
A Stochastic Queueing Model for the Pricing of Time-Sensitive Services in the Demand-Sharing Alliance
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
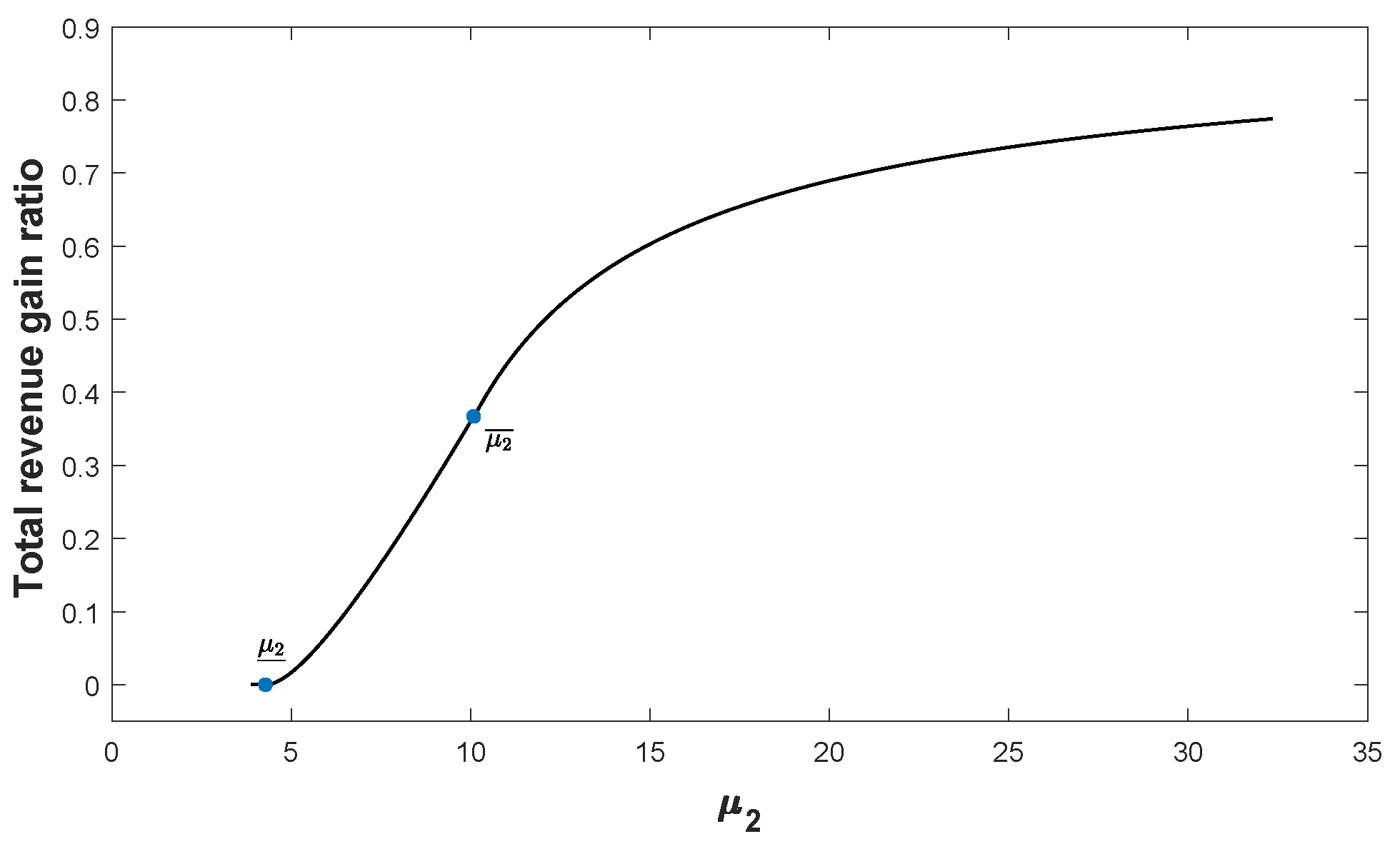
- we obtain the threshold condition for HS’s idle capacity under which the demand sharing works.
