1. Introduction
The share of the automobile industry in view of the overall size of the national economy varies across countries. The automobile industry accounts for a large portion of output in the large automobile-producing countries such as Germany, Japan, and the Republic of Korea [
1].
In Korea, the automobile sector is a key industry that occupies a very large proportion of production, employment, and exports in the national economy. Moreover, there are many related up and downstream industries for the automobile industry from raw materials, equipment, dealers, and services, so the influence of the automobile industry on the entire economy is great.
In Korea, the manufacture of motor vehicles, trailers, and semitrailers employed 359,831 persons in 2019, which accounts for 1.58% of the total employment that year [
2]. However, in the U.S., the manufacture of motor vehicles, trailers and semitrailers employed 839,550 persons, which accounts for 0.60% of the total employment in 2020 [
3].
Among automobile manufacturing industries, the largest sector is the manufacture of parts and accessories for motor vehicles (new products), accounting for 72.4% of the overall automobile manufacturing industry employment [
2]. The manufacture of motor vehicles and engines for the motor vehicle sector (23.8%) follows.
Working conditions for the industry have improved along with the automation, mechanical material handling, and the enclosure of working stations. However, production workers in the automobile industry are still exposed to a wide range of risk factors. ILO [
4] addressed the hazards in motor vehicle manufacturing processes: Chemical and physical hazards in foundry processes include silica-containing dust, carbon monoxide, metal fumes, noise, vibration, and heat. Exposure to vapors from the acid plating baths is involved in the electroplating process. Exposure to noise, oil smoke, and heat are hazards in forging and heat treatment. Foreign body injuries, coolant mist, airborne toxic substances, metal dust, ergonomic risk, and noise are common hazards in the machining process. Ergonomic risks, exposure to visible and ultraviolet radiation from welding, welding fumes, noise, and solvent vapor are included in vehicle assembly.
Manual handling of heavy parts and operation of dangerous power tools or high-speed machines are still prevalent [
5,
6,
7]. Also, the incidence of musculoskeletal disorders (MSDs) is high in the automobile manufacturing industry [
8,
9,
10]. In Korea in 2019, of the 9440 workers who suffered work-related musculoskeletal disorders (WMSDs), 1658 (17.56%) occurred in the machine tools, non-metallic and metal product manufacturing sector, which includes the automobile industry [
11]. Typical physical hazards in automobile assembly work include repeatability due to a short work cycle time of less than 1 min, uncomfortable posture, and vibration caused by excessive force and power tools. These harmful factors are the main causes of work-related musculoskeletal disorders (WMSDs) [
12]. Most of the auto parts manufacturing workers work while standing and complain of shoulder, leg, and back pain due to simple repetitive work that requires physical strength and endurance and handicraft [
13].
Subjective symptoms of body parts have been the focus of previous studies [
8,
9,
10,
14,
15,
16]. Kang et al. [
17] investigated WMSDs in automobile assembly workers and found that ergonomic and management factors are risk factors for occupational WMSDs. Jamdade et al. [
18,
19] studied the relationship between low back pain and various factors like core muscle strength, work posture, and flexibility of the workers. Akter et al. [
20] found that, among automobile mechanics, musculoskeletal symptoms are prevalent and are associated with physical risk factors. Alipour et al. [
21] showed that neck and shoulder pain are prevalent and are associated with lifestyle, work-related physical factors, and psychosocial factors.
Most of the prior studies on WMSDs in the automobile industry restrict the research scope to the specific plant or specific company and some of the working environmental factors, which leads to the lack of industry-wide interpretation and implication or the lack of the overall effect of the working conditions.
Therefore, this study aims to investigate the relationships between personal characteristics or occupational hazard (physical, chemical, and ergonomic) exposure and subjective overall fatigue or musculoskeletal pain in the automobile manufacturing industry based on a nation-wide working condition survey.
