
A 3D CBCT Analysis of Airway and Cephalometric Values in Patients Diagnosed with Juvenile Idiopathic Arthritis Compared to a Control Group

 , ,
, , 
Abstract
:1. Introduction
2. Subject and Methods
2.1. CBCT Acquisition
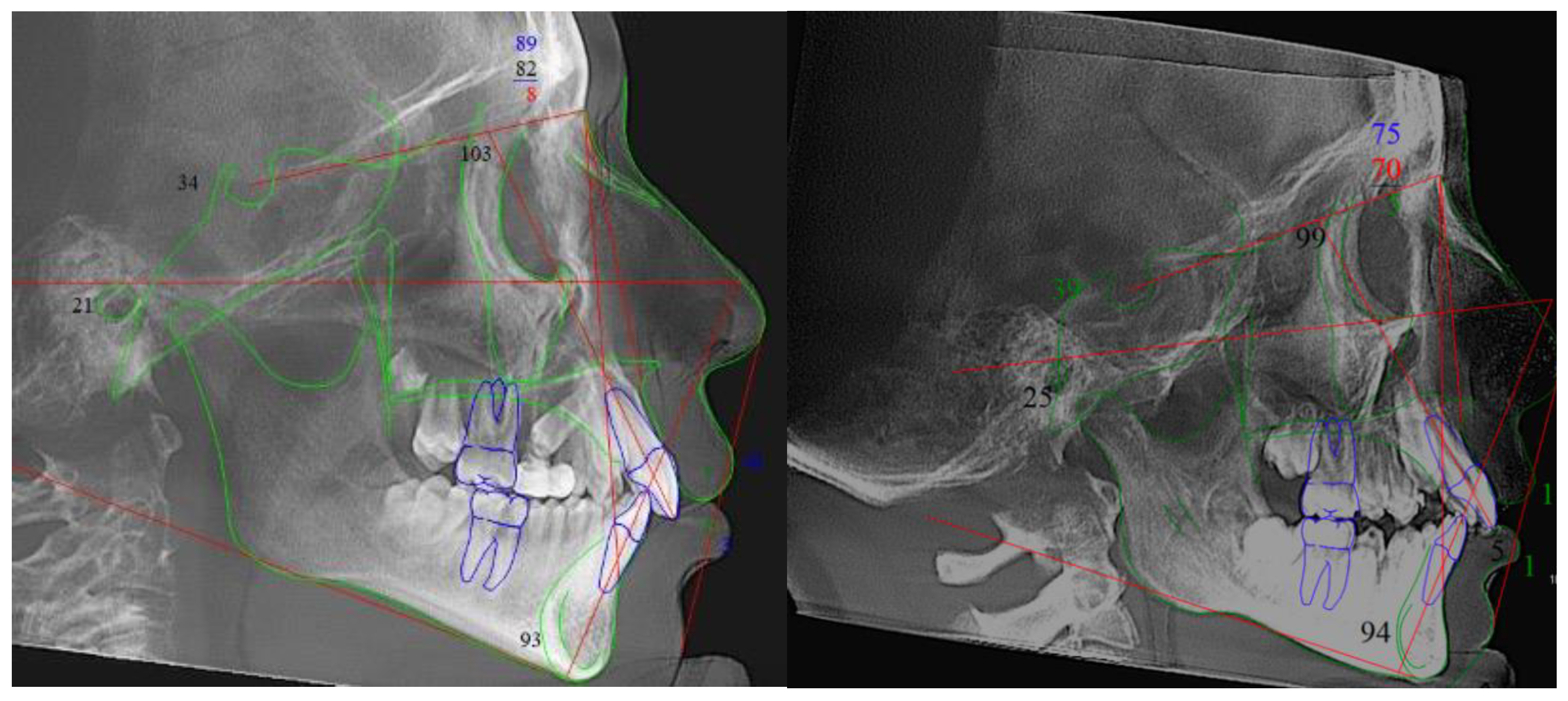
2.2. Cephalometric Rendering and Analysis
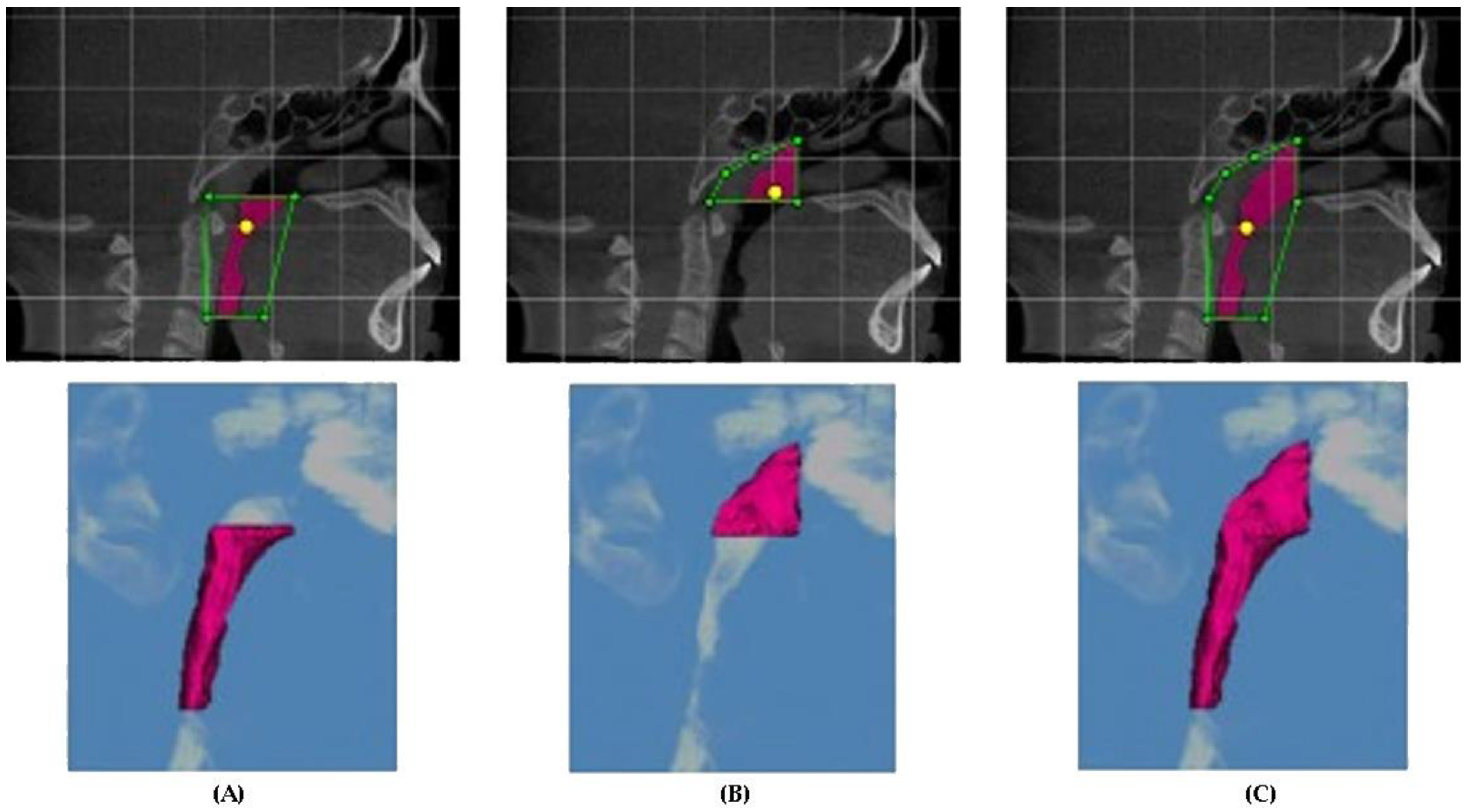
2.3. Airway Measurements
2.4. Statistical Analysis
3. Results
3.1. Cephalometric Analysis
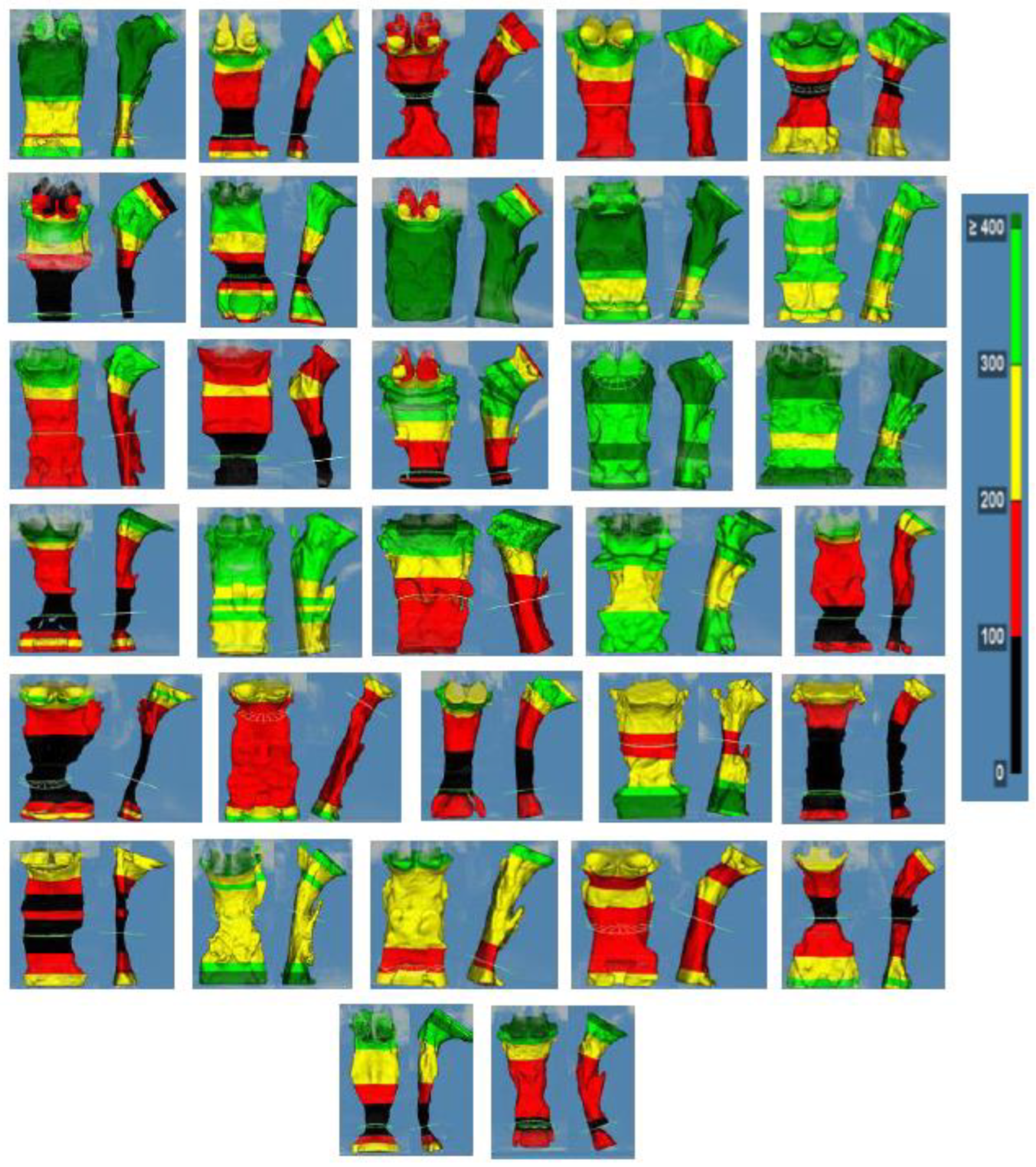
