
Strength, Flexibility and Postural Control of the Trunk and Lower Body in Participants with and without Patellofemoral Pain


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
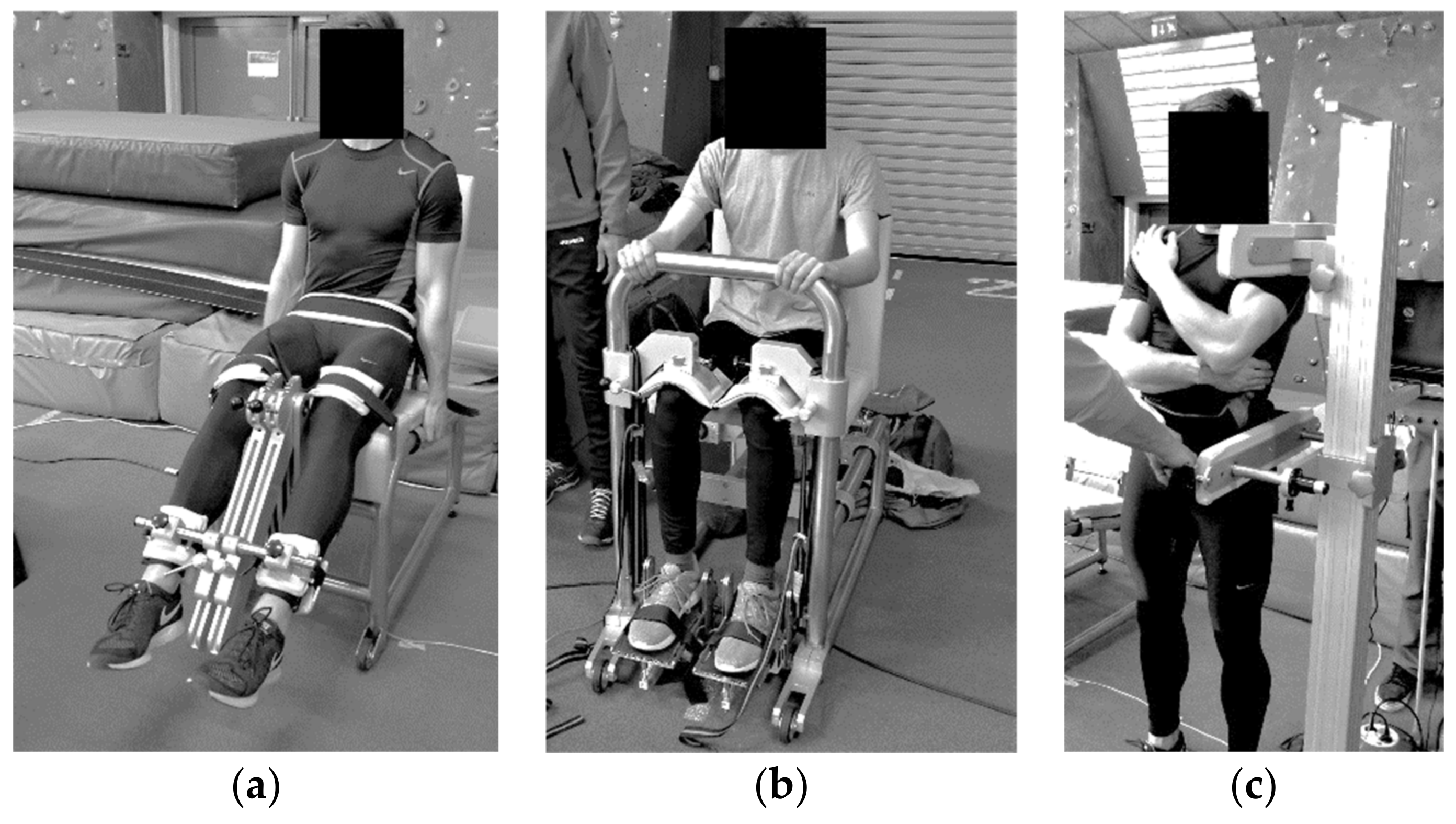
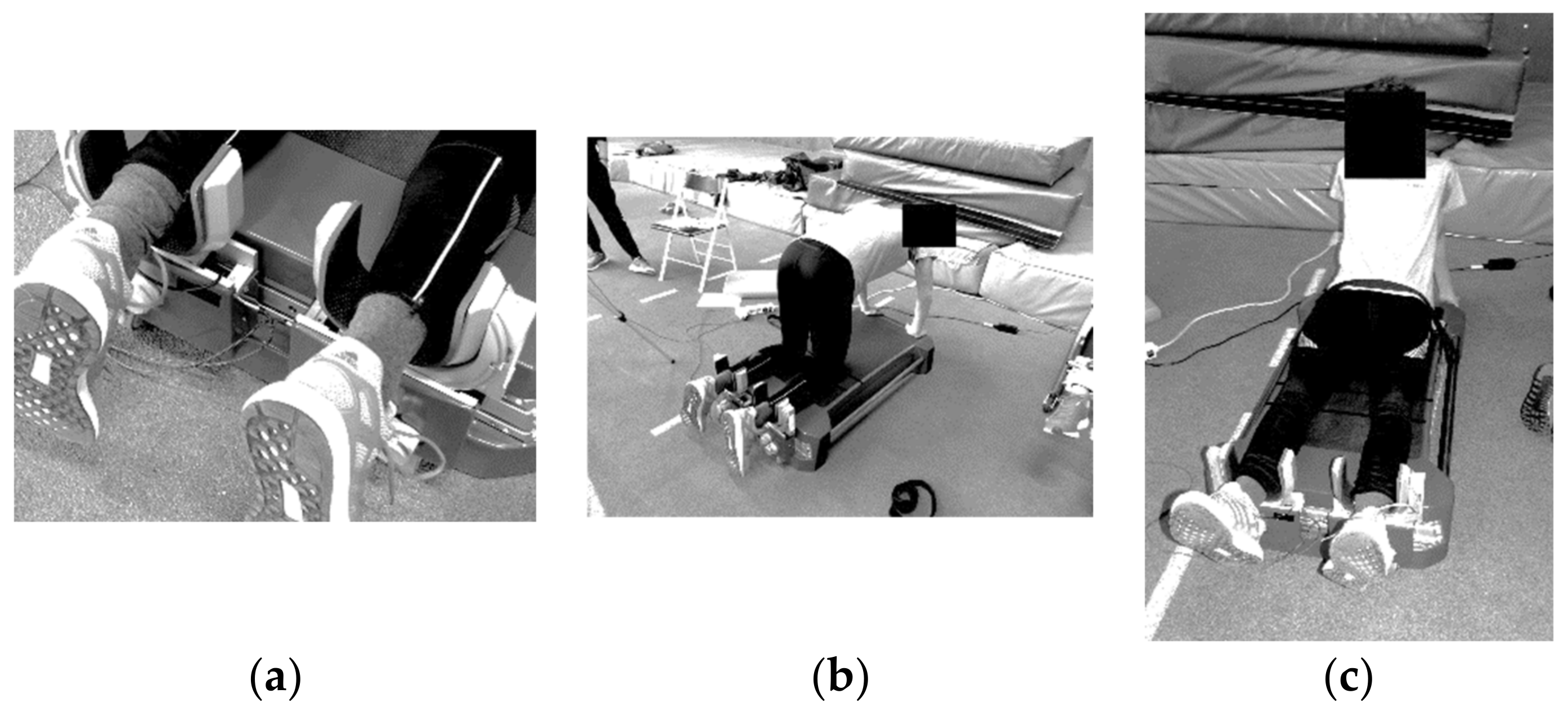
2.2. Study Design, Tasks and Measurement Procedure
2.3. Statistical Analysis
3. Results
3.1. Within-Group Differences
3.2. Between-Groups Differences
3.3. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smith, B.E.; Selfe, J.; Thacker, D.; Hendrick, P.; Bateman, M.; Moffatt, F.; Rathleff, M.S.; Smith, T.O.; Logan, P. Incidence and prevalence of patellofemoral pain: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0190892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crossley, K.M.; Stefanik, J.J.; Selfe, J.; Collins, N.J.; Davis, I.S.; Powers, C.M.; McConnell, J.; Vicenzino, B.; Bazett-Jones, D.M.; Esculier, J.F.; et al. 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 1: Terminology, definitions, clinical examination, natural history, patellofemoral osteoarthritis and patient-reported outcome measures. Br. J. Sports Med. 2016, 50, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Lankhorst, N.E.; Bierma-Zeinstra, S.M.A.; Van Middelkoop, M. Risk factors for patellofemoral pain syndrome: A systematic review. J. Orthop. Sports Phys. Ther. 2012, 42, 81–94. [Google Scholar] [CrossRef]
- Farrokhi, S.; Keyak, J.H.; Powers, C.M. Individuals with patellofemoral pain exhibit greater patellofemoral joint stress: A finite element analysis study. Osteoarthr. Cartil. 2011, 19, 287–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brechter, J.H.; Powers, C.M. Patellofemoral stress during walking in persons with and without patellofemoral pain. Med. Sci. Sports Exerc. 2002, 34, 1582–1593. [Google Scholar] [CrossRef] [PubMed]
- Magalhães, E.; Fukuda, T.Y.; Sacramento, S.N.; Forgas, A.; Cohen, M.; Abdalla, R.J. A comparison of hip strength between sedentary females with and without patellofemoral pain syndrome. J. Orthop. Sports Phys. Ther. 2010, 40, 641–647. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, T.H.; Maciel, C.D.; Serrão, F.V. Trunk biomechanics and its association with hip and knee kinematics in patients with and without patellofemoral pain. Man. Ther. 2015, 20, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Ireland, M.L.; Willson, J.D.; Ballantyne, B.T.; Davis, I.M.C. Hip Strength in Females with and without Patellofemoral Pain. J. Orthop. Sports Phys. Ther. 2003, 33, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Willson, J.D.; Ellis, E.D.; Kernozek, T.W. Plantar loading characteristics during walking in females with and without patellofemoral pain. J. Am. Podiatr. Med. Assoc. 2015, 105, 1–7. [Google Scholar] [CrossRef]
