
Narrative Review on Methods of Activating Irrigation Liquids for Root Canal Treatment


 ,
,  ,
, {kind=link}
Abstract
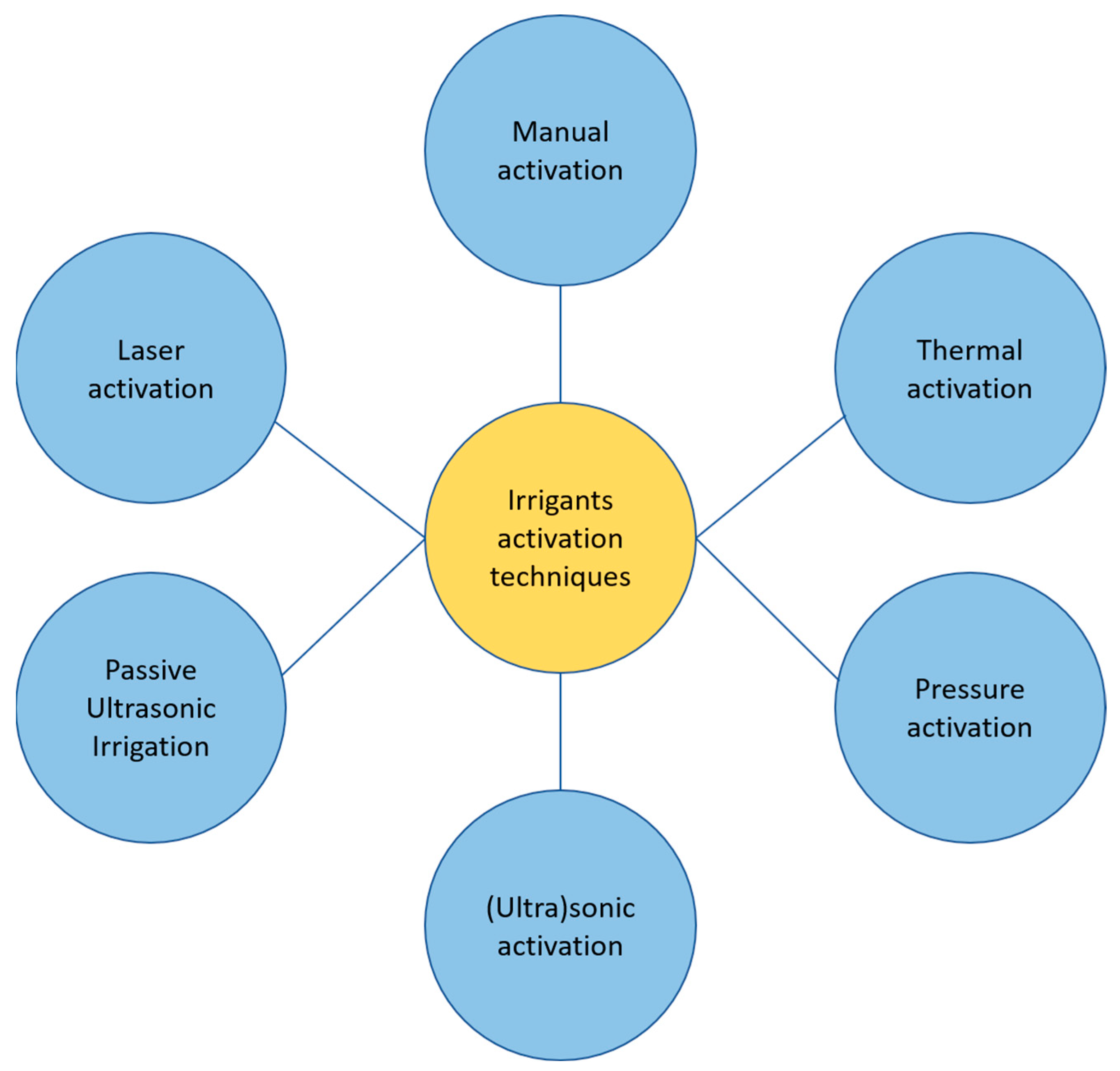
:1. Introduction
- Manual activation;
- Thermal techniques (internal or external to the root);
- Pressure techniques (EndoVac, Kerr Endodontics, Gilbert, AZ, USA; Rinsendo, Dürr Dental, Bietigheim, Germany);
- Sonic/ultrasound techniques (EndoAcivator, Dentsply Maillefer, Ballaigues, Switzerland; EDDY, VDW, München, Germany; Ripsisonic, Medidenta International Inc., Woodside, NY, USA; SAF, ReDent, Ra’anana, Israel);
- Passive Ultrasonic Irrigation (PUI);
- Laser techniques.
