
Kinetic and Kinematic Analysis of Gait Termination: A Comparison between Planned and Unplanned Conditions

Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Measurements
2.2.1. Motion Analysis System
2.2.2. Force Plates
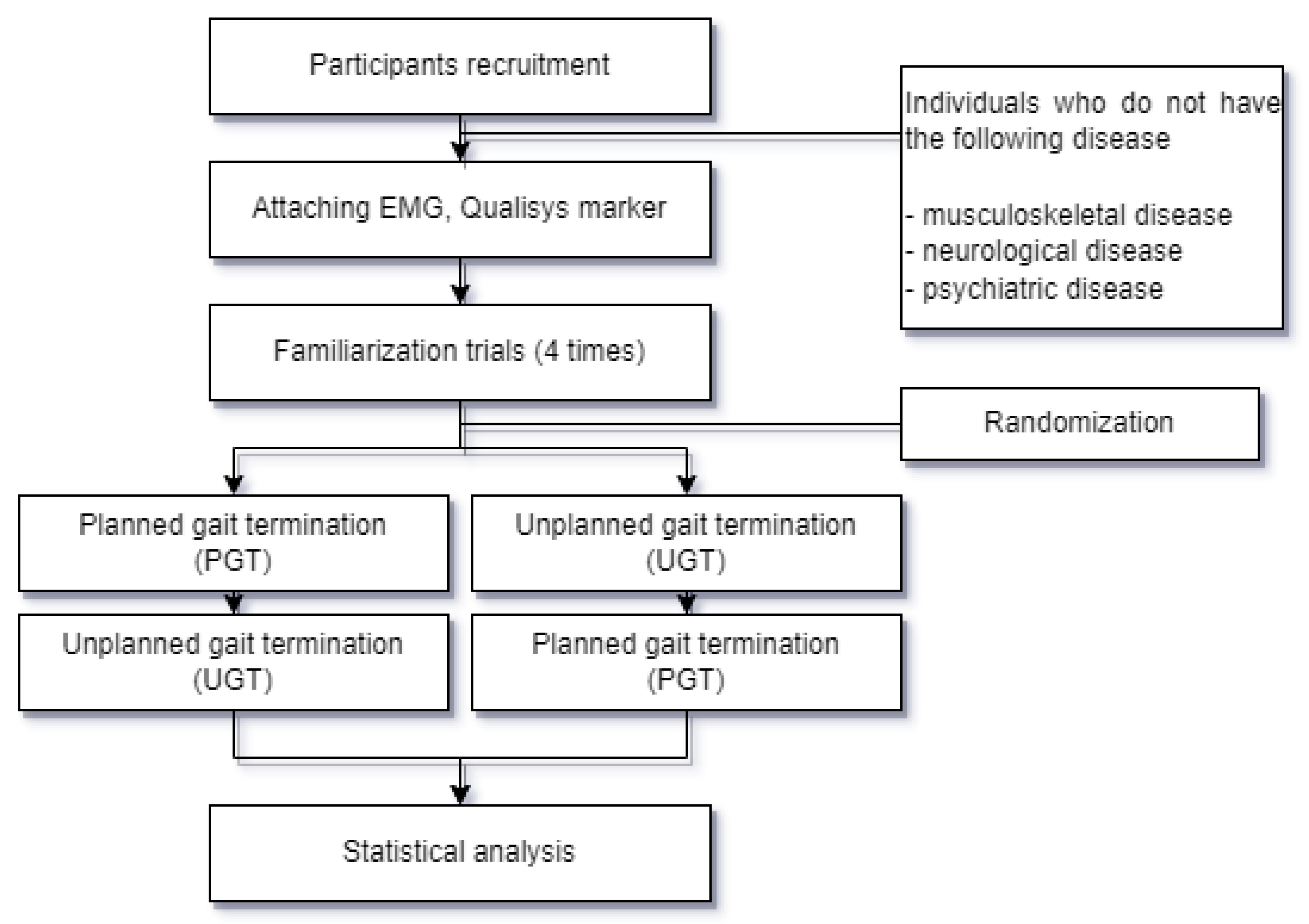
2.2.3. Experimental Procedure
2.2.4. Data Analysis
2.2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cimolin, V.; Cau, N.; Galli, M.; Santovito, C.; Grugni, G.; Capodaglio, P. Gait initiation and termination strategies in patients with Prader-Willi syndrome. J. Neuroeng. Rehabil. 2017, 14, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryckewaert, G.; Delval, A.; Bleuse, S.; Blatt, J.-L.; Defebvre, L. Biomechanical mechanisms and centre of pressure trajectory during planned gait termination. Neurophysiol. Clin./Clin. Neurophysiol. 2014, 44, 227–233. [Google Scholar] [CrossRef]
- Lynch, J.; Robertson, D. Biomechanics of planned gait termination. J. Biomech. 2007, 40, S500. [Google Scholar] [CrossRef]
- Cen, X.; Lu, Z.; Baker, J.S.; István, B.; Gu, Y. A comparative biomechanical analysis during planned and unplanned gait termination in individuals with different arch Stiffnesses. Appl. Sci. 2021, 11, 1871. [Google Scholar] [CrossRef]
- Jung, S.; Yi, J.; Song, C. Biomechanical alterations of gait termination in middle-aged and elderly women. J. Phys. Ther. Sci. 2016, 28, 861–867. [Google Scholar] [CrossRef] [Green Version]
- Cen, X.; Yu, P.; Song, Y.; Sárosi, J.; Mao, Z.; Bíró, I.; Gu, Y. The Effect of Arch Stiffness on the Foot–Ankle Temporal Kinematics during Gait Termination: A Statistical Nonparametric Mapping Study. Bioengineering 2022, 9, 703. [Google Scholar] [CrossRef]
- Zhang, S.; Li, L. Feedforward and feedback control for gait and balance. Gait Biom. 2014, 191–205. [Google Scholar]
- Ridge, S.T.; Henley, J.; Manal, K.; Miller, F.; Richards, J.G. Kinematic and kinetic analysis of planned and unplanned gait termination in children. Gait Posture 2013, 37, 178–182. [Google Scholar] [CrossRef] [Green Version]
- Roeing, K.L.; Moon, Y.; Sosnoff, J.J. Unplanned gait termination in individuals with multiple sclerosis. Gait Posture 2017, 53, 168–172. [Google Scholar] [CrossRef]
- Sparrow, W.; Tirosh, O. Gait termination: A review of experimental methods and the effects of ageing and gait pathologies. Gait Posture 2005, 22, 362–371. [Google Scholar] [CrossRef]
- Koo, D.-K.; Kwon, J.-W. Biomechanical Analysis of Unplanned Gait Termination According to a Stop-Signal Task Performance: A Preliminary Study. Brain Sci. 2023, 13, 304. [Google Scholar] [CrossRef]
- Zhou, H.; Cen, X.; Song, Y.; Ugbolue, U.C.; Gu, Y. Lower-limb biomechanical characteristics associated with unplanned gait termination under different walking speeds. JoVE (J. Vis. Exp.) 2020, 162, e61558. [Google Scholar]