- Leetun, D.T.; Ireland, M.L.; Willson, J.D.; Ballantyne, B.T.; Davis, I.M.C. Core stability measures as risk factors for lower extremity injury in athletes. Med. Sci. Sports Exerc. 2004, 36, 926–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yelvar, G.D.Y.; Çirak, Y.; Dalkilinç, M.; Demir, Y.P.; Baltaci, G.; Kömürcü, M. Impairments of postural stability, core endurance, fall index and functional mobility skills in patients with patello femoral pain syndrome. J. Back Musculoskelet. Rehabil. 2017, 30, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Powers, C.M. The influence of abnormal hip mechanics on knee injury: A biomechanical perspective. J. Orthop. Sports Phys. Ther. 2010, 40, 42–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cowan, S.M.; Crossley, K.M.; Bennell, K.L. Altered hip and trunk muscle function in individuals with patellofemoral pain. Br. J. Sports Med. 2009, 43, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Almeida, G.P.L.; De Moura Campos Carvalho e Silva, A.P.; França, F.J.R.; Magalhães, M.O.; Burke, T.N.; Marques, A.P. Relationship between frontal plane projection angle of the knee and hip and trunk strength in women with and without patellofemoral pain. J. Back Musculoskelet. Rehabil. 2016, 29, 259–266. [Google Scholar] [CrossRef]
- Powers, C.M.; Witvrouw, E.; Davis, I.S.; Crossley, K.M. Evidence-based framework for a pathomechanical model of patellofemoral pain: 2017 patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester, UK: Part 3. Br. J. Sports Med. 2017, 51, 1713–1723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, C.J.; Lack, S.; Hemmings, S.; Tufail, S.; Morrissey, D. The “Best Practice Guide to Conservative Management of Patellofemoral Pain”: Incorporating level 1 evidence with expert clinical reasoning. Br. J. Sports Med. 2015, 923–934. [Google Scholar] [CrossRef] [PubMed]
- Boling, M.; Padua, D.; Marshall, S.; Guskiewicz, K.; Pyne, S.; Beutler, A. A prospective investigation of biomechanical risk factors for patellofemoral pain syndrome. The joint undertaking to monitor and prevent ACL injury (JUMP-ACL) cohort. Am. J. Sports Med. 2009, 37, 2108. [Google Scholar] [CrossRef] [Green Version]
- Barton, C.J.; Bonanno, D.; Levinger, P.; Menz, H.B. Foot and ankle characteristics in patellofemoral pain syndrome: A case control and reliability study. J. Orthop. Sports Phys. Ther. 2010, 40, 286–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalho, A.P.D.M.C. Comparison of isometric ankle strength between females with and without patellofemoral pain syndrome. Int. J. Sports Phys. Ther. 2014, 9, 628–634. [Google Scholar]
