
Interaction of Voice Onset Time with Vocal Hyperfunction and Voice Quality


Abstract
:Featured Application
Abstract
1. Introduction
1.1. Concept of Voice Onset Time
1.2. Voice Onset Time in Vocal Hyperfunction
- (1)
- Does the VH condition influence VOT, fo, and speaking voice intensity?
- (2)
- Is there a relationship between vocal quality, VOT, fo, and speaking voice intensity?
- (3)
- Does the phonetic environment influence VOT, fo, and speaking voice intensity?
2. Materials and Methods
2.1. Database
2.2. Patient Inclusion Criteria
Diagnosis Criteria of PVH and NPVH
2.3. Description of Included Cases
2.4. Voice Recording Technique and Study Corpus
Composition of Study Corpus
2.5. Perceptual Assessment
2.6. Acoustic Recording Preparation and Analysis
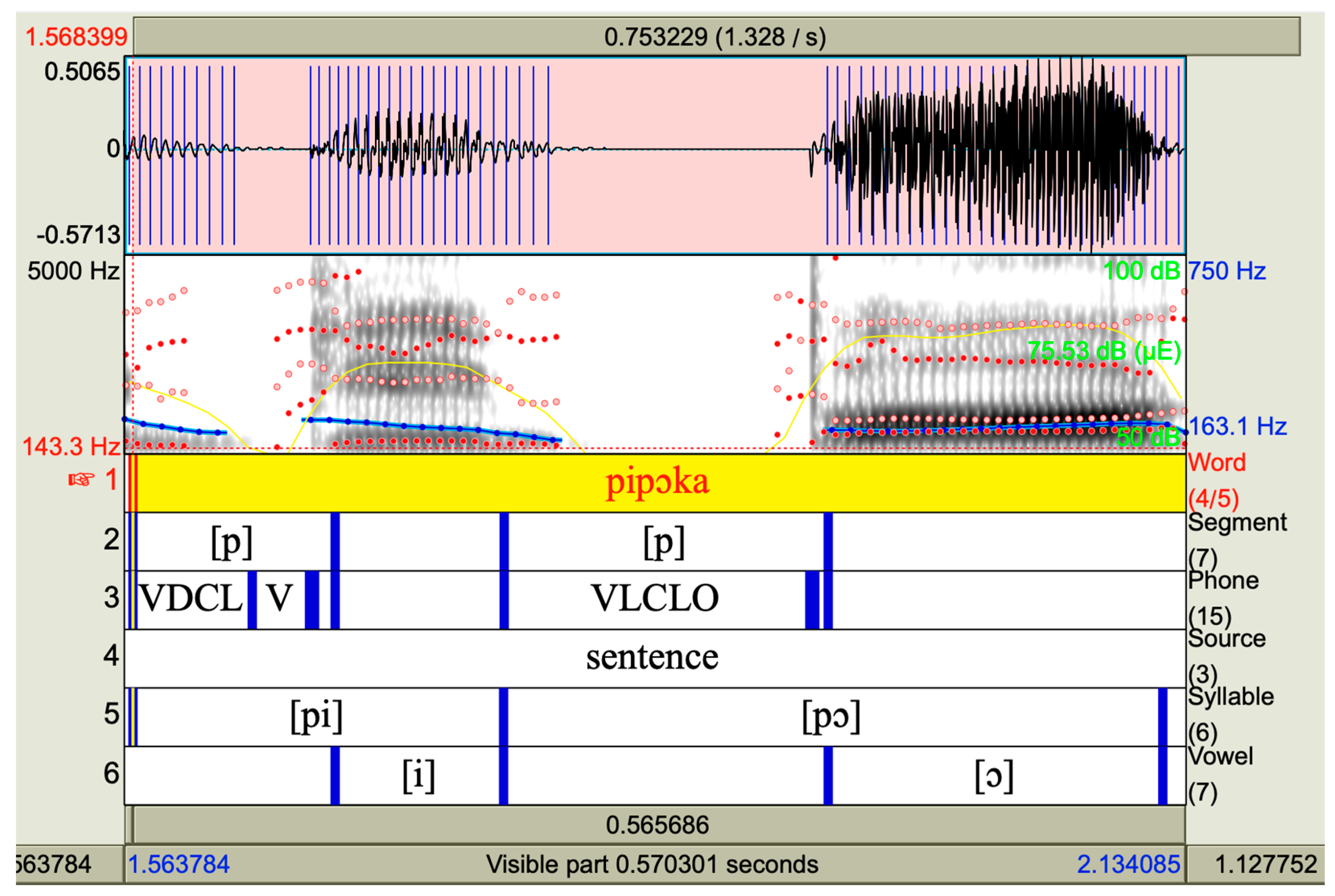
2.6.1. Acoustic Features of the Consonant [p]
2.6.2. Instrumental Acoustic Analysis
2.7. Statistical Analysis
3. Results
3.1. Descriptive Results
3.2. Effects of VH Condition, OS, and Gender on VOT, fo, and SPL
3.2.1. VH Condition
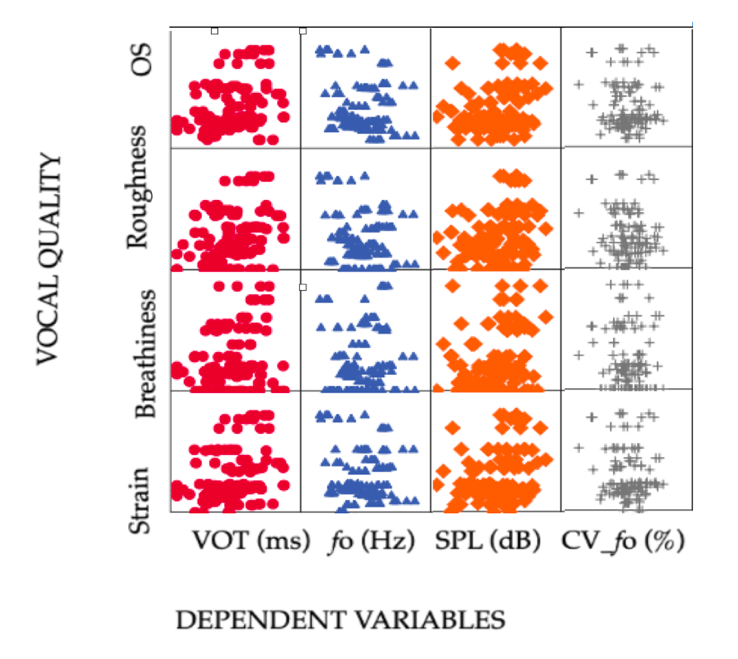
3.2.2. Vocal Quality
3.2.3. Gender
3.3. Relation of VQ with VOT, fo, and SPL
3.4. Effects of Phonetic Environment on VOT, fo, and SPL
4. Discussion
4.1. VOT Mean Duration
4.2. Influence of VH Condition on VOT, fo, and SPL
4.3. VQ Is Correlated with VOT
4.4. Influence of Phonetic Environment
4.5. Gender Effects
4.6. Clinical Relevance and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kreiman, J.; Gerratt, B. Measuring Vocal Quality. In Voice Quality Measurement; Kent, R., Ball, M.J., Eds.; Singular Publishing Group: San Diego, CA, USA, 2000; Volume 1, pp. 73–101. [Google Scholar]
- Buder, E.H. Acoustic Analysis of Voice Quality: A tabulation of Algorithms 1902–1990. In Voice Quality Measurement; Kent, R., Ball, M., Eds.; Singular Publishing Group: San Diego, CA, USA, 2000; pp. 119–244. [Google Scholar]
- Hillman, R.E.; Holmberg, E.B.; Perkell, J.S.; Walsh, M.; Vaughan, C. Objective Assessment of Vocal Hyperfunction: An experimental framework and initial results. J. Speech Lang. Hear. Res. 1989, 32, 373–392. [Google Scholar] [CrossRef] [PubMed]
- Hillman, R.E.; Holmberg, E.B.; Perkell, J.S.; Walsh, M.; Vaughan, C. Phonatory function associated with hyperfunctionally related vocal fold lesions. J. Voice 1990, 4, 52–63. [Google Scholar] [CrossRef]
- Hillman, R.E.; Stepp, C.E.; Van Stan, J.H.; Zañartu, M.; Mehta, D.D. An Updated Theoretical Framework for Vocal Hyperfunction. Am. J. Speech-Lang. Pathol. 2020, 29, 2254–2260. [Google Scholar] [CrossRef] [PubMed]
