
Seizure Prediction Based on Transformer Using Scalp Electroencephalogram



Abstract
:1. Introduction
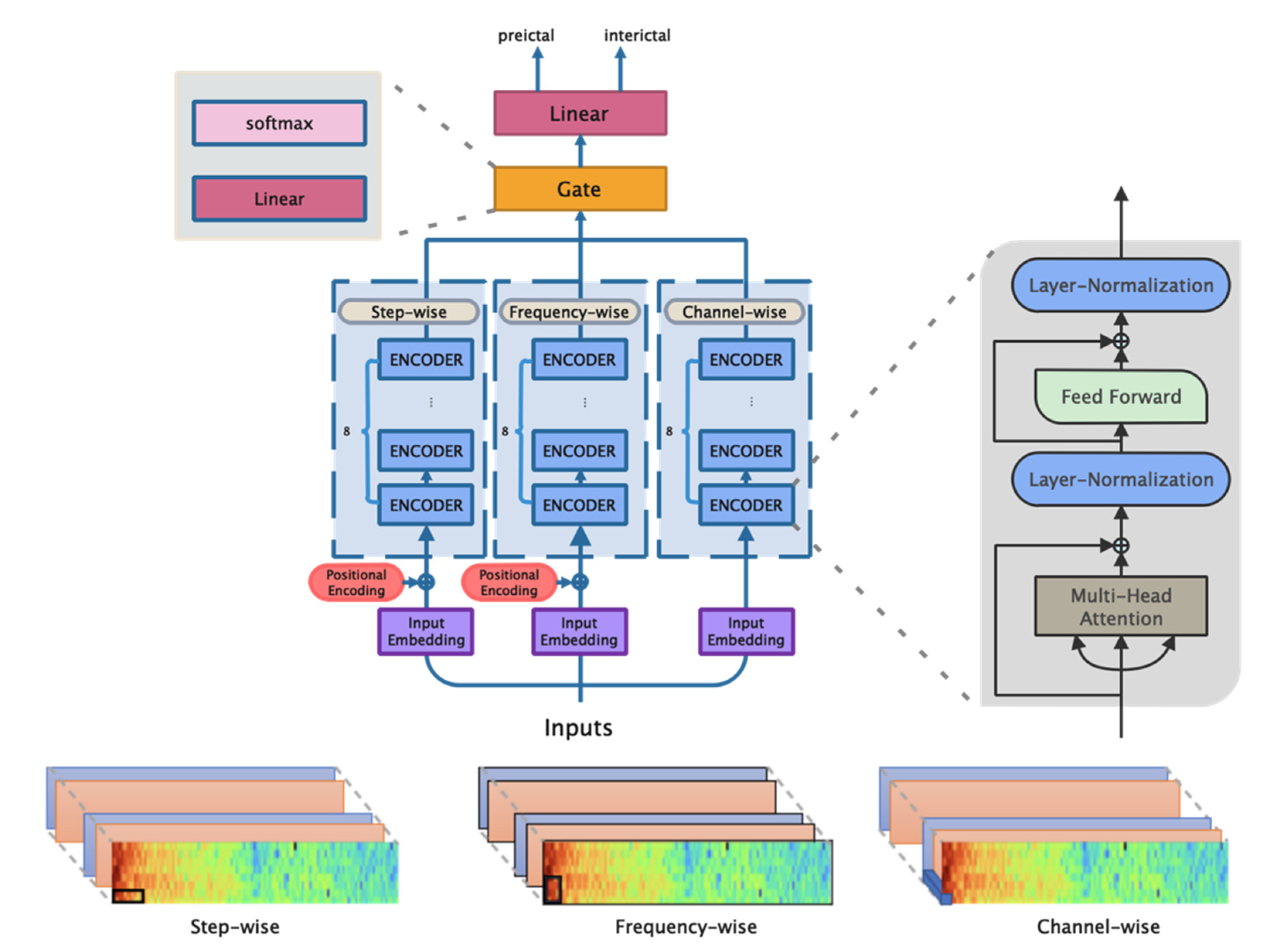
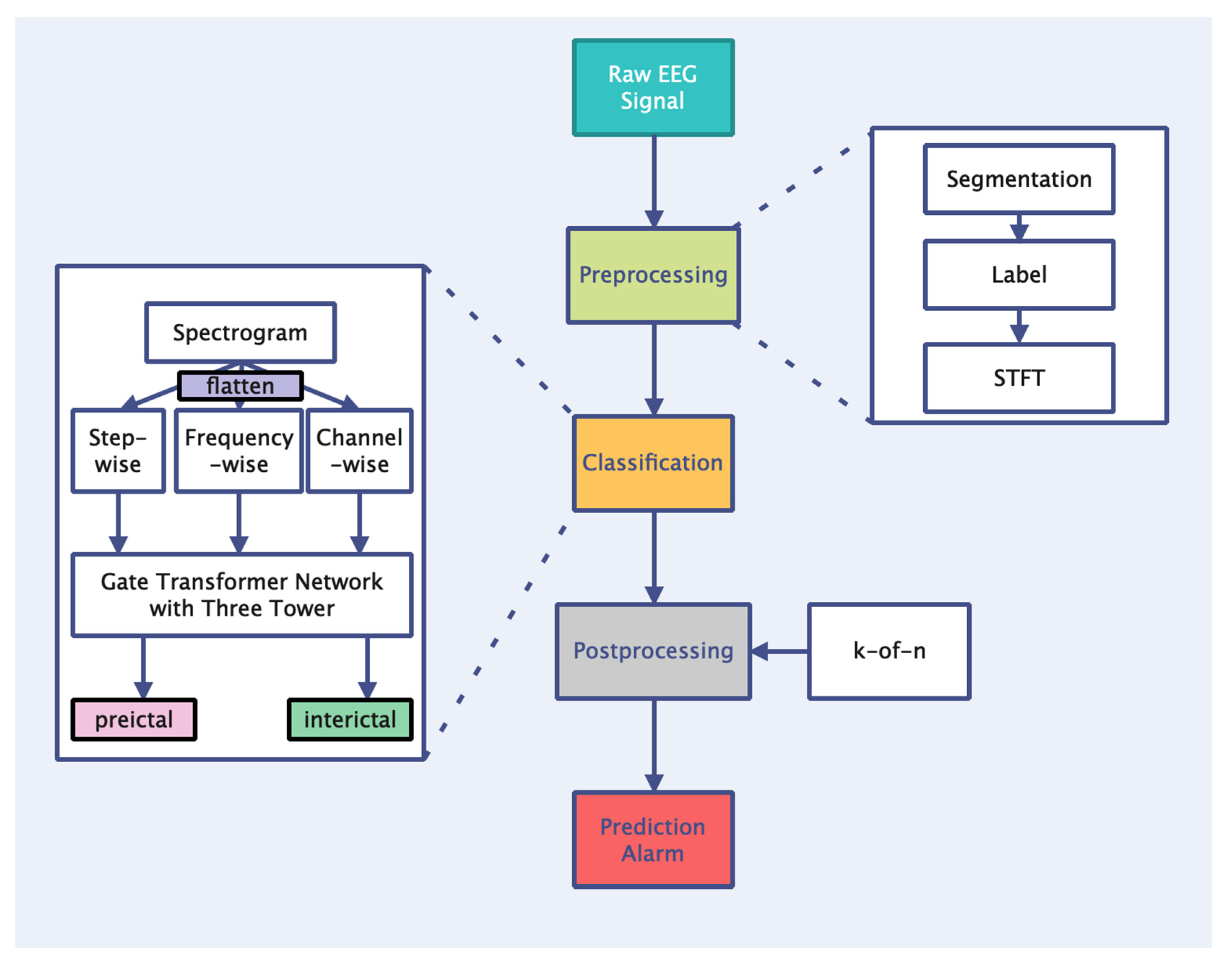
- Based on the transformer’s self-attention coding layer and gating mechanism, a transformer network with a three-tower structure is established to extract and fuse the features of epileptic EEG signals from different dimensions, which improves the learning ability of the time, spectrum, and spatial information.
- A feature engineering scheme for the EEG sequence prediction task is proposed that uses STFT to extract the hidden laws of EEG signals and improve the upper-performance limit of the model.
