

Growth of Escherichia coli in Human Milk and Powdered Infant Formula under Various Treatments and Feeding Conditions in Neonatal Units
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Study of Growth of E. coli in HM and PIF Held at 22 °C for 4 h
2.3. Study of the Influence of Different Thawing Methods on the Growth of E. coli in HM
2.4. Data Analysis
3. Results
3.1. Study of Growth of E. coli in HM and PIF Held at 22 °C for 4 h
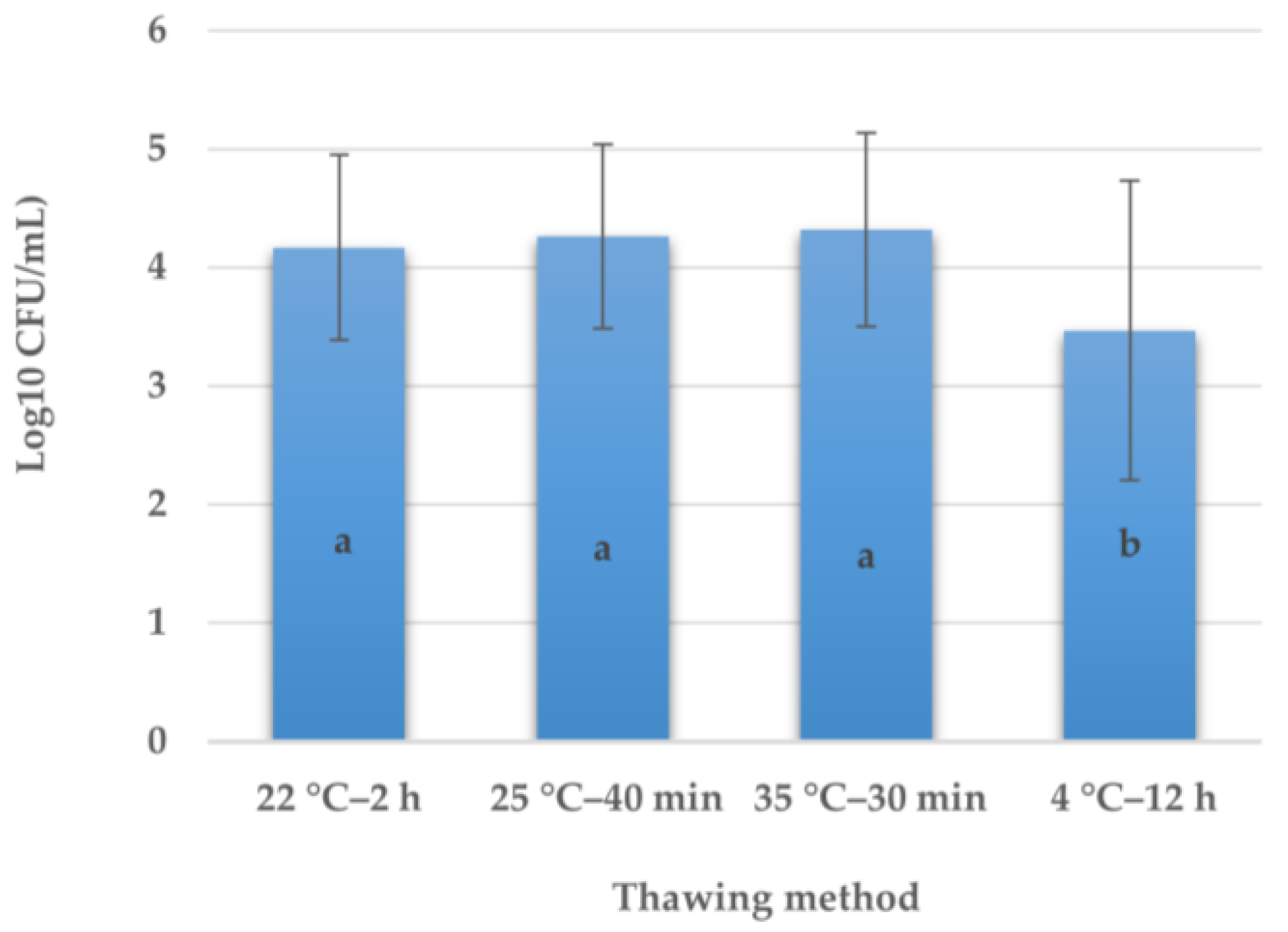
3.2. Influence of Different Thawing Methods on the Development of E. coli in HM
4. Discussion
4.1. Significance and Practical Application of Results
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Breastfeeding. Available online: https://www.who.int/health-topics/breastfeeding (accessed on 16 January 2023).
