
The Power Setting of Focused Ultrasound for the Palliative Treatment of Advanced Pancreatic Cancer: A Study in an Ex Vivo Bovine Liver
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ultrasound Field Calculations
2.2. Temperature Profile Calculations
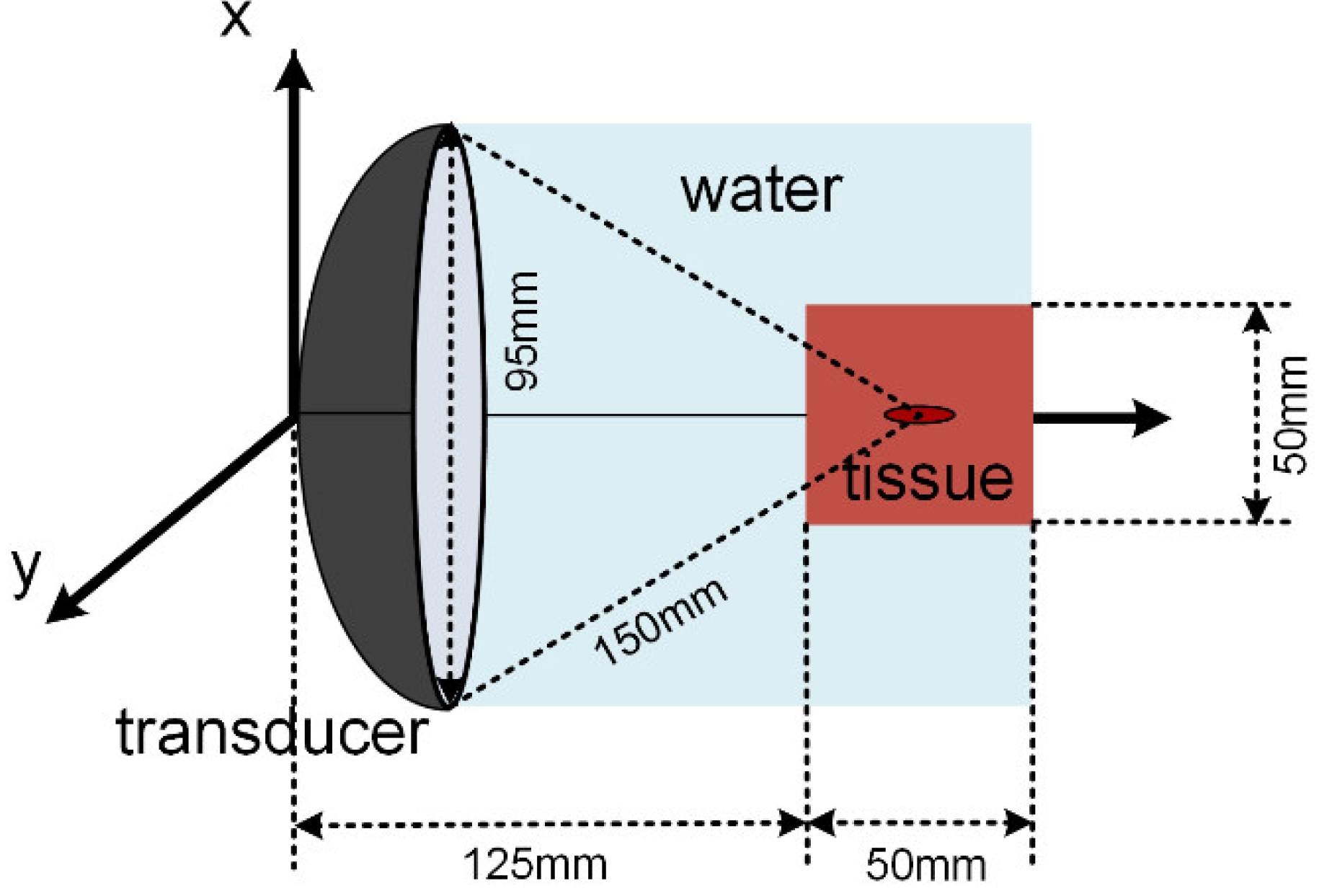
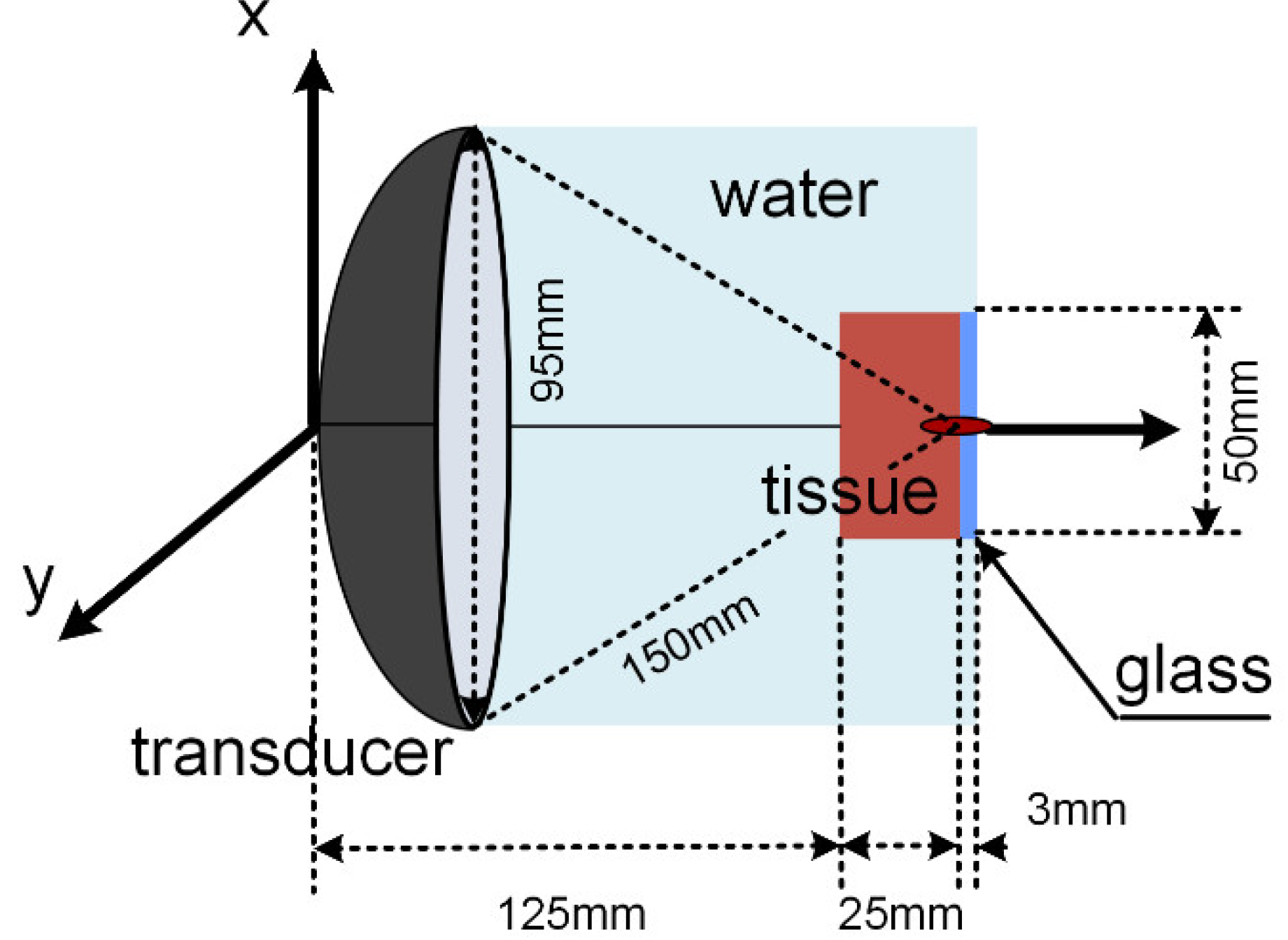
2.3. Simulation Model
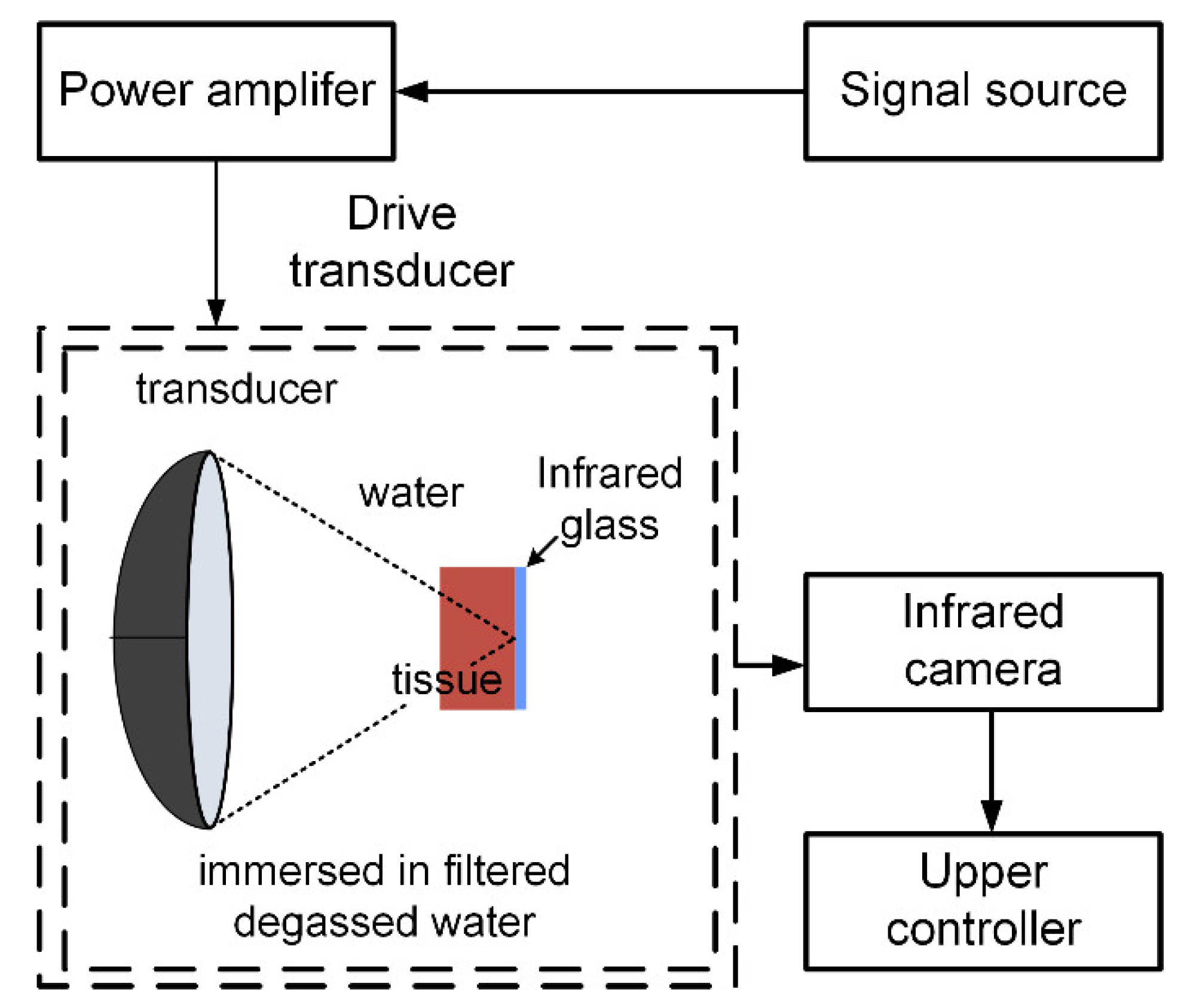
2.4. Experimental Setup
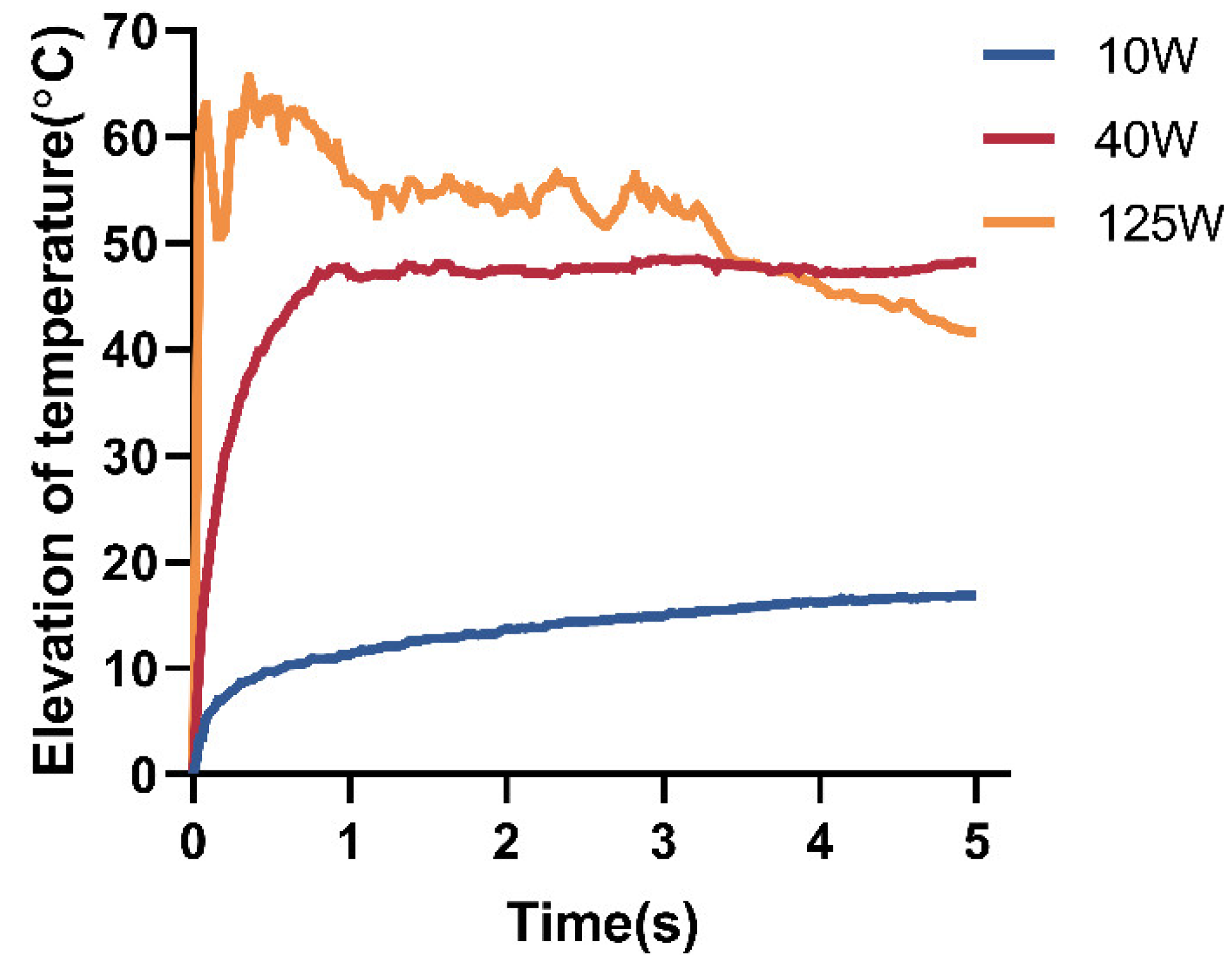
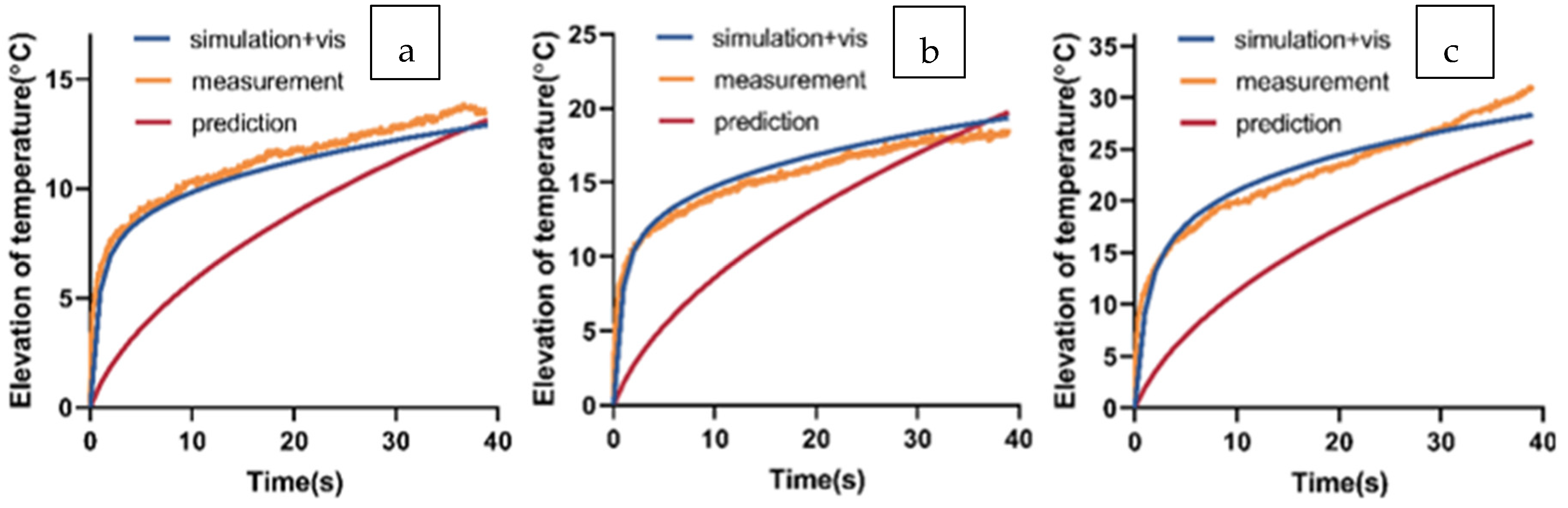
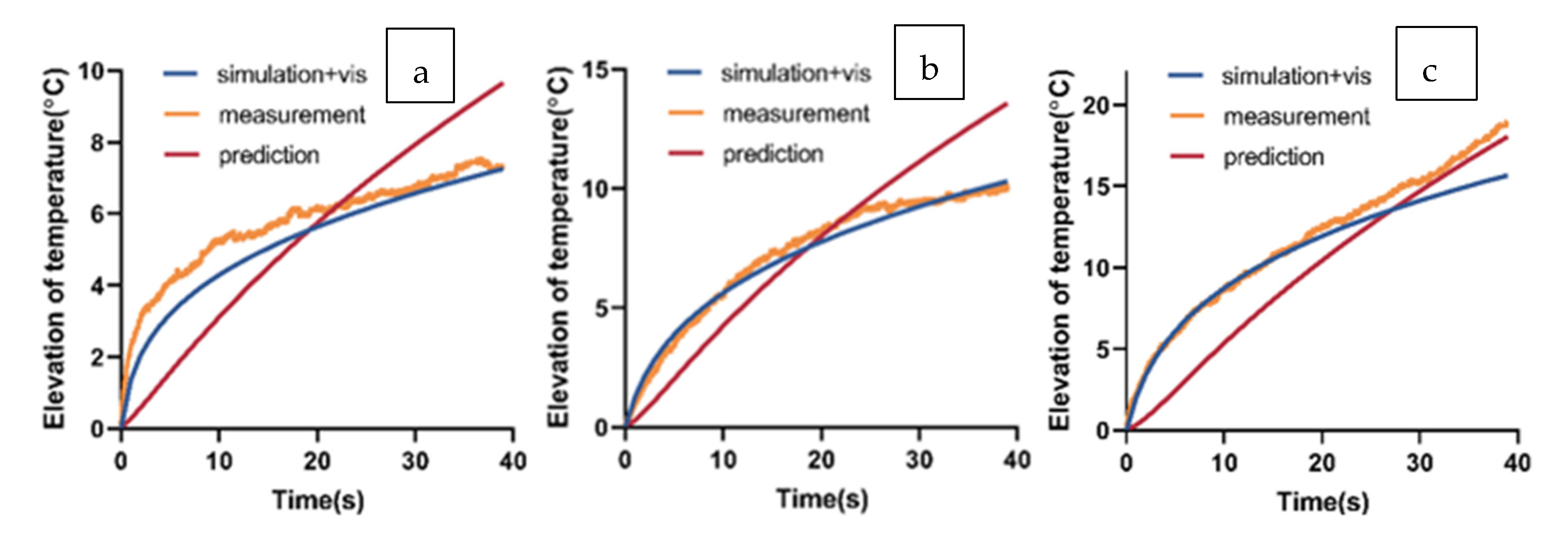
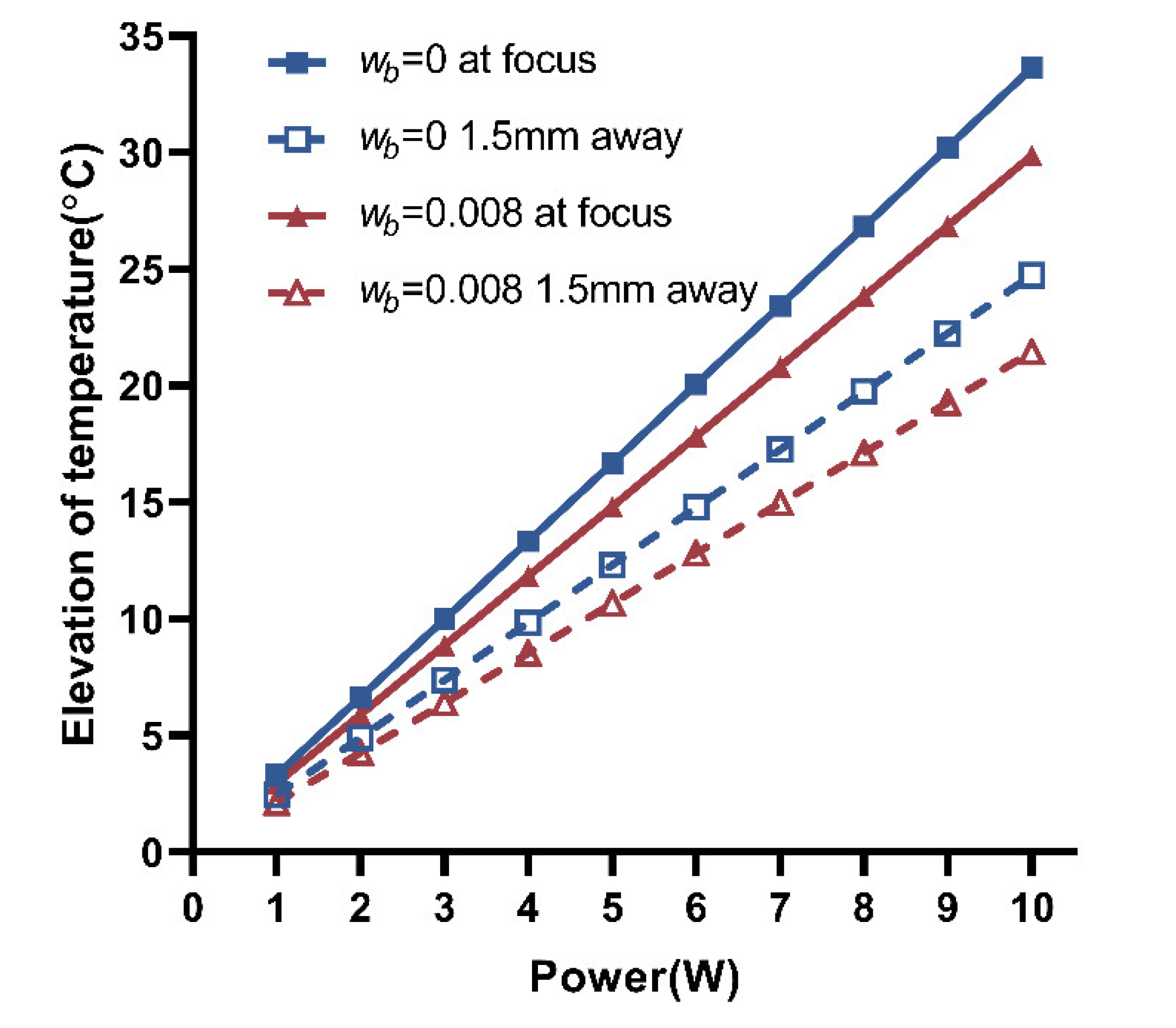
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Ullman, N.A.; Burchard, P.R.; Dunne, R.F.; Linehan, D.C. Immunologic strategies in pancreatic cancer: Making cold tumors hot. J. Clin. Oncol. 2022, 40, 2789. [Google Scholar] [CrossRef] [PubMed]
- Khokhlova, T.D.; Hwang, J.H. HIFU for palliative treatment of pancreatic cancer. In Therapeutic Ultrasound; Springer: Cham, Switzerland, 2016; pp. 83–95. [Google Scholar]
- Ter Haar, G.; Coussios, C. High intensity focused ultrasound: Physical principles and devices. Int. J. Hyperther. 2007, 23, 89–104. [Google Scholar] [CrossRef] [PubMed]
