
Robotic-Assisted Hand Therapy with Gloreha Sinfonia for the Improvement of Hand Function after Pediatric Stroke: A Case Report


 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participant
2.3. Gloreha Sinfonia
- Passive mobilization exercises (the movements are carried out entirely by the device);
- Active-assisted exercises with graphic interface (the patient trains in flexion–extension of the fingers thanks to motivating games; the motors support and integrate the patient’s voluntary movements only to the extent necessary);
- Active-assisted functional exercises with real objects (the patient trains fine grip);
- Interactive games (the patient can improve dexterity);
- All possible combinations of flexion–extension of the fingers;
- Therapies based on the action–observation approach (the patient performs a task that he first observed in a preview video, supported by the robot);
- Exercises with partial or total compensation of the weight of the upper limb, free to float in space interacting with real objects (the system is able to self-adjust based on the residual abilities of the patient).
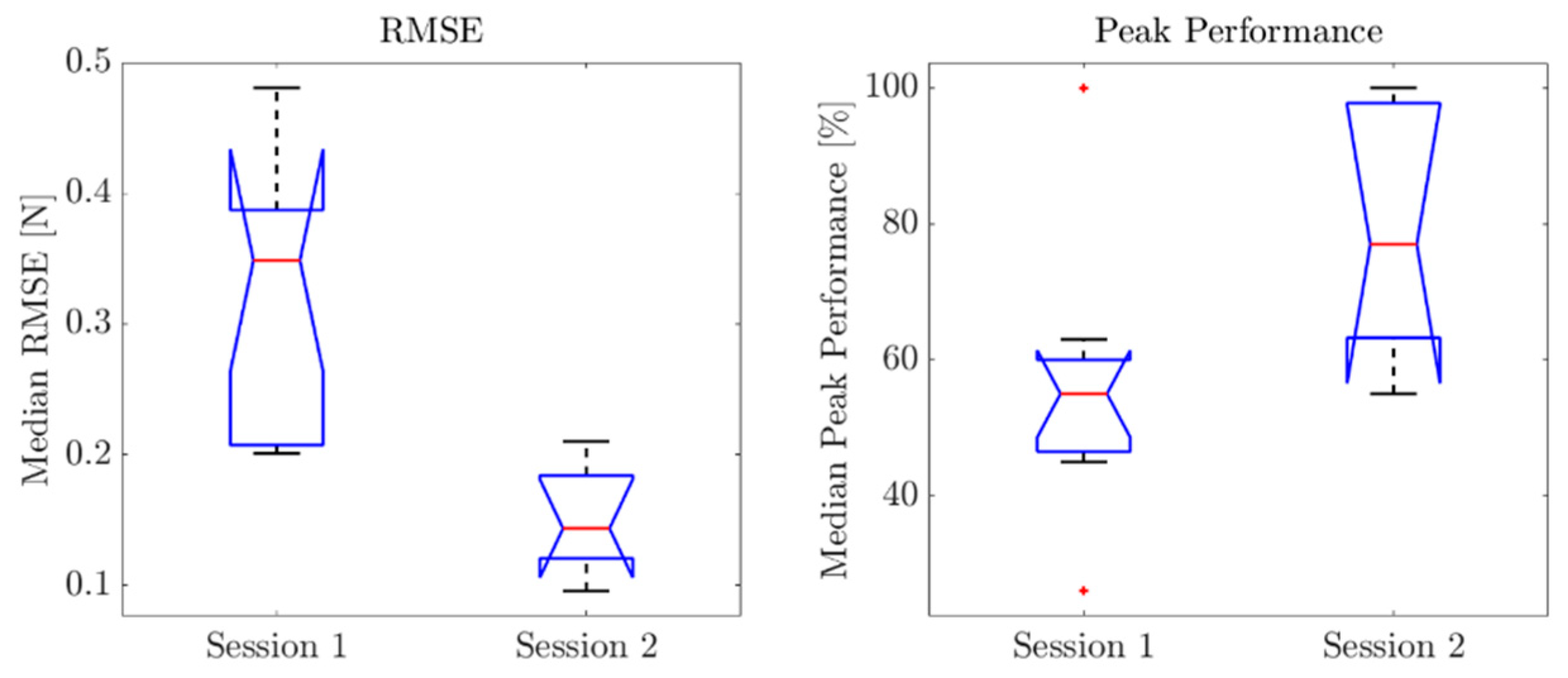
2.4. Force Assessment System Based on Virtual Reality Games
2.5. Intervention
2.6. Outcome Measures
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferriero, D.M.; Fullerton, H.J.; Bernard, T.J.; Billinghurst, L.; Daniels, S.R.; DeBaun, M.R.; Deveber, G.; Ichord, R.N.; Jordan, L.C.; Massicotte, P.; et al. Management of Stroke in Neonates and Children: A Scientific Statement from the American Heart Association/American Stroke Association. Stroke 2019, 50, e51–e96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallick, A.A.; Ganesan, V.; Kirkham, F.J.; Fallon, P.; Hedderly, T.; McShane, T.; Parker, A.P.; Wassmer, E.; Wraige, E.; Amin, S.; et al. Diagnostic Delays in Paediatric Stroke. J. Neurol. Neurosurg. Psychiatry 2015, 86, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Mallick, A.A.; Ganesan, V.; Kirkham, F.J.; Fallon, P.; Hedderly, T.; McShane, T.; Parker, A.P.; Wassmer, E.; Wraige, E.; Amin, S.; et al. Childhood Arterial Ischaemic Stroke Incidence, Presenting Features, and Risk Factors: A Prospective Population-Based Study. Lancet Neurol. 2014, 13, 35–43. [Google Scholar] [CrossRef]
- Lanthier, S.; Carmant, L.; David, M.; Larbrisseau, A.; de Veber, G. Stroke in Children: The Coexistence of Multiple Risk Factors Predicts Poor Outcome. Neurology 2000, 54, 371–378. [Google Scholar] [CrossRef]
- Riela, A.R.; Roach, E.S. Etiology of Stroke in Children. J. Child Neurol. 1993, 8, 201–220. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Paediatrics and Child Health Stroke in Childhood—Clinical Guideline for Diagnosis, Management and Rehabilitation|RCPCH. Available online: https://www.rcpch.ac.uk/resources/stroke-in-childhood-clinical-guideline (accessed on 10 March 2022).
