
Clinical Characterization of Inpatients with Acute Conjunctivitis: A Retrospective Analysis by Natural Language Processing and Machine Learning



Abstract
:1. Introduction
2. Materials and Methods
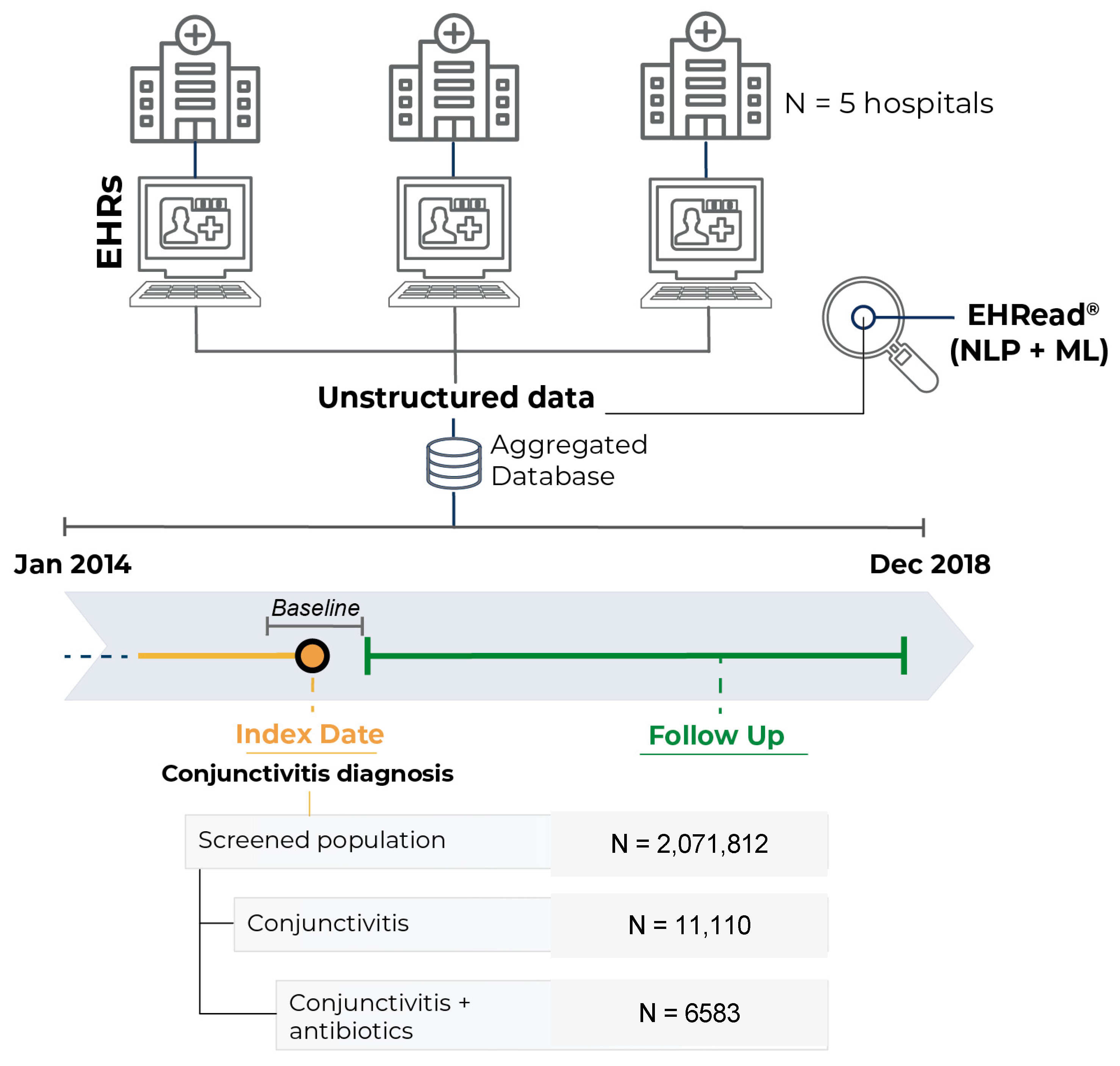
2.1. Study Design
2.2. Data Source
2.3. Objectives
2.4. Study Population
2.5. Extraction of the Unstructured Information from EHRs
2.6. External Validation of EHRead®’s Performance
2.7. Statistical Data Analyses
2.8. Ethical Considerations
3. Results
3.1. Study Population and Linguistic Validation of the System
3.2. Characterization of the Target Population
3.3. Microbiology Results and Conjunctivitis-Related Signs and Symptoms
3.4. Treatments
3.5. Visits
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leibowitz, H.M. The red eye. N. Engl. J. Med. 2000, 343, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Udeh, B.L.; Schneider, J.E.; Ohsfeldt, R.L. Cost effectiveness of a point-of-care test for adenoviral conjunctivitis. Am. J. Med. Sci. 2008, 336, 254–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azari, A.A.; Barney, N.P. Conjunctivitis: A systematic review of diagnosis and treatment. JAMA 2013, 310, 1721–1729. [Google Scholar] [CrossRef] [PubMed]
- Epling, J. Bacterial conjunctivitis. BMJ Clin. Evid. 2012, 2012, 704. [Google Scholar]
- Bielory, B.P.; O’Brien, T.P.; Bielory, L. Management of seasonal allergic conjunctivitis: Guide to therapy. Acta Ophthalmol. 2012, 90, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Hovding, G. Acute bacterial conjunctivitis. Acta Ophthalmol. 2008, 86, 5–17. [Google Scholar] [CrossRef]
- Alfonso, S.A.; Fawley, J.D.; Alexa Lu, X. Conjunctivitis. Prim. Care 2015, 42, 325–345. [Google Scholar] [CrossRef]
- Smith, A.F.; Waycaster, C. Estimate of the direct and indirect annual cost of bacterial conjunctivitis in the United States. BMC Ophthalmol. 2009, 9, 13. [Google Scholar] [CrossRef] [Green Version]
- Azari, A.A.; Arabi, A. Conjunctivitis: A Systematic Review. J. Ophthalmic Vis. Res. 2020, 15, 372–395. [Google Scholar] [CrossRef]
- Sheikh, A.; Hurwitz, B.; van Schayck, C.P.; McLean, S.; Nurmatov, U. Antibiotics versus placebo for acute bacterial conjunctivitis. Cochrane Database Syst. Rev. 2012, 9, CD001211. [Google Scholar] [CrossRef] [Green Version]
- Lovato, L.C.; Hill, K.; Hertert, S.; Hunninghake, D.B.; Probstfield, J.L. Recruitment for controlled clinical trials: Literature summary and annotated bibliography. Control Clin. Trials 1997, 18, 328–352. [Google Scholar] [CrossRef] [PubMed]
