
Feasibility of Osseous Landmarks for ACL Reconstruction—A Macroscopic Anatomical Study

Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Specimens
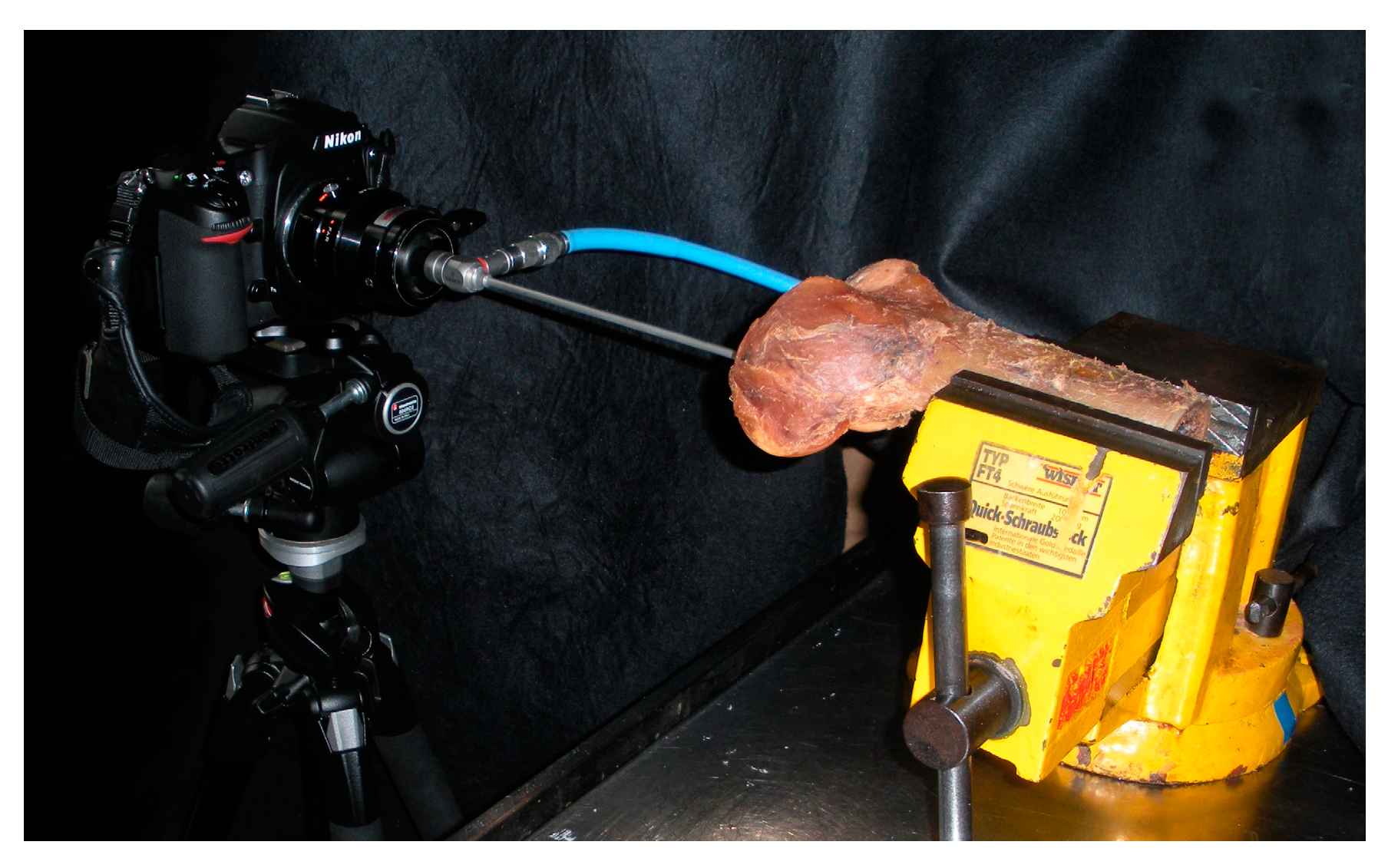
2.2. Photographic Setting and Specimen Preparation
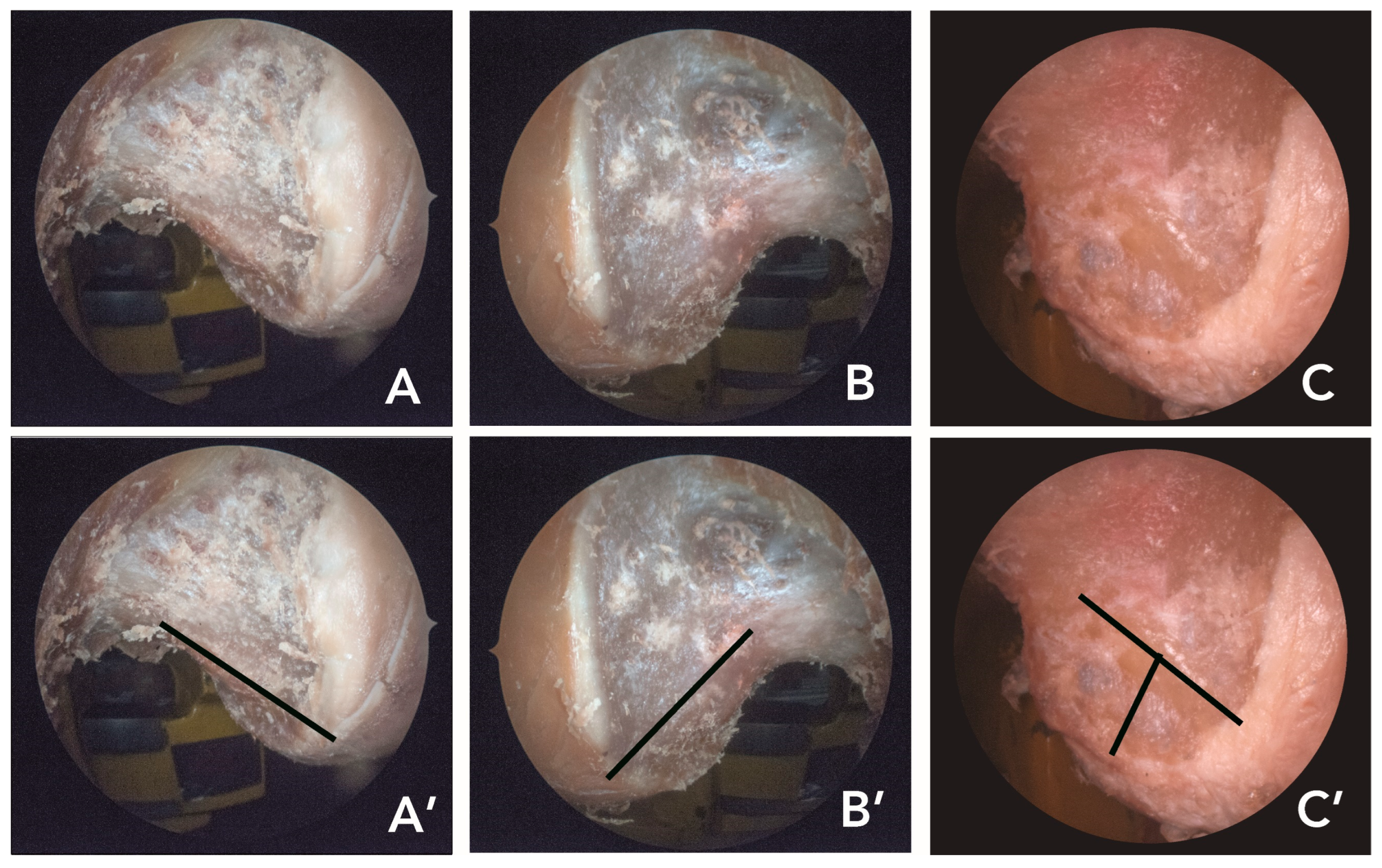
2.3. Identification of the Ridges as Control
2.4. Evaluation
- Medical student (6th year): Anatomical tutor experienced in general macroscopic anatomy, who was given a short introduction regarding the existence and location of the two ridges.
- Anatomist: Research focus is on bone and joint anatomy, has some in-depth knowledge of the ridges but minor experience in arthroscopy.
- Orthopedic surgeon: Specialized in knee arthroscopy with a focus on ACL reconstruction, high level of surgical experience.