- Taft, D.H.; Salinero, L.K.; Vongbhavit, K.; Kalanetra, K.M.; Masarweh, C.; Yu, A.; Underwood, M.A.; Mills, D.A. Bacterial colonization and antimicrobial resistance genes in neonatal enteral feeding tubes. FEMS Microbiol. Ecol. 2019, 95, fiz039. [Google Scholar] [CrossRef]
- Calvo, J.; García, N.R.; Gormaz, M.; Peña, M.; Martínez, M.J.; Ortiz, P.; Brull, J.M.; Samaniego, C.M.; Gaya, A. Recomendaciones para la creación y el funcionamiento de los bancos de leche materna en España [Recommendations for the creation and operation of maternal milk banks in Spain]. An. Pediatr. 2018, 89, 65.e1–65.e6. [Google Scholar] [CrossRef] [PubMed]
- Scott, H.; Sweet, L.; Strauch, L.; Muller, A. Expressed breastmilk handling and storage guidelines available to mothers in the community: A scoping review. Women Birth 2020, 33, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Steele, C.; Collins, E. (Eds.) Infant and Pediatric Feedings: Guidelines for Preparation of Human Milk and Formula in Health Care Facilities, 3rd ed.; Academy of Nutrition and Dietetics: Chicago, IL, USA, 2018; pp. 1–248. [Google Scholar]
- Gao, X.; Li, Y.; Olin, A.B.; Nguyen, D.N. Fortification with bovine colostrum enhances antibacterial activity of human milk. J. Parenter. Enter. Nutr. 2021, 45, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Barbarska, O.; Strom, K.; Oledzka, G.; Calvo, J.; Gayà, A.; López-Mendoza, M.C.; Rutkowska, M.; Rosiak, E.; Wesolowska, A.M. Effect of nonthermal processing on human milk bactericidal activity against Escherichia coli. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 864–867. [Google Scholar] [CrossRef]
- Fernández-Pastor, S.; Silvestre, D.; López-Mendoza, M.C. Stability of the antimicrobial capacity of human milk against Cronobacter sakazakii during handling. J. Hum. Lact. 2021, 37, 139–146. [Google Scholar] [CrossRef]
- Schlotterer, H.R.; Parvez, B.; Perrin, M.T. The Effects of Fortification and Refrigerated Storage on Bioactive Proteins in Holder-pasteurized Donor Human Milk. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 370–374. [Google Scholar] [CrossRef]
- British Dietetic Association. Guidelines for the Preparation and Handling of Expressed and Donor Breast Milk and Specialist Feeds for Infants and Children in Neonatal and Paediatric Health Care Settings. Available online: https://www.bda.uk.com/uploads/assets/913a1f78-c805-42c1-8d85e37ca75e0fc0/2019sfuguidelines.pdf (accessed on 16 January 2023).
- PATH. Strengthening Human Milk Banking: A Resource Toolkit for Establishing and Integrating Human Milk Bank Programs—A Global Implementation Framework. Version 2.0; PATH: Seattle, WA, USA, 2019; Available online: https://www.aeblh.org/images/publicaciones/2019/20191009_path_hmb_toolkit_0.global_implementation_framework.pdf (accessed on 16 January 2023).
- Eglash, A.; Simon, L. ABM Clinical Protocol #8: Human milk storage information for home use for full-term infants, Revised 2017. Breastfeed. Med. 2017, 12, 390–395, Erratum in Breastfeed. Med. 2018, 13, 459. [Google Scholar]
- Boullata, J.I.; Carrera, A.L.; Harvey, L.; Escuro, A.A.; Hudson, L.; Mays, A.; McGinnis, C.; Wessel, J.J.; Bajpai, S.; Beebe, M.L.; et al. ASPEN safe practices for enteral nutrition therapy. J. Parenter. Enter. Nutr. 2017, 41, 15–103. [Google Scholar] [CrossRef] [Green Version]
- United States Centers for Diseases Control and Prevention. Proper Storage and Preparation of Breast Milk. Available online: https://www.cdc.gov/breastfeeding/recommendations/handling_breastmilk.htm (accessed on 1 March 2023).