- DeLaroche, A.M.; Sivaswamy, L.; Farooqi, A.; Kannikeswaran, N. Pediatric Stroke and Its Mimics: Limitations of a Pediatric Stroke Clinical Pathway. Pediatr. Neurol. 2018, 80, 35–41. [Google Scholar] [CrossRef]
- Ictus Cerebrale: Linee Guida Italiane Di Prevenzione e Trattamento Raccomandazioni e Sintesi. Available online: https://www.iso-stroke.it/wp-content/uploads/2017/02/LIBRO-SPREAD-VIII-ED-13-09-16.pdf (accessed on 10 March 2022).
- Bütefisch, C.; Hummelsheim, H.; Denzler, P.; Mauritz, K.H. Repetitive Training of Isolated Movements Improves the Outcome of Motor Rehabilitation of the Centrally Paretic Hand. J. Neurol. Sci. 1995, 130, 59–68. [Google Scholar] [CrossRef]
- Hendricks, H.T.; van Limbeek, J.; Geurts, A.C.; Zwarts, M.J. Motor Recovery after Stroke: A Systematic Review of the Literature. Arch. Phys. Med. Rehabil. 2002, 83, 1629–1637. [Google Scholar] [CrossRef]
- Thielman, G.; Kaminski, T.; Gentile, A.M. Rehabilitation of Reaching after Stroke: Comparing 2 Training Protocols Utilizing Trunk Restraint. Neurorehabil. Neural Repair 2008, 22, 697–705. [Google Scholar] [CrossRef]
- Eliasson, A.C.; Nordstrand, L.; Ek, L.; Lennartsson, F.; Sjöstrand, L.; Tedroff, K.; Krumlinde-Sundholm, L. The Effectiveness of Baby-CIMT in Infants Younger than 12 Months with Clinical Signs of Unilateral-Cerebral Palsy; an Explorative Study with Randomized Design. Res. Dev. Disabil. 2018, 72, 191–201. [Google Scholar] [CrossRef]
- Kwakkel, G.; Wagenaar, R.C.; Koelman, T.W.; Lankhorst, G.J.; Koetsier, J.C. Effects of Intensity of Rehabilitation after Stroke. A Research Synthesis. Stroke 1997, 28, 1550–1556. [Google Scholar] [CrossRef] [PubMed]
- Feys, H.M.; de Weerdt, W.J.; Selz, B.E.; Cox Steck, G.A.; Spichiger, R.; Vereeck, L.E.; Putman, K.D.; van Hoydonck, G.A. Effect of a Therapeutic Intervention for the Hemiplegic Upper Limb in the Acute Phase after Stroke: A Single-Blind, Randomized, Controlled Multicenter Trial. Stroke 1998, 29, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Frascarelli, F.; Masia, L.; Di Rosa, G.; Cappa, P.; Petrarca, M.; Castelli, E.; Krebs, H.I. The Impact of Robotic Rehabilitation in Children with Acquired or Congenital Movement Disorders. Eur. J. Phys. Rehabil. Med. 2009, 45, 135–141. Available online: https://www.minervamedica.it/it/riviste/europa-medicophysica/articolo.php?cod=R33Y2009N01A0135 (accessed on 10 March 2022). [PubMed]
- Doerbeck, V.; Nallinger, A.; Burger, H.; Rosner, V.; Machuta, K.; Gruender, S.; Nastulla, T.; Schroeder, S.; Berweck, S. Integration of Armeo Spring Pediatrics in Inpatient Rehabilitation of Children and Adolescents with Hemiparesis. Neuropediatrics 2012, 43, PS14_11. [Google Scholar] [CrossRef]