- Pacella, C.M.; Bizzarri, G.; Guglielmi, R.; Anelli, V.; Bianchini, A.; Crescenzi, A.; Pacella, S.; Papini, E. Thyroid tissue: US-guided percutaneous interstitial laser ablation—A feasibility study. Radiology 2000, 217, 673–677. [Google Scholar] [CrossRef]
- Khokhlova, V.A.; Bailey, M.R.; Reed, J.A.; Cunitz, B.W.; Kaczkowski, P.J.; Crum, L.A. Effects of nonlinear propagation, cavitation, and boiling in lesion formation by high intensity focused ultrasound in a gel phantom. J. Acoust. Soc. Am. 2006, 19, 1834–1848. [Google Scholar] [CrossRef] [Green Version]
- Lv, W.; Yan, T.; Wang, G.; Zhao, W.; Zhang, T.; Zhou, D. High-intensity focused ultrasound therapy in combination with gemcitabine for unresectable pancreatic carcinoma. Ther. Clin. Risk Manag. 2016, 12, 687. [Google Scholar]
- Dababou, S.; Marrocchio, C.; Rosenberg, J.; Bitton, R.; Pauly, K.B.; Napoli, A.; Hwang, J.H.; Ghanouni, P. A meta-analysis of palliative treatment of pancreatic cancer with high intensity focused ultrasound. J. Ther. Ultras. 2017, 5, 9. [Google Scholar] [CrossRef] [Green Version]