- Boling, M.C.; Nguyen, A.D.; Padua, D.A.; Cameron, K.L.; Beutler, A.; Marshall, S.W. Gender-Specific Risk Factor Profiles for Patellofemoral Pain. Clin. J. Sport Med. 2021, 31, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Martins Kalytczak, M.; Roberto Garcia Lucareli, P.; Curcio dos Reis, A.; Serra Bley, A.; Aparecida Biasotto-Gonzalez, D.; Carlos Ferrari Correa, J.; Politti, F. Kinematic and electromyographic analysis in patients with patellofemoral pain syndrome during single leg triple hop test. Gait Posture 2016, 49, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.S.; Lack, S.D.; Lankhorst, N.E.; Raye, A.; Morrissey, D.; Van Middelkoop, M. Risk factors for patellofemoral pain: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 270–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathleff, C.R.; Neill Baird, W.; Olesen, J.L.; Roos, E.M.; Rasmussen, S.; Rathleff, M.S. Hip and Knee Strength Is Not Affected in 12–16 Year Old Adolescents with Patellofemoral Pain-A Cross-Sectional Population-Based Study. PLoS ONE 2013, 8, e79153. [Google Scholar] [CrossRef] [Green Version]
- Morishige, Y.; Harato, K.; Kobayashi, S.; Niki, Y.; Matsumoto, M.; Nakamura, M.; Nagura, T. Difference in leg asymmetry between female collegiate athletes and recreational athletes during drop vertical jump. J. Orthop. Surg. Res. 2019, 14, 424. [Google Scholar] [CrossRef] [PubMed]
- Dolak, K.L.; Silkman, C.; Mckeon, J.M.; Hosey, R.G.; Lattermann, C.; Uhl, T.L. Hip strengthening prior to functional exercises reduces pain sooner than quadriceps strengthening in females with patellofemoral pain syndrome: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2011, 41, 560–570. [Google Scholar] [CrossRef] [Green Version]
- Vambergue, A.; Vantyghem, M.C.; Leclerc, L.; Hober, C.; Fourrier, F. Syndrome De Wiedemann-Beckwith Infantile, Avec Hypoglycemie Maternelle Severe, Steatose Hepatique Aigue Gravidique Et Syndrome De Sheehan. Rev. Fr. Endocrinol. Clin. Nutr. Metab. 1994, 35, 69–76. [Google Scholar] [CrossRef]
- Nakagawa, T.H.; Moriya, E.T.U.; MacIel, C.D.; Serrão, F.V. Trunk, pelvis, hip, and knee kinematics, hip strength, and gluteal muscle activation during a single-leg squat in males and females with and without patellofemoral pain syndrome. J. Orthop. Sports Phys. Ther. 2012, 42, 491–501. [Google Scholar] [CrossRef] [Green Version]
- Eslami, M.; Damavandi, M.; Ferber, R. Association of navicular drop and selected lower-limb biomechanical measures during the stance phase of running. J. Appl. Biomech. 2014, 30, 250–254. [Google Scholar] [CrossRef]
- Aenumulapalli, A.; Kulkarni, M.M.; Gandotra, A.R. Prevalence of flexible flat foot in adults: A cross-sectional study. J. Clin. Diagn. Res. 2017, 11, AC17–AC20. [Google Scholar] [CrossRef]
- Biedert, R.M.; Tscholl, P.M. Patella Alta: A Comprehensive Review of Current Knowledge. Am. J. Orthop. 2017, 46, 290–300. [Google Scholar]