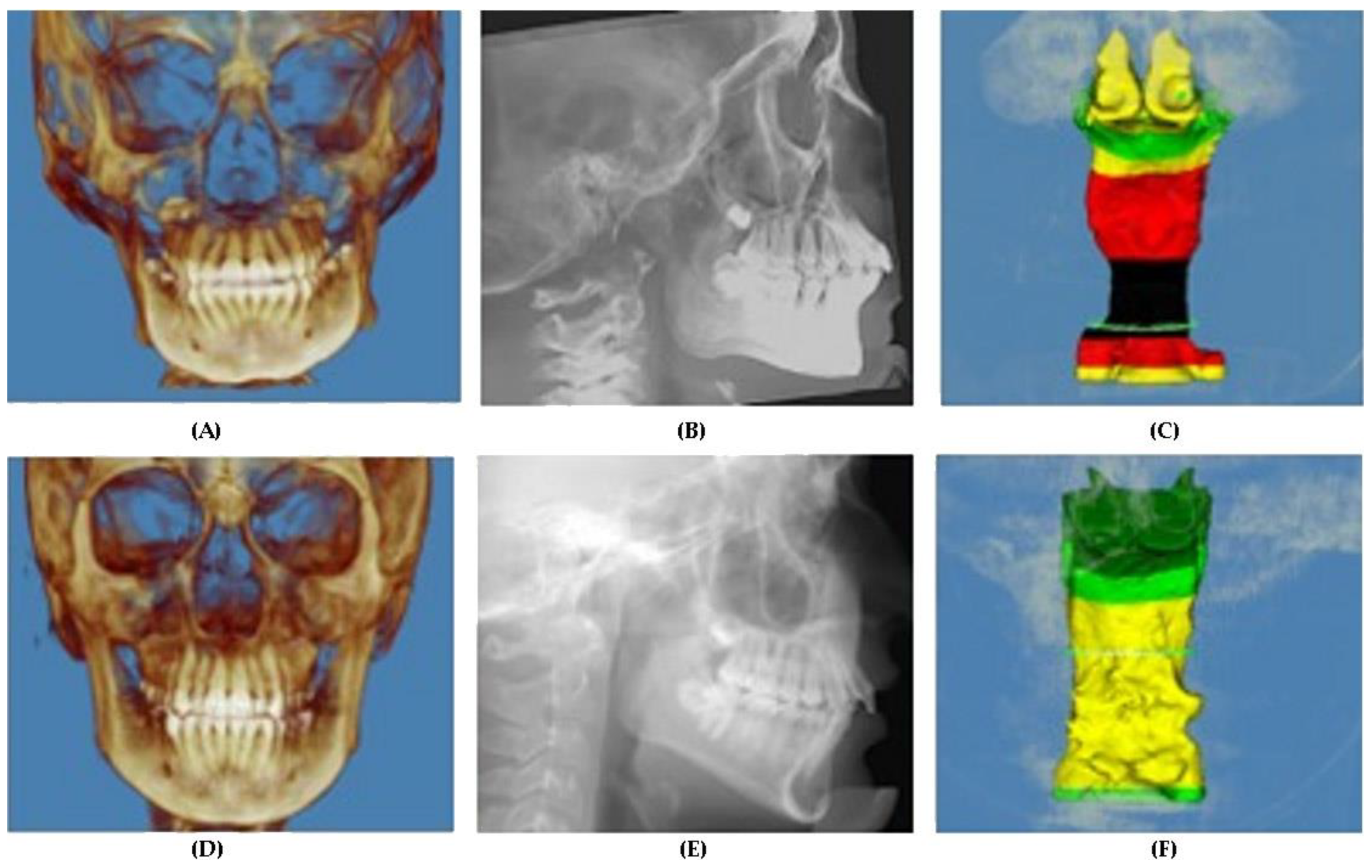
3.2. Airway Analysis
4. Discussion
4.1. Cephalometric Parameters
4.2. Airway Parameters
4.3. Software Analysis and Interpretations
4.4. JIA, Airway and OSA
4.5. Study Limitations
5. Conclusions
- (1).