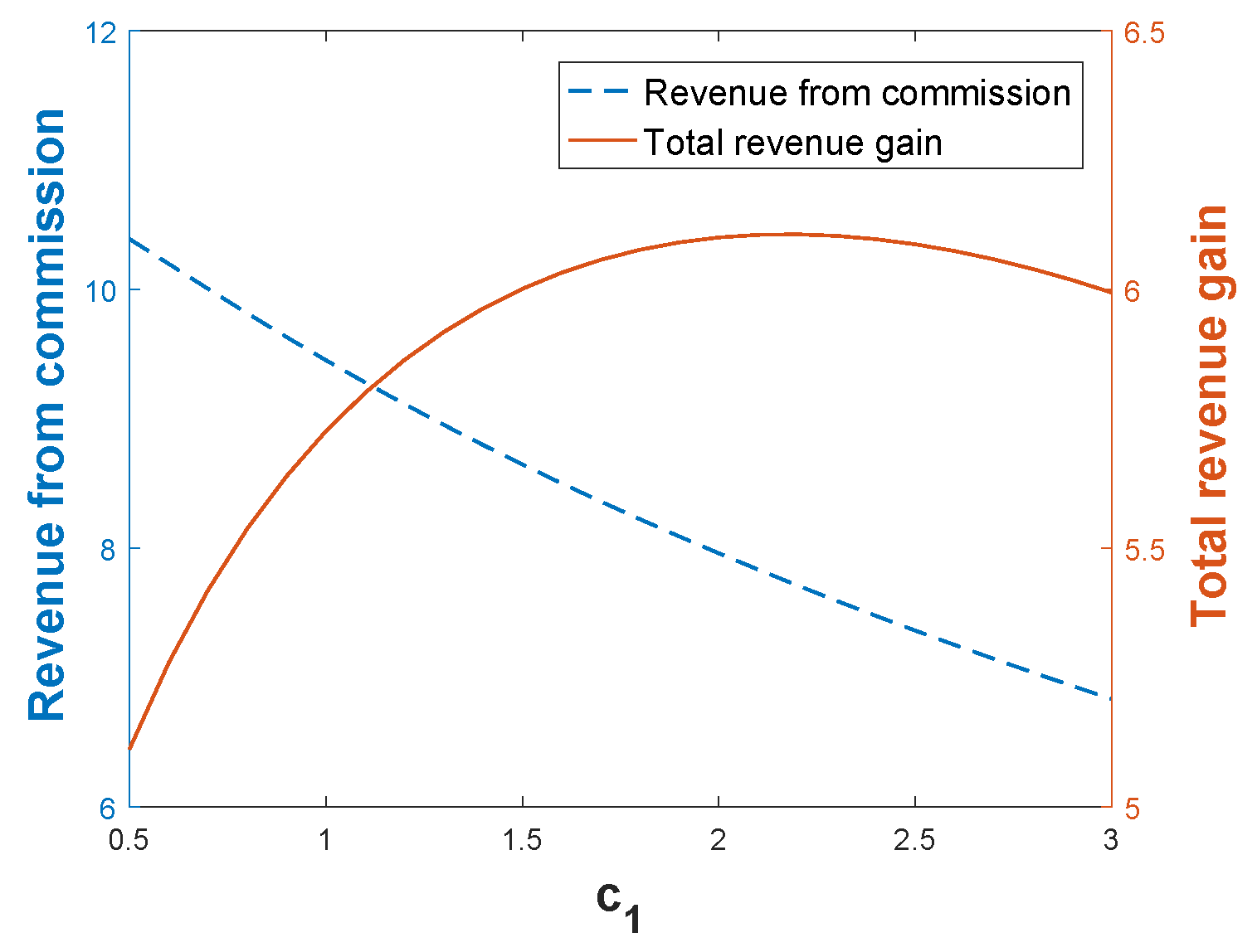
- we provide the optimal (or stable) commission fee charged by HD that makes demand sharing alliance work.