2. Materials and Methods
3. Types of Irrigants and Irrigation Protocols
4. Irrigants Activation Techniques
4.1. Manual Activation
4.2. Thermal Techniques
4.3. Ultrasound Techniques
4.4. Laser Activation Techniques
4.5. Other Activation Systems
5. Efficacy of Activation Systems in Curved Canals
6. Discussion
7. Final Remarks
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Giraud, T.; Jeanneau, C.; Rombouts, C.; Bakhtiar, H.; Laurent, P.; About, I. Pulp Capping Materials Modulate the Balance between Inflammation and Regeneration. Dent. Mater. 2019, 35, 24–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathur, V.P.; Dhillon, J.K. Dental Caries: A Disease Which Needs Attention. Indian J. Pediatr. 2018, 85, 202–206. [Google Scholar] [CrossRef] [PubMed]
- MacHiulskiene, V.; Campus, G.; Carvalho, J.C.; Dige, I.; Ekstrand, K.R.; Jablonski-Momeni, A.; Maltz, M.; Manton, D.J.; Martignon, S.; Martinez-Mier, E.A.; et al. Terminology of Dental Caries and Dental Caries Management: Consensus Report of a Workshop Organized by ORCA and Cariology Research Group of IADR. Caries Res. 2020, 54, 7–14. [Google Scholar] [CrossRef]
- Wong, J.; Cheung, G.S.P.; Lee, A.H.C.; McGrath, C.; Neelakantan, P. PROMs following Root Canal Treatment and Surgical Endodontic Treatment. Int. Dent. J. 2023, 73, 28–41. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, J.C.; Cuenin, P.R. Efficacy of Several Concentrations of Sodium Hypochlorite for Root Canal Irrigation. J. Endod. 1992, 18, 605–612. [Google Scholar] [CrossRef]
- Zehnder, M. Root Canal Irrigants. J. Endod. 2006, 32, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Bhosale, A.; Pawar, S.; Kakti, A.; Bichpuriya, A.; Agwan, M.A. Current Trends in Root Canal Irrigation. Cureus 2022, 14, e24833. [Google Scholar] [CrossRef]
- Vivekananda Pai, A.R. Factors Influencing the Occurrence and Progress of Sodium Hypochlorite Accident: A Narrative and Update Review. J. Conserv. Dent. 2023, 26, 3–11. [Google Scholar] [CrossRef]
- Peters, O.A.; Boessler, C.; Zehnder, M. Effect of Liquid and Paste-Type Lubricants on Torque Values during Simulated Rotary Root Canal Instrumentation. Int. Endod. J. 2005, 38, 223–229. [Google Scholar] [CrossRef]
- Wong, S.; Mundy, L.; Chandler, N.; Upritchard, J.; Purton, D.; Tompkins, G. Antibacterial Properties of Root Canal Lubricants: A Comparison with Commonly Used Irrigants. Aust. Endod. J. 2014, 40, 111–115. [Google Scholar] [CrossRef]
- Boessler, C.; Peters, O.A.; Zehnder, M. Impact of Lubricant Parameters on Rotary Instrument Torque and Force. J. Endod. 2007, 33, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Jahromi, M.Z.; Fathi, M.H.; Zamiran, S. Experimental Study of Smear Layer and Debris Remaining following the Use of Four Root Canal Preparation Systems Using Scanning Electron Microscopy. J. Islam. Dent. Assoc. Iran 2013, 25, 235–241. [Google Scholar]
- Jena, A.; Sahoo, S.K.; Govind, S. Root Canal Irrigants: A Review of Their Interactions, Benefits, and Limitations. Compend. Contin. Educ. Dent. 2015, 36, 256–261. [Google Scholar] [PubMed]
- Violich, D.R.; Chandler, N.P. The Smear Layer in Endodontics—A Review. Int. Endod. J. 2010, 43, 2–15. [Google Scholar] [CrossRef]