- Flannery, D.D.; Akinboyo, I.C.; Mukhopadhyay, S.; Tribble, A.C.; Song, L.; Chen, F.; Li, Y.; Gerber, J.S.; Puopolo, K.M. Antibiotic susceptibility of Escherichia coli among infants admitted to neonatal intensive care units across the US from 2009 to 2017. JAMA Pediatr. 2021, 175, 168–175. [Google Scholar] [CrossRef]
- Xiao, R.; Li, Y.; Liu, X.; Ding, Y.; Lai, J.; Li, Y.; Kang, W.; Zou, P.; Wang, J.; Du, Y.; et al. Antibiotic susceptibility of Escherichia coli isolated from neonates admitted to neonatal intensive care units across China from 2015 to 2020. Front. Cell. Infect. Microbiol. 2023, 13, 1183736. [Google Scholar] [CrossRef] [PubMed]
- Chishiki, M.; Nishiyama, K.; Suzutani, T.; Hiruta, S.; Ichikawa, H.; Haneda, K.; Maeda, H.; Shimizu, H.; Kanai, Y.; Ogasawara, K.; et al. Sterilization efficacy of a new water-free breast milk pasteurizer. Pediatr. Int. 2023, 65, e15574. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Kaneko, M.; Abe, Y.; Yamamoto, N.; Mori, H.; Yoshida, A.; Ohashi, K.; Miura, S.; Yang, T.T.; Momoi, N.; et al. Outbreak of extended-spectrum β-lactamase-producing Escherichia coli transmitted through breast milk sharing in a neonatal intensive care unit. J. Hosp. Infect. 2016, 92, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Siviroj, P.; Ruangsuriya, J.; Yousaibua, N.; Ongprasert, K. Effects of the thawing rate and heating temperature on immunoglobulin A and lysozyme activity in human milk. Int. Breastfeed. J. 2022, 17, 52. [Google Scholar] [CrossRef] [PubMed]
- Asociación Española de Bancos de Leche Humana. Donación de Leche. [Milk Donation]. Available online: https://www.aeblh.org/banco-de-leche/como-donar-leche (accessed on 3 March 2023).
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull. World Health Organ. 2001, 79, 373–374. [Google Scholar]
- Spanish Ministry of the Presidency. Royal Decree 867/2008 of 23 May 2008 Approving the Specific Technical Health Regulations for Infant Formulae and Follow-on Formulae. Available online: https://www.boe.es/diario_boe/txt.php?id=BOE-A-2008-9289 (accessed on 13 July 2023).
- Lenati, R.F.; O’Connor, D.L.; Hébert, K.C.; Farber, J.M.; Pagotto, F.J. Growth and survival of Enterobacter sakazakii in human breast milk with and without fortifiers as compared to powdered infant formula. Int. J. Food Microbiol. 2008, 122, 171–179. [Google Scholar] [CrossRef]
- International Organization for Standardization. Microbiology of the Food Chain—Horizontal Method for the Detection and Enumeration of Enterobacteriaceae—ISO Standard No. 21528-2:2017; International Organization for Standardization: Geneva, Switzerland, 2017.