- There was a difference in the posterior face height between JIA and control patients.
- (2).
- There was a significant difference in total upper airway volume, nasopharynx airway volume, and most constricted cross-sectional area measurements between JIA and control patients.
- (3).
- The ODDs ratio analysis confirmed the association of the statistically significant parameters above.
- (4).
- 50% of JIA patients had an airway with a most constricted cross-sectional area of less than 100 mm2.
- (5).
- 67% of JIA patients had an asymmetric airway form.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crayne, C.B.; Beukelman, T. Juvenile Idiopathic Arthritis: Oligoarthritis and Polyarthritis. Pediatr Clin. N. Am. 2018, 65, 657–674. [Google Scholar] [CrossRef] [Green Version]
- Prakken, B.; Albani, S.; Martini, A. Juvenile idiopathic arthritis. Lancet 2011, 377, 2138–2149. [Google Scholar] [CrossRef] [Green Version]
- Bukovac, L.T.; Perica, M. Juvenile Idiopathic Arthritis. Reumatizam 2016, 63 (Suppl. 1), 53–58. [Google Scholar]
- Hersh, A.O.; Prahalad, S. Immunogenetics of juvenile idiopathic arthritis: A comprehensive review. J. Autoimmun. 2015, 64, 113–124. [Google Scholar] [CrossRef] [Green Version]
- Ringold, S.; Cron, R.Q. The temporomandibular joint in juvenile idiopathic arthritis: Frequently used and frequently arthritic. Pediatr. Rheumatol. 2009, 7, 11. [Google Scholar] [CrossRef] [Green Version]
- Twilt, M.; Schulten, A.J.M.; Nicolaas, P.; Dülger, A.; van Suijlekom-Smit, L.W. Facioskeletal changes in children with juvenile idiopathic arthritis. Ann. Rheum. Dis. 2006, 65, 823–825. [Google Scholar] [CrossRef] [Green Version]
- Kau, C.H.; Allareddy, V.; Stoustrup, P.; Pedersen, T.; Kinard, B.; Cron, R.Q.; Stoll, M.L.; Gilbert, G.H. Management of juvenile idiopathic arthritis: Preliminary qualitative findings from the National Dental Practice-Based Research Network. J. World Fed. Orthod. 2021, 10, 70–73. [Google Scholar] [CrossRef]
- Abramowicz, S.; Levy, J.M.; Prahalad, S.; Travers, C.D.; Angeles-Han, S. Temporomandibular joint involvement in children with juvenile idiopathic arthritis: A preliminary report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 19–23. [Google Scholar] [CrossRef]
- Arabshahi, B.; Cron, R. Temporomandibular joint arthritis in juvenile idiopathic arthritis: The forgotten joint. Curr. Opin. Rheumatol. 2006, 18, 490–495. [Google Scholar] [CrossRef]
- Pawlaczyk-Kamieńska, T.; Paczyk-Wróblewskawla, E.; Borysewicz-Lewicka, M. Early diagnosis of temporomandibular joint arthritis in children with juvenile idiopathic arthritis. A systematic review. Eur. J. Paediatr. Dent. 2020, 21, 219–226. [Google Scholar]
- Stoll, M.L.; Kau, C.H.; Waite, P.D.; Cron, R.Q. Temporomandibular joint arthritis in juvenile idiopathic arthritis, now what? Pediatr. Rheumatol. 2018, 16, 32. [Google Scholar] [CrossRef] [Green Version]
- Abramowicz, S.; Kim, S.; Prahalad, S.; Chouinard, A.-F.; Kaban, L.B. Juvenile arthritis: Current concepts in terminology, etiopathogenesis, diagnosis, and management. Int. J. Oral Maxillofac. Surg. 2016, 45, 801–812. [Google Scholar] [CrossRef]
- Billiau, A.D.; Hu, Y.; Verdonck, A.; Carels, C.; Wouters, C. Temporomandibular joint arthritis in juvenile idiopathic arthritis: Prevalence, clinical and radiological signs, and relation to dentofacial morphology. J. Rheumatol. 2007, 34, 1925–1933. [Google Scholar]
- Abramowicz, S.; Susarla, H.K.; Kim, S.; Kaban, L.B. Physical Findings Associated with Active Temporomandibular Joint Inflammation in Children with Juvenile Idiopathic Arthritis. J. Oral Maxillofac. Surg. 2013, 71, 1683–1687. [Google Scholar] [CrossRef]
- Stabrun, A.E.; Larheim, T.A.; Höyeraal, H.M.; Rösler, M. Reduced mandibular dimensions and asymmetry in juvenile rheumatoid arthritis. Pathogenetic factors. Arthritis Rheum. 1988, 31, 602–611. [Google Scholar] [CrossRef]