- Solomon, N.P. Vocal fatigue and its relation to vocal hyperfunction. Int. J. Speech-Lang. Pathol. 2008, 10, 254–266. [Google Scholar] [CrossRef]
- Hunter, E.J.; Cantor-Cutiva, L.C.; van Leer, E.; van Mersbergen, M.; Nanjundeswaran, C.D.; Bottalico, P.; Sandage, M.J.; Whitling, S. Toward a Consensus Description of Vocal Effort, Vocal Load, Vocal Loading, and Vocal Fatigue. J. Speech Lang. Hear. Res. 2020, 63, 509–532. [Google Scholar] [CrossRef]
- Roy, N.; Fetrow, R.A.; Merrill, R.M.; Dromey, C. Exploring the Clinical Utility of Relative Fundamental Frequency as an Objective Measure of Vocal Hyperfunction. J. Speech Lang. Hear. Res. 2016, 59, 1002–1017. [Google Scholar] [CrossRef]
- Lopes, L.W.; Batista Simoes, L.; Delfino da Silva, J.; da Silva Evangelista, D.; da Nobrega, E.U.A.C.; Oliveira Costa Silva, P.; Jefferson Dias Vieira, V. Accuracy of Acoustic Analysis Measurements in the Evaluation of Patients with Different Laryngeal Diagnoses. J. Voice 2017, 31, 382.e15–382.e26. [Google Scholar] [CrossRef]
- Groll, M.D.; Hablani, S.; Stepp, C.E. The Relationship Between Voice Onset Time and Increase in Vocal Effort and Fundamental Frequency. J. Speech Lang. Hear. Res. 2021, 64, 1197–1209. [Google Scholar] [CrossRef]
- Heller Murray, E.S.; Lien, Y.S.; Van Stan, J.H.; Mehta, D.D.; Hillman, R.E.; Pieter Noordzij, J.; Stepp, C.E. Relative Fundamental Frequency Distinguishes Between Phonotraumatic and Non-Phonotraumatic Vocal Hyperfunction. J. Speech Lang. Hear. Res. 2017, 60, 1507–1515. [Google Scholar] [CrossRef] [Green Version]
- Stepp, C.E.; Merchant, G.R.; Heaton, J.T.; Hilmann, R.E. Effects of Voice Therapy on Relative Fundamental Frequency During Voicing Offset and Onset in Patients with Vocal Hyperfunction. J. Speech Lang. Hear. Res. 2011, 54, 1260–1266. [Google Scholar] [CrossRef] [Green Version]
- Stepp, C.E.; Hillman, R.E.; Heaton, J.T. The Impact of Vocal Hyperfunction on Relative Fundamental Frequency During Voicing Offset and Onset. J. Speech Lang. Hear. Res. 2010, 53, 1220–1226. [Google Scholar] [CrossRef] [PubMed]
- McKenna, V.S.; Heller Murray, E.S.; Lien, Y.-A.S.; Stepp, C.E. The Relationship Between Relative Fundamental Frequency and a Kinematic Estimate of Laryngeal Stiffness in Healthy Adults. J. Speech Lang. Hear. Res. 2016, 19, 1283–1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groll, M.D.; Vojtech, J.M.; Hablani, S.; Mehta, D.D.; Buckley, D.P.; Noordzij, J.P.; Stepp, C.E. Automated Relative Fundamental Frequency Algorithms for Use with Neck-Surface Accelerometer Signals. J. Voice 2022, 36, 156–169. [Google Scholar] [CrossRef] [PubMed]