- Madigan, M.T.; Bender, K.S.; Bucley, W.; Sattley, M.; Stahl, D.A. Brock Biology of Microorganisms, 15th ed.; Pearson: London, UK, 2018. [Google Scholar]
- Lemons, P.M.; Miller, K.; Eitzen, H.; Strodtbeck, F.; Lemons, J.A. Bacterial growth in human milk during continuous feeding. Am. J. Perinatol. 1983, 1, 76–80. [Google Scholar] [CrossRef]
- Handa, D.; Ahrabi, A.F.; Codipilly, C.N.; Shah, S.; Ruff, S.; Potak, D.; Williams, J.E.; McGuire, M.A.; Schanler, R.J. Do thawing and warming affect the integrity of human milk? J. Perinatol. 2014, 34, 863–866. [Google Scholar] [CrossRef]
- Paulaviciene, I.J.; Liubsys, A.; Eidukaite, A.; Molyte, A.; Tamuliene, L.; Usonis, V. The effect of prolonged freezing and holder pasteurization on the macronutrient and bioactive protein compositions of human milk. Breastfeed. Med. 2020, 15, 583–588. [Google Scholar] [CrossRef]
- Arroyo, G.; Ortiz Barrientos, K.A.; Lange, K.; Nave, F.; Miss Mas, G.; Lam Aguilar, P.; Soto Galindo, M.A. Effect of the various steps in the processing of human milk in the concentrations of IgA, IgM, and lactoferrin. Breastfeed. Med. 2017, 12, 443–445. [Google Scholar] [CrossRef]
- Vongbhavit, K.; Salinero, L.K.; Kalanetra, K.M.; Masarweh, C.; Yu, A.; Taft, D.H.; Mills, D.A.; Underwood, M.A. A comparison of bacterial colonization between nasogastric and orogastric enteral feeding tubes in infants in the neonatal intensive care unit. J. Perinatol. 2022, 42, 1446–1452. [Google Scholar] [CrossRef] [PubMed]
- Telang, S.; Berseth, C.L.; Ferguson, P.W.; Kinder, J.M.; DeRoin, M.; Petschow, B.W. Fortifying fresh human milk with commercial powdered human milk fortifiers does not affect bacterial growth during 6 hours at room temperature. J. Am. Diet. Assoc. 2005, 105, 1567–1572. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Timilsena, Y.P.; Blanch, E.; Adhikari, B. Lactoferrin: Structure, function, denaturation and digestion. Crit. Rev. Food Sci. Nutr. 2017, 59, 580–596. [Google Scholar] [CrossRef]
- Ackerman, D.L.; Craft, K.M.; Doster, R.S.; Weitkamp, J.H.; Aronoff, D.M.; Gaddy, J.A.; Townsend, S.D. Antimicrobial and antibiofilm activity of human milk oligosaccharides against Streptococcus agalactiae, Staphylococcus aureus, and Acinetobacter baumannii. ACS Infect. Dis. 2018, 4, 315–324. [Google Scholar] [CrossRef]
- Ochoa, T.J.; Mendoza, K.; Carcamo, C.; Zegarra, J.; Bellomo, S.; Jacobs, J.; Cossey, V. Is mother’s own milk lactoferrin intake associated with reduced neonatal sepsis, necrotizing enterocolitis, and death? Neonatology 2020, 117, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Schlievert, P.M.; Kilgore, S.H.; Seo, K.S.; Leung, D.Y.M. Glycerol Monolaurate Contributes to the Antimicrobial and Anti-inflammatory Activity of Human Milk. Sci. Rep. 2019, 9, 14550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Zhou, Y.; Liu, X.; Zhang, F.; Yan, L.; Chen, L.; Wang, X.; Ruan, H.; Ji, C.; Cui, X.; et al. Antimicrobial activity and mechanism of PDC213, an endogenous peptide from human milk. Biochem. Biophys. Res. Commun. 2017, 484, 132–137. [Google Scholar] [CrossRef]
- Thai, J.D.; Gregory, K.E. Bioactive factors in human breast milk attenuate intestinal inflammation during early life. Nutrients 2020, 12, 581. [Google Scholar] [CrossRef] [Green Version]
- Odeyemi, O.A.; Sani, N.A. The prevention of Cronobacter infections in hospital neonatal intensive care units. J. Infect. Public Health 2016, 9, 110–112. [Google Scholar] [CrossRef] [Green Version]