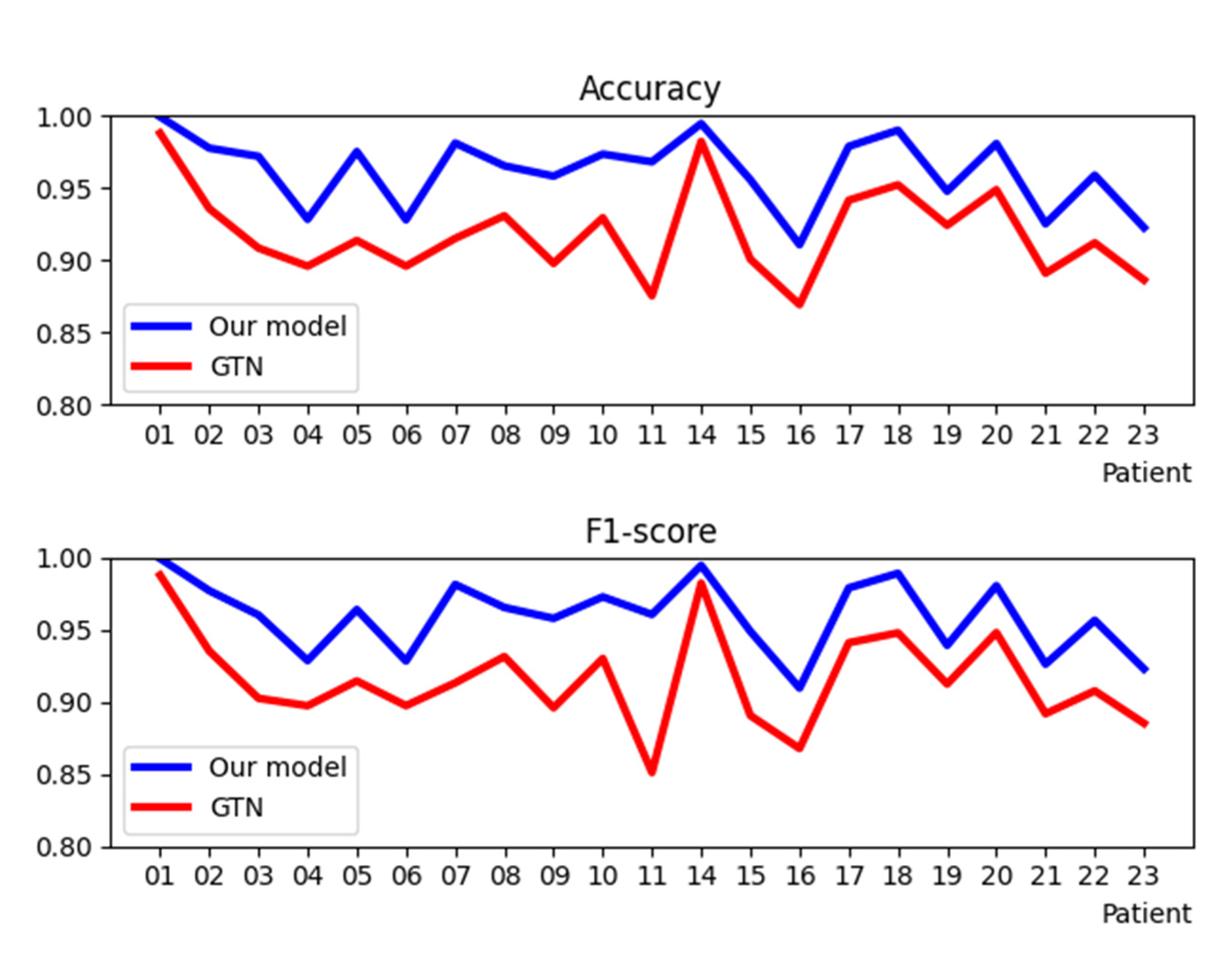
- A three-tower transformer network is proposed to deal with the seizure prediction task. The experimental results for a Children’s Hospital Boston and the Massachusetts Institute of Technology (CHB-MIT) dataset show that our method is superior to the existing ones.