- Cen, X.; Xu, D.; Baker, J.S.; Gu, Y. Association of arch stiffness with plantar impulse distribution during walking, running, and gait termination. Int. J. Environ. Res. Public Health 2020, 17, 2090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bautmans, I.; Jansen, B.; Van Keymolen, B.; Mets, T. Reliability and clinical correlates of 3D-accelerometry based gait analysis outcomes according to age and fall-risk. Gait Posture 2011, 33, 366–372. [Google Scholar] [CrossRef]
- Cappozzo, A.; Catani, F.; Della Croce, U.; Leardini, A. Position and orientation in space of bones during movement: Anatomical frame definition and determination. Clin. Biomech. 1995, 10, 171–178. [Google Scholar] [CrossRef]
- Buczek, F.L.; Rainbow, M.J.; Cooney, K.M.; Walker, M.R.; Sanders, J.O. Implications of using hierarchical and six degree-of-freedom models for normal gait analyses. Gait Posture 2010, 31, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Fournier, B. Model and Characterization of a Passive Biomimetic Ankle for Lower Extremity Powered Exoskeleton. Ph.D. Thesis, Université d’Ottawa/University of Ottawa, Ottawa, ON, Canada, 2018. [Google Scholar]
- Rum, L.; Brasiliano, P.; Vannozzi, G.; Laudani, L.; Macaluso, A. Non-specific chronic low back pain elicits kinematic and neuromuscular changes in walking and gait termination. Gait Posture 2021, 84, 238–244. [Google Scholar] [CrossRef]
- Wikstrom, E.A.; Bishop, M.D.; Inamdar, A.D.; Hass, C.J. Gait termination control strategies are altered in chronic ankle instability subjects. Med. Sci. Sport. Exerc. 2010, 42, 197–205. [Google Scholar] [CrossRef] [Green Version]
- Wikstrom, E.A.; Hass, C.J. Gait termination strategies differ between those with and without ankle instability. Clin. Biomech. 2012, 27, 619–624. [Google Scholar] [CrossRef]
- Svoboda, Z.; Bizovska, L.; Janura, M.; Kubonova, E.; Janurova, K.; Vuillerme, N. Variability of spatial temporal gait parameters and center of pressure displacements during gait in elderly fallers and nonfallers: A 6-month prospective study. PLoS ONE 2017, 12, e0171997. [Google Scholar] [CrossRef] [Green Version]
- Pirker, W.; Katzenschlager, R. Gait disorders in adults and the elderly: A clinical guide. Wien. Klin. Wochenschr. 2017, 129, 81–95. [Google Scholar] [CrossRef] [Green Version]
- Wong, D.W.-C.; Lam, W.-K.; Lee, W.C.-C. Gait asymmetry and variability in older adults during long-distance walking: Implications for gait instability. Clin. Biomech. 2020, 72, 37–43. [Google Scholar] [CrossRef]
- Jaeger, R.; Vanitchatchavan, P. Ground reaction forces during termination of human gait. J. Biomech. 1992, 25, 1233–1236. [Google Scholar] [CrossRef]
- Ridge, S.T.; Henley, J.; Manal, K.; Miller, F.; Richards, J.G. Biomechanical analysis of gait termination in 11–17 year old youth at preferred and fast walking speeds. Hum. Mov. Sci. 2016, 49, 178–185. [Google Scholar] [CrossRef]
- Conte, C.; Serrao, M.; Casali, C.; Ranavolo, A.; Silvia, M.; Draicchio, F.; Di Fabio, R.; Monami, S.; Padua, L.; Iavicoli, S. Planned gait termination in cerebellar ataxias. Cerebellum 2012, 11, 896–904. [Google Scholar] [CrossRef]