- Lien, Y.A.S.; Gattuccio, C.I.; Stepp, C.E. Effects of Phonetic Context on Relative Fundamental Frequency. J. Speech Lang. Hear. Res. 2014, 57, 1259–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behlau, M.; Madazio, G.; Feijo, D.; Pontes, P. Avaliação de Voz. In Voz O Livro do Especialista, 1st ed.; Behlau, M., Ed.; Revinter: Rio de Janeiro, Brazil, 2000; Volume 1, pp. 85–180. [Google Scholar]
- Koike, Y. Experimental Studies on Vocal Attack. Pr. Oto-Rhino-Laryngol. 1967, 60, 663–688. [Google Scholar] [CrossRef] [Green Version]
- Maryn, Y.; Poncelet, S. How Reliable Is the Auditory-Perceptual Evaluation of Phonation Onset Hardness? J. Voice 2021, 35, 869–875. [Google Scholar] [CrossRef]
- Cho, T.; Ladefoged, P. Variation and universals in VOT: Evidence from 18 languages. J. Phon. 1999, 27, 207–229. [Google Scholar] [CrossRef]
- Lisker, L.; Abramson, A.S. A Cross-Language Study of Voicing in Initial Stops: Acoustical Measurements. Word 1964, 20, 384–422. [Google Scholar] [CrossRef] [Green Version]
- Klein, S. Estudo do VOT no Português Brasileiro; Universidade Federal de Santa Catarina: Florianópolis, Brazil, 1999. [Google Scholar]
- Schwartzhaupt, B. Factors Influencing Voice Onset Time: Analyzing Brazilian Portuguese, English and Interlanguage Data; Universidade Federal do Rio Grande do Sul: Porto Alegre, Brazil, 2012. [Google Scholar]
- Silva, T.C.; Seara, I.C.; Silva, A.; Rauber, A.S.; Cantoni, M.M. Fonética Acústica. Os Sons do Português Brasileiro; Editora Contexto: São Paulo, Brazil, 2019. [Google Scholar]
- Alves, M.A. Estudo dos Parâmetros Acústicos Relacionados à Produção das Plosivas do Português Brasileiro na Fala Adulta: Análise Acústico-Quantitativa; Universidade Federal de Santa Catarina: Florianópolis, Brazil, 2015. [Google Scholar]
- Keating, P.A. Universal phonetics and the organization of grammars. In Phonetic Linguistics: Essays in Honor of Peter Ladefoged; Fromkin, V.A., Ed.; Academic Press: Oxford, UK, 1985; pp. 115–132. [Google Scholar]
- Narayan, C.; Bowden, M. Pitch affects voice onset time (VOT): A cross-linguistic study. In Proceedings of the Meeting on Acoustics, Montreal, QC, Canada, 2–7 June 2013. [Google Scholar]
- Park, S.-Y.; Kim, S.-T.; Kim, S.-Y.; Choi, S.-H.; Roh, J.-L.; Nam, S.-Y. Voice Onset Time in Patients with Bilateral Vocal Nodules. J. Korean Soc. Laryngol. Phoniatr. Logop. 2006, 17, 107–110. [Google Scholar]
- Marciniec, S.A. Voice Onset Time of Women with Vocal Nodules; Rush University, ProQuest Dissertations Publishing: Chicago, IL, USA, 2009. [Google Scholar]
- Colletti, L. Voice Onset Time in Children with and without Vocal Fold Nodules; Temple University: Philadelphia, PA, USA, 2022; Available online: http://hdl.handle.net/20.500.12613/7709 (accessed on 5 October 2022).