2.5. Statistical Analysis
2.6. Intra-Rater Reliability
3. Results
3.1. Control Data
3.2. Comparison of the Subjects
3.3. Intra-Rater Reliability
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Cheatham, S.A.; Johnson, D.L. Anatomic Revision ACL Reconstruction. Sports Med. Arthrosc. Rev. 2010, 18, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Forkel, P.; Achtnich, A.; Metzlaff, S.; Zantop, T.; Petersen, W. Causes for revision after arthoscopic reconstruction of the anterior cruciate ligament: A retrospective review of preoperative findings of 100 cases of revision. Unfallchirurg 2011, (Suppl. S2), 119. [Google Scholar]
- Jorge, P.B.; Escudeiro, D.; Severino, N.R.; Santili, C.; Cury, R.D.P.L.; Junior, A.D.; Guglielmetti, L.G.B. Positioning of the femoral tunnel in anterior cruciate ligament reconstruction: Functional anatomical reconstruction. BMJ Open Sport Exerc. Med. 2018, 4, e000420. [Google Scholar] [CrossRef] [PubMed]
- Rowan, F.A.; Marshall, T.; Gombosh, M.R.; Farrow, L.D. Utilization of Osseous Landmarks for Anatomic Anterior Cruciate Ligament Femoral Tunnel Placement. J. Knee Surg. 2017, 30, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, M.; Ekdahl, M.; Shen, W.; Fu, F.H. Osseous Landmarks of the Femoral Attachment of the Anterior Cruciate Ligament: An Anatomic Study. Arthrosc. J. Arthrosc. Relat. Surg. 2007, 23, 1218–1225. [Google Scholar] [CrossRef]
- Petersen, W.; Zantop, T. Anatomy of the Anterior Cruciate Ligament with Regard to Its Two Bundles. Clin. Orthop. Relat. Res. 2007, 454, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Bicer, E.K.; Lustig, S.; Servien, E.; Selmi, T.A.S.; Neyret, P. Current knowledge in the anatomy of the human anterior cruciate ligament. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 1075–1084. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, M.R.; Ash, S.A. Resident’s ridge: Assessing the cortical thickness of the lateral wall and roof of the intercondylar notch. Arthrosc. J. Arthrosc. Relat. Surg. 2003, 19, 931–935. [Google Scholar] [CrossRef]
- Fu, F.H.; Jordan, S.S. The lateral intercondylar ridge—A key to anatomic anterior cruciate ligament reconstruction. J. Bone Jt. Surg. Am. 2007, 89, 2103–2104. [Google Scholar]
- Kopf, S.; Musahl, V.; Tashman, S.; Szczodry, M.; Shen, W.; Fu, F.H. A systematic review of the femoral origin and tibial insertion morphology of the ACL. Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 213–219. [Google Scholar] [CrossRef]
- Forsythe, B.; Kopf, S.; Wong, A.K.; Martins, C.A.; Anderst, W.; Tashman, S.; Fu, F.H. The Location of Femoral and Tibial Tunnels in Anatomic Double-Bundle Anterior Cruciate Ligament Reconstruction Analyzed by Three-Dimensional Computed Tomography Models. J. Bone Jt. Surg. 2010, 92, 1418–1426. [Google Scholar] [CrossRef] [Green Version]
- Abrams, D.A.; Nicol, T.; Zecker, S.; Kraus, N. Rapid acoustic processing in the auditory brainstem is not related to cortical asymmetry for the syllable rate of speech. Clin. Neurophysiol. 2010, 121, 1343–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Eck, C.F.; Morse, K.R.; Lesniak, B.P.; Kropf, E.J.; Tranovich, M.J.; van Dijk, C.N.; Fu, F.H. Does the lateral intercondylar ridge disappear in ACL deficient patients? Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 1184–1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Eck, C.F.; Schreiber, V.M.; Liu, T.T.; Fu, F.H. The anatomic approach to primary, revision and augmentation anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 1154–1163. [Google Scholar] [CrossRef]
