
Lung Nodules Localization and Report Analysis from Computerized Tomography (CT) Scan Using a Novel Machine Learning Approach

 ,
,  , , ,
, , ,  ,
,  , and
, and
Abstract
:1. Introduction
1.1. Problem Statement and Goal
1.2. Research Question
- RQ1: What are the obstacles to utilizing CT imaging to detect early lung nodules?
- RQ2: How can an effective lung nodule identification system that minimizes false positives and reduces computing time be developed?
- RQ3: How can we increase nodule detection sensitivity for different lung nodules?
1.3. Objectives of the Study
- To develop quick nodule detection and analysis methods for computed tomography (CT) scan pictures.
- To use advanced Python and MATLAB tools that will make this procedure more precise, consistent and improve the radiologist workflow.
- To create a robust algorithm for detecting lung nodules in 2D and 3D pictures.
2. Related Works
3. Methods and Techniques
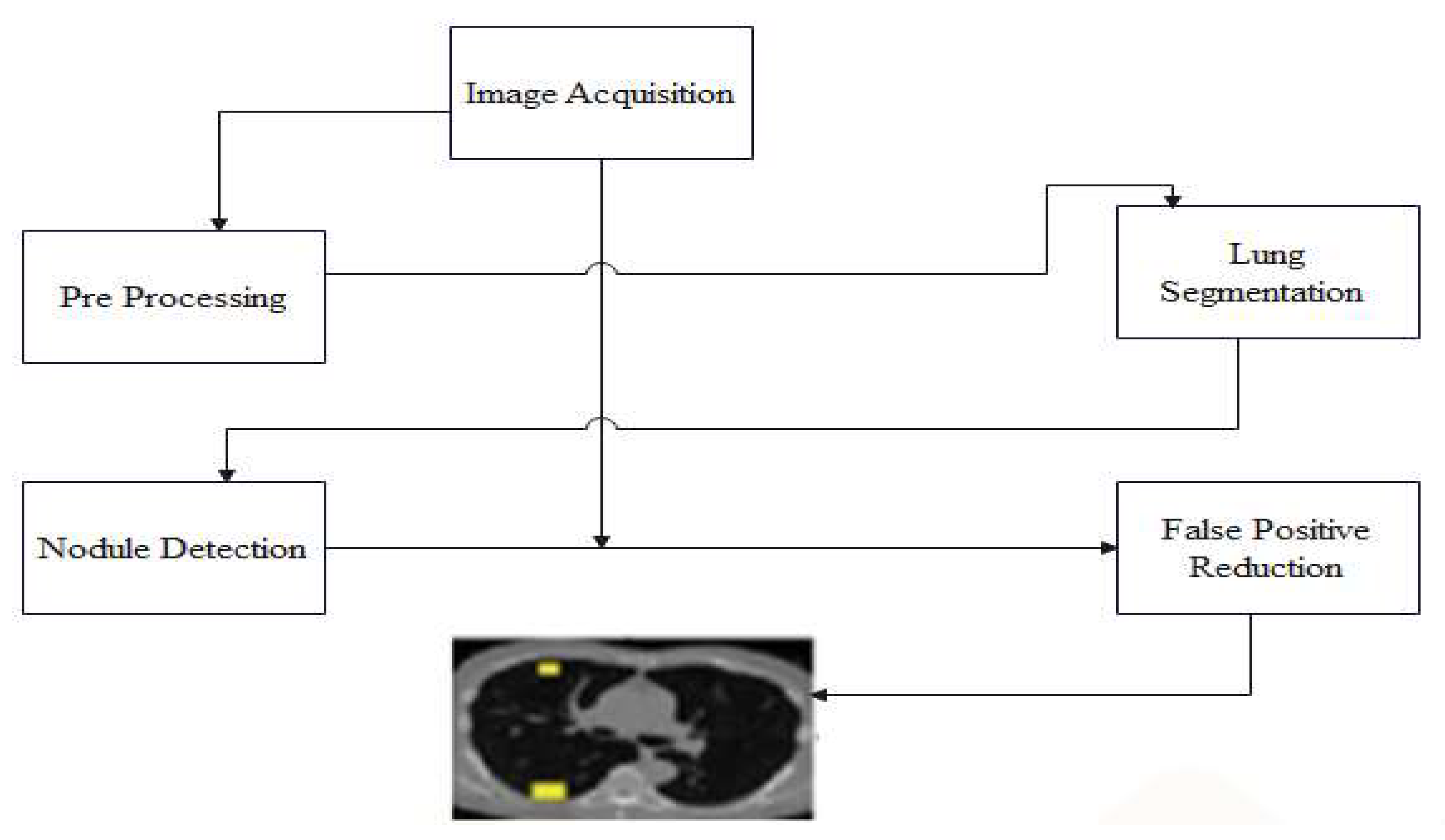
3.1. Proposed Method for Lung Nodule Localization
3.1.1. Pre-Processing
3.1.2. Bitmap Conversion
3.1.3. Noise Removal
3.1.4. Grayscale Conversion
3.1.5. Image Enhancement
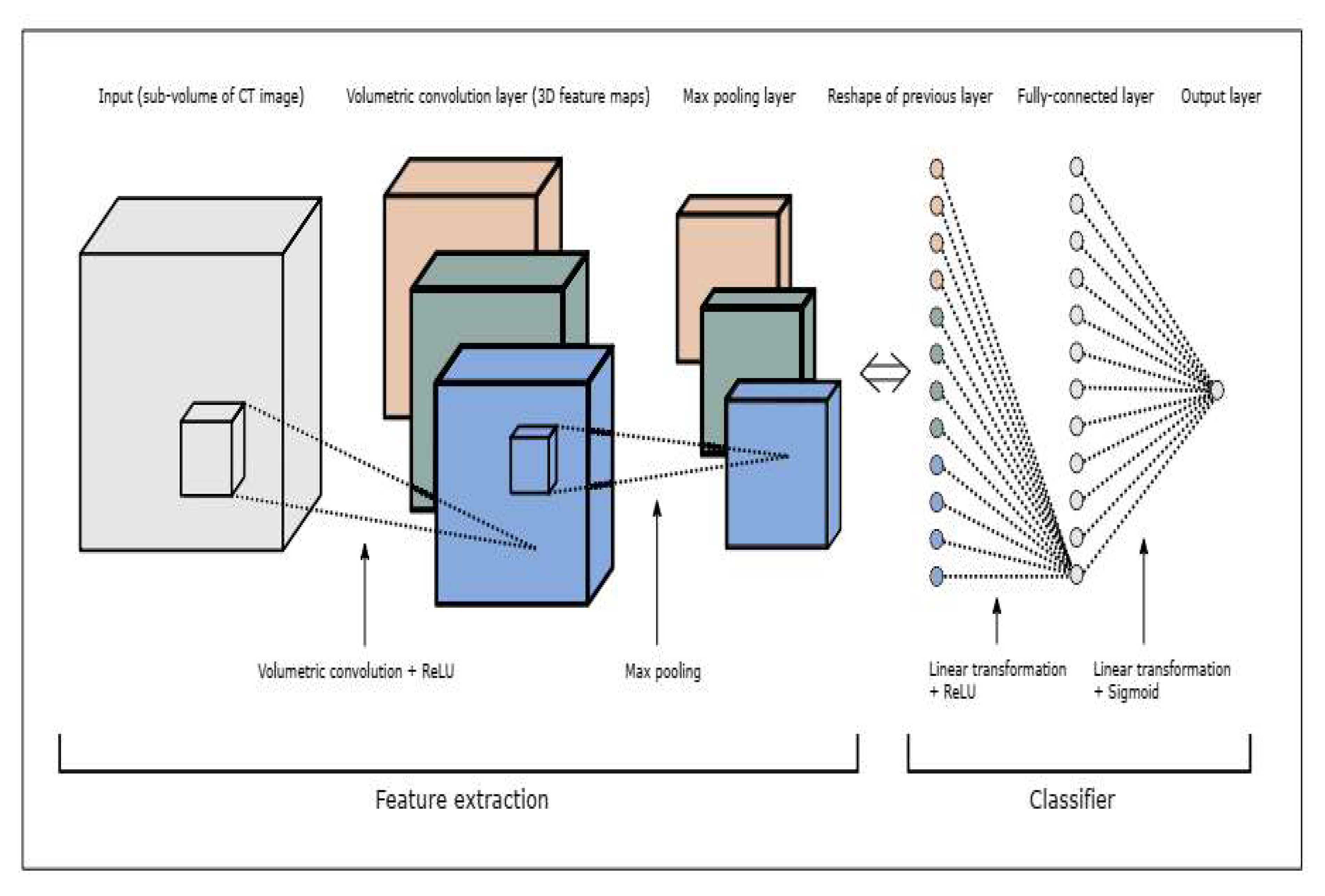
3.1.6. CNN Architecture
- S[t] is the feature map,
- x is the input, and w is the kernel.