- McKenna, V.S.; Hylkema, J.A.; Tardif, M.C.; Stepp, C.E. Voice Onset Time in Individuals with Hyperfunctional Voice Disorders: Evidence for Disordered Vocal Motor Control. J. Speech Lang. Hear. Res. 2020, 63, 405–420. [Google Scholar] [CrossRef]
- Mehta, D.D.; Van Stan, J.H.; Zañartu, M.; Ghassemi, M.; Guttag, J.V.; Espinoza, V.M.; Cortés, J.P.; Cheyne, H.A.; Hillman, R.E. Using Ambulatory Voice Monitoring to Investigate Common Voice Disorders: Research Update. Front. Bioeng. Biotechnol. 2015, 3, 155. [Google Scholar] [CrossRef] [Green Version]
- McCrea, C.R.; Morris, R.J. The Effects of Fundamental Frequency Level on Voice Onset Time in Normal Adult Male Speakers. J. Speech Lang. Hear. Res. 2005, 48, 1013–1024. [Google Scholar] [CrossRef] [PubMed]
- Bohlender, J.E.; Mehta, D.D. Acoustic Perturbation Measures Improve with Increasing Vocal Intensity in Individuals with and without Voice Disorders. J. Voice 2017, 32, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Sampaio, M.; Vaz Masson, M.L.; de Paula Soares, M.F.; Bohlender, J.E.; Brockmann-Bauser, M. Effects of Fundamental Frequency, Vocal Intensity, Sample Duration, and Vowel Context in Cepstral and Spectral Measures of Dysphonic Voices. J. Speech Lang. Hear. Res. 2020, 63, 1326–1339. [Google Scholar] [CrossRef] [PubMed]
- Kempster, G.B.; Gerratt, B.R.; Abbott, K.V.; Barkmeier-Kraemer, J.; Hillman, R.E. Consensus Auditory-Perceptual Evaluation of Voice: Development of a Standardized Clinical Protocol. Am. J. Speech-Lang. Pathol. 2009, 18, 124–132. [Google Scholar] [CrossRef] [Green Version]
- Behlau, M.; Alves dos Santos, L.d.M.; Oliveira, G. Cross-Cultural Adaptation and Validation of the Voice Handicap Index Into Brazilian Portuguese. J. Voice 2011, 25, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Gasparini, G.; Behlau, M. Quality of Life: Validation of the Brazilian Version of the Voice-Related Quality of Life (V-RQOL) Measure. J. Voice 2009, 23, 76–81. [Google Scholar] [CrossRef]
- Barbosa, P.A.; Madureira, S. Manual de Fonética Acústica Experimental: Aplicações a Dados do Português, 1st ed.; Cortez Publisher: São Paulo, SP, Brazil, 2015; p. 591. [Google Scholar]
- Titze, I.R. Toward standards in acoustic analysis of voice. J. Voice 1994, 8, 1–7. [Google Scholar] [CrossRef]
- Boersma, P.; Weenink, D. Praat: Doing Phonetics by Computer [Computer Program], version 6.2.06; 2022. Available online: https://www.praat.org (accessed on 1 February 2022).