- Van Eck, C.F.; Schreiber, V.M.; Mejia, H.A.; Samuelsson, K.; van Dijk, C.N.; Karlsson, J.; Fu, F.H. “Anatomic” anterior cruciate ligament reconstruction: A systematic review of surgical techniques and reporting of surgical data. Arthroscopy 2010, 26, S2–S12. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, C.G.; Pietrini, S.D.; Westerhaus, B.D.; Anderson, C.J.; Wijdicks, C.A.; Johansen, S.; Engebretsen, L.; LaPrade, R.F. Arthroscopically Pertinent Landmarks for Tunnel Positioning in Single-Bundle and Double-Bundle Anterior Cruciate Ligament Reconstructions. Am. J. Sports Med. 2010, 39, 743–752. [Google Scholar] [CrossRef]
- Farrow, L.D.; Gillespie, R.J.; Victoroff, B.N.; Cooperman, D.R. Radiographic location of the lateral intercondylar ridge: Its relationship to Blumensaat’s line. Am. J. Sports Med. 2008, 36, 2002–2006. [Google Scholar] [CrossRef]
- Zantop, T.; Wellmann, M.; Fu, F.H.; Petersen, W. Tunnel positioning of anteromedial and posterolateral bundles in anatomic anterior cruciate ligament reconstruction: Anatomic and radiographic findings. Am. J. Sports Med. 2008, 36, 65–72. [Google Scholar] [CrossRef]
- Tashman, S.; Kopf, S.; Fu, F.H. The Kinematic Basis of ACL Reconstruction. Oper. Tech. Sports Med. 2008, 16, 116–118. [Google Scholar] [CrossRef] [Green Version]
- Tajima, G.; Iriuchishima, T.; Ingham, S.J.; Shen, W.; van Houten, A.H.; Aerts, M.M.; Shimamura, T.; Smolinski, P.; Fu, F.H. Anatomic Double-Bundle Anterior Cruciate Ligament Reconstruction Restores Patellofemoral Contact Areas and Pressures More Closely Than Nonanatomic Single-Bundle Reconstruction. Arthrosc. J. Arthrosc. Relat. Surg. 2010, 26, 1302–1310. [Google Scholar] [CrossRef]
- Zantop, T.; Peterson, W. Anatomical reconstruction of the anterior cruciate ligament. Arthroskopie 2007, 20, 94–104. [Google Scholar] [CrossRef]
- Hofbauer, M.; Muller, B.; Murawski, C.D.; Baraga, M.; van Eck, C.F.; Fu, F.H. Strategies for revision surgery after primary double-bundle anterior cruciate ligament (ACL) reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2072–2080. [Google Scholar] [CrossRef]
- Hofbauer, M.; Murawski, C.D.; Muller, B.; van Eck, C.F.; Fu, F.H. Revision surgery after primary double-bundle ACL reconstruction: AAOS exhibit selection. J. Bone Jt. Surg. Am. 2014, 96, e30. [Google Scholar] [CrossRef] [PubMed]
- Zauleck, M.K.; Gabriel, S.; Fischmeister, M.F.; Hirtler, L. Origin of the anterior cruciate ligament and the surrounding osseous landmarks of the femur. Clin. Anat. 2014, 27, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhang, W.; Ren, S.; Zhou, R.; Zhang, X.; You, T.; Bai, L. Relationship Between Number of Lateral Intercondylar Ridges and Area of Denser Bone on the Lateral Intercondylar Wall. Orthop. J. Sports Med. 2022, 10, 23259671221091332. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, M.; Levicoff, E.A.; Macpherson, T.A.; Moreland, M.S.; Cohen, M.; Fu, F.H. The Fetal Anterior Cruciate Ligament: An Anatomic and Histologic Study. Arthrosc. J. Arthrosc. Relat. Surg. 2007, 23, 278–283. [Google Scholar] [CrossRef]
- Brantigan, O.C.; Voshell, A.F. The Mechanics of the Ligaments and Menisci of the Knee Joint. J. Bone Jt. Surg. Am. 1941, 23, 44–66. [Google Scholar]
- Girgis, F.G.; Marshall, J.L.; Monajem, A. The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin. Orthop. Relat. Res. 1975, 106, 216–231. [Google Scholar] [CrossRef]