- McDonald, A.M.; Knight, R.C.; Campbell, M.K. What influences recruitment to randomised controlled trials? A review of trials funded by two UK funding agencies. Trials 2006, 7, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheikhalishahi, S.; Miotto, R.; Dudley, J.T.; Lavelli, A.; Rinaldi, F.; Osmani, V. Natural Language Processing of Clinical Notes on Chronic Diseases: Systematic Review. JMIR Med. Inform. 2019, 7, e12239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, B.A.; Navar, A.M.; Pencina, M.J.; Ioannidis, J.P. Opportunities and challenges in developing risk prediction models with electronic health records data: A systematic review. J. Am. Med. Inform. Assoc. 2017, 24, 198–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, Y.; Thompson, W.K.; Herr, T.M. Natural Language Processing for EHR-Based Pharmacovigilance: A Structured Review. Drug Saf. 2017, 40, 1075–1089. [Google Scholar] [CrossRef]
- Izquierdo, J.L.; Almonacid, C.; González, Y. The Impact of COVID-19 on Patients with Asthma. Eur. Res. J. 2020, 57, 2003142. [Google Scholar] [CrossRef]
- Ancochea, J.; Izquierdo, J.L.; Medrano, I.H.; Porras, A.; Serrano, M.; Lumbreras, S.; Del Rio-Bermudez, C.; Marchesseau, S.; Salcedo, I.; Zubizarreta, I.; et al. Evidence of gender differences in the diagnosis and management of COVID-19 patients: An analysis of Electronic Health Records using Natural Language Processing and machine learning. J. Women Health 2021, 30, 393–404. [Google Scholar] [CrossRef]
- Izquierdo, J.L.; Ancochea, J.; Soriano, J.B. Clinical Characteristics and Prognostic Factors for Intensive Care Unit Admission of Patients With COVID-19: Retrospective Study Using Machine Learning and Natural Language Processing. J. Med. Internet Res. 2020, 22, e21801. [Google Scholar] [CrossRef]
- Graziani, D.; Soriano, J.B.; Del Rio-Bermudez, C. Characteristics and Prognosis of COVID-19 in Patients with COPD. J. Clin. Med. 2020, 9, 3259. [Google Scholar] [CrossRef]
- González-Juanatey, C.; Anguita-Sánchez, M.; Barrios, V.; Núñez-Gil, I.; Gómez-Doblas, J.J.; García-Moll, X. Assessment of medical management in Coronary Type 2 Diabetic patients with previous percutaneous coronary intervention in Spain: A retrospective analysis of electronic health records using Natural Language Processing. PLoS ONE 2022, 17, e0263277. [Google Scholar] [CrossRef]
- Gomollón, F.G.; Gisbert, J.P.; Guerra, I.; Montoto, C. Clinical Characteristics and Prognostic Factors for Crohn’s Disease Relapses using Natural Language Processing and Machine Learning—A Pilot Study. Eur. J. Gastroenterol. Hepatol. 2022, 34, 389–397. [Google Scholar] [CrossRef]
- Del Rio-Bermudez, C.; Medrano, I.H.; Yebes, L.; Poveda, J.L. Towards a symbiotic relationship between big data, artificial intelligence, and hospital pharmacy. J. Pharm. Policy Pract. 2020, 13, 75. [Google Scholar] [CrossRef]
- Canales, L.; Menke, S.; Marchesseau, S.; D’Agostino, A.; Del Rio-Bermudez, C.; Taberna, M. Assessing the Performance of Clinical Natural Language Processing Systems: Development of an Evaluation Methodology. JMIR Med. Inform. 2021, 9, e20492. [Google Scholar] [CrossRef] [PubMed]
- Espinosa-Anke, L.T.J.; Pardo, A.; Medrano, I.; Ureña, A.; Salcedo, I.; Saggion, H. Savana: A Global Information Extraction and Terminology Expansion Framework in the Medical Domain Procesamiento del Lenguaje Natural. Soc. Espanol. Proc. Nat. 2016, 57, 23–30. [Google Scholar]