2. Materials and Methods
2.1. EEG Database
2.2. Preprocessing
2.3. Classification
2.4. Performance Evaluation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Report. 2018. Available online: http://www.who.int/mediacentre/factsheets/fs999/en/ (accessed on 10 February 2022).
- Alshebeili, S.A.; Sedik, A.; Abd El-Rahiem, B.; Alotaiby, T.N.; El Banby, G.M.; El-Khobby, H.A.; Ali, M.A.A.; Khalaf, A.A.M.; Abd El-Samie, F.E. Inspection of EEG signals for efficient seizure prediction. Appl. Acoust. 2020, 166, 107327. [Google Scholar] [CrossRef]
- Gotman, J. Automatic recognition of eplieptic seizures in the EEG. Electroencephalogr. Clin. Neurophysiol. 1982, 54, 530–540. [Google Scholar] [CrossRef]
- Srinivasan, V.; Eswaran, C. Artificial neural network based epileptic detection using time-domain and frequency-domain features. J. Med. Syst. 2005, 29, 647–660. [Google Scholar] [CrossRef] [PubMed]
- Winterhalder, M.; Maiwald, T.; Voss, H.; Aschenbrenner-Scheibe, R.; Timmer, J.; Schulze-Bonhage, A. The seizure prediction characteristic: A general framework to assess and compare seizure prediction methods. Epilepsy Behav. 2003, 4, 318–325. [Google Scholar] [CrossRef]
- Joshi, V.; Pachori, R.B.; Vijesh, A. Classification of ictal and seizure-free EEG signals using fractional linear prediction. Biomed. Signal Processing Control 2014, 9, 1–5. [Google Scholar] [CrossRef]
- Pathak, A.; Ramesh, A.; Mitra, A.; Majumdar, K. Automatic seizure detection by modified line length and Mahalanobis distance function. Biomed. Signal Processing Control 2018, 44, 279–287. [Google Scholar] [CrossRef]
- Jahankhani, P.; Revett, K.; Kodogiannis, V. Data mining an EEG dataset with an emphasis on dimensionality reduction. In Proceedings of the 2007 IEEE Symposium on Computational Intelligence and Data Mining, Honolulu, HI, USA, 1 March–5 April 2007; pp. 405–412. [Google Scholar]
- Kaleem, M.; Guergachi, A.; Krishnan, S. Patient-specific seizure detection in long-term EEG using wavelet decomposition. Biomed. Signal Processing Control 2018, 46, 157–165. [Google Scholar] [CrossRef]
- Pérez-Elvira, R.; Oltra-Cucarella, J.; Carrobles, J.A.; Teodoru, M.; Bacila, C.; Neamtu, B. Individual alpha peak frequency, an important biomarker for live z-score training neurofeedback in adolescents with learning disabilities. Brain Sci. 2021, 11, 167. [Google Scholar] [CrossRef]
- Tsipouras, M.G. Spectral information of EEG signals with respect to epilepsy classification. EURASIP J. Adv. Signal Processing 2019, 2019, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Truong, N.D.; Nguyen, A.D.; Kuhlmann, L.; Bonyadi, M.R.; Yang, J.; Ippolito, S.; Kavehei, O. Convolutional neural networks for seizure prediction using intracranial and scalp electroencephalogram. Neural Netw. 2018, 105, 104–111. [Google Scholar] [CrossRef] [Green Version]
- Ghosh-Dastidar, S.; Adeli, H.; Dadmehr, N. Mixed-band wavelet-chaos-neural network methodology for epilepsy and epileptic seizure detection. IEEE Trans. Biomed. Eng. 2007, 54, 1545–1551. [Google Scholar] [CrossRef] [PubMed]