2. Related Literature
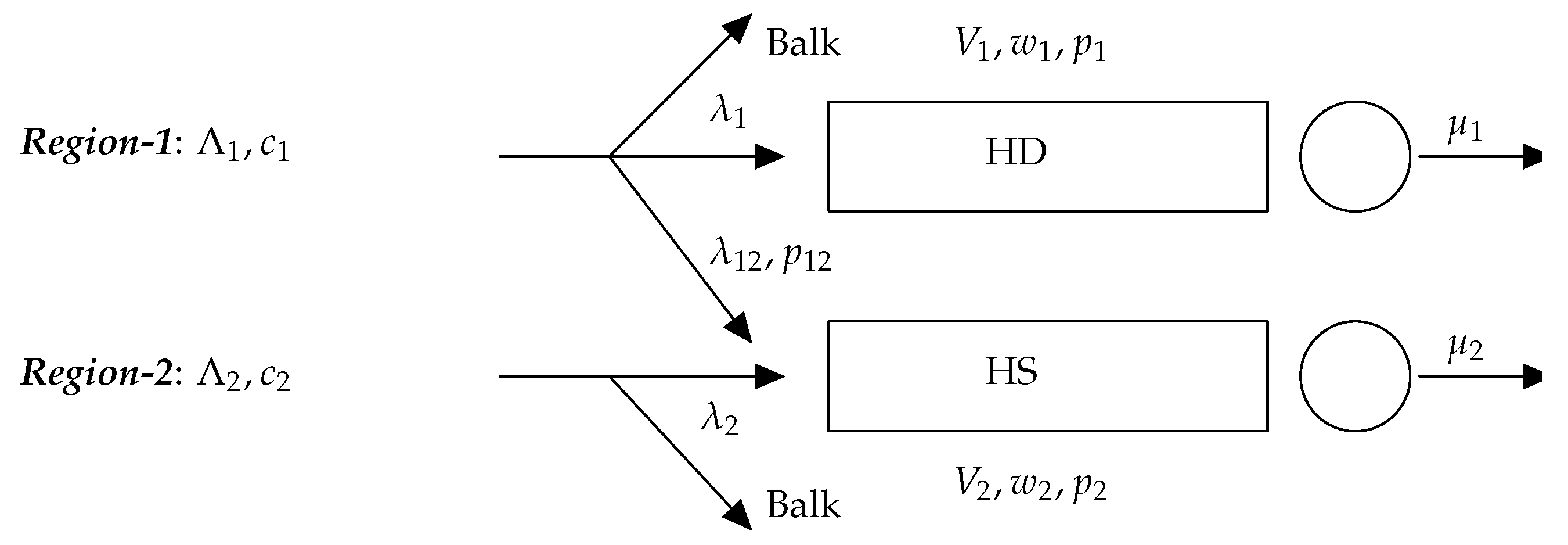
3. Model Formulation
3.1. Two Hospitals with Unbalanced Congestion
- if , then the optimal price is , the optimal effective arrival rate is , and the corresponding optimal revenue is .
- if , then the optimal price is , the optimal effective arrival rate is , and the corresponding optimal revenue is .