- Benson, T. Principles of Health Interoperability HL7 and SNOMED; Springer: London, UK, 2012. [Google Scholar]
- Yeu, E.; Hauswirth, S. A Review of the Differential Diagnosis of Acute Infectious Conjunctivitis: Implications for Treatment and Management. Clin. Ophthalmol. 2020, 14, 805–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, P. Management strategies for acute infective conjunctivitis in primary care: A systematic review. Expert Opin. Pharmacother. 2007, 8, 1903–1921. [Google Scholar] [CrossRef]
- Woodward, M.; Maganti, N.; Niziol, L.; Amin, S.; Hou, A.; Singh, K. Development and Validation of a Natural Language Processing Algorithm to Extract Descriptors of Microbial Keratitis from the Electronic Health Record. Cornea 2021, 40, 1548–1553. [Google Scholar] [CrossRef]
- Meaders, B.C.; Azar, J.M. Bacterial conjunctivitis: A review of therapies and approaches. Adv. NPs PAs 2012, 3, 25–29, 34. [Google Scholar]
- Mas-Tur, V.; Jawaid, I.; Poostchi, A.; Verma, S. Optometrist referrals to an emergency ophthalmology department: A retrospective review to identify current practise and development of shared care working strategies, in England. Eye 2021, 35, 1340–1346. [Google Scholar] [CrossRef] [PubMed]
- Orden Martínez, B.; Martínez Ruiz, R.; Millán Pérez, R. Bacterial conjunctivitis: Most prevalent pathogens and their antibiotic sensitivity. An. Pediatr. 2004, 61, 32–36. [Google Scholar] [CrossRef]
- Benitez-Del-Castillo, J.; Verboven, Y.; Stroman, D.; Kodjikian, L. The role of topical moxifloxacin, a new antibacterial in Europe, in the treatment of bacterial conjunctivitis. Clin. Drug Investig. 2011, 31, 543–557. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N = 6583 | |
|---|---|
| Demographic characteristics | |
| Age (years) | |
| Mean ± SD | 54.83 ± 20.64 |
| Median (Q1, Q3) | 53 (37.5, 72) |
| <65 years old, % | 64.4 |
| ≥65 years old, % | 35.5 |
| Gender, N (%) | |
| Female | 3760 (57.1) |
| Male | 2823 (42.9) |
| Comorbidities, N (%) | |
| Cardiovascular disorders | |
| Anemia | 1064 (16.2) |
| Angina | 307 (4.7) |
| Atrial Fibrillation | 711 (10.8) |
| Heart Failure | 972 (14.8) |
| Hypertension | 3343 (50.8) |
| Endocrine disorders | |
| Diabetes | 797 (12.1) |
| Dyslipidemia | 2627 (39.9) |
| Hypoglycemia | 207 (3.1) |
| Hyperthyroidism | 137 (2.1) |
| Hypothyroidism | 636 (9.7) |
| Musculoskeletal and connective tissue disorders | |
| Foot ulcer | 15 (0.2) |
| Nervous system disorders | |
| Diabetic peripheral neuropathy | 38 (0.6) |
| Psychiatric disorders | |
| Depression | 800 (12.2) |
| Anxiety | 962 (14.6) |
| Respiratory, thoracic, and mediastinal disorders | |
| COPD | 530 (8.1) |
| Asthma | 1024 (15.6) |
| Cancer | 1558 (23.7) |
| Eye disorders | |
| Astigmatism | 77 (1.2) |
| Diabetic retinopathy | 196 (3) |
| Glaucoma | 340 (5.2) |
| Farsightedness | 36 (0.5) |
| Myopia | 318 (4.8) |