- Vidyaratne, L.S.; Iftekharuddin, K.M. Real-time epileptic seizure detection using EEG. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 2146–2156. [Google Scholar] [CrossRef] [PubMed]
- Orosco, L.; Correa, A.G.; Diez, P.; Laciar, E. Patient non-specific algorithm for seizures detection in scalp EEG. Comput. Biol. Med. 2016, 71, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Chandel, G.; Upadhyaya, P.; Farooq, O.; Khan, Y. Detection of seizure event and its onset/offset using orthonormal triadic wavelet based features. IRBM 2019, 40, 103–112. [Google Scholar] [CrossRef]
- Li, Q.; Gao, J.; Huang, Q.; Wu, Y.; Xu, B. Distinguishing Epileptiform Discharges From Normal Electroencephalograms Using Scale-Dependent Lyapunov Exponent. Front. Bioeng. Biotechnol. 2020, 8, 1006. [Google Scholar] [CrossRef]
- Brari, Z.; Belghith, S. A novel Machine Learning approach for epilepsy diagnosis using EEG signals based on Correlation Dimension. IFAC-PapersOnLine 2021, 54, 7–11. [Google Scholar] [CrossRef]
- Polat, K.; Güneş, S. Classification of epileptiform EEG using a hybrid system based on decision tree classifier and fast Fourier transform. Appl. Math. Comput. 2007, 187, 1017–1026. [Google Scholar] [CrossRef]
- Arunkumar, N.; Ram Kumar, K.; Venkataraman, V. Automatic detection of epileptic seizures using permutation entropy, Tsallis entropy and Kolmogorov complexity. J. Med. Imaging Health Inform. 2016, 6, 526–531. [Google Scholar] [CrossRef]
- Nicolaou, N.; Georgiou, J. Detection of epileptic electroencephalogram based on permutation entropy and support vector machines. Expert Syst. Appl. 2012, 39, 202–209. [Google Scholar] [CrossRef]
- Li, K.; Zhang, X.; Du, Y. A SVM based classification of EEG for predicting the movement intent of human body. In Proceedings of the 2013 10th International Conference on Ubiquitous Robots and Ambient Intelligence (URAI), Jeju, Korea, 30 October–2 November 2013; pp. 402–406. [Google Scholar]
- Wang, S.; Chaovalitwongse, W.A.; Wong, S. Online seizure prediction using an adaptive learning approach. IEEE Trans. Knowl. Data Eng. 2013, 25, 2854–2866. [Google Scholar] [CrossRef]
- Wang, G.; Deng, Z.; Choi, K.-S. Detection of epileptic seizures in EEG signals with rule-based interpretation by random forest approach. In International Conference on Intelligent Computing; Springer: Berlin/Heidelberg, Germany, 2015; pp. 738–744. [Google Scholar]
- Hussein, R.; Palangi, H.; Ward, R.K.; Wang, Z.J. Optimized deep neural network architecture for robust detection of epileptic seizures using EEG signals. Clin. Neurophysiol. 2019, 130, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Yuan, S.; Xu, F.; Leng, Y.; Yuan, K.; Yuan, Q. Scalp EEG classification using deep Bi-LSTM network for seizure detection. Comput. Biol. Med. 2020, 124, 103919. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Zou, J.; Zhang, J.; Xu, J. Automatic epileptic EEG detection using convolutional neural network with improvements in time-domain. Biomed. Signal Processing Control 2019, 53, 101551. [Google Scholar] [CrossRef]