- Vaverka, F.; Elfmark, M.; Svoboda, Z.; Janura, M. System of gait analysis based on ground reaction force assessment. Acta Gymnica 2015, 45, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Whittle, M.W. Gait Analysis: An Introduction; Butterworth-Heinemann: Oxford, UK, 2014. [Google Scholar]
- Kharb, A.; Saini, V.; Jain, Y.; Dhiman, S. A review of gait cycle and its parameters. Int. J. Comput. Eng. Manag. 2011, 13, 78–83. [Google Scholar]
- Tirosh, O.; Sparrow, W. Gait termination in young and older adults: Effects of stopping stimulus probability and stimulus delay. Int. J. Comput. Eng. Manag. 2004, 19, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.; Darter, B. Principles of Normal and Pathologic Gait; Atlas of orthoses and Assistive Devices; Elsevier: Amsterdam, The Netherlands, 2019; pp. 46–62. [Google Scholar]
- Shen, X.-A.; Cen, X.; Song, Y. Investigating Temporal Kinematic Differences Caused by Unexpected Stimulation during Gait Termination through the Waveform-Level Variance Equality Test. BioMed Res. Int. 2022, 2022, 4043426. [Google Scholar] [CrossRef]
- Cen, X.; Gao, L.; Yang, M.; Liang, M.; Bíró, I.; Gu, Y. Arch-support induced changes in foot-ankle coordination in young males with flatfoot during unplanned gait termination. J. Clin. Med. 2021, 10, 5539. [Google Scholar] [CrossRef]
- Oates, A.R.; Patla, A.E.; Frank, J.S.; Greig, M.A. Control of dynamic stability during gait termination on a slippery surface. J. Neurophysiol. 2005, 93, 64–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oates, A.R.; Frank, J.S.; Patla, A.E. Control of dynamic stability during adaptation to gait termination on a slippery surface. Exp. Brain Res. 2010, 201, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Arnold, A.S.; Thelen, D.G.; Schwartz, M.H.; Anderson, F.C.; Delp, S.L. Muscular coordination of knee motion during the terminal-swing phase of normal gait. J. Biomech. 2007, 40, 3314–3324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, T.; Singer, M.L.; Orendurff, M.S.; Gao, F.; Daly, W.K.; Foreman, K.B. The effect of changing plantarflexion resistive moment of an articulated ankle–foot orthosis on ankle and knee joint angles and moments while walking in patients post stroke. Clin. Biomech. 2015, 30, 775–780. [Google Scholar] [CrossRef] [Green Version]
- Ugbolue, U.C.; Robson, C.; Donald, E.; Speirs, K.L.; Dutheil, F.; Baker, J.S.; Dias, T.; Gu, Y. Joint angle, range of motion, force, and moment assessment: Responses of the lower limb to ankle plantarflexion and dorsiflexion. Appl. Bionics Biomech. 2021, 2021, 1–13. [Google Scholar] [CrossRef]
- Brockett, C.L.; Chapman, G.J. Biomechanics of the ankle. Orthop. Trauma 2016, 30, 232–238. [Google Scholar] [CrossRef] [Green Version]
- Bishop, M.; Brunt, D.; Pathare, N.; Patel, B. The effect of velocity on the strategies used during gait termination. Gait Posture 2004, 20, 134–139. [Google Scholar] [CrossRef]
- JudgeRoy, J.O.; Davis, B., III; Õunpuu, S.J. Step length reductions in advanced age: The role of ankle and hip kinetics. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1996, 51, M303–M312. [Google Scholar] [CrossRef]