- Roberti, F.; Savaris, J.M.; Tay, F.R.; Bortoluzzi, A. Smear Layer Removal Using Passive Ultrasonic Irrigation and Different Concentrations of Sodium Hypochlorite. J. Endod. 2020, 46, 1738–1744. [Google Scholar] [CrossRef]
- Niu, W.; Yoshioka, T.; Kobayashi, C.; Suda, H. A Scanning Electron Microscopic Study of Dentinal Erosion by Final Irrigation with EDTA and NaOCl Solutions. Int. Endod. J. 2002, 35, 934–939. [Google Scholar] [CrossRef]
- Olivieri, J.G.; García Font, M.; Stöber, E.; de Ribot, J.; Mercadé, M.; Duran-Sindreu, F. Effect of Manual Dynamic Activation with Citric Acid Solutions in Smear Layer Removal: A Scanning Electron Microscopic Evaluation. J. Dent. Sci. 2016, 11, 360–364. [Google Scholar] [CrossRef] [Green Version]
- Silva, P.V.; Guedes, D.F.C.; Pécora, J.D.; da Cruz-Filho, A.M. Time-Dependent Effects of Chitosan on Dentin Structures. Braz. Dent. J. 2012, 23, 357–361. [Google Scholar] [CrossRef] [Green Version]
- Kuah, H.G.; Lui, J.N.; Tseng, P.S.K.; Chen, N.N. The Effect of EDTA with and without Ultrasonics on Removal of the Smear Layer. J. Endod. 2009, 35, 393–396. [Google Scholar] [CrossRef]
- Yamada, R.S.; Armas, A.; Goldman, M.; Lin, P.S. A Scanning Electron Microscopic Comparison of a High Volume Final Flush with Several Irrigating Solutions: Part 3. J. Endod. 1983, 9, 137–142. [Google Scholar] [CrossRef]
- Berber, V.B.; Gomes, B.P.F.A.; Sena, N.T.; Vianna, M.E.; Ferraz, C.C.R.; Zaia, A.A.; Souza-Filho, F.J. Efficacy of Various Concentrations of NaOCl and Instrumentation Techniques in Reducing Enterococcus Faecalis within Root Canals and Dentinal Tubules. Int. Endod. J. 2006, 39, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F.; Rôças, I.N.; Favieri, A.; Lima, K.C. Chemomechanical Reduction of the Bacterial Population in the Root Canal after Instrumentation and Irrigation with 1%, 2.5%, and 5.25% Sodium Hypochlorite. J. Endod. 2000, 26, 331–334. [Google Scholar] [CrossRef]
- Yesilsoy, C.; Whitaker, E.; Cleveland, D.; Phillips, E.; Trope, M. Antimicrobial and Toxic Effects of Established and Potential Root Canal Irrigants. J. Endod. 1995, 21, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Önçaǧ, Ö.; Hoşgör, M.; Hilmioǧlu, S.; Zekioǧlu, O.; Eronat, C.; Burhanoǧlu, D. Comparison of Antibacterial and Toxic Effects of Various Root Canal Irrigants. Int. Endod. J. 2003, 36, 423–432. [Google Scholar] [CrossRef]
- Williamson, A.E.; Cardon, J.W.; Drake, D.R. Antimicrobial Susceptibility of Monoculture Biofilms of a Clinical Isolate of Enterococcus Faecalis. J. Endod. 2009, 35, 95–97. [Google Scholar] [CrossRef]
- Dunavant, T.R.; Regan, J.D.; Glickman, G.N.; Solomon, E.S.; Honeyman, A.L. Comparative Evaluation of Endodontic Irrigants against Enterococcus Faecalis Biofilms. J. Endod. 2006, 32, 527–531. [Google Scholar] [CrossRef]
- Ruksakiet, K.; Hanák, L.; Farkas, N.; Hegyi, P.; Sadaeng, W.; Czumbel, L.M.; Sang-ngoen, T.; Garami, A.; Mikó, A.; Varga, G.; et al. Antimicrobial Efficacy of Chlorhexidine and Sodium Hypochlorite in Root Canal Disinfection: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Endod. 2020, 46, 1032–1041.e7. [Google Scholar] [CrossRef] [PubMed]
- Zamany, A.; Safavi, K.; Spångberg, L.S.W. The Effect of Chlorhexidine as an Endodontic Disinfectant. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 578–581. [Google Scholar] [CrossRef]