- Sundararajan, M.; Enane, L.A.; Kidwell, L.A.; Gentry, R.; Danao, S.; Bhumbra, S.; Lehmann, C.; Teachout, M.; Yeadon-Fagbohun, J.; Krombach, P.; et al. Notes from the field: Cronobacter sakazakii meningitis in a full-term neonate fed exclusively with breast milk. Indiana, 2018. Morb. Mortal Wkly. Rep. 2018, 67, 1248–1249. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Number of Generations | Generation Time 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Treatment 1 | 0.5 h | 1 h | 1.5 h | 2 h | 2.5 h | 3 h | 3.5 h | 4 h | p | (Minutes) |
| A (n = 12) | −0.09 ± 0.15 | −0.02 ± 0.16 | 0.14 ± 0.11 | 0.06 ± 0.13 | 0.39 ± 0.28 * | 0.45 ± 0.22 | 0.75 ± 0.30 | 1.04 ± 0.19 | 0.013 | 229.72 ± 37.84 a |
| B (n = 12) | −0.12 ± 0.49 | 0.13 ± 0.55 | 0.58 ± 0.46 * | 0.71 ± 0.59 | 0.93 ± 0.62 | 1.20 ± 0.73 | 1.79 ± 0.79 | 1.89 ± 0.71 | 0.001 | 126.65 ± 53.32 b |
| C (n = 12) | −0.17 ± 0.24 | 0.20 ± 0.44 | 0.15 ± 0.60 | 0.65 ± 0.69 * | 0.73 ± 0.54 | 0.90 ± 0.63 | 1.30 ± 0.46 | 1.53 ± 0.58 | 0.001 | 157.05 ± 66.17 a,b |
| Number of Generations | Generation Time 1 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Brand | 0.5 h | 1 h | 1.5 h | 2 h | 2.5 h | 3 h | 3.5 h | 4 h | p | (Minutes) |
| A (n = 5) | −0.11 ± 0.26 | 0.19 ± 0.17 | 0.20 ± 0.13 | 0.07 ± 0.07 | 0.20 ± 0.17 | 0.47 ± 0.04 * | 0.74 ± 0.04 | 0.77 ± 0.08 | 0.029 | 313.61 ± 33.16 a |
| B (n = 5) | −0.17 ± 0.39 | −0.08 ± 0.09 | 0.18 ± 0.19 * | 0.30 ± 0.16 | 0.38 ± 0.16 | 0.67 ± 0.15 | 0.76 ± 0.13 | 0.98 ± 0.22 | 0.035 | 256.95 ± 61.34 a.b |
| C (n = 5) | 0.16 ± 0.17 | 0.10 ± 0.09 | 0.31 ± 0.16 | 0.42 ± 0.20 | 0.58 ± 0.14 | 0.75 ± 0.14 * | 0.78 ± 0.13 | 1.04 ± 0.30 | 0.002 | 244.94 ± 67.17 a.b |
| D (n = 5) | 0.09 ± 0.08 | 0.16 ± 0.08 | 0.10 ± 0.08 | 0.19 ± 0.14 | 0.40 ± 0.11 | 0.71 ± 0.07 * | 0.99 ± 0.38 | 1.39 ± 0.28 | 0.009 | 179.24 ± 40.18 b |
| Time at 22 °C | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0.5 h | 1 h | 1.5 h | 2 h | 2.5 h | 3 h | 3.5 h | 4 h | p | |
| HM 1 | −0.12 ± 0.2 | 0.10 ± 0.41 | 0.29 ± 0.49 | 0.47 ± 0.59 | 0.68 ± 0.54 | 0.85 ± 0.64 | 1.28 ± 0.69 | 1.48 ± 0.75 | 0.054 |
| PIF 2 | −0.001 ± 0.27 | 0.09 ± 0.15 | 0.20 ± 0.15 | 0.24 ± 0.20 | 0.39 ± 0.21 | 0.65 ± 0.15 | 0.82 ± 0.22 | 1.05 ± 0.32 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Mendoza, M.C.; Lozano, M.; García-Romero, E.; Ruiz-García, P.; Gormaz, M.; Jordano, R.; Medina, L.M.; Ramón-Beltrán, A.; Silvestre, D. Growth of Escherichia coli in Human Milk and Powdered Infant Formula under Various Treatments and Feeding Conditions in Neonatal Units. Appl. Sci. 2023, 13, 8978. https://doi.org/10.3390/app13158978
López-Mendoza MC, Lozano M, García-Romero E, Ruiz-García P, Gormaz M, Jordano R, Medina LM, Ramón-Beltrán A, Silvestre D. Growth of Escherichia coli in Human Milk and Powdered Infant Formula under Various Treatments and Feeding Conditions in Neonatal Units. Applied Sciences. 2023; 13(15):8978. https://doi.org/10.3390/app13158978
Chicago/Turabian StyleLópez-Mendoza, María Carmen, Marta Lozano, Edgar García-Romero, Pilar Ruiz-García, María Gormaz, Rafael Jordano, Luis Manuel Medina, Amparo Ramón-Beltrán, and Dolores Silvestre. 2023. "Growth of Escherichia coli in Human Milk and Powdered Infant Formula under Various Treatments and Feeding Conditions in Neonatal Units" Applied Sciences 13, no. 15: 8978. https://doi.org/10.3390/app13158978