- Truong, N.D.; Kuhlmann, L.; Bonyadi, M.R.; Querlioz, D.; Zhou, L.; Kavehei, O. Epileptic seizure forecasting with generative adversarial networks. IEEE Access 2019, 7, 143999–144009. [Google Scholar] [CrossRef]
- Tsiouris, Κ.Μ.; Pezoulas, V.C.; Zervakis, M.; Konitsiotis, S.; Koutsouris, D.D.; Fotiadis, D.I. A long short-term memory deep learning network for the prediction of epileptic seizures using EEG signals. Comput. Biol. Med. 2018, 99, 24–37. [Google Scholar] [CrossRef]
- Ra, J.S.; Li, T.; Li, Y. A Novel Permutation Entropy-Based EEG Channel Selection for Improving Epileptic Seizure Prediction. Sensors 2021, 21, 7972. [Google Scholar] [CrossRef]
- Aung, S.T.; Wongsawat, Y. Prediction of epileptic seizures based on multivariate multiscale modified-distribution entropy. Peerj Comput. Sci. 2021, 7, e744. [Google Scholar] [CrossRef]
- Vaswani, A.; Shazeer, N.; Parmar, N.; Uszkoreit, J.; Jones, L.; Gomez, A.N.; Kaiser, Ł.; Polosukhin, I. Attention is all you need. Adv. Neural Inf. Processing Syst. 2017, 30, 5999–6009. [Google Scholar]
- Tao, Y.; Sun, T.; Muhamed, A.; Genc, S.; Jackson, D.; Arsanjani, A.; Yaddanapudi, S.; Li, L.; Kumar, P. Gated Transformer for Decoding Human Brain EEG Signals. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 125–130. [Google Scholar]
- Shoeb, A.H. Application of Machine Learning to Epileptic Seizure Onset Detection and Treatment; Massachusetts Institute of Technology: Cambridge, MA, USA, 2009. [Google Scholar]
- Kovacs, P.; Samiee, K.; Gabbouj, M. On application of rational discrete short time fourier transform in epileptic seizure classification. In Proceedings of the 2014 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Florence, Italy, 4–9 May 2014; pp. 5839–5843. [Google Scholar]
- Tsai, A.-C.; Luh, J.-J.; Lin, T.-T. A novel STFT-ranking feature of multi-channel EMG for motion pattern recognition. Expert Syst. Appl. 2015, 42, 3327–3341. [Google Scholar] [CrossRef]
- Chen, R.; Parhi, K.K. Seizure Prediction using Convolutional Neural Networks and Sequence Transformer Networks. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 6483–6486. [Google Scholar]
- Sun, B.A.; Lv, J.J.; Rui, L.G.; Yang, Y.X.; Chen, Y.G.; Ma, C.; Gao, Z.K. Seizure prediction in scalp EEG based channel attention dual-input convolutional neural network. Phys. A-Stat. Mech. Its Appl. 2021, 584, 126376. [Google Scholar] [CrossRef]
- Fourth International Workshop on Seizure Prediction. Available online: http://www.iwsp4.org/patients.htm (accessed on 5 April 2022).
- Nesaei, S.; Sharafat, A.R. Real-time mining of epileptic seizure precursors via nonlinear mapping and dissimilarity features. IET Signal Processing 2015, 9, 193–200. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, J.; Wu, H.; Zhu, J.; Sawan, M. Power efficient refined seizure prediction algorithm based on an enhanced benchmarking. Sci. Rep. 2021, 11, 23498. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Fields, M.; Panov, F.; Ghatan, S.; Yener, B.; Marcuse, L. Deep Learning of Simultaneous Intracranial and Scalp EEG for Prediction, Detection, and Lateralization of Mesial Temporal Lobe Seizures. Front. Neurol. 2021, 12, 705119. [Google Scholar] [CrossRef] [PubMed]