3.2. Demand Sharing between Two Hospitals
4. Analysis
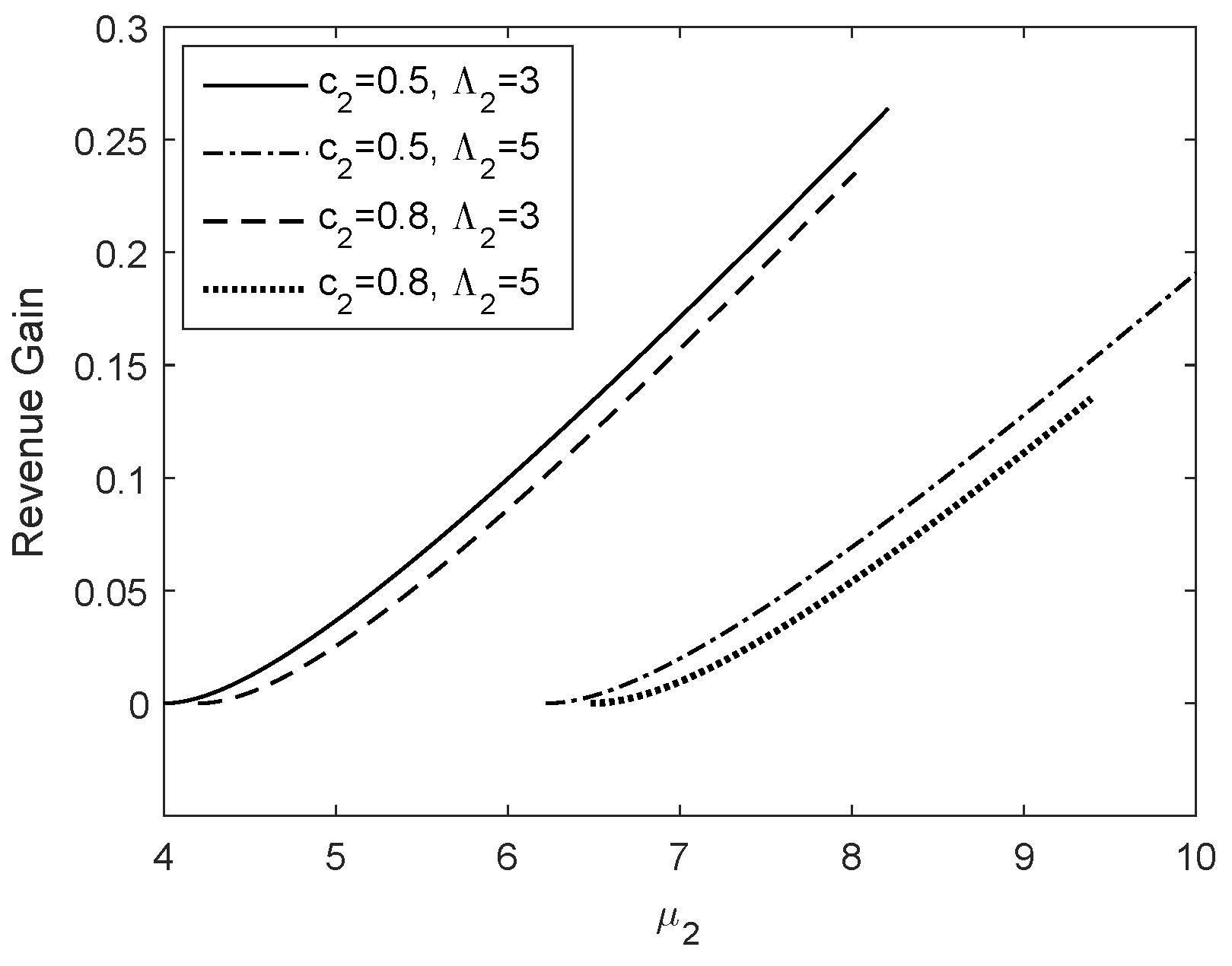
4.1. Total Benefit of Demand Sharing
4.2. Revenue Allocation in the Medical Alliance
5. Conclusions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A. Proof for Proposition 1, Proposition 2 and Lemma 1
- Suppose that , then the optimal pricing strategy is as follows:Additionally, the corresponding actual demand rates are as follows:
- Suppose that , then the optimal prices satisfy the following:Additionally, the corresponding actual demand rates are as follows:
- Suppose that , then the optimal prices satisfy the following:Additionally, the corresponding actual demand rates are as follows:
- Suppose that , then the optimal pricing strategy is Additionally, the corresponding actual demand rate is
- Suppose that , then the optimal price is Additionally, the corresponding actual demand rate is
Appendix B. Proof for Lemma 2, Proposition 3 and Lemma 3
References
- Allen, D. Telemedicine Expanded to Rural China: Across the Divide. Available online: https://emag.medicalexpo.com/telemedicine-expanded-to-rural-china-across-the-divide/ (accessed on 6 October 2022).