- Koos, B.; Twilt, M.; Kyank, U.; Fischer-Brandies, H.; Gaßling, V.; Tzaribachev, N. Reliability of Clinical Symptoms in Diagnosing Temporomandibular Joint Arthritis in Juvenile Idiopathic Arthritis. J. Rheumatol. 2014, 41, 1871–1877. [Google Scholar] [CrossRef]
- Pedersen, T.K.; Küseler, A.; Gelineck, J.; Herlin, T. A prospective study of magnetic resonance and radiographic imaging in relation to symptoms and clinical findings of the temporomandibular joint in children with juvenile idiopathic arthritis. J. Rheumatol. 2008, 35, 1668–1675. [Google Scholar]
- Celebi, A.A.; Cron, R.; Stoll, M.; Simsek, S.; Kinard, B.; Waite, P.D.; Wang, J.; Vo, V.; Tran, L.; Kau, C.H. Comparison of the condyle-fossa relationship and resorption between patients with and without Juvenile Idiopathic Ar-thritis (JIA). J. Oral Maxillofac. Surg. 2022, 80, 422–430. [Google Scholar] [CrossRef]
- Twilt, M.; Mobers, S.M.L.M.; Arends, L.R.; Cate, R.T.; Van Suijlekom-Smit, L. Temporomandibular involvement in juvenile idiopathic arthritis. J. Rheumatol. 2004, 31, 1418–1422. [Google Scholar] [CrossRef]
- Kristensen, K.D.; Stoustrup, P.; Küseler, A.; Pedersen, T.K.; Twilt, M.; Herlin, T. Clinical predictors of temporomandibular joint arthritis in juvenile idiopathic arthritis: A systematic literature review. Semin. Arthritis Rheum. 2016, 45, 717–732. [Google Scholar] [CrossRef]
- Weiss, P.F.; Arabshahi, B.; Johnson, A.; Bilaniuk, L.T.; Zarnow, D.; Cahill, A.M.; Feudtner, C.; Cron, R. High prevalence of temporomandibular joint arthritis at disease onset in children with juvenile idiopathic arthritis, as detected by magnetic resonance imaging but not by ultrasound. Arthritis Rheum. 2008, 58, 1189–1196. [Google Scholar] [CrossRef]
- Koos, B.; Gassling, V.; Bott, S.; Tzaribachev, N.; Godt, A. Pathological changes in the TMJ and the length of the ramus in patients with confirmed juvenile idiopathic arthritis. J. Cranio -Maxillofac. Surg. 2014, 42, 1802–1807. [Google Scholar] [CrossRef]
- Piancino, M.G.; Cannavale, R.; Dalmasso, P.; Tonni, I.; Garagiola, U.; Perillo, L.; Olivieri, A.N. Cranial structure and condylar asymmetry of patients with juvenile idiopathic arthritis: A risky growth pattern. Clin. Rheumatol. 2018, 37, 2667–2673. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, Y.-J.; Darvann, T.A.; Hermann, N.V.; Larsen, P.; Liao, Y.-F.; Bjoern-Joergensen, J.; Kreiborg, S. Facial morphology in children and adolescents with juvenile idiopathic arthritis and moderate to severe temporomandibular joint involvement. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 182–191. [Google Scholar] [CrossRef]
- Kjellberg, H.; Fasth, A.; Kiliaridis, S.; Wenneberg, B.; Thilander, B. Craniofacial structure in children with juvenile chronic arthritis (JCA) compared with healthy children with ideal or postnormal occlusion. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 67–78. [Google Scholar] [CrossRef]
- Kjellberg, H. Juvenile chronic arthritis. Dentofacial morphology, growth, mandibular function and orthodontic treatment. Swed. Dent. J. Suppl. 1995, 109, 1–56. [Google Scholar]
- Sidiropoulou-Chatzigianni, S.; Papadopoulos, M.A.; Kolokithas, G. Dentoskeletal Morphology in Children with Juvenile Idiopathic Arthritis Compared with Healthy Children. J. Orthod. 2001, 28, 53–58. [Google Scholar] [CrossRef]
- Srivastava, K.C.; Shrivastava, D.; Austin, R.D. Journey towards the 3D dental imaging—The milestones in the advancement of dental imaging. Int. J. Adv. Res. 2016, 4, 377–382. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, T.; Enciso, R.; Shintaku, W.H.; Clark, G.T. Evaluation of cross-section airway configuration of obstructive sleep apnea. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Enciso, R.; Nguyen, M.; Shigeta, Y.; Ogawa, T.; Clark, G.T. Comparison of cone-beam CT parameters and sleep questionnaires in sleep apnea patients and control subjects. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, 285–293. [Google Scholar] [CrossRef] [Green Version]