3.2. Dataset for Evaluation of System
4. Experimentation and Results
4.1. Proposed CNN Architecture
4.2. Evaluation of Mean Squared Error (MSE)
4.3. Results and Discussion
4.4. Comparison of Results
5. Discussion of Experimental Findings
- The classification accuracy is affected by various algorithm factors, notably patch size, hidden layer nodes, and architectural decisions regarding the CNN.
- Optimizing the CNN architecture to obtain the highest possible accuracy in classification is vital.
- It is possible to reduce false positives by iteratively training the CNN algorithm. In addition, using a training set comprising both unseen true and false positives is of great assistance in reducing the number of false positives to an acceptable level.
- Optimization of the CNN relies on parameters such as the dropout value, the activation function, the number of convolutional layers, and the number of max pooling layers.
- Observation of the distribution of the dataset is necessary for both the statistical analysis and the machine learning-based categorization of lung nodules. Adjusting the voxel size is one of the steps that should be taken to optimize the learning advantage while simultaneously lowering the MSE (the patch size option should be utilized). Significant nodules may be missed if a smaller patch size is used instead of a larger one. If, on the other hand, a considerable number were selected for the patch size, the tiny nodule threshold would not be taken into consideration.
- During the process of detecting lung nodules, it is essential to give careful consideration to both the patch size and the threshold value to achieve the highest achievable level of classification precision.
6. Conclusions
7. Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Healthline. Lung (Pulmonary) Nodules: Symptoms, Causes, and Treatment. August 2022. Available online: https://www.healthline.com/health/lung-cancer/lung-nodule#causes-and-risk-factors (accessed on 23 November 2022).
- Today, M.N. Lung Nodule. 29 November 2021. Available online: https://www.medicalnewstoday.com/articles/317531 (accessed on 23 November 2022).
- Tufail, A.B.; Ma, Y.K.; Kaabar, M.K.; Martínez, F.; Junejo, A.R.; Ullah, I.; Khan, R. Deep learning in cancer diagnosis and prognosis prediction: A minireview on challenges, recent trends, and future directions. Comput. Math. Methods Med. 2021, 2021, 9025470. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Yang, Q.; Ullah, I.; Rehman, A.U.; Tufail, A.B.; Noor, A.; Rehman, A.; Cengiz, K. 3D convolutional neural networks based automatic modulation classification in the presence of channel noise. IET Commun. 2022, 16, 497–509. [Google Scholar] [CrossRef]
- Tufail, A.B.; Ma, Y.K.; Zhang, Q.N.; Khan, A.; Zhao, L.; Yang, Q.; Adeel, M.; Khan, R.; Ullah, I. 3D convolutional neural networks-based multiclass classification of Alzheimer’s and Parkinson’s diseases using PET and SPECT neuroimaging modalities. Brain Inform. 2021, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Lu, X.; Zhang, B.; Zhao, Y.; Yu, D.; Gao, L.; Cui, G.; Wu, L.; Zhou, T. Automatic lung nodule detection using multi-scale dot nodule-enhancement filter and weighted support vector machines in chest computed tomography. PLoS ONE 2019, 14, e0210551. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, A.; Fujita, H. Automated lung nodule detection using positron emission tomography/computed tomography. In Artificial Intelligence in Decision Support Systems for Diagnosis in Medical Imaging; Springer: Berlin/Heidelberg, Germany, 2018; pp. 87–110. [Google Scholar]
- Siddiqui, E.A.; Chourasia, V.; Shandilya, M.; Patel, V. Computed Tomography Image Processing Methods for Lung Nodule Detection and Classification: A Review. In Data, Engineering and Applications; Lecture Notes in Electrical Engineering; Sharma, S., Peng, S.L., Agrawal, J., Shukla, R.K., Le, D.N., Eds.; Springer: Singapore, 2022; Volume 907. [Google Scholar] [CrossRef]
- Zhang, G.; Jiang, S.; Yang, Z.; Gong, L.; Ma, X.; Zhou, Z.; Bao, C.; Liu, Q. Automatic nodule detection for lung cancer in CT images: A review. Comput. Biol. Med. 2018, 103, 287–300. [Google Scholar] [CrossRef]
- Abrar, A.; Rajpoot, P. “Classification and Detection of Lung Cancer Nodule using Deep Learning of CT Scan Images”: A Systematic Review. 2022. Available online: https://assets.researchsquare.com/files/rs-2145172/v1/2a94278e-c16b-4346-ae89-3042ca2fb409.pdf?c=1666567759 (accessed on 25 November 2022).