- Dioguardi, M.; Di Gioia, G.; Illuzzi, G.; Laneve, E.; Cocco, A.; Troiano, G. Endodontic Irrigants: Different Methods to Improve Efficacy and Related Problems. Eur. J. Dent. 2018, 12, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, C.S.; Felippe, M.C.S.; Felippe, W.T. The Effect of Application Time of EDTA and NaOCI on Intracanal Smear Layer Removal: An SEM Analysis. Int. Endod. J. 2005, 38, 285–290. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Arias-Moliz, M.T. Present Status and Future Directions—Irrigants and Irrigation Methods. Int. Endod. J. 2022, 55, 588–612. [Google Scholar] [CrossRef] [PubMed]
- Rito Pereira, M.; Silva, G.; Semiao, V.; Silverio, V.; Martins, J.N.R.; Pascoal-Faria, P.; Alves, N.; Dias, J.R.; Ginjeira, A. Experimental Validation of a Computational Fluid Dynamics Model Using Micro-Particle Image Velocimetry of the Irrigation Flow in Confluent Canals. Int. Endod. J. 2022, 55, 1394–1403. [Google Scholar] [CrossRef]
- Pladisai, P.; Ampornaramveth, R.S.; Chivatxaranukul, P. Effectiveness of Different Disinfection Protocols on the Reduction of Bacteria in Enterococcus Faecalis Biofilm in Teeth with Large Root Canals. J. Endod. 2016, 42, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Stojicic, S.; Zivkovic, S.; Qian, W.; Zhang, H.; Haapasalo, M. Tissue Dissolution by Sodium Hypochlorite: Effect of Concentration, Temperature, Agitation, and Surfactant. J. Endod. 2010, 36, 1558–1562. [Google Scholar] [CrossRef] [PubMed]
- Boutsioukis, C.; Lambrianidis, T.; Kastrinakis, E. Irrigant Flow within a Prepared Root Canal Using Various Flow Rates: A Computational Fluid Dynamics Study. Int. Endod. J. 2009, 42, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Abou-Rass, M.; Piccinino, M. V The Effectiveness of Four Clinical Irrigation Methods on the Removal of Root Canal Debris. Oral Surg. Oral Med. Oral Pathol. 1982, 54, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Boutsioukis, C.; Lambrianidis, T.; Kastrinakis, E.; Bekiaroglou, P. Measurement of Pressure and Flow Rates during Irrigation of a Root Canal Ex Vivo with Three Endodontic Needles. Int. Endod. J. 2007, 40, 504–513. [Google Scholar] [CrossRef]
- Barańska-Gachowska, M. Endodoncja Wieku Rozwojowego i Dojrzałego, 3rd ed.; Czelej: Lublin, Poland, 2021; ISBN 9788375633061. [Google Scholar]
- Andrabi, S.M.U.N.; Kumar, A.; Mishra, S.K.; Tewari, R.K.; Alam, S.; Siddiqui, S. Effect of Manual Dynamic Activation on Smear Layer Removal Efficacy of Ethylenediaminetetraacetic Acid and SmearClear: An in Vitro Scanning Electron Microscopic Study. Aust. Endod. J. 2013, 39, 131–136. [Google Scholar] [CrossRef]
- Khaord, P.; Amin, A.; Shah, M.; Uthappa, R.; Raj, N.; Kachalia, T.; Kharod, H. Effectiveness of Different Irrigation Techniques on Smear Layer Removal in Apical Thirds of Mesial Root Canals of Permanent Mandibular First Molar: A Scanning Electron Microscopic Study. J. Conserv. Dent. 2015, 18, 321–326. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.Y.; Gulabivala, K.; Ng, Y.L. A Bio-Molecular Film Ex-Vivo Model to Evaluate the Influence of Canal Dimensions and Irrigation Variables on the Efficacy of Irrigation. Int. Endod. J. 2008, 41, 60–71. [Google Scholar] [CrossRef]
- Topçuoğlu, H.S.; Topçuoğlu, G.; Arslan, H. The Effect of Different Irrigation Agitation Techniques on Postoperative Pain in Mandibular Molar Teeth with Symptomatic Irreversible Pulpitis: A Randomized Clinical Trial. J. Endod. 2018, 44, 1451–1456. [Google Scholar] [CrossRef] [PubMed]