- Buchanan, A.; Cohen, R.; Looney, S.; Kalathingal, S.; De Rossi, S. Cone-beam CT analysis of patients with obstructive sleep apnea compared to normal controls. Imaging Sci. Dent. 2016, 46, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Momany, S.M.; AlJamal, G.; Shugaa-Addin, B.; Khader, Y.S. Cone Beam Computed Tomography Analysis of Upper Airway Measurements in Patients with Obstructive Sleep Apnea. Am. J. Med. Sci. 2016, 352, 376–384. [Google Scholar] [CrossRef]
- Tikku, T.; Khanna, R.; Sachan, K.; Agarwal, A.; Srivastava, K.; Lal, A. Dimensional and volumetric analysis of the oropharyngeal region in obstructive sleep apnea patients: A cone beam computed tomography study. Dent. Res. J. 2016, 13, 396–404. [Google Scholar]
- Hsu, W.; Kang, K.; Yao, C.J.; Chou, C.; Weng, W.; Lee, P.; Chen, Y. Evaluation of Upper Airway in Children with Obstructive Sleep Apnea Using Cone-Beam Computed Tomography. Laryngoscope 2021, 131, 680–685. [Google Scholar] [CrossRef]
- Masoud, A.I.; Alwadei, A.H.; Gowharji, L.F.; Park, C.G.; Carley, D.W. Relating three-dimensional airway measurements to the apnea-hypopnea index in pediatric sleep apnea patients. Orthod. Craniofac. Res. 2021, 24, 137–146. [Google Scholar] [CrossRef]
- Ward, T.M.; Chen, M.L.; Landis, C.A.; Ringold, S.; Beebe, D.W.; Pike, K.C.; Wallace, C.A. Congruence between polysomnography obstructive sleep apnea and the pediatric sleep questionnaire: Fatigue and health-related quality of life in juvenile idiopathic arthritis. Qual. Life Res. 2017, 26, 779–788. [Google Scholar] [CrossRef] [Green Version]
- Tarakçı, E.; Arman, N.; Barut, K.; Şahin, S.; Adroviç, A.; Kasapçopur, Ö. Fatigue and sleep in children and adolescents with juvenile idiopathic arthritis: A cross-sectional study. Turk. J. Med. Sci. 2019, 49, 58–65. [Google Scholar] [CrossRef]
- Armbrust, W.; Siers, N.E.; Lelieveld, O.T.; Mouton, L.J.; Tuinstra, J.; Sauer, P. Fatigue in patients with juvenile idiopathic arthritis: A systematic review of the literature. Semin. Arthritis Rheum. 2016, 45, 587–595. [Google Scholar] [CrossRef]
- Trosman, I.; Trosman, S.J. Cognitive and Behavioral Consequences of Sleep Disordered Breathing in Children. Med. Sci. 2017, 5, 30. [Google Scholar] [CrossRef]
- Guilleminault, C.; Korobkin, R.; Winkle, R. A review of 50 children with obstructive sleep apnea syndrome. Lung 1981, 159, 275–287. [Google Scholar] [CrossRef]
- Özdemir, H.; Altin, R.; Söğüt, A.; Çınar, F.; Mahmutyazıcıoğlu, K.; Kart, L.; Uzun, L.; Davşancı, H.; Gündoğdu, S.; Tomaç, N. Craniofacial differences according to AHI scores of children with obstructive sleep apnoea syndrome: Cephalometric study in 39 patients. Pediatr. Radiol. 2004, 34, 393–399. [Google Scholar]
- Katz, E.S.; D’Ambrosio, C.M. Pathophysiology of Pediatric Obstructive Sleep Apnea. Proc. Am. Thorac. Soc. 2008, 5, 253–262. [Google Scholar] [CrossRef]
- Galeotti, A.; Festa, P.; Viarani, V.; Pavone, M.; Sitzia, E.; Piga, S.; Cutrera, R.; De Vincentiis, G.; D’Antò, V. Correlation between cephalometric variables and obstructive sleep apnoea severity in children. Eur. J. Paediatr. Dent. 2019, 20, 43–47. [Google Scholar] [PubMed]
- Joseph, A.; Elbaum, J.; Cisneros, G.J.; Eisig, S.B. A cephalometric comparative study of the soft tissue airway dimensions in persons with hyperdivergent and normodivergent facial patterns. J. Oral Maxillofac. Surg. 1998, 56, 135–139; discussion 139–140. [Google Scholar] [CrossRef]
- Flores-Mir, C.; Korayem, M.; Heo, G.; Witmans, M.; Major, M.P.; Major, P.W. Craniofacial morphological characteristics in children with obstructive sleep apnea syndrome: A systematic review and meta-analysis. J. Am. Dent. Assoc. 2013, 144, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Katyal, V.; Pamula, Y.; Martin, A.J.; Daynes, C.N.; Kennedy, J.D.; Sampson, W.J. Craniofacial and upper airway morphology in pediatric sleep-disordered breathing: Systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 20–30.e3. [Google Scholar] [CrossRef]