- Tufail, A.B.; Ullah, I.; Khan, R.; Ali, L.; Yousaf, A.; Rehman, A.U.; Alhakami, W.; Hamam, H.; Cheikhrouhou, O.; Ma, Y.K. Recognition of Ziziphus lotus through Aerial Imaging and Deep Transfer Learning Approach. Mob. Inf. Syst. 2021, 2021, 4310321. [Google Scholar] [CrossRef]
- Ahmad, I.; Ullah, I.; Khan, W.U.; Ur Rehman, A.; Adrees, M.S.; Saleem, M.Q.; Cheikhrouhou, O.; Hamam, H.; Shafiq, M. Efficient algorithms for E-healthcare to solve multiobject fuse detection problem. J. Healthc. Eng. 2021, 2021, 9500304. [Google Scholar] [CrossRef]
- Tufail, A.B.; Anwar, N.; Othman, M.T.; Ullah, I.; Khan, R.A.; Ma, Y.K.; Adhikari, D.; Rehman, A.U.; Shafiq, M.; Hamam, H. Early-stage Alzheimer’s disease categorization using PET neuroimaging modality and convolutional neural networks in the 2D and 3D domains. Sensors 2022, 22, 4609. [Google Scholar] [CrossRef]
- Ahmed, I.; Chehri, A.; Jeon, G.; Piccialli, F. Automated pulmonary nodule classification and detection using deep learning architectures. IEEE/ACM Trans. Comput. Biol. Bioinform. 2022, 1–12. [Google Scholar] [CrossRef]
- Agnes, S.A.; Anitha, J.; Solomon, A.A. Two-stage lung nodule detection framework using enhanced UNet and convolutional LSTM networks in CT images. Comput. Biol. Med. 2022, 149, 106059. [Google Scholar] [CrossRef]
- Rodrigues, M.B.; Da Nobrega, R.V.M.; Alves, S.S.A.; Rebouças Filho, P.P.; Duarte, J.B.F.; Sangaiah, A.K.; De Albuquerque, V.H.C. Health of things algorithms for malignancy level classification of lung nodules. IEEE Access 2018, 6, 18592–18601. [Google Scholar] [CrossRef]
- Kumar, D.; Wong, A.; Clausi, D.A. Lung nodule classification using deep features in CT images. In Proceedings of the 2015 12th Conference on Computer and Robot Vision, Halifax, NS, Canada, 3–5 June 2015; pp. 133–138. [Google Scholar]
- Aresta, G.; Cunha, A.; Campilho, A. Detection of juxta-pleural lung nodules in computed tomography images. In Proceedings of the Medical Imaging 2017: Computer-Aided Diagnosis, Orlando, FL, USA, 3 March 2017; pp. 952–958. [Google Scholar]
- Ahmad, S.; Ullah, T.; Ahmad, I.; Al-Sharabi, A.; Ullah, K.; Khan, R.A.; Rasheed, S.; Ullah, I.; Uddin, M.; Ali, M. A novel hybrid deep learning model for metastatic cancer detection. Comput. Intell. Neurosci. 2022, 2022, 8141530. [Google Scholar] [CrossRef] [PubMed]
- Tufail, A.B.; Ullah, K.; Khan, R.A.; Shakir, M.; Khan, M.A.; Ullah, I.; Ma, Y.K.; Ali, M. On Improved 3D-CNN-Based Binary and Multiclass Classification of Alzheimer’s Disease Using Neuroimaging Modalities and Data Augmentation Methods. J. Healthc. Eng. 2022, 2022, 1302170. [Google Scholar] [CrossRef] [PubMed]
- Nakrani, M.G.; Sable, G.S.; Shinde, U.B. Lung Nodule Detection from Computed Tomography Images Using Stacked Deep Convolutional Neural Network. In Intelligent Systems, Technologies and Applications; Springer: Singapore, 2021; pp. 237–246. [Google Scholar]
- Hamidian, S.; Sahiner, B.; Petrick, N.; Pezeshk, A. 3D convolutional neural network for automatic detection of lung nodules in chest CT. In Proceedings of the Medical Imaging 2017: Computer-Aided Diagnosis, Orlando, FL, USA, 3 March 2017; pp. 54–59. [Google Scholar]
- Sun, L.; Wang, Z.; Pu, H.; Yuan, G.; Guo, L.; Pu, T.; Peng, Z. Attention-embedded complementary-stream CNN for false positive reduction in pulmonary nodule detection. Comput. Biol. Med. 2021, 133, 104357. [Google Scholar] [CrossRef]
