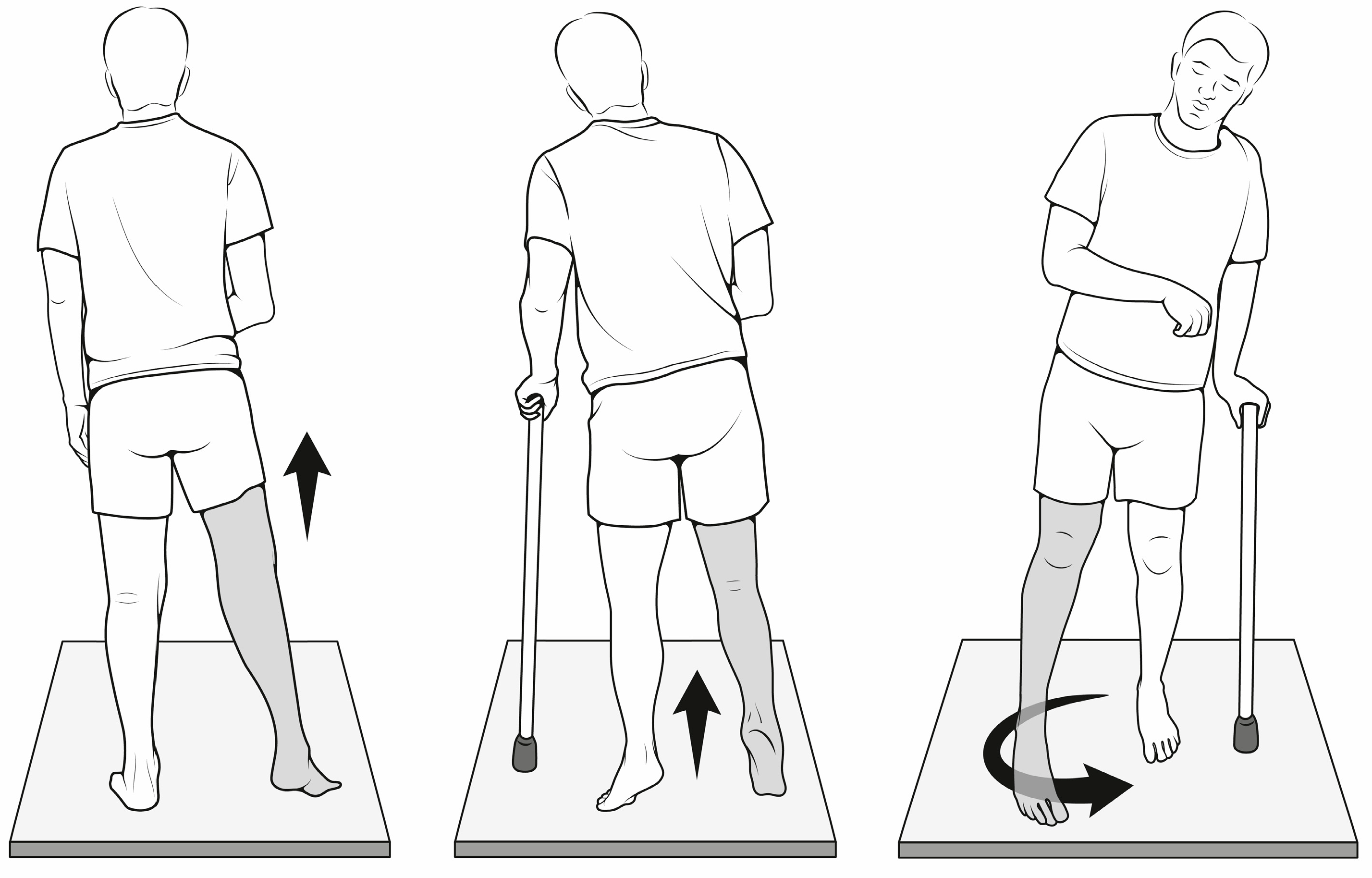
| Compensatory gait strategy | 2 Vaulting 5 Hip hiking 2 Circumduction 4 Vaulting + hip hiking 5 Vaulting + hip hiking + circumduction 11 Non classifiable |
| VAS | 19.7 (SD 24.9) |
| BI | 71.6 (SD 16.4) |
| MI paretic side | 76.5 (SD 25.0) |
| NEAS | 10.3 (SD 4.3) |
| Pattern | N Patients | Mean Speed cm/s | SD |
|---|---|---|---|
| Vaulting | 2 | 30.3 | 8.7 |
| Hip hiking | 5 | 28.3 | 14.8 |
| Circumduction | 2 | 58.9 | 11.2 |
| Hip hiking + vaulting | 4 | 43.2 | 9.9 |
| Hip hiking + vaulting + circumduction | 5 | 46.0 | 5.1 |
| Non classifiable | 11 | 51.5 | 23.6 |
| Joint aROM (n pts) Hemiplegic Side | Mean | SD | Spearman Rank Correlation (p) |
| Hip flexion (30) | 106.3 | 10.1 | Ns |
| Hip extension (19) | 15.0 | 5.27 | Rho 0.480, p = 0.03 |
| Hip Abduction (30) | 27.93 | 19.9 | Ns |
| Hip Adduction (30) | 15.1 | 5.5 | Ns |
| Knee flexion (30) | 121.5 | 18.7 | Ns |
| Knee extension (20) | −9.9 | 8.8 | Ns |
| Dorsiflexion TT (28) | 9.3 | 2.9 | Ns |
| Plantarflexion TT (30) | 29.3 | 10.9 | Ns |
| Muscular Strength (n pts) Hemiplegic side | mean | SD | Spearman rank correlation (p) |
| Quadriceps (30) | 72.4 | 31.3 | Rho 0.604, p = 0.001 |
| Ilio-psoas (29) | 57.3 | 26.6 | Rho 0.358, p = 0.061 |
| Tibialis anterior (10) | 25.5 | 13.3 | Ns |
| Gluteus Maximus (15) | 34.1 | 15.4 | Ns |