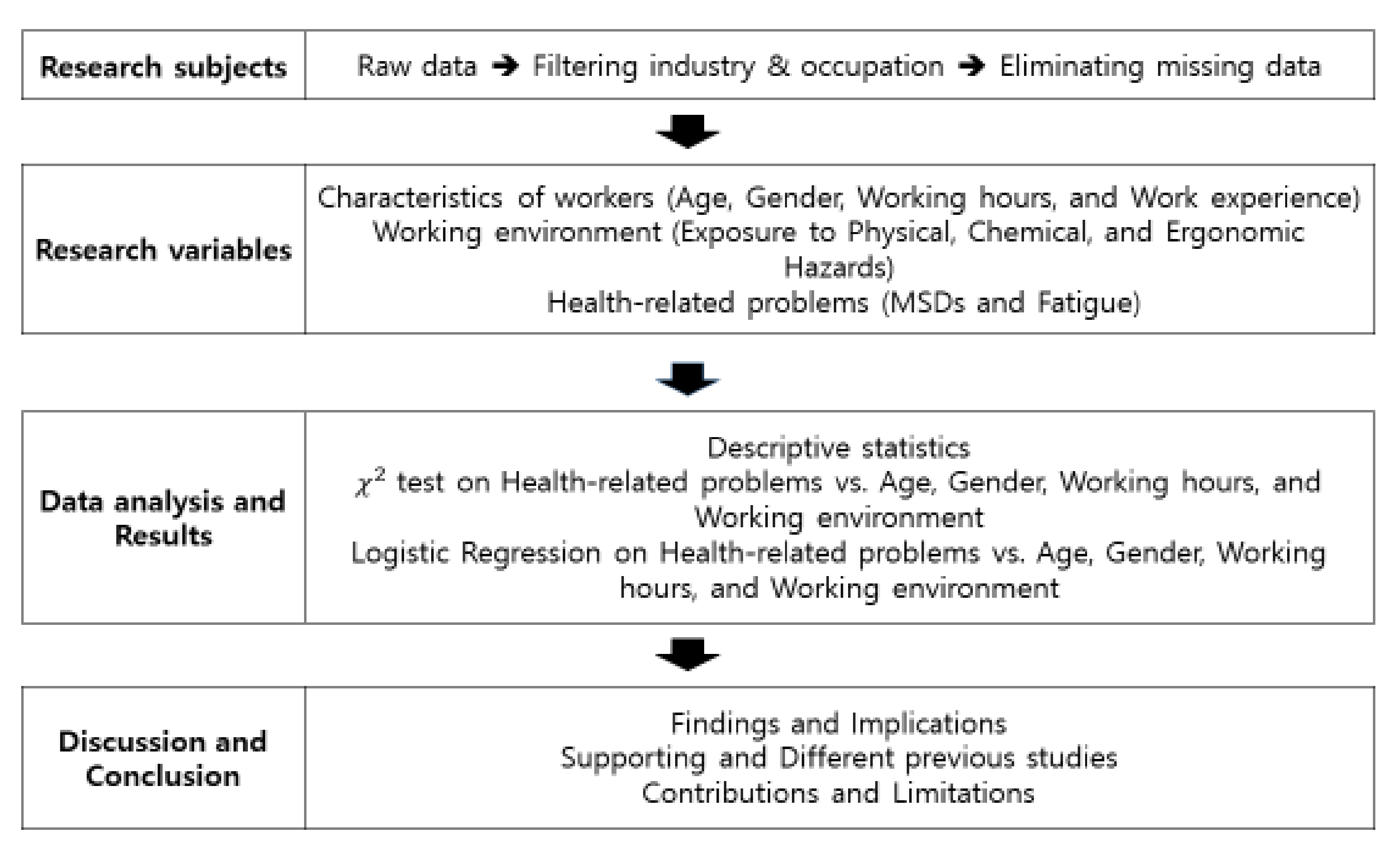
2. Materials and Methods
The extraction of research subjects, the selection of research variables, data analysis, results, discussion on the findings, and conclusive remarks are summarized in
Figure 1.
2.1. Data Collection
The raw data of the 5th Korean Working Conditions Survey (KWCS) [
22], which was open to the public to promote secondary analysis, was used for this study. The KWCS is the Korean version of the European Working Conditions Survey (EWCS) [
23]. The KWCS is a periodic national survey that is designed to investigate risk factors and working conditions of workers by industry and occupation [
22]. The KWCS was conducted by professional interviewers [
22]. The response rate of the 5th KWCS was 0.449, and 50,205 workers in proportion to each region’s population participated. According to the Korean Standard Industrial Classification (KSIC) [
24], we extracted automobile manufacturing workers (workers in “manufacture of motor vehicles and engines for motor vehicles” and in “manufacture of parts and accessories for motor vehicles (new products)”) in the production process and filtered 446 production workers as subjects. They consisted of 15.5% under 29 years, 23.3% in their 30s, 26.5% in their 40s, and 34.8% aged 50 or older. The mean of work experience is 9.85 years. The mean of monthly wage is 3.74 million South Korean Won (KRW). The mean of working hours per week was 44.14 h.
2.2. Research Variables
Table 1 shows the research variables of this study. The research variables consisted of the characteristics of workers, working environments, and the health-related problems from the KWCS questionnaire [
22].
Table 1 presents the research variables, descriptions (or questions), and scores observed. Worker characteristics consisted of age, gender, work experience, and working hours per week. Most workers begin their career in their early 20s (female) or mid 20s (male) and retire in their late 50s or early 60s in Korea. Accordingly, the age groups of workers were classified into the following categories: under 29, the 30s, the 40s, and 50 or older. The voluntary turnover rate for those with early careers peaks one to two years after joining the company and shows relatively high value until 5 years, and then tends to decrease [
25]. Taking this into consideration, the duration of work experience was classified into less than three years, three to five years, and longer than five years.