- Singadkar, G.; Mahajan, A.; Thakur, M.; Talbar, S. Automatic lung segmentation for the inclusion of juxtapleural nodules and pulmonary vessels using curvature based border correction. J. King Saud Univ. Comput. Inf. Sci. 2021, 33, 975–987. [Google Scholar] [CrossRef]
- Eisapour Moghaddam, A.; Akbarizadeh, G.; Kaabi, H. Automatic detection and segmentation of blood vessels and pulmonary nodules based on a line tracking method and generalized linear regression model. Signal Image Video Process. 2019, 13, 457–464. [Google Scholar] [CrossRef]
- Choi, W.-J.; Choi, T.-S. Automated pulmonary nodule detection based on three-dimensional shape-based feature descriptor. Comput. Methods Programs Biomed. 2014, 113, 37–54. [Google Scholar] [CrossRef]
- de Sousa Costa, R.W.; da Silva, G.L.F.; de Carvalho Filho, A.O.; Silva, A.C.; de Paiva, A.C.; Gattass, M. Classification of malignant and benign lung nodules using taxonomic diversity index and phylogenetic distance. Med. Biol. Eng. Comput. 2018, 56, 2125–2136. [Google Scholar] [CrossRef]
- Kasinathan, G.; Jayakumar, S.; Gandomi, A.H.; Ramachandran, M.; Fong, S.J.; Patan, R. Automated 3-D lung tumor detection and classification by an active contour model and CNN classifier. Expert Syst. Appl. 2019, 134, 112–119. [Google Scholar] [CrossRef]
- Gong, L.; Jiang, S.; Yang, Z.; Zhang, G.; Wang, L. Automated pulmonary nodule detection in CT images using 3D deep squeeze-and-excitation networks. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1969–1979. [Google Scholar] [CrossRef]
- Karkra, S.; Patel, J.K.B. Multi-atlas Segmentation: Label Propagation and Fusion Based Approach. In Advances in Computer Communication and Computational Sciences; Springer: Singapore, 2019; pp. 323–335. [Google Scholar]
- Sharp, G.C. Introduction to Multi-Atlas Auto-Segmentation. In Auto-Segmentation for Radiation Oncology; CRC Press: Boca Raton, FL, USA, 2021; pp. 13–18. [Google Scholar]
- Zuo, W.; Zhou, F.; He, Y.; Li, X. Automatic classification of lung nodule candidates based on a novel 3D convolution network and knowledge transferred from a 2D network. Med. Phys. 2019, 46, 5499–5513. [Google Scholar] [CrossRef] [PubMed]
- Spadea, M.F.; Pileggi, G.; Zaffino, P.; Salome, P.; Catana, C.; Izquierdo-Garcia, D.; Amato, F.; Seco, J. Deep convolution neural network (DCNN) multiplane approach to synthetic CT generation from MR images—Application in brain proton therapy. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, A.T.; Wasserman, G.A.; Arafa, E.I.; Wooten, A.K.; Smith, N.; Martin, I.; Jones, M.R.; Quinton, L.J.; Mizgerd, J.P. Lung CD4+ resident memory T cells remodel epithelial responses to accelerate neutrophil recruitment during pneumonia. Mucosal Immunol. 2020, 13, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.D.; Chen, D. Segmentation for Object-Based Image Analysis (OBIA): A review of algorithms and challenges from remote sensing perspective. ISPRS J. Photogramm. Remote Sens. 2019, 150, 115–134. [Google Scholar] [CrossRef]
- Wong, J.F.; Mohan, M.D.; Young, E.W.; Simmons, C.A. Integrated electrochemical measurement of endothelial permeability in a 3D hydrogel-based microfluidic vascular model. Biosens. Bioelectron. 2020, 147, 111757. [Google Scholar] [CrossRef] [PubMed]