| Gluteus Medius (22) | 55.4 | 23.7 | Ns |
| Biceps femoris (17) | 32.4 | 17.2 | Ns |
| Semitendinosus (20) | 34.7 | 18.2 | Ns |
| Mean | SD | Spearman Rank Correlation | ||
|---|---|---|---|---|
| Stance time (% stride) | Plegic Unaffected | 65.7 72.5 | 6.6 5.4 | Rho −0.631, p < 0.000 Rho −0.865, p < 0.000 |
| Stride lenght normalized (%h) | 38.1 | 10.8 | Rho 0.879, p < 0.000 | |
| Cycle time | 1.5 | 0.4 | Rho 0.568, p = 0.001 | |
| Cadence (stride/min) | 42.6 | 10.7 | Rho 0.561, p = 0.002 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nesi, B.; Taviani, A.; D’Auria, L.; Bardelli, R.; Zuccarello, G.; Platano, D.; Benedetti, M.G.; Benvenuti, F. The Relationship between Gait Velocity and Walking Pattern in Hemiplegic Patients. Appl. Sci. 2023, 13, 934. https://doi.org/10.3390/app13020934
Nesi B, Taviani A, D’Auria L, Bardelli R, Zuccarello G, Platano D, Benedetti MG, Benvenuti F. The Relationship between Gait Velocity and Walking Pattern in Hemiplegic Patients. Applied Sciences. 2023; 13(2):934. https://doi.org/10.3390/app13020934
Chicago/Turabian StyleNesi, Barbara, Antonio Taviani, Lucia D’Auria, Roberta Bardelli, Giuseppe Zuccarello, Daniela Platano, Maria Grazia Benedetti, and Francesco Benvenuti. 2023. "The Relationship between Gait Velocity and Walking Pattern in Hemiplegic Patients" Applied Sciences 13, no. 2: 934. https://doi.org/10.3390/app13020934