- Strunk, H.M.; Henseler, J.; Rauch, M.; Mucke, M.; Kukuk, G.; Cuhls, H.; Radbruch, L.; Zhang, L.; Schild, H.H.; Marinova, M. Clinical use of high-intensity focused ultrasound (HIFU) for tumor and pain reduction in advanced pancreatic cancer. In RöFo-Fortschritte auf dem Gebiet der Röntgenstrahlen und der bildgebenden Verfahren; Georg Thieme Verlag KG: Stuttgart, Germany, 2016; Volume 188, pp. 662–670. [Google Scholar]
- Sung, H.Y.; Jung, S.E.; Cho, S.H.; Zhou, K.; Han, J.Y.; Han, S.T.; Kim, J.I.; Kim, J.K.; Choi, J.Y.; Yoon, S.K.; et al. Long-term outcome of high-intensity focused ultrasound in advanced pancreatic cancer. Pancreas 2011, 40, 1080–1086. [Google Scholar] [CrossRef]
- Esnault, O.; Franc, B.; Ménégaux, F.; Rouxel, A.; Kerviler, E.D.; Bourrier, P.; Lacoste, F.; Chapelon, J.Y.; Leenhardt, L. High-intensity focused ultrasound ablation of thyroid nodules: First human feasibility study. Thyroid 2011, 21, 965–973. [Google Scholar] [CrossRef] [PubMed]