- Tufail, A.B.; Ullah, I.; Khan, W.U.; Asif, M.; Ahmad, I.; Ma, Y.K.; Khan, R.; Ali, M. Diagnosis of diabetic retinopathy through retinal fundus images and 3D convolutional neural networks with limited number of samples. Wirel. Commun. Mob. Comput. 2021, 2021, 6013448. [Google Scholar] [CrossRef]
- Yousafzai, B.K.; Khan, S.A.; Rahman, T.; Khan, I.; Ullah, I.; Ur Rehman, A.; Baz, M.; Hamam, H.; Cheikhrouhou, O. Student-performulator: Student academic performance using hybrid deep neural network. Sustainability 2021, 13, 9775. [Google Scholar] [CrossRef]
- Tufail, A.B.; Ullah, I.; Rehman, A.U.; Khan, R.A.; Khan, M.A.; Ma, Y.-K.; Hussain Khokhar, N.; Sadiq, M.T.; Khan, R.; Shafiq, M.; et al. On Disharmony in Batch Normalization and Dropout Methods for Early Categorization of Alzheimer’s Disease. Sustainability 2022, 14, 14695. [Google Scholar] [CrossRef]
- Khairuzzaman, A.K.M.; Chaudhury, S. Multilevel thresholding using grey wolf optimizer for image segmentation. Expert Syst. Appl. 2017, 86, 64–76. [Google Scholar] [CrossRef]
- Lessmann, N.; Išgum, I.; Setio, A.A.; de Vos, B.D.; Ciompi, F.; de Jong, P.A.; Oudkerk, M.; Willem, P.T.M.; Viergever, M.A.; van Ginneken, B. Deep convolutional neural networks for automatic coronary calcium scoring in a screening study with low-dose chest CT. In Proceedings of the Medical Imaging 2016: Computer-Aided Diagnosis, San Diego, CA, USA, 24 March 2016; pp. 255–260. [Google Scholar]
- Setio, A.A.A.; Traverso, A.; De Bel, T.; Berens, M.S.; Van Den Bogaard, C.; Cerello, P.; Chen, H.; Dou, Q.; Fantacci, M.E.; Geurts, B. Validation, comparison, and combination of algorithms for automatic detection of pulmonary nodules in computed tomography images: The LUNA16 challenge. Med. Image Anal. 2017, 42, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Gao, Z.; Wang, X.; Yang, Y.; Mu, C.; Cai, Q.; Dang, W.; Zuo, S. EEG-based spatio–temporal convolutional neural network for driver fatigue evaluation. IEEE Trans. Neural Netw. Learn. Syst. 2019, 30, 2755–2763. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Patch Size | 36, 48, 48 |
| Convolution Layer | 3 × 5 × 5 |
| Max Pooling | 3 × 3 × 3 |
| Dropout Value | 0.2 |
| Convolution Layer 2 | 3 × 5 × 5 |
| Max Pooling 2 | 2 × 2 × 2 |
| Dropout Value | 0.2 |
| Fully Connected Layer | 350 nodes |
| Fully Connected Layer 2 (Nodes) | 2 |
| Activation | Softmax |
| N = 1018 | Predicted Yes | Predicted No |
|---|---|---|
| Actual Yes | TP | FP |
| 427 | 45 | |
| Actual No | FN | TN |
| 110 | 436 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haq, I.; Mazhar, T.; Malik, M.A.; Kamal, M.M.; Ullah, I.; Kim, T.; Hamdi, M.; Hamam, H. Lung Nodules Localization and Report Analysis from Computerized Tomography (CT) Scan Using a Novel Machine Learning Approach. Appl. Sci. 2022, 12, 12614. https://doi.org/10.3390/app122412614
Haq I, Mazhar T, Malik MA, Kamal MM, Ullah I, Kim T, Hamdi M, Hamam H. Lung Nodules Localization and Report Analysis from Computerized Tomography (CT) Scan Using a Novel Machine Learning Approach. Applied Sciences. 2022; 12(24):12614. https://doi.org/10.3390/app122412614
Chicago/Turabian StyleHaq, Inayatul, Tehseen Mazhar, Muhammad Amir Malik, Mian Muhammad Kamal, Inam Ullah, Taejoon Kim, Monia Hamdi, and Habib Hamam. 2022. "Lung Nodules Localization and Report Analysis from Computerized Tomography (CT) Scan Using a Novel Machine Learning Approach" Applied Sciences 12, no. 24: 12614. https://doi.org/10.3390/app122412614