- Iandolo, A.; Iandolo, G.; Malvano, M.; Pantaleo, G.; Simeone, M. Modern Technologies in Endodontics. G. Ital. Endod. 2016, 30, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, W.T.; Cole, J.S.; Balekjian, A.Y. Effect of Alcohol on the Spreading Ability of Sodium Hypochlorite Endodontic Irrigant. Oral Surg. Oral Med. Oral Pathol. 1982, 54, 333–335. [Google Scholar] [CrossRef] [PubMed]
- Sirtes, G.; Waltimo, T.; Schaetzle, M.; Zehnder, M. The Effects of Temperature on Sodium Hypochlorite Short-Term Stability, Pulp Dissolution Capacity, and Antimicrobial Efficacy. J. Endod. 2005, 31, 669–671. [Google Scholar] [CrossRef] [Green Version]
- De Hemptinne, F.; Slaus, G.; Vandendael, M.; Jacquet, W.; De Moor, R.J.; Bottenberg, P. In Vivo Intracanal Temperature Evolution during Endodontic Treatment after the Injection of Room Temperature or Preheated Sodium Hypochlorite. J. Endod. 2015, 41, 1112–1115. [Google Scholar] [CrossRef]
- Mohammadi, Z. Sodium Hypochlorite in Endodontics: An Update Review. Int. Dent. J. 2008, 58, 329–341. [Google Scholar] [CrossRef]
- Wright, P.P.; Kahler, B.; Walsh, L.J. The Effect of Heating to Intracanal Temperature on the Stability of Sodium Hypochlorite Admixed with Etidronate or EDTA for Continuous Chelation. J. Endod. 2019, 45, 57–61. [Google Scholar] [CrossRef]
- Ertugrul, I.F.; Maden, M.; Orhan, E.O.; Ozkorucuklu, S.P.; Aglarca, A.V. Rapid Tissue Dissolution Efficiency of Electrically-Activated Sodium Hypochlorite on Bovine Muscle. Eur. J. Dent. 2014, 08, 464–468. [Google Scholar] [CrossRef]
- Jaiswal, S.; Gupta, S.; Nikhil, V.; Bhadoria, A.; Raj, S. Effect of Intracanal and Extracanal Heating on Pulp Dissolution Property of Continuous Chelation Irrigant. J. Conserv. Dent. 2021, 24, 544–548. [Google Scholar] [CrossRef]
- Iandolo, A.; Amato, M.; Dagna, A.; Poggio, C.; Abdellatif, D.; Franco, V.; Pantaleo, G. Intracanal Heating of Sodium Hypochlorite: Scanning Electron Microscope Evaluation of Root Canal Walls. J. Conserv. Dent. 2018, 21, 569. [Google Scholar] [CrossRef]
- Iandolo, A.; Abdellatif, D.; Amato, M.; Pantaleo, G.; Blasi, A.; Franco, V.; Neelakantan, P. Dentinal Tubule Penetration and Root Canal Cleanliness following Ultrasonic Activation of Intracanal-Heated Sodium Hypochlorite. Aust. Endod. J. 2020, 46, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.; Pantaleo, G.; Abtellatif, D.; Blasi, A.; Gagliani, M.; Iandolo, A. An in Vitro Evaluation of the Degree of Pulp Tissue Dissolution through Different Root Canal Irrigation Protocols. J. Conserv. Dent. 2018, 21, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Plotino, G.; Pameijer, C.H.; Maria Grande, N.; Somma, F. Ultrasonics in Endodontics: A Review of the Literature. J. Endod. 2007, 33, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Macedo, R.G.; Verhaagen, B.; Rivas, D.F.; Versluis, M.; Wesselink, P.; Van Der Sluis, L. Cavitation Measurement during Sonic and Ultrasonic Activated Irrigation. J. Endod. 2014, 40, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Sabins, R.A.; Johnson, J.D.; Hellstein, J.W. A Comparison of the Cleaning Efficacy of Short-Term Sonic and Ultrasonic Passive Irrigation after Hand Instrumentation in Molar Root Canals. J. Endod. 2003, 29, 674–678. [Google Scholar] [CrossRef]