- Friel, K.M.; Kuo, H.C.; Fuller, J.; Ferre, C.L.; Brandão, M.; Carmel, J.B.; Bleyenheuft, Y.; Gowatsky, J.L.; Stanford, A.D.; Rowny, S.B.; et al. Skilled Bimanual Training Drives Motor Cortex Plasticity in Children with Unilateral Cerebral Palsy. Neurorehabil. Neural Repair 2016, 30, 834–844. [Google Scholar] [CrossRef] [Green Version]
- Mirkowski, M.; McIntyre, A.; Faltynek, P.; Sequeira, N.; Cassidy, C.; Teasell, R. Nonpharmacological Rehabilitation Interventions for Motor and Cognitive Outcomes following Pediatric Stroke: A Systematic Review. Eur. J. Pediatr. 2019, 178, 433–454. [Google Scholar] [CrossRef]
- Gordon, A.M.; Okita, S.Y. Augmenting Pediatric Constraint-Induced Movement Therapy and Bimanual Training with Video Gaming Technology. Technol. Disabil. 2010, 22, 179–191. [Google Scholar] [CrossRef]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; Group, C. Standards & Guidelines CARE: Linee Guida per Il Reporting Di Casi Clinici. Evidence 2016, 8, e1000147. [Google Scholar]
- Miccinilli, S.; Bravi, M.; Foti, C.; Morrone, M.; Maselli, M.; Santacaterina, F.; Scotto Di Luzio, F.; Zollo, L.; Sterzi, S.; Bressi, F. Robotic Hand Treatment of Patients Affected by Chronic Stroke: A Monocentric Longitudinal Pilot Study. J. Biol. Regul. Homeost. Agents 2020, 34, 79–86. [Google Scholar]
- Kurillo, G.; Gregoric, M.; Goljar, N.; Bajd, T. Grip Force Tracking System for Assessment and Rehabilitation of Hand Function. Technol. Health Care 2005, 13, 137–149. Available online: https://pubmed.ncbi.nlm.nih.gov/15990417/ (accessed on 6 April 2022). [CrossRef]
- Lindberg, P.G.; Roche, N.; Robertson, J.; Roby-Brami, A.; Bussel, B.; Maier, M.A. Affected and Unaffected Quantitative Aspects of Grip Force Control in Hemiparetic Patients after Stroke. Brain Res. 2012, 1452, 96–107. [Google Scholar] [CrossRef] [PubMed]
- de Pasquale, G.; Mastrototaro, L.; Pia, L.; Burin, D. Wearable System with Embedded Force Sensors for Neurologic Rehabilitation Trainings. In Proceedings of the Symposium on Design, Test, Integration and Packaging of MEMS/MOEMS, DTIP 2018, Rome, Italy, 22–25 May 2018; pp. 1–4. [Google Scholar] [CrossRef]
- Lapresa, M.; Tamantini, C.; Scotto Di Luzio, F.; Cordella, F.; Bravi, M.; Miccinilli, S.; Zollo, L. A Smart Solution for Proprioceptive Rehabilitation through M-IMU Sensors. In Proceedings of the 2020 IEEE International Workshop on Metrology for Industry 4.0 and IoT, MetroInd 4.0 and IoT 2020, Rome, Italy, 3–5 June 2020; pp. 591–595. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The index of adl: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.W.; Lin, K.C.; Wu, C.Y.; Shih, T.Y.; Li, M.W.; Chen, C.L. Comparison of Proximal versus Distal Upper-Limb Robotic Rehabilitation on Motor Performance after Stroke: A Cluster Controlled Trial. Sci. Rep. 2018, 8, 2091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, S.J.; Fulk, G.D.; Boyne, P. Clinically Important Differences for the Upper-Extremity Fugl-Meyer Scale in People with Minimal to Moderate Impairment Due to Chronic Stroke. Phys. Ther. 2012, 92, 791–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, D.T. Benefits of a Virtual Play Rehabilitation Environment for Children with Cerebral Palsy on Perceptions of Self-Efficacy: A Pilot Study. Pediatr. Rehabil. 2002, 5, 141–148. [Google Scholar] [CrossRef]
- Wann, J.P.; Rushton, S.K.; Smyth, M.; Jones, D. Virtual Environments for the Rehabilitation of Disorders of Attention and Movement. Stud. Health Technol. Inform. 1997, 44, 157–164. [Google Scholar] [CrossRef]
- Rizzo, A.A.; Buckwalter, J.G.; Neumann, U.; Kesselman, C.; Thiebaux, M. Basic Issues in the Application of Virtual Reality for the Assessment and Rehabilitation of Cognitive Impairments and Functional Disabilities. CyberPsychol. Behav. 2009, 1, 59–78. [Google Scholar] [CrossRef]
- Alt Murphy, M.; Häger, C.K. Kinematic Analysis of the Upper Extremity after Stroke—How Far Have We Reached and What Have We Grasped? Phys. Ther. Rev. 2015, 20, 137–155. [Google Scholar] [CrossRef]
- Čolović, H.; Dimitrijević, L.; Đurić, V.; Janković, S. Upper Limb Robotic Neurorehabilitation after Pediatric Stroke. Srp. Arh. Za Celok. Lek. 2020, 148, 368–376. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T0 | T1 | |
|---|---|---|
| ADL | 4/6 | 6/6 |
| FMA-UE | 34/66 | 49/66 |
| VAS | 0/10 | 0/10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bressi, F.; Santacaterina, F.; Cricenti, L.; Campagnola, B.; Nasto, F.; Assenza, C.; Morelli, D.; Cordella, F.; Lapresa, M.; Zollo, L.; et al. Robotic-Assisted Hand Therapy with Gloreha Sinfonia for the Improvement of Hand Function after Pediatric Stroke: A Case Report. Appl. Sci. 2022, 12, 4206. https://doi.org/10.3390/app12094206
Bressi F, Santacaterina F, Cricenti L, Campagnola B, Nasto F, Assenza C, Morelli D, Cordella F, Lapresa M, Zollo L, et al. Robotic-Assisted Hand Therapy with Gloreha Sinfonia for the Improvement of Hand Function after Pediatric Stroke: A Case Report. Applied Sciences. 2022; 12(9):4206. https://doi.org/10.3390/app12094206
Chicago/Turabian StyleBressi, Federica, Fabio Santacaterina, Laura Cricenti, Benedetta Campagnola, Francesca Nasto, Carla Assenza, Daniela Morelli, Francesca Cordella, Martina Lapresa, Loredana Zollo, and et al. 2022. "Robotic-Assisted Hand Therapy with Gloreha Sinfonia for the Improvement of Hand Function after Pediatric Stroke: A Case Report" Applied Sciences 12, no. 9: 4206. https://doi.org/10.3390/app12094206