- Adi, L.; Yuval, W.; Carroll, J.S.; Paul, B.; dayan Yaron, B. Waiting time is a major predictor of patient satisfaction in a primary military clinic. Mil. Med. 2002, 167, 842. [Google Scholar]
- Grossman, M. On the Concept of Health Capital and the Demand for Health. J. Political Econ. 1972, 80, 223–255. [Google Scholar] [CrossRef] [Green Version]
- Song, H.; Zuo, X.; Cui, C.; Meng, K. The willingness of patients to make the first visit to primary care institutions and its influencing factors in Beijing medical alliances: A comparative study of Beijing’s medical resource-rich and scarce regions. BMC Health Serv. Res. 2019, 19, 361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Lu, Y.; Huang, X. Comparative Study on Medical Cost of Local and Nonlocal Patients in 4 Third Grade First Class Hospitals in Nanjing City. Med. Soc. 2019, 32, 56–59. [Google Scholar]
- Xie, F.; Wang, Y.; Zhang, Q.; Chen, Z.; Gu, S.; Guan, W.; Li, C.; Li, T.; Li, X.; Luo, L.; et al. Development of mental health alliances in China (2017 Edition). J. Hosp. Manag. Health Policy 2018, 2, 37. [Google Scholar] [CrossRef]
- Wang, X. Medical Alliance Launched to Aid Rural Patients. Available online: http://www.chinadaily.com.cn/china/2016-07/27/content_26240288.htm (accessed on 27 July 2016).
- Yang, F.; Yang, Y.; Liao, Z. Evaluation and analysis for Chinese Medical Alliance’s governance structure modes based on Preker-Harding Model. Int. J. Integr. Care 2020, 20, 14. [Google Scholar] [CrossRef]
- Li, L.; Zhang, R.Q. Cooperation through capacity sharing between competing forwarders. Transp. Res. Part E Logist. Transp. Rev. 2015, 75, 115–131. [Google Scholar] [CrossRef]
- Chen, Y.; Zhou, W.; Hua, Z.; Shan, M. Pricing and capacity planning of the referral system with delay-sensitive patients. J. Manag. Sci. China 2015, 18, 73–83. [Google Scholar]
- Anily, S.; Haviv, M. Cooperation in Service Systems. Oper. Res. 2010, 58, 660–673. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.; Benjaafar, S.; Gerchak, Y. Capacity Sharing and Cost Allocation among Independent Firms with Congestion. Prod. Oper. Manag. 2015, 24, 1285–1310. [Google Scholar] [CrossRef]
- Zeng, Y.; Zhang, L.; Cai, X.; Li, J. Cost Sharing for Capacity Transfer in Cooperating Queueing Systems. Prod. Oper. Manag. 2018, 27, 644–662. [Google Scholar] [CrossRef]
- Anily, S.; Haviv, M. Line Balancing in Parallel M/M/1 Lines and Loss Systems as Cooperative Games. Prod. Oper. Manag. 2017, 26, 1568–1584. [Google Scholar] [CrossRef]
- Zhou, Y.P.; Ren, Z.J.; Cochran, J.J.; Cox, L.A.; Keskinocak, P.; Kharoufeh, J.P.; Smith, J.C. Service Outsourcing. In Wiley Encyclopedia of Operations Research and Management Science; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010. [Google Scholar]
- Aksin, O.Z.; de Vericourt, F.; Karaesmen, F. Call Center Outsourcing Contract Analysis and Choice. Manag. Sci. 2008, 54, 354–368. [Google Scholar] [CrossRef]
- Lee, H.H.; Pinker, E.J.; Shumsky, R.A. Outsourcing a Two-Level Service Process. Manag. Sci. 2012, 58, 1569–1584. [Google Scholar] [CrossRef] [Green Version]
- Guo, L.; Wu, X. Capacity Sharing between Competitors. Manag. Sci. 2018, 64, 3554–3573. [Google Scholar] [CrossRef] [Green Version]
- Cetinkaya, E.; Ahn, H.S.; Duenyas, I. Benefits of Collaboration in Capacity Investment and Allocation. Available online: http://dx.doi.org/10.2139/ssrn.2169490 (accessed on 16 September 2012).