- Castelo-Baz, P.; Martín-Biedma, B.; Cantatore, G.; Ruíz-Piñón, M.; Bahillo, J.; Rivas-Mundiña, B.; Varela-Patiño, P. In Vitro Comparison of Passive and Continuous Ultrasonic Irrigation in Simulated Lateral Canals of Extracted Teeth. J. Endod. 2012, 38, 688–691. [Google Scholar] [CrossRef]
- Caron, G.; Nham, K.; Bronnec, F.; MacHtou, P. Effectiveness of Different Final Irrigant Activation Protocols on Smear Layer Removal in Curved Canals. J. Endod. 2010, 36, 1361–1366. [Google Scholar] [CrossRef]
- Al-Jadaa, A.; Paqué, F.; Attin, T.; Zehnder, M. Acoustic Hypochlorite Activation in Simulated Curved Canals. J. Endod. 2009, 35, 1408–1411. [Google Scholar] [CrossRef] [Green Version]
- Guerisoli, D.M.Z.; Marchesan, M.A.; Walmsley, A.D.; Lumley, P.J.; Pecora, J.D. Evaluation of Smear Layer Removal by EDTAC and Sodium Hypochlorite with Ultrasonic Agitation. Int. Endod. J. 2002, 35, 418–421. [Google Scholar] [CrossRef]
- Van Der Sluis, L.W.M.; Wu, M.K.; Wesselink, P.R. The Evaluation of Removal of Calcium Hydroxide Paste from an Artificial Standardized Groove in the Apical Root Canal Using Different Irrigation Methodologies. Int. Endod. J. 2007, 40, 52–57. [Google Scholar] [CrossRef]
- McGill, S.; Gulabivala, K.; Mordan, N.; Ng, Y.L. The Efficacy of Dynamic Irrigation Using a Commercially Available System (RinsEndo®) Determined by Removal of a Collagen “bio-Molecular Film” from an Ex Vivo Model. Int. Endod. J. 2008, 41, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Xiang, D.; He, W.; Qiu, J.; Han, B.; Yu, Q.; Tian, Y. Bactericidal Effect of Er:YAG Laser-Activated Sodium Hypochlorite Irrigation Against Biofilms of Enterococcus Faecalis Isolate from Canal of Root-Filled Teeth with Periapical Lesions. Photomed. Laser Surg. 2017, 35, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Huang, Z.; Ju, Y.; Tang, X. Bactericidal Efficacy of Three Parameters of Nd:YAP Laser Irradiation against Enterococcus Faecalis Compared with NaOCl Irrigation. Lasers Med. Sci. 2019, 34, 359–366. [Google Scholar] [CrossRef] [PubMed]
- De Meyer, S.; Meire, M.A.; Coenye, T.; De Moor, R.J.G. Effect of Laser-Activated Irrigation on Biofilms in Artificial Root Canals. Int. Endod. J. 2017, 50, 472–479. [Google Scholar] [CrossRef]
- Nagahashi, T.; Yahata, Y.; Handa, K.; Nakano, M.; Suzuki, S.; Kakiuchi, Y.; Tanaka, T.; Kanehira, M.; Suresh Venkataiah, V.; Saito, M. Er:YAG Laser-Induced Cavitation Can Activate Irrigation for the Removal of Intraradicular Biofilm. Sci. Rep. 2022, 12, 4897. [Google Scholar] [CrossRef]
- Wang, X.; Cheng, X.; Liu, B.; Liu, X.; Yu, Q.; He, W. Effect of Laser-Activated Irrigations on Smear Layer Removal from the Root Canal Wall. Photomed. Laser Surg. 2017, 35, 688–694. [Google Scholar] [CrossRef]
- George, R.; Meyers, I.A.; Walsh, L.J. Laser Activation of Endodontic Irrigants with Improved Conical Laser Fiber Tips for Removing Smear Layer in the Apical Third of the Root Canal. J. Endod. 2008, 34, 1524–1527. [Google Scholar] [CrossRef] [Green Version]
- Mikołajczyk, M. Laseroterapia w Endodoncji. Forum Stomatol. Prakt. 2014, 30–42. Available online: https://www.praktycznastomatologia.pl/artykul/laseroterapia-w-endodoncji (accessed on 10 May 2023).