- Bandarabadi, M.; Rasekhi, J.; Teixeira, C.A.; Karami, M.R.; Dourado, A. On the proper selection of preictal period for seizure prediction. Epilepsy Behav. 2015, 46, 158–166. [Google Scholar] [CrossRef]
- Liu, M.; Ren, S.; Ma, S.; Jiao, J.; Chen, Y.; Wang, Z.; Song, W. Gated Transformer Networks for Multivariate Time Series Classification. arXiv 2021, arXiv:2103.14438. [Google Scholar]
- Rukhsar, S.; Khan, Y.; Farooq, O.; Sarfraz, M.; Khan, A. Patient-specific epileptic seizure prediction in long-term scalp EEG signal using multivariate statistical process control. IRBM 2019, 40, 320–331. [Google Scholar] [CrossRef]
- Xu, Y.; Yang, J.; Zhao, S.; Wu, H.; Sawan, M. An end-to-end deep learning approach for epileptic seizure prediction. In Proceedings of the 2020 2nd IEEE International Conference on Artificial Intelligence Circuits and Systems (AICAS), Genova, Italy, 31 August–2 September 2020; pp. 266–270. [Google Scholar]
- Tang, L.; Xie, N.; Zhao, M.; Wu, X. Seizure Prediction Using Multi-View Features and Improved Convolutional Gated Recurrent Network. IEEE Access 2020, 8, 172352–172361. [Google Scholar] [CrossRef]
- Zhao, S.; Yang, J.; Xu, Y.; Sawan, M. Binary single-dimensional convolutional neural network for seizure prediction. In Proceedings of the 2020 IEEE International Symposium on Circuits and Systems (ISCAS), Seville, Spain, 12–14 October 2020; pp. 1–5. [Google Scholar]
- Zhang, S.; Chen, D.; Ranjan, R.; Ke, H.; Tang, Y.; Zomaya, A.Y. A lightweight solution to epileptic seizure prediction based on EEG synchronization measurement. J. Supercomput. 2021, 77, 3914–3932. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Gender | Age (Years) | Number of Channels | Number of Seizures |
|---|---|---|---|---|
| Chb01 | F | 11 | 23 | 7 |
| Chb02 | M | 11 | 23 | 3 |
| Chb03 | F | 14 | 23 | 7 |
| Chb04 | M | 22 | 23 | 4 |
| Chb05 | F | 7 | 23 | 5 |
| Chb06 | F | 1.5 | 23 | 10 |
| Chb07 | F | 14.5 | 23 | 3 |
| Chb08 | M | 3.5 | 23 | 5 |
| Chb09 | F | 10 | 23 | 4 |
| Chb10 | M | 3 | 23 | 7 |
| Chb11 | F | 12 | 23 | 3 |
| Chb12 | F | 2 | 18 | 40 |
| Chb13 | F | 3 | 23 | 12 |
| Chb14 | F | 9 | 18 | 8 |
| Chb15 | M | 16 | 18 | 20 |
| Chb16 | F | 7 | 18 | 10 |
| Chb17 | F | 12 | 18 | 3 |
| Chb18 | F | 18 | 18 | 6 |
| Chb19 | F | 19 | 23 | 3 |
| Chb20 | F | 6 | 23 | 8 |
| Chb21 | F | 13 | 23 | 4 |
| Chb22 | F | 9 | 23 | 3 |
| Chb23 | F | 6 | 23 | 7 |
| Chb24 | - | - | 23 | 16 |
| Preictal | Interictal | |
|---|---|---|
| Subject No. | 21 | 21 |
| No. of channels | 18 | 18 |
| No. of spectrograms | 312,552 | 329,437 |
| Patient | No. of Seizures | GTN 1 | Our Model | ||||
|---|---|---|---|---|---|---|---|
| Sen 2 (%) | Spec 3 (%) | Pre 4 (%) | Sen 2 (%) | Spec 3 (%) | Pre 4 (%) | ||
| Chb01 | 7 | 98.62 | 98.99 | 98.96 | 100 | 99.88 | 99.9 |
| Chb02 | 3 | 92.61 | 94.56 | 94.49 | 96.88 | 98.64 | 98.58 |
| Chb03 | 7 | 90.65 | 91.01 | 89.87 | 97.82 | 96.87 | 94.31 |
| Chb04 | 4 | 91.25 | 87.94 | 88.28 | 93.53 | 92.15 | 92.23 |
| Chb05 | 5 | 92.34 | 90.40 | 90.6 | 94 | 99.45 | 98.95 |