- Ismail, M.M.; Gamaleldein, M.H.; Hassa, K.A. Closed Kinetic Chain exercises with or without additional hip strengthening exercises in management of Patellofemoral pain syndrome: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2013, 49, 687–698. [Google Scholar] [PubMed]
- Kozinc, Ž.; Trajković, N.; Smajla, D.; Šarabon, N. The Effect of Fatigue on Single-Leg Postural Sway and Its Transient Characteristics in Healthy Young Adults. Front. Physiol. 2021, 12, 720905. [Google Scholar] [CrossRef] [PubMed]
- Kozinc, Ž.; Smajla, D.; Šarabon, N. Relationship between hip abductor strength, rate of torque development scaling factor and medio-lateral stability in older adults. Gait Posture 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Smajla, D.; Žitnik, J.; Šarabon, N. Advancements in the Protocol for Rate of Force Development/Relaxation Scaling Factor Evaluation. Front. Hum. Neurosci. 2021, 15, 159. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Aagaard, P.; Blazevich, A.J.; Folland, J.; Tillin, N.; Duchateau, J. Rate of force development: Physiological and methodological considerations. Eur. J. Appl. Physiol. 2016, 116, 1091. [Google Scholar] [CrossRef] [Green Version]
- Meyer, C.; Corten, K.; Wesseling, M.; Peers, K.; Simon, J.-P.; Jonkers, I.; Desloovere, K. Test-Retest Reliability of Innovated Strength Tests for Hip Muscles. PLoS ONE 2013, 8, 81149. [Google Scholar] [CrossRef] [Green Version]
- Narouei, S.; Imai, A.; Akuzawa, H.; Hasebe, K.; Kaneoka, K. Hip and trunk muscles activity during nordic hamstring exercise. J. Exerc. Rehabil. 2018, 14, 231. [Google Scholar] [CrossRef] [Green Version]
- Roach, S.; San Juan, J.G.; Suprak, D.N.; Lyda, M. Concurrent validity of digital inclinometer and universal goniometer in assessing passive hip mobility in healthy subjects. Int. J. Sports Phys. Ther. 2013, 8, 680–688. [Google Scholar]
- Fraeulin, L.; Holzgreve, F.; Brinkbäumer, M.; Dziuba, A.; Friebe, D.; Klemz, S.; Schmitt, M.; Anna-Lena Theis, A.; Tenberg, S.; van Mark, A.; et al. Intra- And inter-rater reliability of joint range of motion tests using tape measure, digital inclinometer and inertial motion capturing. PLoS ONE 2020, 15, e0243646. [Google Scholar] [CrossRef]
- Trajković, N.; Kozinc, Ž.; Smajla, D.; Šarabon, N. Relationship between ankle strength and range of motion and postural stability during single-leg quiet stance in trained athletes. Sci. Rep. 2021, 11, 11749. [Google Scholar] [CrossRef]
- Norkin, C.; White, J. Measurement of Joint Motion: A Guide to Goniometry; F.A. Davis: Philadelphia, PA, USA, 2016. [Google Scholar]