Working environment characteristics consisted of exposure to physical and mechanical hazards, ergonomic hazards, and chemical and biological hazards. Exposure to hazards was measured by the adjusted daily hazard exposure time (ADHE). ADHE was assessed on a daily basis by dividing working hours per week by working days per week and then multiplying the frequency of hazard exposures. The frequency of hazard exposure is answered by the questionnaire asking about the proportion of working time exposed to a sort of hazard with seven possible answers (“all of the time”, “almost all of the time”, “around 3/4 of the time”, “around half of the time”, “around 1/4 of the time”, “almost never”, and “never”). The frequency of hazard exposure is as follows: 0.75 for “all of the time”, “almost all of the time”, and “around 3/4 of the time”; 0.5 for “around half of the time”; 0.25 for “around 1/4 of the time”; 0.1 for “almost never” and “never”). Physical or mechanical hazards (exposure to vibration, noise, high and low temperature), chemical and biological hazards (exposure to fumes, and dust, vapor, skin contact, tobacco smoke, infection), and ergonomic hazards (exposure to awkward posture, handling of heavy objects, standing posture, and repetitive motion) comprised the characteristics of the working environment.
Health-related problems are complaints of musculoskeletal pain (backache, upper limb pain, lower limb pain, and any pain (pain complaints in any one of back, upper limb, and lower limb)) and complaints of overall fatigue. Musculoskeletal pain complaints or overall fatigue were answered in response to the question “Over the last 12 months, did you have any of the following health problems due to your job?” with the answer “yes” or “no”.
2.3. Data Analysis
The descriptive statistics for the degree of exposure to physical, ergonomic, and chemical/biological hazards of the respondents are given.
In addition, the χ2 test was done to test whether there is a difference in the distribution of complaints of musculoskeletal pain and the overall fatigue in view of age group, gender, work experience, working hours per week, and ADHE of working environment hazards.
Odds ratios (OR) and 95% confidence intervals (95% CI) for complaints of musculoskeletal pain and overall fatigue according to age, gender, work experience, working hours per week, and working environment hazards were estimated using a logistic regression model. The Hosmer-Lemeshow test (HL test) for goodness of fit test is used for logistic regression and the Nagelkerke’s R squared is used for the power of explanation of the model. The overall classification accuracy rate to assess the performance of a model is also provided.
The statistical package used for statistical analysis was SPSS 18.0, and the significance level was 0.05.
4. Discussion
In this study, the characteristics of workers, working environments, and work-related health problems were analyzed for production workers in the automobile manufacturing industry.
As for health problems, the complaint rate for backache was the lowest. This is consistent with the trend that among musculoskeletal diseases, the number of patients with low back pain caused by excessive force such as handling heavy objects is gradually decreasing, but the number of patients suffering from physical burdens such as repetitive motions and awkward posture increases every year in Korea [
26].
The complaints of some work-related health problems were different by age, gender, and working hours per week. The complaint rate of upper limb pain increases to the highest for those in their 40s (26.3%). Musculoskeletal disorders are health disorders that occur in workers who are engaged in long-term work that repeatedly burdens the body. It is more likely to occur in older workers than in younger workers since aging leads to a decrease in bone mass and in bone density due to changes in the musculoskeletal system [
27,
28,
29,
30]. Upper limb pain (32.5%) and overall fatigue (30.1%) were higher for females. This is consistent with the review article showing that females had significantly higher incidences of various types of upper extremity musculoskeletal disorders [
31]. The gender difference can be attributed to the fact that the females are more comfortable reporting discomfort than men, or that women report more illnesses than men [
32,
33,
34,
35]. Upper limb pain (27.6%), pain complaints in any one area (33.3%), and overall fatigue (27.6%) were higher for those who work longer than 41 h per week. It was consistent with the results showing that the risk of musculoskeletal symptoms increases because the musculoskeletal system’s opportunity to rest and recover decreases with prolonged physical load duration through prolonged work [
36,
37,
38].
The proportions of the overall fatigue and MSDs complaining group increase as the hazard exposure time increases, as was expected. It was consistent with the results showing hazards in the work process such as repetitive use of specific body parts, excessive force, a cold work environment, vibration, and chronic exposure to awkward postures that results in MSDs [
39,
40,
41,
42,
43].