| Presbyopia | 82 (1.2) |
| Patients (6583) | |
|---|---|
| Microbiologically confirmed bacterial conjunctivitis n (%) | 795 (12.1) |
| Polymicrobial positivity n (%) | 257 (32.3) |
| Enterobacteriaceae n (%) | 90 (11.3) |
| Haemophilus influenzae n (%) | 55 (6.9) |
| Moraxella catarrhalis n (%) | 18 (2.3) |
| Moraxella lacunata n (%) | 1 (0.1) |
| Neisseria meningitidis n (%) | 33 (4.2) |
| Non-fermentative Gram-negative bacilli n (%) | 296 (37.2) |
| Proteus n (%) | 37 (4.7) |
| Pseudomonas n (%) | 110 (13.8) |
| Staphylococcus aureus n (%) | 189 (23.8) |
| Staphylococcus epidermidis n (%) | 64 (8.1) |
| Streptococcus pneumoniae n (%) | 279 (35.1) |
| Streptococcus pyogenes n (%) | 34 (4.3) |
| Streptococcus viridans n (%) | 7 (0.9) |
| Patients (6583) | |
|---|---|
| Conjunctival hyperemia n (%) | 4908 (74.6) |
| Conjunctival discharge n (%) | 618 (9.4) |
| Bulbar conjunctival injection n (%) | 105 (1.6) |
| Ocular pain n (%) | 731 (11.1) |
| Chemosis n (%) | 500 (7.6) |
| Foreign body sensation n (%) | 643 (9.8) |
| Tearing n (%) | 1367 (20.8) |
| Ocular itching n (%) | 2809 (42.7) |
| Photophobia n (%) | 232 (3.5) |
| Corneal ulcer n (%) | 180 (2.7) |
| Patients (6583) | |
|---|---|
| Classes of topical treatment | |
| Antibiotics + Corticosteroids n (%) | 4487 (68.2) |
| Antibiotics + NSAIDs n (%) | 2368 (36) |
| Antibiotics + NSAIDs + Corticosteroids n (%) | 1148 (17.4) |
| Specific topical treatments | |
| Gentamycin (Oftalmolosa Cusi Gentamicina) n (%) | 613 (9.3) |
| Tobramycin (Tobrex) n (%) | 4631 (70.3) |
| Tobramycin and Dexamethasone | |
| (Tobradex) n (%) | 3513 (53.4) |
| Neomycin (Maxitrol) n (%) | 212 (3.2) |
| Tobramycin (Terracortril) n (%) | 373 (5.7) |
| Corticosteroids n (%) | 4855 (73.8) |
| Dexamethasone (Colircusi Dexamethasone+) n (%) | 3965 (60.2) |
| Hydrocortisone (Oftalmolosa Cusi Hydrocortisone+) n (%) | 657 (10) |
| Fluorometholone (Isopto Flucon) n (%) | 801 (12.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdés Sanz, N.; García-Layana, A.; Colas, T.; Moriche, M.; Montero Moreno, M.; Ciprandi, G. Clinical Characterization of Inpatients with Acute Conjunctivitis: A Retrospective Analysis by Natural Language Processing and Machine Learning. Appl. Sci. 2022, 12, 12352. https://doi.org/10.3390/app122312352
Valdés Sanz N, García-Layana A, Colas T, Moriche M, Montero Moreno M, Ciprandi G. Clinical Characterization of Inpatients with Acute Conjunctivitis: A Retrospective Analysis by Natural Language Processing and Machine Learning. Applied Sciences. 2022; 12(23):12352. https://doi.org/10.3390/app122312352
Chicago/Turabian StyleValdés Sanz, Nuria, Alfredo García-Layana, Teresa Colas, Manuel Moriche, Manuel Montero Moreno, and Giorgio Ciprandi. 2022. "Clinical Characterization of Inpatients with Acute Conjunctivitis: A Retrospective Analysis by Natural Language Processing and Machine Learning" Applied Sciences 12, no. 23: 12352. https://doi.org/10.3390/app122312352