- Kozinc, Ž.; Šarabon, N. Inter-limb asymmetries in volleyball players: Differences between testing approaches and association with performance. J. Sport. Sci. Med. 2020, 19, 745–752. [Google Scholar]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Bernards, J.; Sato, K.; Haff, G.; Bazyler, C. Current Research and Statistical Practices in Sport Science and a Need for Change. Sports 2017, 5, 87. [Google Scholar] [CrossRef] [Green Version]
- Willson, J.D.; Binder-Macleod, S.; Davis, I.S. Lower extremity jumping mechanics of female athletes with and without patellofemoral pain before and after exertion. Am. J. Sports Med. 2008, 36, 1587–1596. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.H.; Moriya, É.T.U.; MacIel, C.D.; Serrão, F.V. Frontal plane biomechanics in males and females with and without patellofemoral pain. Med. Sci. Sports Exerc. 2012, 44, 1747–1755. [Google Scholar] [CrossRef] [PubMed]
- Teng, H.L.; Powers, C.M. Sagittal Plane Trunk Posture Influences Patellofemoral Joint Stress during Running. J. Orthop. Sport. Phys. Ther. 2014, 44, 785–792. [Google Scholar] [CrossRef] [Green Version]
- Rabelo, N.D.d.A.; Costa, L.O.P.; de Lima, B.M.; dos Reis, A.C.; Bley, A.S.; Fukuda, T.Y.; Lucareli, P.R.G. Adding motor control training to muscle strengthening did not substantially improve the effects on clinical or kinematic outcomes in women with patellofemoral pain: A randomised controlled trial. Gait Posture 2017, 58, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Bolgla, L.A.; Earl-Boehm, J.; Emery, C.; Hamstra-Wright, K.; Ferber, R. Pain, Function, and Strength Outcomes for Males and Females with Patellofemoral Pain Who Participate in Either a Hip/Core- or Knee-Based Rehabilitation Program. Int. J. Sports Phys. Ther. 2016, 11, 926–935. [Google Scholar] [PubMed]
- Emamvirdi, M.; Letafatkar, A.; Khaleghi Tazji, M. The Effect of Valgus Control Instruction Exercises on Pain, Strength, and Functionality in Active Females with Patellofemoral Pain Syndrome. Sports Health 2019, 11, 223–237. [Google Scholar] [CrossRef]
- Crossley, K.M.; van Middelkoop, M.; Barton, C.J.; Culvenor, A.G. Best Practice & Research Clinical Rheumatology Rethinking patellofemoral pain: Prevention, management and long-term consequences. Best Pract. Res. Clin. Rheumatol. 2019, 33, 48–65. [Google Scholar] [CrossRef]
- Lankhorst, N.E.; Bierma-Zeinstra, S.M.A.; Van Middelkoop, M. Factors associated with patellofemoral pain syndrome: A systematic review. Br. J. Sports Med. 2013, 47, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Zamboti, C.L.; da Silva, R.A., Jr.; Gobbi, C.; Shigaki, L.; Macedo, C.d.S.G. Analysis of pain, functional capacity, muscular strength and balance in young women with Patellofemoral Pain Syndrome. Fisioter. Mov. 2017, 30, 433–441. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.P.; Souza, R.B.; Powers, C.M. The influence of hip abductor muscle performance on dynamic postural stability in females with patellofemoral pain. Gait Posture 2012, 36, 425–429. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patellofemoral Pain | Control | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Females | Males | All | Females | Males | All | ||