- Korkusuz, H.; Fehre, N.; Sennert, M.; Happel, C.; Grunwald, F. Early assessment of high-intensity focused ultrasound treatment of benign thyroid nodules by scintigraphic means. J. Ther. Ultras. 2014, 2, 18. [Google Scholar] [CrossRef] [PubMed]
- Lang, B.H.H.; Woo, Y.C.; Chiu, K.W.H. Single-session high-intensity focused ultrasound treatment in large-sized benign thyroid nodules. Thyroid 2017, 27, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Paiella, S.; De Pastena, M.; D’Onofrio, M.; Crinò, S.F.; Pan, T.L.; De Robertis, R.; Elio, G.; Martone, E.; Salvia, R. Palliative therapy in pancreatic cancer—Interventional treatment with radiofrequency ablation/irreversible electroporation. Transl. Gastroenterol. Hepatol. 2018, 3, 80. [Google Scholar] [CrossRef]
- Hariharan, P.; Myers, M.R.; Banerjee, R.K. HIFU procedures at moderate intensities—Effect of large blood vessels. Phys. Med. Biol. 2007, 52, 3493. [Google Scholar] [CrossRef]
- Xu, Z.; Fowlkes, J.B.; Ludomirsky, A.; Cain, C.A. Investigation of intensity thresholds for ultrasound tissue erosion. Ultrasound Med. Biol. 2005, 31, 1673–1682. [Google Scholar] [CrossRef] [Green Version]