- Aviles, S.A.; Allen, C.R. Knee Arthroscopy: The Basics. In Operative Techniques in Orthopaedic Surgery; Wiesel, S.W., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; pp. 248–256. [Google Scholar]
- Brennan, R.L.; Prediger, D.J. Coefficient Kappa: Some Uses, Misuses, and Alternatives. Educ. Psychol. Meas. 1981, 41, 687–699. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Tsukada, S.; Fujishiro, H.; Watanabe, K.; Nimura, A.; Mochizuki, T.; Mahakkanukrauh, P.; Yasuda, K.; Akita, K. Anatomic variations of the lateral intercondylar ridge: Relationship to the anterior margin of the anterior cruciate ligament. Am. J. Sports Med. 2014, 42, 1110–1117. [Google Scholar] [CrossRef]
- Norman, D.; Metcalfe, A.J.; Barlow, T.; Hutchinson, C.E.; Thompson, P.J.; Spalding, T.J.; Williams, M.A. Cortical Bony Thickening of the Lateral Intercondylar Wall: The Functional Attachment of the Anterior Cruciate Ligament. Am. J. Sports Med. 2017, 45, 394–402. [Google Scholar] [CrossRef] [Green Version]
- Norman, D.G.; Getgood, A.; Thornby, J.; Bird, J.; Turley, G.A.; Spalding, T.; Williams, M.A. Quantitative topographic anatomy of the femoral ACL footprint: A micro-CT analysis. Med. Biol. Eng. Comput. 2014, 52, 985–995. [Google Scholar] [CrossRef] [PubMed]
- Fu, F.H.; Van Eck, C.F.; Tashman, S.; Irrgang, J.J.; Moreland, M.S. Anatomic anterior cruciate ligament reconstruction: A changing paradigm. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 640–648. [Google Scholar] [CrossRef]
- Lim, H.-C.; Yoon, Y.-C.; Wang, J.-H.; Bae, J.-H. Anatomical versus Non-Anatomical Single Bundle Anterior Cruciate Ligament Reconstruction: A Cadaveric Study of Comparison of Knee Stability. Clin. Orthop. Surg. 2012, 4, 249–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amis, A.A.; Dawkins, G.P. Functional anatomy of the anterior cruciate ligament. Fibre bundle actions related to ligament replacements and injuries. J. Bone Jt. Surg. 1991, 73, 260–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loh, J.C.; Fukuda, Y.; Tsuda, E.; Steadman, R.J.; Fu, F.H.; Woo, S.L.-Y. Knee stability and graft function following anterior cruciate ligament reconstruction: Comparison between 11 o’clock and 10 o’clock femoral tunnel placement. Arthrosc. J. Arthrosc. Relat. Surg. 2003, 19, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Zavras, T.D.; Race, A.; Amis, A.A. The effect of femoral attachment location on anterior cruciate ligament reconstruction: Graft tension patterns and restoration of normal anterior-posterior laxity patterns. Knee Surg. Sports Traumatol. Arthrosc. 2005, 13, 92–100. [Google Scholar] [CrossRef]
- Karlsson, J.; Irrgang, J.J.; Van Eck, C.F.; Samuelsson, K.; Mejia, H.A.; Fu, F.H. Anatomic Single- and Double-Bundle Anterior Cruciate Ligament Reconstruction, Part 2. Am. J. Sports Med. 2011, 39, 2016–2026. [Google Scholar] [CrossRef]
- Kondo, E.; Merican, A.M.; Yasuda, K.; Amis, A.A. Biomechanical Comparison of Anatomic Double-Bundle, Anatomic Single-Bundle, and Nonanatomic Single-Bundle Anterior Cruciate Ligament Reconstructions. Am. J. Sports Med. 2011, 39, 279–288. [Google Scholar] [CrossRef]
- Kondo, E.; Yasuda, K.; Azuma, H.; Tanabe, Y.; Yagi, T. Prospective Clinical Comparisons of Anatomic Double-Bundle versus Single-Bundle Anterior Cruciate Ligament Reconstruction Procedures in 328 Consecutive Patients. Am. J. Sports Med. 2008, 36, 1675–1687. [Google Scholar] [CrossRef]