| n | 13 | 5 | 18 | 26 | 11 | 37 | / |
| Unilateral PFP | 7 | 5 | 12 | / | / | / | / |
| Bilateral PFP | 6 | 0 | 6 | / | / | / | / |
| Age (years) | 19.1 ± 8.4 | 37.4 ± 12.3 | 24.2 ± 12.5 | 20.0 ± 7.4 | 25.3 ± 11.2 | 21.6 ± 8.8 | 0.436 |
| Body height (cm) | 167.5 ± 7.1 | 181.0 ± 11.4 | 170.7 ± 10.2 | 167.6 ± 7.4 | 177.8 ± 8.5 | 170.6 ± 9.0 | 0.972 |
| Body mass (kg) | 57.9 ± 6.7 | 84.2 ± 19.7 | 62.5 ± 11.4 | 60.1 ± 9.0 | 73.7 ± 14.3 | 64.1 ± 12.4 | 0.638 |
| Average training frequency (x/week) | 4.2 ± 2.8 | 3.5 ± 0.6 | 4.1 ± 2.4 | 3.7 ± 1.4 | 3.36 ± 0.9 | 3.6 ± 1.2 | 0.413 |
| Average training session duration (min) | 86.3 ± 24.0 | 112.5 ± 15.0 | 92.8 ± 24.6 | 91.7 ± 16.1 | 80.0 ± 22.4 | 88.2 ± 18.6 | 0.489 |
| Average pain (cm) | 6.0 ± 1.1 | 5.2 ± 0.9 | 5.8 ± 1.2 | / | / | / | / |
| Average pain duration (months) | 9.0 ± 4.0 | 9.2 ± 4.1 | 9.1 ± 3.9 | / | / | / | / |
| Patellar Tilt/Compression | Internal Femoral Rotation | Lateral Patellar Tilt | Patellar Hyper/Hypomobility | Contralateral Pelvic Drop | Knee Valgus | Navicular Drop | Poor Foot Flexibility | High-Riding Patella | |
|---|---|---|---|---|---|---|---|---|---|
| Unilateral | 9 | 3 | 0 | 3 | 4 | 3 | 2 | 1 | 1 |
| Bilateral | 6 | 2 | 1 | 1 | 0 | 1 | 1 | 2 | 0 |
| All | 15 | 5 | 1 | 4 | 4 | 4 | 3 | 3 | 1 |
| Percent | 94% | 31% | 6% | 25% | 25% | 25% | 19% | 19% | 6% |
| Outcome Measure | Means ± SD | Difference | |||
|---|---|---|---|---|---|
| Affected Leg | Non-Affected Leg | t | p | ES | |
| Knee extension (Nm/kg) | 2.36 ± 0.56 | 2.51 ± 0.61 | −1.61 | 0.136 | 0.25 |
| Knee flexion (Nm/kg) | 1.23 ± 0.34 | 1.09 ± 0.31 | 2.02 | 0.069 | 0.43 |
| Ankle extension (Nm/kg) | 1.70 ± 0.86 | 1.90 ± 0.78 | −0.52 | 0.114 | 0.24 |
| Ankle flexion (Nm/kg) | 0.85 ± 0.38 | 0.62 ± 0.21 | 1.68 | 0.022 * | 0.75 |
| Trunk lateral flexion (Nm/kg) | 3.87 ± 1.82 | 3.92 ± 1.74 | −0.21 | 0.840 | 0.03 |
| Hip abduction (Nm/kg) | 0.87 ± 0.11 | 0.88 ± 0.15 | −0.12 | 0.877 | 0.08 |
| Hip adduction (Nm/kg) | 0.79 ± 0.14 | 0.79 ± 0.13 | −0.35 | 0.731 | 0.09 |
| Hip external rotation (Nm/kg) | 0.80 ± 0.20 | 0.82 ± 0.21 | −1.83 | 0.097 | 1.00 |
| Hip internal rotation (Nm/kg) | 0.99 ± 0.23 | 0.87 ± 0.20 | 1.68 | 0.041 * | 0.92 |
| Hip flexion (Nm/kg) | 1.72 ± 0.31 | 1.75 ± 0.25 | −0.45 | 0.663 | 0.11 |
| Hip extension (Nm/kg) | 2.03 ± 0.34 | 1.92 ± 0.38 | 1.50 | 0.164 | 0.31 |
| Nordic hamstring (Nm/kg) | 1.47 ± 0.33 | 1.53 ± 0.29 | −1.11 | 0.293 | 0.19 |