- Tang, C.S.; Bai, J.; So, K.C.; Chen, X.M.; Wang, H. Coordinating Supply and Demand on an on-Demand Platform: Price, Wage, and Payout Ratio. Available online: https://ssrn.com/abstract=2831794 (accessed on 20 December 2017).
- Taylor, T. On-Demand Service Platforms. Manuf. Serv. Oper. Manag. 2018, 20, 704–720. [Google Scholar] [CrossRef] [Green Version]
- Naor, P. The Regulation of Queue Size by Levying Tolls. Econometrica 1969, 37, 15–24. [Google Scholar] [CrossRef]
- Levhari, D.; Luski, I. Duopoly pricing and waiting lines. Eur. Econ. Rev. 1978, 11, 17–35. [Google Scholar] [CrossRef]
- Hassin, R. Rational Queueing; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Hassin, R.; Haviv, M. To Queue or Not to Queue: Equilibrium Behavior in Queueing Systems; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2003; Volume 59. [Google Scholar]
- Ghosh, S.; Hassin, R. Inefficiency in stochastic queueing systems with strategic customers. Eur. J. Oper. Res. 2021, 295, 1–11. [Google Scholar] [CrossRef]
- Chen, H.; Frank, M. Monopoly pricing when customers queue. IIE Trans. 2004, 36, 569–581. [Google Scholar] [CrossRef]
- Chen, H.; Wan, Y.W. Price Competition of Make-to-Order Firms. IIE Trans. 2003, 35, 817–832. [Google Scholar] [CrossRef]
- Printezis, A.; Burnetas, A. The effect of discounts on optimal pricing under limited capacity. Int. J. Oper. Res. 2011, 10, 160. [Google Scholar] [CrossRef]
- Suk, T.; Wang, X. Optimal pricing policies for tandem queues: Asymptotic optimality. IISE Trans. 2020, 53, 199–220. [Google Scholar] [CrossRef]
- Canadian Institute for Health Information. Wait Times for Priority Procedures in Canada. Available online: https://www.cihi.ca/en/wait-times-for-priority-procedures-in-canada (accessed on 25 November 2022).
- Hospital Authority. Elective Cataract Surgery. Available online: https://www.ha.org.hk/visitor/ha_visitor_text_index.asp?Parent_ID=214172&Content_ID=214184 (accessed on 30 September 2022).
- Nagarajan, M.; Sošić, G. Game-theoretic analysis of cooperation among supply chain agents: Review and extensions. Eur. J. Oper. Res. 2008, 187, 719–745. [Google Scholar] [CrossRef]
- Muthoo, A. Bargaining Theory with Applications; Cambridge University Press: Cambridg, UK, 1999. [Google Scholar]
- Myerson, R.B. Game Theory: Analysis of Conflict; Harvard University Press: Cambridge, MA, USA, 1991. [Google Scholar]
- Roth, A.E. Axiomatic Models of Bargaining; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012; Volume 170. [Google Scholar]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wen, J. A Stochastic Queueing Model for the Pricing of Time-Sensitive Services in the Demand-Sharing Alliance. Appl. Sci. 2022, 12, 12121. https://doi.org/10.3390/app122312121
Wen J. A Stochastic Queueing Model for the Pricing of Time-Sensitive Services in the Demand-Sharing Alliance. Applied Sciences. 2022; 12(23):12121. https://doi.org/10.3390/app122312121
Chicago/Turabian StyleWen, Jianpei. 2022. "A Stochastic Queueing Model for the Pricing of Time-Sensitive Services in the Demand-Sharing Alliance" Applied Sciences 12, no. 23: 12121. https://doi.org/10.3390/app122312121