- Behlau, M.; Rocha, B.; Englert, M.; Madazio, G. Validation of the Brazilian Portuguese CAPE-V Instrument-Br CAPE-V for Auditory-Perceptual Analysis. J. Voice 2022, 36, 586.e15–586.e20. [Google Scholar] [CrossRef]
- Hillenbrand, J.M.; Gayvert, R.T.; Clark, M.J. Phonetics Exercises Using the Alvin Experiment-Control Software. J. Speech Lang. Hear. Res. 2015, 58, 171–184. [Google Scholar] [CrossRef] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Kent, R.A.; Read, C. The Acoustic Analysis of Speech; Singular Publishing Group: San Diego, CA, USA, 1992; p. 238. [Google Scholar]
- Kang, J.; Whalen, D.H. Get VOT Script. Available online: https://github.com/HaskinsLabs/get_vot#readme (accessed on 20 June 2021).
- Kawahara, S. get_intensity_minmax.praat. Available online: http://user.keio.ac.jp/~kawahara/scripts/get_intensity_minmax.praat (accessed on 20 June 2021).
- Bennett, B.M. On multivariate coefficients of variation. Stat. Hefte 1977, 18, 123–128. [Google Scholar] [CrossRef]
- IBM Corp. SPSS Statistics for Machintosh; IBM Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Peterson, S.J.; Foley, S. Clinician’s Guide to Understanding Effect Size, Alpha Level, Power, and Sample Size. Nutr. Clin. Pract. 2021, 36, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Andrade, D.F.; Heuer, R.; Hockstein, N.E.; Castro, E.; Spiegel, J.R.; Sataloff, R.T. The frequency of hard glottal attacks in patients with muscle tension dysphonia, unilateral benign masses and bilateral benign masses. J. Voice 2000, 14, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Uygun, M.N.; Esen Aydinli, F.; Aksoy, S.; Ozcebe, E. Turkish Standardized Reading Passage for the Evaluation of Hard Glottal Attack Occurrence Frequency. J. Voice 2017, 32, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Revis, J.; Giovanni, A.; Triglia, J.M. Influence of voice onset on the perceptual analysis of dysphonia. Folia Phoniatr Logop. 2002, 54, 19–25. [Google Scholar] [CrossRef]
- Alves, M.A.; Dias, E.C.O. Estudo da produção do VOT em plosivas não-vozeadas diante de vogal alta anterior e posterior no português brasileiro. In Proceedings of the IX Encontro do Celsul, Palhoça, SC, Brazil, 20–22 October 2010. [Google Scholar]
- Van Stan, J.H.; Mehta, D.D.; Zeitels, S.M.; Burns, J.A.; Barbu, A.M.; Hillman, R.E. Average Ambulatory Measures of Sound Pressure Level, Fundamental Frequency, and Vocal Dose Do Not Differ Between Adult Females with Phonotraumatic Lesions and Matched Control Subjects. Ann. Otol. Rhinol. Laryngol. 2015, 124, 864–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinoza, V.M.; Zañartu, M.; Van Stan, J.H.; Mehta, D.D.; Hillman, R.E. Glottal Aerodynamic Measures in Women with Phonotraumatic and Nonphonotraumatic Vocal Hyperfunction. J. Speech Lang. Hear. Res. 2017, 60, 2159–2169. [Google Scholar] [CrossRef] [PubMed]