| Outcome Measure | Means ± SD | Difference | Means ± SD | Difference | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Unilateral PFP (n = 12) | Control (n = 37) | t | p | ES | Bilateral PFP (n = 6) | Control (n= 37) | t | p | ES | |
| Knee extension (Nm/kg) | 2.36 ± 0.56 | 2.79 ± 0.92 | −1.54 | 0.048 * | 0.56 | 1.91 ± 0.27 | 2.79 ± 0.92 | −2.29 | 0.027 * | 1.29 |
| Knee flexion (Nm/kg) | 1.23 ± 0.34 | 1.49 ± 0.38 | −2.09 | 0.042 * | 0.72 | 1.25 ± 0.22 | 1.49 ± 0.38 | −1.35 | 0.186 | 0.77 |
| Ankle extension (Nm/kg) | 1.70 ± 0.86 | 1.67 ± 0.52 | 0.19 | 0.853 | 0.04 | 1.64 ± 0.44 | 1.67 ± 0.52 | −0.13 | 0.899 | 0.06 |
| Ankle flexion (Nm/kg) | 0.85 ± 0.38 | 0.48 ± 0.11 | 5.40 | 0.000 * | 1.32 | 0.75 ± 0.28 | 0.48 ± 0.11 | 4.37 | 0.000 * | 1.27 |
| Trunk lateral flexion (Nm/kg) | 3.87 ± 1.82 | 5.32 ± 1.26 | −3.09 | 0.003 * | 0.92 | 3.53 ± 1.79 | 5.32 ± 1.26 | −3.04 | 0.004 * | 1.16 |
| Trunk extension (Nm/kg) | 5.22 ± 2.56 | 7.72 ± 2.19 | −3.31 | 0.002 * | 1.05 | 4.45 ± 2.38 | 7.72 ± 2.19 | −3.36 | 0.002 * | 1.42 |
| Trunk flexion (Nm/kg) | 4.25 ± 2.48 | 5.84 ± 1.40 | −0.58 | 0.567 | 0.79 | 3.17 ± 1.47 | 5.84 ± 1.40 | −4.30 | 0.000 * | 1.86 |
| Hip abduction (Nm/kg) | 0.87 ± 0.11 | 0.90 ± 0.18 | −2.78 | 0.008 * | 0.20 | 0.86 ± 0.10 | 0.90 ± 0.18 | −0.52 | 0.603 | 0.27 |
| Hip adduction (Nm/kg) | 0.79 ± 0.14 | 0.90 ± 0.22 | −1.62 | 0.111 | 0.60 | 0.83 ± 0.10 | 0.90 ± 0.22 | −0.69 | 0.495 | 0.41 |
| Hip external rotation (Nm/kg) | 0.80 ± 0.20 | 0.80 ± 0.17 | −0.08 | 0.939 | 0.09 | 0.86 ± 0.15 | 0.80 ± 0.17 | 0.69 | 0.496 | 0.37 |
| Hip internal rotation (Nm/kg) | 0.99 ± 0.23 | 0.98 ± 0.19 | 0.09 | 0.926 | 0.05 | 1.10 ± 0.21 | 0.98 ± 0.19 | 1.25 | 0.220 | 0.59 |
| Hip flexion (Nm/kg) | 1.72 ± 0.31 | 1.87 ± 0.33 | −0.61 | 0.542 | 0.47 | 2.04 ± 0.32 | 1.87 ± 0.33 | −0.33 | 0.743 | 0.52 |
| Hip extension (Nm/kg) | 2.03 ± 0.34 | 2.13 ± 0.48 | −1.28 | 0.206 | 0.24 | 2.06 ± 0.37 | 2.13 ± 0.48 | 1.12 | 0.270 | 0.16 |
| Nordic hamstring (Nm/kg) | 1.47 ± 0.33 | 3.20 ± 0.81 | −1.39 | 0.170 | 2.79 | 1.42 ± 0.26 | 3.20 ± 0.81 | −1.39 | 0.172 | 2.95 |
| Outcome Measure | Means ± SD | Difference | Means ± SD | Difference | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Unilateral PFP (n = 12) | Control (n = 37) | t | p | ES | Bilateral PFP (n = 6) | Control (n = 37) | t | p | ES | |
| Knee extension (°) | 3.78 ± 3.92 | 3.84 ± 3.72 | −0.18 | 0.861 | 0.02 | 4.01 ± 5.18 | 3.84 ± 3.72 | 0.09 | 0.926 | 0.03 |
| Knee flexion (°) | 148.78 ± 6.92 | 152.38 ± 6.44 | −1.90 | 0.063 | 0.54 | 148.33 ± 3.14 | 152.38 ± 6.44 | −1.50 | 0.142 | 0.79 |
| Ankle extension (°) | 76.72 ± 10.47 | 81.46 ± 6.94 | −2.00 | 0.050 * | 0.53 | 77.83 ± 13.78 | 81.46 ± 6.94 | −1.02 | 0.314 | 0.33 |
| Ankle flexion (°) | 18.22 ± 7.04 | 15.24 ± 0.42 | 1.10 | 0.278 | 0.34 | 18.00 ± 6.36 | 15.24 ± 0.42 | 0.63 | 0.535 | 0.61 |