- Cen, X.; Biro, I.; Gu, Y. Impacts of Different Arch Stiffness on Lower Extremity Joint Kinematics during Unexpected Gait Termination. In Proceedings of the 2022 International Conference on Intelligent Medicine and Health, Xiamen, China, 19–21 August 2022; pp. 14–18. [Google Scholar]
- Dugan, S.A.; Bhat, K.P. Biomechanics and analysis of running gait. Phys. Med. Rehabil. Clin. 2005, 16, 603–621. [Google Scholar] [CrossRef]
- Jian, Y.; Winter, D.A.; Ishac, M.G.; Gilchrist, L. Trajectory of the body COG and COP during initiation and termination of gait. Gait Posture 1993, 1, 9–22. [Google Scholar] [CrossRef]
- Peterson, C.L.; Kautz, S.A.; Neptune, R.R. Braking and propulsive impulses increase with speed during accelerated and decelerated walking. Gait Posture 2011, 33, 562–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Walking | PGT | UGT | p-Value | |
|---|---|---|---|---|
| Stride length (m) | 1.27 ± 0.12 | 1.25 ± 0.09 | 1.28 ± 0.12 | 0.350 |
| Normalized stride length (ratio) | 1.47 ± 0.10 | 1.45 ± 0.11 | 1.48 ± 0.10 | 0.350 |
| Gait velocity (m/s) | 1.16 ± 0.12 | 1.11 ± 0.10 | 1.14 ± 0.12 | 0.076 |
| GT time (s) | - | 0.86 ± 0.10 | 0.58 ± 0.14 | <0.001 * |
| GT step length (m) | - | 0.59 ± 0.05 | 0.66 ± 0.07 | 0.002 * |
| Walking | PGT | UGT | p-Value | Post Hoc | |||
|---|---|---|---|---|---|---|---|
| ROM (°) | Phase 1 | Hip joint | 36.23 ± 4.22 | 36.64 ± 2.57 | 36.21 ± 4.01 | 0.638 | |
| Knee joint | 48.86 ± 4.99 | 48.62 ± 5.61 | 49.90 ± 4.59 | 0.387 | |||
| Ankle joint | 29.41 ± 5.41 | 27.35 ± 4.96 | 29.71 ± 4.12 | 0.032 * | b < c | ||
| Phase 2 | Hip joint | 5.48 ± 0.91 | 4.15 ± 1.36 | 4.73 ± 1.37 | 0.006 * | a > b | |
| Knee joint | 52.77 ± 5.51 | 48.57 ± 7.62 | 54.50 ± 4.63 | 0.004 * | b < c | ||
| Ankle joint | 7.05 ± 4.82 | 8.44 ± 5.40 | 8.80 ± 4.38 | 0.001 * | a < b, c | ||
| Phase 3 | Hip joint | - | 23.30 ± 3.33 | 10.07 ± 3.97 | <0.001 * | ||
| Knee joint | - | 10.66 ± 6.55 | 14.28 ± 6.78 | 0.010 * | |||
| Ankle joint | - | 14.09 ± 4.62 | 14.38 ± 2.80 | 0.217 | |||
| GRF (N/kg) | Peak GRF | - | 0.21 ± 0.05 | 0.34 ± 0.08 | <0.001 * | ||
| GRF impulse | - | 0.08 ± 0.02 | 0.09 ± 0.02 | <0.001 * | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, C.-W.; Yun, S.-H.; Koo, D.-K.; Kwon, J.-W. Kinetic and Kinematic Analysis of Gait Termination: A Comparison between Planned and Unplanned Conditions. Appl. Sci. 2023, 13, 7323. https://doi.org/10.3390/app13127323
Kwon C-W, Yun S-H, Koo D-K, Kwon J-W. Kinetic and Kinematic Analysis of Gait Termination: A Comparison between Planned and Unplanned Conditions. Applied Sciences. 2023; 13(12):7323. https://doi.org/10.3390/app13127323
Chicago/Turabian StyleKwon, Chae-Won, Seong-Ho Yun, Dong-Kyun Koo, and Jung-Won Kwon. 2023. "Kinetic and Kinematic Analysis of Gait Termination: A Comparison between Planned and Unplanned Conditions" Applied Sciences 13, no. 12: 7323. https://doi.org/10.3390/app13127323