- Mahoney, K.; Fjield, T.; McDannold, N.; Clement, G.; Hynynen, K. Comparison of modelled and observed in vivo temperature elevations induced by focused ultrasound: Implications for treatment planning. Phys. Med. Biol. 2001, 46, 1785. [Google Scholar] [CrossRef]
- Damianou, C.; Hynynen, K. The effect of various physical parameters on the size and shape of necrosed tissue volume during ultrasound surgery. J. Acoust. Soc. Am. 1994, 95, 1641–1649. [Google Scholar] [CrossRef]
- Karaböce, B.; Çetin, E.; Durmuş, H.O.; Özdingiş, M.; Korkmaz, H.; Altun, J.; Argun, S. Experimental investigations of viscous heating effect of thermocouples under focused ultrasound applications. In Proceedings of the 2017 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Rochester, MN, USA, 7–10 May 2017; pp. 88–93. [Google Scholar]
- Norton, G.V.; Purrington, R.D. The Westervelt equation with viscous attenuation versus a causal propagation operator: A numerical comparison. J. Sound. Vib. 2009, 327, 163–172. [Google Scholar] [CrossRef]
- Yee, K. Numerical solution of initial boundary value problems involving Maxwell’s equations in isotropic media. IEEE Trans. Antennas Propag. 1966, 14, 302–307. [Google Scholar]