- Yagi, M.; Wong, E.K.; Kanamori, A.; Debski, R.E.; Fu, F.H.; Woo, S.L.-Y. Biomechanical Analysis of an Anatomic Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2002, 30, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, K.; Kondo, E.; Ichiyama, H.; Tanabe, Y.; Tohyama, H. Clinical Evaluation of Anatomic Double-Bundle Anterior Cruciate Ligament Reconstruction Procedure Using Hamstring Tendon Grafts: Comparisons Among 3 Different Procedures. Arthrosc. J. Arthrosc. Relat. Surg. 2006, 22, 240–251. [Google Scholar] [CrossRef] [PubMed]
- Marchant, B.G.; Noyes, F.R.; Barber-Westin, S.D.; Fleckenstein, C. Prevalence of Nonanatomical Graft Placement in a Series of Failed Anterior Cruciate Ligament Reconstructions. Am. J. Sports Med. 2010, 38, 1987–1996. [Google Scholar] [CrossRef]
- Shino, K.; Suzuki, T.; Iwahashi, T.; Mae, T.; Nakamura, N.; Nakata, K.; Nakagawa, S. The resident’s ridge as an arthroscopic landmark for anatomical femoral tunnel drilling in ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 1164–1168. [Google Scholar] [CrossRef]
- Pirri, C.; Stecco, C.; Porzionato, A.; Boscolo-Berto, R.; Fortelny, R.H.; Macchi, V.; Konschake, M.; Merigliano, S.; De Caro, R. Forensic Implications of Anatomical Education and Surgical Training with Cadavers. Front. Surg. 2021, 8, 641581. [Google Scholar] [CrossRef]
- Petersen, W. Tunnel Positioning. In The Anteruir Cruciate Ligament; Petersen, W., Zantop, T., Eds.; Deutscher Ärzte-Verlag: Köln, Germany, 2009. [Google Scholar]
- Giron, F.; Cuomo, P.; Aglietti, P.; Bull, A.M.J.; Amis, A.A. Femoral attachment of the anterior cruciate ligament. Knee Surg. Sports Traumatol. Arthrosc. 2005, 14, 250–256. [Google Scholar] [CrossRef]
- Arnoczky, S.P. Anatomy of the anterior cruciate ligament. Clin. Orthop. Relat. Res. 1983, 172, 19–25. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LIR (%) | LBR (%) | |||||
|---|---|---|---|---|---|---|
| Correct | Unmarked | Incorrect | Correct | Unmarked | Incorrect | |
| Medical student | 19.4 * | 47.2 * | 33.4 | 0 | 83.3 | 16.7 |
| Anatomist | 72.2 | 13.9 | 13.9 | 5.6 | 75 | 19.4 |
| Orthopedic surgeon | 77.8 | 2.8 | 19.4 | 8.4 | 33.3 | 58.3 * |
| n | LIR (%) | LBR (%) | Material | |
|---|---|---|---|---|
| Ferretti et al. [5] | 7 | - | 85.7 | Fetus |
| 60 | 100.0 | 81.7 | Arthroscopic | |
| 16 | 100.0 | 81.6 | Anatomical specimens | |
| Van Eck et al. [13] | 50 | 88.0 | 48.0 | Arthroscopic |
| Ziegler et al. [16] | 26 | 100.0 | 92.3 | Anatomical specimens |
| Zauleck et al. [24] | 166 | 97.6 | 24.7 | Bones |
| 69 | 85.3 | 13.2 | Anatomical specimens | |
| Tsukada et al. [32] | 318 | 94.0 | - | Bones |
| Norman et al. [33] | 7 | 57.0 | 29.0 | Anatomical specimens |
| Li et al. [25] | 89 | 87.5% | - | Patients |
| This study | 36 | 80.6 | 13.8 | Anatomical specimens |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirtler, L.; Rieschl, D.; Kandathil, S.A.; Weninger, P. Feasibility of Osseous Landmarks for ACL Reconstruction—A Macroscopic Anatomical Study. Appl. Sci. 2023, 13, 7345. https://doi.org/10.3390/app13127345
Hirtler L, Rieschl D, Kandathil SA, Weninger P. Feasibility of Osseous Landmarks for ACL Reconstruction—A Macroscopic Anatomical Study. Applied Sciences. 2023; 13(12):7345. https://doi.org/10.3390/app13127345
Chicago/Turabian StyleHirtler, Lena, Dominik Rieschl, Sam A. Kandathil, and Patrick Weninger. 2023. "Feasibility of Osseous Landmarks for ACL Reconstruction—A Macroscopic Anatomical Study" Applied Sciences 13, no. 12: 7345. https://doi.org/10.3390/app13127345