| Chb06 | 10 | 91.26 | 87.93 | 88.29 | 93.51 | 92.1 | 92.18 |
| Chb07 | 3 | 89.04 | 93.99 | 93.73 | 99.11 | 97.12 | 97.2 |
| Chb08 | 5 | 94.44 | 91.72 | 91.89 | 97.22 | 95.86 | 95.89 |
| Chb09 | 4 | 87.59 | 92 | 91.71 | 94.53 | 97.15 | 97.1 |
| Chb10 | 7 | 95.65 | 90.33 | 90.53 | 96.48 | 98.2 | 98.11 |
| Chb11 | 3 | 89.5 | 86.25 | 81.14 | 97.48 | 96.39 | 94.69 |
| Chb14 | 6 | 98.59 | 97.88 | 97.89 | 99.29 | 99.65 | 99.65 |
| Chb15 | 13 | 91.60 | 88.87 | 86.67 | 93.22 | 97.43 | 96.63 |
| Chb16 | 5 | 85.85 | 88 | 87.74 | 89.85 | 92.31 | 92.11 |
| Chb17 | 3 | 93.19 | 95.12 | 95.04 | 98.54 | 97.24 | 97.28 |
| Chb18 | 5 | 94.25 | 96.06 | 95.35 | 98.24 | 99.67 | 99.61 |
| Chb19 | 3 | 93.56 | 91.59 | 89.05 | 95.56 | 94.21 | 92.35 |
| Chb20 | 6 | 95.20 | 94.58 | 94.43 | 98.64 | 97.55 | 97.49 |
| Chb21 | 4 | 89.58 | 88.63 | 88.81 | 93.50 | 91.55 | 91.77 |
| Chb22 | 3 | 91.20 | 91.21 | 90.35 | 95.53 | 96.21 | 95.79 |
| Chb23 | 5 | 88.25 | 89.01 | 88.81 | 93.33 | 91.21 | 91.29 |
| Average | - | 92.11 | 91.72 | 91.12 | 96.01 | 96.23 | 95.86 |
| Patient | No. of Seizures | Without Post-Processing | After Post-Processing |
|---|---|---|---|
| FPR 1 (h−1) | FPR 1 (h−1) | ||
| Chb01 | 7 | 0 | 0 |
| Chb02 | 3 | 0.07 | 0.01 |
| Chb03 | 7 | 0.3 | 0.07 |
| Chb04 | 4 | 0.9 | 0.22 |
| Chb05 | 5 | 0.02 | 0 |
| Chb06 | 10 | 0.52 | 0.13 |
| Chb07 | 3 | 0.3 | 0.07 |
| Chb08 | 5 | 0.02 | 0 |
| Chb09 | 4 | 0.3 | 0.08 |
| Chb10 | 7 | 0.1 | 0.02 |
| Chb11 | 3 | 0.1 | 0.02 |
| Chb14 | 6 | 0 | 0 |
| Chb15 | 13 | 0.05 | 0 |
| Chb16 | 5 | 0.1 | 0.03 |
| Chb17 | 3 | 0.07 | 0.02 |
| Chb18 | 5 | 0.02 | 0 |
| Chb19 | 3 | 0.3 | 0.08 |
| Chb20 | 6 | 0.1 | 0.03 |
| Chb21 | 4 | 0.45 | 0.11 |
| Chb22 | 3 | 0.1 | 0.03 |
| Chb23 | 5 | 0.3 | 0.07 |
| Average | - | 0.19 | 0.047 |
| Year | Authors | Feature | Classifier | No. of Patients | No. of Seizures | Sen 1 (%) | FPR (h−1) | SPH |
|---|---|---|---|---|---|---|---|---|
| 2018 | Truong | STFT | CNN | 13 | 64 | 81.2 | 0.16 | 5 min |
| 2019 | Rukhsar | Eight temporal-based features | MSPC | 10 | 90 | 88.89 | 0.39 | - |
| 2020 | Xu | - | CNN | 7 | 45 | 98.8 | 0.074 | 5 min |
| 2020 | Tang | L-DFA, relative band energy, synchronization modularity | Mv-CGRNi | 24 | 140 | 94.5 | 0.118 | - |
| 2020 | Zhao | - | BSDCNN | 6 | - | 94.69 | 0.095 | 5 min |
| 2021 | Zhang | Pearson correlation coefficient matrices. | CNN | 19 | - | 92.9 | - | 15 min |
| - | This work | STFT | Three tower transformer | 21 | 111 | 96.01 | 0.047 | 3 min |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, J.; Li, J.; Xu, H.; Yu, Y.; Xu, T. Seizure Prediction Based on Transformer Using Scalp Electroencephalogram. Appl. Sci. 2022, 12, 4158. https://doi.org/10.3390/app12094158
Yan J, Li J, Xu H, Yu Y, Xu T. Seizure Prediction Based on Transformer Using Scalp Electroencephalogram. Applied Sciences. 2022; 12(9):4158. https://doi.org/10.3390/app12094158
Chicago/Turabian StyleYan, Jianzhuo, Jinnan Li, Hongxia Xu, Yongchuan Yu, and Tianyu Xu. 2022. "Seizure Prediction Based on Transformer Using Scalp Electroencephalogram" Applied Sciences 12, no. 9: 4158. https://doi.org/10.3390/app12094158