- Arslan, H.; Capar, I.D.; Saygili, G.; Gok, T.; Akcay, M. Effect of Photon-Initiated Photoacoustic Streaming on Removal of Apically Placed Dentinal Debris. Int. Endod. J. 2014, 47, 1072–1077. [Google Scholar] [CrossRef]
- Koch, J.D.; Jaramillo, D.E.; DiVito, E.; Peters, O.A. Irrigant Flow during Photon-Induced Photoacoustic Streaming (PIPS) Using Particle Image Velocimetry (PIV). Clin. Oral Investig. 2016, 20, 381–386. [Google Scholar] [CrossRef]
- Yost, R.A.; Bergeron, B.E.; Kirkpatrick, T.C.; Roberts, M.D.; Roberts, H.W.; Himel, V.T.; Sabey, K.A. Evaluation of 4 Different Irrigating Systems for Apical Extrusion of Sodium Hypochlorite. J. Endod. 2015, 41, 1530–1534. [Google Scholar] [CrossRef] [PubMed]
- De Groot, S.D.; Verhaagen, B.; Versluis, M.; Wu, M.K.; Wesselink, P.R.; Van Der Sluis, L.W.M. Laser-Activated Irrigation within Root Canals: Cleaning Efficacy and Flow Visualization. Int. Endod. J. 2009, 42, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Bogari, D.F.; Alessa, M.; Aljaber, M.; Alghamdi, F.; Alamoudi, M.; Alhamed, M.; Alghamdi, A.J.; Elsherief, S.; Almalki, M.; Alhazzazi, T.Y. The Biological and Mechanical Effect of Using Different Irrigation Methods on the Bond Strength of Bioceramic Sealer to Root Dentin Walls. Cureus 2022, 14, e24022. [Google Scholar] [CrossRef]
- Korkut, E.; Torlak, E.; Gezgin, O.; Özer, H.; Sener, Y. Antibacterial and Smear Layer Removal Efficacy of Er:YAG Laser Irradiation by Photon-Induced Photoacoustic Streaming in Primary Molar Root Canals: A Preliminary Study. Photomed. Laser Surg. 2018, 36, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Golob, B.S.; Olivi, G.; Vrabec, M.; El Feghali, R.; Parker, S.; Benedicenti, S. Efficacy of Photon-Induced Photoacoustic Streaming in the Reduction of Enterococcus Faecalis within the Root Canal: Different Settings and Different Sodium Hypochlorite Concentrations. J. Endod. 2017, 43, 1730–1735. [Google Scholar] [CrossRef] [PubMed]
- Azim, A.A.; Aksel, H.; Zhuang, T.; Mashtare, T.; Babu, J.P.; Huang, G.T.-G. Efficacy of 4 Irrigation Protocols in Killing Bacteria Colonized in Dentinal Tubules Examined by a Novel Confocal Laser Scanning Microscope Analysis. J. Endod. 2016, 42, 928–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, B.A.; Craig Baumgartner, J. Comparison of the EndoVac System to Needle Irrigation of Root Canals. J. Endod. 2007, 33, 611–615. [Google Scholar] [CrossRef]
- Kumar, R.S.; Ankola, A.; Peerzade, M.; Sankeshwari, R.; Hampiholi, V.; Pai Khot, A.; Shah, M.A. Comparative Efficacy of Different Irrigant Activation Techniques for Irrigant Delivery Up to the Working Length of Mature Permanent Teeth: A Systematic Review and Meta-Analysis. Eur. Endod. J. 2023, 8, 1–19. [Google Scholar] [CrossRef]
- Gondim, E.; Setzer, F.C.; Dos Carmo, C.B.; Kim, S. Postoperative Pain after the Application of Two Different Irrigation Devices in a Prospective Randomized Clinical Trial. J. Endod. 2010, 36, 1295–1301. [Google Scholar] [CrossRef] [Green Version]
- Parente, J.M.; Loushine, R.J.; Susin, L.; Gu, L.; Looney, S.W.; Weller, R.N.; Pashley, D.H.; Tay, F.R. Root Canal Debridement Using Manual Dynamic Agitation or the EndoVac for Final Irrigation in a Closed System and an Open System. Int. Endod. J. 2010, 43, 1001–1012. [Google Scholar] [CrossRef]
- Desai, P.; Himel, V. Comparative Safety of Various Intracanal Irrigation Systems. J. Endod. 2009, 35, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Malentacca, A.; Uccioli, U.; Zangari, D.; Lajolo, C.; Fabiani, C. Efficacy and Safety of Various Active Irrigation Devices When Used with Either Positive or Negative Pressure: An in Vitro Study. J. Endod. 2012, 38, 1622–1626. [Google Scholar] [CrossRef] [PubMed]