- Pennes, H.H. Analysis of tissue and arterial blood temperatures in the resting human forearm. J. Appl. Physiol. 1948, 1, 93–122. [Google Scholar] [CrossRef] [PubMed]
- Tiennot, T.; Kamimura, H.A.S.; Lee, S.A.; Aurup, C.; Konofagou, E.E. Numerical modeling of ultrasound heating for the correction of viscous heating artifacts in soft tissue temperature measurements. Appl. Phys. Lett. 2019, 114, 203702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, C.R.; Cleveland, R.O.; Coussios, C.C. Real-time temperature estimation and monitoring of HIFU ablation through a combined modeling and passive acoustic mapping approach. Phys. Med. Biol. 2013, 58, 5833. [Google Scholar] [CrossRef] [PubMed]
- Chang, N.; Lu, S.; Qin, D.; Xu, T.; Han, M.; Wang, S.; Wan, M. Efficient and controllable thermal ablation induced by short-pulsed HIFU sequence assisted with perfluorohexane nanodroplets. Ultrason Sonochem. 2018, 45, 57–64. [Google Scholar] [CrossRef]
- Chen, L.; ter Haar, G.; Hill, C.R. Influence of ablated tissue on the formation of high-intensity focused ultrasound lesions. Ultrasound Med. Biol. 1997, 23, 921–931. [Google Scholar] [CrossRef]
- Bini, F.; Trimboli, P.; Marinozzi, F.; Giovanella, L. Treatment of benign thyroid nodules by high intensity focused ultrasound (HIFU) at different acoustic powers: A study on in-silico phantom. Endocrine 2018, 59, 506–509. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | ||
|---|---|---|
| Acoustic parameters | Frequency (MHz) | 1.12 |
| Aperture diameter (mm) | 95 | |
| Focal length (mm) | 150 | |
| Water | Sound speed (m/s) | 1500 |
| Density (kg/m3) | 1000 | |
| Thermal capacity (J/kg K) | 4180 | |
| Thermal conductivity (W/m K) | 0.6 | |
| Absorption coefficient (Np/m/MHz) | 0.025 | |
| Nonlinear coefficient | 5 | |
| Liver properties | Sound speed (m/s) | 1595 |
| Density (kg/m3) | 1060 | |
| Thermal capacity (J/kg K) | 3400 | |
| Thermal conductivity (W/m K) | 0.45 | |
| Absorption coefficient (Np/m/MHz) | 5.8 | |
| Nonlinear coefficient | 6.6 | |
| Dynamic viscosity (Pa s) | 1.59 | |
| Infrared glass properties | Sound speed (m/s) | 2692 |