- Van Stan, J.H.; Mehta, D.D.; Ortiz, A.J.; Burns, J.A.; Toles, L.E.; Marks, K.L.; Vangel, M.; Hron, T.; Zeitels, S.; Hillman, R.E. Differences in Weeklong Ambulatory Vocal Behavior Between Female Patients with Phonotraumatic Lesions and Matched Controls. J. Speech Lang. Hear. Res. 2020, 63, 372–384. [Google Scholar] [CrossRef]
- Chen, X.; Xiong, Z.; Hu, J. The Trajectory of Voice Onset Time with Vocal Aging. In Proceedings of the Interspeech, Hyderabad, India, 2–6 September 2018; pp. 1556–1560. [Google Scholar]
- Colton, R.H.; Casper, J.K.; Leonard, R. Compreendendo os Problemas da Voz—Uma Perspectiva Fisiológica no Diagnóstico e Tratamento das Disfonias, 3rd ed.; Revinter: Rio de Janeiro, Brazil, 2010. [Google Scholar]
- Hecker, P.; Steckhan, N.; Eyben, F.; Schuller, B.W.; Arnrich, B. Voice Analysis for Neurological Disorder Recognition—A Systematic Review and Perspective on Emerging Trends. Front. Digit. Health 2022, 4, 842301. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Men (n) | Women (n) | Total (n) | % | ||
|---|---|---|---|---|---|
| Vocal Hyperfunction | NPVH | 3 | 6 | 9 | 29 |
| PVH | 7 | 15 | 22 | 71 |
| Sentence | Word | Vowel | Stress |
|---|---|---|---|
| [ɛ’.ɾi.kə to.m’ow s’u.kw ʤɪ p’e.ɾɐ ya.m’ɔ.ɾɐ] | /p’e.ɾa/ | [e] | Stressed |
| Erica tomou suco de pera e amora | |||
| [pa. pˈaj tr ˈo.ʃi pi.pˈɔ.kɐ kˈẽ.tʃi] | /pa.p’aj/ | [aj] | Unstressed |
| Papai trouxe pipoca quente | /pi.p’ɔ.ka/ | [I] | Unstressed |
| /pi.p’ɔ.ka/ | [ɔ] | Stressed |
| Display | Setting |
|---|---|
| Spectrogram | View range (Hz): 0.0 to 5.00 Window length (s): 0.005 Dynamic Range (dB): 40.0 |
| Pitch setting | View range (Hz): 75 to 500 Unit: Hertz Analysis method: Cross correlation Drawing method: Automatic |
| Formant tracking | Default setting |
| Intensity | Default setting |
| Window zoom to set voicing boundary | 20 to 50 ms |
| [p] Acoustic Feature | Description * |
| Voiced closure interval (VDCLO) | The voiced portion of the stop closure |
| Voiceless closure interval (VLCLO) | The voiceless portion of the stop closure |
| Release (REL) | Release of the burst |
| Aspiration (ASP) | The aspiration after the burst |
| Overall Severity of Dysphonia | Men (n) | Women (n) | Total (n) | % |
|---|---|---|---|---|
| Mild | 8 | 11 | 19 | 61.29 |
| Moderate | 1 | 7 | 8 | 25.81 |
| Severe | 1 | 3 | 4 | 12.90 |
| Total | 10 | 21 | 31 | 100 |
| Gender | n | Mean | SD | Range | Minimum | Maximum | |
|---|---|---|---|---|---|---|---|
| Men | VOT | 40 | 19.39 | 8.18 | 37 | 0 | 37 |