- Hauser, V.; Braun, A.; Frentzen, M. Penetration Depth of a Dye Marker into Dentine Using a Novel Hydrodynamic System (RinsEndo®). Int. Endod. J. 2007, 40, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Uzunoglu-Özyürek, E.; Dik Güzel, C.; Dogan Buzoglu, H. Effect of Different Irrigation Methods in the Presence of a Separated Instrument: An in Vitro Study. Acta Odontol. Scand. 2020, 78, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Klyn, S.L.; Kirkpatrick, T.C.; Rutledge, R.E. In Vitro Comparisons of Debris Removal of the EndoActivatorTM System, the F FileTM, Ultrasonic Irrigation, and NaOCl Irrigation Alone after Hand-Rotary Instrumentation in Human Mandibular Molars. J. Endod. 2010, 36, 1367–1371. [Google Scholar] [CrossRef] [PubMed]
- Ruddle, C. Endodontic Disinfection: Tsunami Irrigation. Saudi Endod. J. 2015, 5, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Chu, X.; Feng, S.; Zhou, W.; Xu, S.; Zeng, X. Cleaning Efficacy of EDDY versus Ultrasonically-Activated Irrigation in Root Canals: A Systematic Review and Meta-Analysis. BMC Oral Health 2023, 23, 155. [Google Scholar] [CrossRef]
- Urban, K.; Donnermeyer, D.; Schäfer, E.; Bürklein, S. Canal Cleanliness Using Different Irrigation Activation Systems: A SEM Evaluation. Clin. Oral Investig. 2017, 21, 2681–2687. [Google Scholar] [CrossRef]
- Güven, Y.; Uygun, A.D.; Arslan, H. Efficacy of EDDY, Ultrasonic Activation, XP-Endo Finisher and Needle Irrigation on the Removal of MTAP from Artificially Created Grooves in Root Canals. Aust. Endod. J. 2021, 47, 639–644. [Google Scholar] [CrossRef]
- Swimberghe, R.C.D.; Buyse, R.; Meire, M.A.; De Moor, R.J.G. Efficacy of Different Irrigation Technique in Simulated Curved Root Canals. Lasers Med. Sci. 2021, 36, 1317–1322. [Google Scholar] [CrossRef]
- Dewsnup, N.; Pileggi, R.; Haddix, J.; Nair, U.; Walker, C.; Varella, C.H. Comparison of Bacterial Reduction in Straight and Curved Canals Using Erbium, Chromium:Yttrium-Scandium-Gallium-Garnet Laser Treatment versus a Traditional Irrigation Technique With Sodium Hypochlorite. J. Endod. 2010, 36, 725–728. [Google Scholar] [CrossRef]
- Haupt, F.; Meinel, M.; Gunawardana, A.; Hülsmann, M. Effectiveness of Different Activated Irrigation Techniques on Debris and Smear Layer Removal from Curved Root Canals: A SEM Evaluation. Aust. Endod. J. 2020, 46, 40–46. [Google Scholar] [CrossRef]
- Pitt Ford, T.R.; Riccucci, D.; Saunders, E.M.; Stabholz, A.; Suter, B. Quality Guidelines for Endodontic Treatment: Consensus Report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef]
- British Endodontic Society A Guide to Good Endodontic Practice. 2022. Available online: https://britishendodonticsociety.org.uk/_userfiles/pages/files/a4_bes_guidelines_2022_hyperlinked_final.pdf?fbclid=IwAR2AGaq0xMu2FbqJTy6CDcyX-hQfOqorYZwYQ4FwF2G3YdPANPUTDQS_KqU (accessed on 28 May 2023).
- Mozo, S.; Llena, C.; Forner, L. Review of Ultrasonic Irrigation in Endodontics: Increasing Action of Irrigating Solutions. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e512–e516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagendrababu, V.; Jayaraman, J.; Suresh, A.; Kalyanasundaram, S.; Neelakantan, P. Effectiveness of Ultrasonically Activated Irrigation on Root Canal Disinfection: A Systematic Review of in Vitro Studies. Clin. Oral Investig. 2018, 22, 655–670. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raducka, M.; Piszko, A.; Piszko, P.J.; Jawor, N.; Dobrzyński, M.; Grzebieluch, W.; Mikulewicz, M.; Skośkiewicz-Malinowska, K. Narrative Review on Methods of Activating Irrigation Liquids for Root Canal Treatment. Appl. Sci. 2023, 13, 7733. https://doi.org/10.3390/app13137733
Raducka M, Piszko A, Piszko PJ, Jawor N, Dobrzyński M, Grzebieluch W, Mikulewicz M, Skośkiewicz-Malinowska K. Narrative Review on Methods of Activating Irrigation Liquids for Root Canal Treatment. Applied Sciences. 2023; 13(13):7733. https://doi.org/10.3390/app13137733
Chicago/Turabian StyleRaducka, Martyna, Aleksandra Piszko, Paweł J. Piszko, Natalia Jawor, Maciej Dobrzyński, Wojciech Grzebieluch, Marcin Mikulewicz, and Katarzyna Skośkiewicz-Malinowska. 2023. "Narrative Review on Methods of Activating Irrigation Liquids for Root Canal Treatment" Applied Sciences 13, no. 13: 7733. https://doi.org/10.3390/app13137733