Exposure to chemical and biological hazards is the major source of overall fatigue. Longer exposure to tobacco smoke shows the highest rate of complaining of overall fatigue, upper limb pain, and pain in any area. It was consistent with the results that show that the high fatigue group were more likely to claim regular exposure to second-hand cigarette smoke than the low fatigue group [
44]. Lee et al. [
45] discuss the effect of the second-hand smoke relating to fatigue, sleep disorders, and decreased physical and mental functioning. Exposure to second-hand tobacco smoke is associated with reduced muscle strength [
46] and leads to increased respiratory symptoms and reduction of pulmonary function [
47]. Respiratory symptoms can induce disc herniation through coughing or cause pathological changes in the intervertebral disc [
48]. Longer exposures to infectious material shows the highest complaining rate of backache. As for infections in the automobile manufacturing industry, there is little chance of handling or being in direct contact with bodily fluids, laboratory materials, etc. Handling the waste from production processes may be considered to be exposure to infectious material. Wearing protection gear when handling the waste could cause MSDs.
The results of logistic regression on overall fatigue show that gender, exposure to fumes and dust, to manual heavy load handling, and to repetitive motion were the risk factors for overall fatigue. Complaints of overall fatigue among females was more likely than for males. Complaints of overall fatigue among those who have long exposure to fumes and dust and to manual heavy loads handling was more likely than those who have less exposure. Guo et al. [
49] state that work-related fatigue is significantly correlated with the working environment and the duration of the working day.
Results of logistic regression on MSDs show that longer exposure to noise and awkward posture was the risk factor for backache. Noise is the source of MSDs, but previous studies do not support the association between noise and backache. Preceding studies support the strong association between noise and head and neck pain [
43,
50,
51,
52]. Basner et al. [
51] state that noise can lead to stress and stress-related responses and Evans and Johnson [
50] state that a link between stress exposure and MSDs may result from the effects of noise. Magnavita et al. [
43] show the association between upper limb disorders and noise and light complaints.
Complaints of upper limb pain among females, those with longer work experience, and those with longer exposure to fumes and dust were more likely. Complaints of lower limb pain among those who have long exposure to fumes and dust was more likely than those who have less exposure. In the automobile industry, fumes and dust are found in foundry processes, casting, heat treatment, machining, welding, plastic works, and vehicle assembly [
4]. The exact mechanism through which exposure to fumes and dust at work relates to musculoskeletal pains is not known. Previous studies on the respiratory syndrome in the automobile manufacturing process indicate that exposure to metal dust, welding fumes, and metalworking fluids contribute to the increase of respiratory syndromes such as asthma [
53,
54,
55]. Lunardi et al. [
56] state that adults with persistent asthma develop chronic alterations in posture and have musculoskeletal problems irrespective of the severity of their disease. Wearing protection gear could affect fatigue and potentially pain responses. Workers should wear respirators, eye and face protection, hand and arm protection, and oil-resistant aprons if necessary [
4]. Wearing respirators makes it uncomfortable to breathe and leads to fatigue [
57,
58]. It is also recognized that working in dirty environments is a psychosocial risk factor and that psychosocial stressors are related to MSDs [
59,
60].
The results of logistic regression on pain complaints in any one area show that gender, work experience, working hours per week, and exposure to high temperature were the risk factors for upper limb pain. Magnavita et al. [
43] show that the association between upper limb disorders and temperature complaints, including both too high and too low temperature.
5. Conclusions and Limitations of the Study
This study has limitations. First, the KWCS data based on a questionnaire is used in this study. All of the information on exposure to working environment hazards and work-related health problems was self-reported. Second, the factors considered in this study are the work environment characteristics, but there are also personal and socio-psychological characteristics to be considered [
61]. Drinking, exercise, hobbies, housework, and personal medical history were considered to be personal factors. In addition, low job satisfaction and lack of social support from colleagues and superiors are considered to be influential as socio-psychological factors [
6,
41]. In terms of further studies, the implementation of safety culture analyses including psychological and communication factors will contribute to the safety and health of automobile manufacturing workers.
This study derives factors affecting the overall fatigue and musculoskeletal pain of production workers in the automobile manufacturing industry. Furthermore, it is considered to be meaningful as basic data for systematic prevention measures and can serve as an educational guide on overall fatigue and musculoskeletal pain.
In spite of the many improvements in the working environment for the automobile manufacturing industry, more efforts should be made to reduce the exposure to working environment hazards for production workers. It is recommended that a working environment with enclosed workstations be developed, in order to address the sources of noise, fumes and dust, and uncomfortable temperature, with appropriate ventilation for smoke or fumes and dust and vapor, with light weight personal protection gear for noise, fumes and dust, and vapor, and with devices to reduce ergonomic discomfort. Furthermore, measures considering the type of hazard exposures for each production process are to be prepared to secure safety and health for the production workers in the automobile manufacturing industry.







{kind=link}