| fo | 40 | 134.74 | 26.07 | 103.0 | 78.0 | 180.0 | |
| SPL | 40 | 55.81 | 5.17 | 20.6 | 45.03 | 65.63 | |
| CV_ƒo | 40 | 1.24 | 0.26 | 1.30 | 0.53 | 1.83 | |
| Women | VOT | 83 | 18.62 | 7.93 | 36 | 0 | 36 |
| fo | 83 | 185.07 | 39.32 | 200.0 | 80 | 281 | |
| SPL | 84 | 58.51 | 4.32 | 19.84 | 48.36 | 68.20 | |
| CV_ƒo | 83 | 1.28 | .342 | 1.80 | .22 | 2.02 |
| Effect | Dependent Variable | F | p-Value | Partial Eta-Square (η2p) | Interpretation Effect Size |
|---|---|---|---|---|---|
| Gender | VOT | 2.45 | 0.12 | 0.02 | |
| Fo | 48.90 | 0.00 | 0.30 | Moderate | |
| SPL | 6.80 | 0.01 | 0.05 | Small | |
| CV_fo | 2.05 | 0.15 | 0.02 | ||
| VH | VOT | 0.01 | 0.90 | 0.00 | |
| Fo | 3.20 | 0.07 | 0.03 | ||
| SPL | 0.26 | 0.60 | 0.00 | ||
| CV_fo | 5.04 | 0.02 | 0.04 | Small | |
| OS | VOT | 6.24 | 0.00 | 0.09 | Small |
| Fo | 0.00 | 0.99 | 0.00 | ||
| SPL | 1.36 | 0.26 | 0.02 | ||
| CV_fo | 0.36 | 0.69 | 0.00 | ||
| VH × OS | VOT | 1.28 | 0.28 | 0.22 | |
| Fo | 4.40 | 0.01 | 0.07 | Small | |
| SPL | 0.10 | 0.90 | 0.00 | ||
| CV_ fo | 0.14 | 0.87 | 0.00 |
| Dependent Variable | (I) OS | (J) OS | Mean Difference (I-J) | Std. Error | Sig | 95% CI | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| VOT | mild | moderate | −4.81 | 1.57 | 0.00 | −8.62 | −0.99 |
| severe | −7.84 | 2.02 | 0.00 | −12.76 | −2.92 | ||
| moderate | severe | −3.03 | 2.26 | 0.55 | −8.53 | 2.47 | |
| fo | mild | moderate | −15.11 | 7.25 | 0.12 | −32.75 | 2.53 |
| severe | 1.37 | 9.35 | 1.00 | −21.38 | 24.11 | ||
| moderate | severe | 16.48 | 10.46 | 0.35 | −8.95 | 41.90 | |
| SPL | mild | moderate | −1.99 | 0.95 | 0.12 | −4.29 | 0.32 |
| severe | −2.84 | 1.22 | 0.06 | −5.82 | 0.13 | ||
| moderate | severe | −0.86 | 1.37 | 1.00 | −4.20 | 2.46 | |
| CV_fo | mild | moderate | 0.06 | 0.06 | 0.89 | −0.09 | 0.23 |
| severe | 0.00 | 0.08 | 1.00 | −0.20 | 0.21 | ||
| moderate | severe | −0.06 | 0.09 | 1.00 | −0.29 | 0.17 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soares, M.F.d.P.; Sampaio, M.; Brockmann-Bauser, M. Interaction of Voice Onset Time with Vocal Hyperfunction and Voice Quality. Appl. Sci. 2023, 13, 8956. https://doi.org/10.3390/app13158956
Soares MFdP, Sampaio M, Brockmann-Bauser M. Interaction of Voice Onset Time with Vocal Hyperfunction and Voice Quality. Applied Sciences. 2023; 13(15):8956. https://doi.org/10.3390/app13158956
Chicago/Turabian StyleSoares, Maria Francisca de Paula, Marília Sampaio, and Meike Brockmann-Bauser. 2023. "Interaction of Voice Onset Time with Vocal Hyperfunction and Voice Quality" Applied Sciences 13, no. 15: 8956. https://doi.org/10.3390/app13158956