| Hip abduction (°) | 42.28 ± 8.64 | 42.68 ± 6.85 | −0.19 | 0.853 | 0.05 | 41.83 ± 8.23 | 42.68 ± 6.85 | −0.27 | 0.787 | 0.11 |
| Hip adduction (°) | 28.61 ± 5.83 | 29.89 ± 6.30 | −0.72 | 0.471 | 0.21 | 27.50 ± 3.94 | 29.89 ± 6.30 | −0.90 | 0.375 | 0.45 |
| Hip external rotation (°) | 57.68 ± 15.01 | 65.50 ± 15.72 | −1.76 | 0.084 | 0.51 | 60.70 ± 18.31 | 65.50 ± 15.72 | −0.68 | 0.501 | 0.28 |
| Hip internal rotation (°) | 56.38 ± 13.42 | 56.17 ± 15.19 | 0.05 | 0.959 | 0.01 | 68.75 ± 10.58 | 56.17 ± 15.19 | 1.94 | 0.059 | 0.96 |
| Hip flexion with knee extended (°) | 96.57 ± 13.18 | 102.81 ± 18.08 | −1.30 | 0.198 | 0.39 | 97.45 ± 15.52 | 102.81 ± 18.08 | −0.68 | 0.498 | 0.32 |
| Hip flexion with knee flexed (°) | 145.34 ± 8.44 | 144.58 ± 10.68 | 0.26 | 0.793 | 0.08 | 143.57 ± 5.81 | 144.58 ± 10.68 | −0.23 | 0.822 | 0.11 |
| Hip extension (°) | 29.57 ± 11.01 | 28.86 ± 10.02 | 0.24 | 0.811 | 0.07 | 31.28 ± 13.24 | 28.86 ± 10.02 | 0.53 | 0.602 | 0.21 |
| Trunk lateral flexion diff (cm) | 24.33 ± 5.89 | 23.37 ± 4.27 | 0.69 | 0.490 | 0.19 | 26.17 ± 4.93 | 23.37 ± 4.27 | 1.46 | 0.152 | 0.60 |
| CoP sway path A-P (mm) | 5.01 ± 1.44 | 5.55 ± 1.46 | −1.29 | 0.201 | 0.37 | 4.98 ± 1.95 | 5.55 ± 1.46 | −1.09 | 0.325 | 0.33 |
| CoP sway path M-L (mm) | 5.95 ± 2.24 | 6.60 ± 2.43 | −0.95 | 0.343 | 0.28 | 5.89 ± 2.22 | 6.60 ± 2.43 | −0.85 | 0.352 | 0.30 |
| CoP sway velocity A-P (mm/s) | 23.22 ± 4.99 | 25.76 ± 6.36 | −1.48 | 0.132 | 0.44 | 23.04 ± 5.17 | 25.76 ± 6.36 | −1.31 | 0.201 | 0.81 |
| CoP sway velocity M-L (mm/s) | 25.64 ± 5.68 | 26.83 ± 6.69 | −0.64 | 0.524 | 0.19 | 24.01 ± 5.27 | 26.83 ± 6.69 | −0.78 | 0.098 | 0.47 |
| Standing asymmetry index (%) | 3.77 ± 3.67 | 3.21 ± 2.56 | 0.66 | 0.510 | 0.18 | 3.11 ± 2.95 | 3.21 ± 2.56 | 0.58 | 0.611 | 0.04 |
| Semi-Squat asymmetry index (%) | 4.70 ± 2.23 | 3.87 ± 2.32 | 1.26 | 0.212 | 0.37 | 4.54 ± 2.02 | 3.87 ± 2.32 | 0.98 | 0.204 | 0.31 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manojlović, D.; Zorko, M.; Spudić, D.; Šarabon, N. Strength, Flexibility and Postural Control of the Trunk and Lower Body in Participants with and without Patellofemoral Pain. Appl. Sci. 2022, 12, 3238. https://doi.org/10.3390/app12073238
Manojlović D, Zorko M, Spudić D, Šarabon N. Strength, Flexibility and Postural Control of the Trunk and Lower Body in Participants with and without Patellofemoral Pain. Applied Sciences. 2022; 12(7):3238. https://doi.org/10.3390/app12073238
Chicago/Turabian StyleManojlović, Denisa, Martin Zorko, Darjan Spudić, and Nejc Šarabon. 2022. "Strength, Flexibility and Postural Control of the Trunk and Lower Body in Participants with and without Patellofemoral Pain" Applied Sciences 12, no. 7: 3238. https://doi.org/10.3390/app12073238