- Kawashima, S.; Niikuni, N.; Chia-Hung, L.; Takahasi, Y.; Kohno, M.; Nakajima, I.; Akasaka, M.; Sakata, H.; Akashi, S. Cephalometric Comparisons of Craniofacial and Upper Airway Structures in Young Children with Obstructive Sleep Apnea Syndrome. Ear Nose Throat J. 2000, 79, 499–502, 505–506. [Google Scholar] [CrossRef] [Green Version]
- Bloom, B.J.; Owens, J.A.; McGuinn, M.; Nobile, C.; Schaeffer, L.; Alario, A.J. Sleep and its relationship to pain, dysfunction, and disease activity in juvenile rheumatoid arthritis. J. Rheumatol. 2002, 29, 169–173. [Google Scholar]
- Ward, T.M.; Beebe, D.W.; Chen, M.L.; Landis, C.A.; Ringold, S.; Pike, K.; Wallace, C.A. Sleep Disturbances and Neurobehavioral Performance in Juvenile Idiopathic Arthritis. J. Rheumatol. 2017, 44, 361–367. [Google Scholar] [CrossRef] [Green Version]
- Lumeng, J.C.; Chervin, R.D. Epidemiology of Pediatric Obstructive Sleep Apnea. Proc. Am. Thorac. Soc. 2008, 5, 242–252. [Google Scholar] [CrossRef] [Green Version]
- Ward, T.M.; Archbold, K.; Lentz, M.; Ringold, S.; Wallace, C.A.; Landis, C.A. Sleep Disturbance, Daytime Sleepiness, and Neurocognitive Performance in Children with Juvenile Idiopathic Arthritis. Sleep 2010, 33, 252–259. [Google Scholar] [CrossRef] [Green Version]
- Schendel, S.A.; Jacobson, R.; Khalessi, S. Airway Growth and Development: A Computerized 3-Dimensional Analysis. J. Oral Maxillofac. Surg. 2012, 70, 2174–2183. [Google Scholar] [CrossRef] [PubMed]
- Nath, M.; Ahmed, J.; Ongole, R.; Denny, C.; Shenoy, N. CBCT analysis of pharyngeal airway volume and comparison of airway volume among patients with skeletal Class I, Class II, and Class III malocclusion: A retrospective study. Cranio 2021, 39, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Alhammadi, M.S.; Almashraqi, A.A.; Halboub, E.; Almahdi, S.; Jali, T.; Atafi, A.; Alomar, F. Pharyngeal airway spaces in different skeletal malocclusions: A CBCT 3D assessment. Cranio 2021, 39, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Chen, H.; Jia, L.; Xu, X.; Guo, J. The relationship between three-dimensional craniofacial and upper airway anatomical variables and severity of obstructive sleep apnoea in adults. Eur. J. Orthod. 2021, 44, 78–85. [Google Scholar] [CrossRef]
- Tseng, Y.-C.; Tsai, F.-C.; Chou, S.-T.; Hsu, C.-Y.; Cheng, J.-H.; Chen, C.-M. Evaluation of pharyngeal airway volume for different dentofacial skeletal patterns using cone-beam computed tomography. J. Dent. Sci. 2021, 16, 51–57. [Google Scholar] [CrossRef]
- Castro-Silva, L.; Monnazzi, M.S.; Spin-Neto, R.; de Moraes, M.; Miranda, S.; Gabrielli, M.F.R.; Filho, V.P. Cone-beam evaluation of pharyngeal airway space in class I, II, and III patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 679–683. [Google Scholar] [CrossRef]
- Redline, S.; Tishler, P.V.; Schluchter, M.; Aylor, J.; Clark, K.; Graham, G. Risk Factors for Sleep-disordered Breathing in Children. Associations with obesity, race, and respiratory problems.Children. Am. J. Respir. Crit. Care Med. 1999, 159 Pt 1, 1527–1532. [Google Scholar] [CrossRef]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Ward, S.D.; Sheldon, S.H.; Shiffman, R.N. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012, 130, 576–584. [Google Scholar] [CrossRef] [Green Version]
- Isono, S.; Shimada, A.; Utsugi, M.; Konno, A.; Nishino, T. Comparison of static mechanical properties of the passive pharynx be-tween normal children and children with sleep-disordered breathing. Am. J. Respir. Crit. Care Med. 1998, 157 Pt 1, 1204–1212. [Google Scholar] [CrossRef]
- Lin, S.Y.; Melvin, T.-A.N.; Boss, E.F.; Ishman, S.L. The association between allergic rhinitis and sleep-disordered breathing in children: A systematic review. Int. Forum Allergy Rhinol. 2013, 3, 504–509. [Google Scholar] [CrossRef]
- Cao, Y.; Wu, S.; Zhang, L.; Yang, Y.; Cao, S.; Li, Q. Association of allergic rhinitis with obstructive sleep apnea: A meta-analysis. Medicine 2018, 97, e13783. [Google Scholar] [CrossRef] [PubMed]