| Density (kg/m3) | 1450 | |
| Thermal capacity (J/kg K) | 410 | |
| Thermal conductivity (W/m K) | 11.72 | |
| Absorption coefficient (Np/m/MHz) | 0 | |
| Geometrical specifications | Liver diameter (mm) | 50 |
| Liver length (mm) | 25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tong, S.; Wang, Y.; Zhao, P.; Tao, J.; Guo, X.; Yu, Y. The Power Setting of Focused Ultrasound for the Palliative Treatment of Advanced Pancreatic Cancer: A Study in an Ex Vivo Bovine Liver. Appl. Sci. 2023, 13, 474. https://doi.org/10.3390/app13010474
Tong S, Wang Y, Zhao P, Tao J, Guo X, Yu Y. The Power Setting of Focused Ultrasound for the Palliative Treatment of Advanced Pancreatic Cancer: A Study in an Ex Vivo Bovine Liver. Applied Sciences. 2023; 13(1):474. https://doi.org/10.3390/app13010474
Chicago/Turabian StyleTong, Shiqi, Yuebing Wang, Peng Zhao, Jie Tao, Xiaoan Guo, and Yaping Yu. 2023. "The Power Setting of Focused Ultrasound for the Palliative Treatment of Advanced Pancreatic Cancer: A Study in an Ex Vivo Bovine Liver" Applied Sciences 13, no. 1: 474. https://doi.org/10.3390/app13010474