- Gileles-Hillel, A.; Alonso-Álvarez, M.L.; Gozal, L.; Peris, E.; Cordero-Guevara, J.A.; Terán-Santos, J.; Martinez, M.G.; Jurado-Luque, M.J.; Corral-Peñafiel, J.; Duran-Cantolla, J.; et al. Inflammatory markers and obstructive sleep apnea in obese children: The NANOS study. Mediat. Inflamm. 2014, 2014, 605280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tam, C.S.; Wong, M.; McBain, R.; Bailey, S.; Waters, K.A. Inflammatory measures in children with obstructive sleep apnoea. J. Paediatr. Child. Health 2006, 42, 277–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Küseler, A.; Pedersen, T.K.; Gelineck, J.; Herlin, T. A 2 year follow up study of enhanced magnetic resonance imaging and clinical examination of the temporomandibular joint in children with juvenile idiopathic arthritis. J. Rheumatol. 2005, 32, 162–169. [Google Scholar] [PubMed]
- Gozal, D.; Serpero, L.D.; Capdevila, O.; Kheirandish, S.; Gozal, L. Systemic inflammation in non-obese children with obstructive sleep apnea. Sleep Med. 2008, 9, 254–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcus, C.L. Pathophysiology of childhood obstructive sleep apnea: Current concepts. Respir. Physiol. 2000, 119, 143–154. [Google Scholar] [CrossRef]
- Ryan, D.P.O.; Bianchi, J.; Ignácio, J.; Wolford, L.M.; Gonçalves, J.R. Cone-beam computed tomography airway measurements: Can we trust them? Am. J. Orthod. Dentofac. Orthop. 2019, 156, 53–60. [Google Scholar] [CrossRef]
- El, H.; Palomo, J.M. Measuring the airway in 3 dimensions: A reliability and accuracy study. Am. J. Orthod. Dentofac. Orthop. 2010, 137 (Suppl. 4), S50.e1–S50.e9. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Control Mean (SD) | JIA Mean (SD) | p-Value Mean (SD) | ODDS Ratio (Confidence Range) |
|---|---|---|---|---|
| Age (years) | 13.75 (2.91) | 13.59 (2.73) | 0.825 | 1 |
| SNA (Degrees) | 83.06 (3.45) | 81.53 (4.27) | 0.12 | 1.00 (0.42–2.35) |
| SNB (Degrees) | 79.29 (3.65) | 78.43 (4.42) | 0.398 | 0.88 (0.32–2.44) |
| ANB (Degrees) | 3.69 (2.84) | 3.21 (2.15) | 0.448 | 0.45 (0.16–1.25) |
| Anterior Face Height(mm) | 113.12 (9.46) | 109.16 (8.51) | 0.083 | 0.72 (0.23–2.23) |
| Posterior Face Height (mm) | 75.39 (7.05) | 71.06 (7.87) | 0.024 * | 5.40 (1.66–17.56) * |
| PFH/AFH Ratio | 66.58 (5.67) | 65.12 (5.08) | 0.281 | 1.29 (0.48–3.44) |
| SN-MP (Degrees) | 32.45 (7.30) | 33.51 (6.12) | 0.529 | 0.85 (0.28–2.59) |
| FMA (Degrees) | 22.97 (7.33) | 22.88 (5.79) | 0.958 | 1 (0.34–2.97) |
| Overbite (mm) | 2.81 (2.37) | 2.13 (1.28) | 0.159 | 0.77 (0.15–3.53) |
| Overjet (mm) | 4.15 (2.33) | 4.43 (3.90) | 0.734 | 0.68 (0.25–1.84) |
| Oropharynx Airway Volume (mm3) | 14,047.31 (5586.36) | 11,098.03 (6268.15) | 0.051 | 3.40 (1.18–9.81) * |
| Nasopharynx Airway Volume (mm3) | 5827.03 (2425.85) | 4392.19 (1203.04) | 0.004 * | 4.59 (1.54–13.67) * |
| Total Upper Airway Volume (mm3) | 19,874.34 (6790.35) | 15,490.22 (6945.79) | 0.013 * | 3.22 (0.77–13.50) * |
| Minimal Cross-Sectional Area (mm2) | 202.50 (103.03) | 143.75 (103.23) | 0.026 * | 2.96 (0.95–9.21) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gibson, M.; Cron, R.Q.; Stoll, M.L.; Kinard, B.E.; Patterson, T.; Kau, C.H. A 3D CBCT Analysis of Airway and Cephalometric Values in Patients Diagnosed with Juvenile Idiopathic Arthritis Compared to a Control Group. Appl. Sci. 2022, 12, 4286. https://doi.org/10.3390/app12094286
Gibson M, Cron RQ, Stoll ML, Kinard BE, Patterson T, Kau CH. A 3D CBCT Analysis of Airway and Cephalometric Values in Patients Diagnosed with Juvenile Idiopathic Arthritis Compared to a Control Group. Applied Sciences. 2022; 12(9):4286. https://doi.org/10.3390/app12094286
Chicago/Turabian StyleGibson, Matthew, Randy Q. Cron, Matthew L. Stoll, Brian E. Kinard, Tessa Patterson, and Chung How Kau. 2022. "A 3D CBCT Analysis of Airway and Cephalometric Values in Patients Diagnosed with Juvenile Idiopathic Arthritis Compared to a Control Group" Applied Sciences 12, no. 9: 4286. https://doi.org/10.3390/app12094286