
Assessment of Spinal Stability after Discectomy Followed by Annulus Fibrosus Repair and Augmentation of the Nucleus Pulposus: A Finite Element Study

 , ,
, ,
Abstract
:1. Introduction
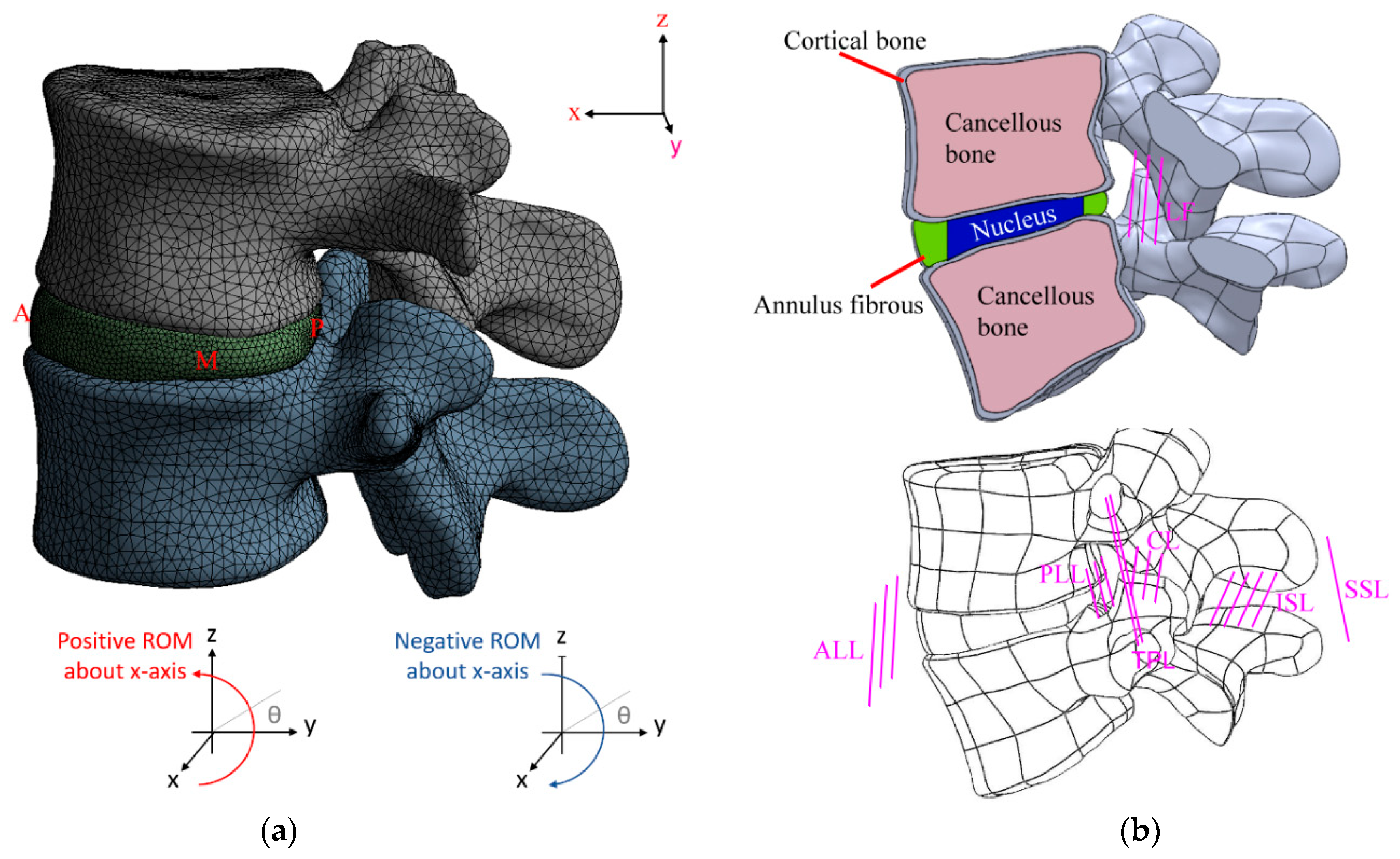
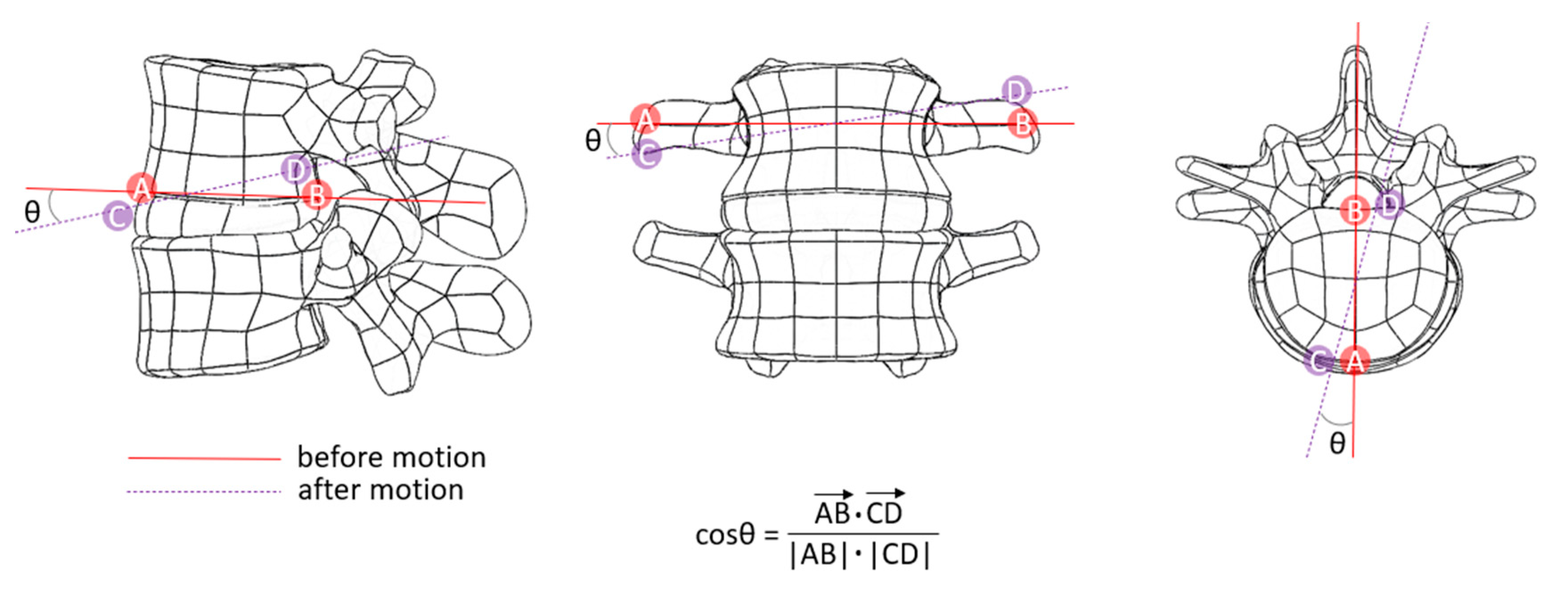
2. Materials and Methods
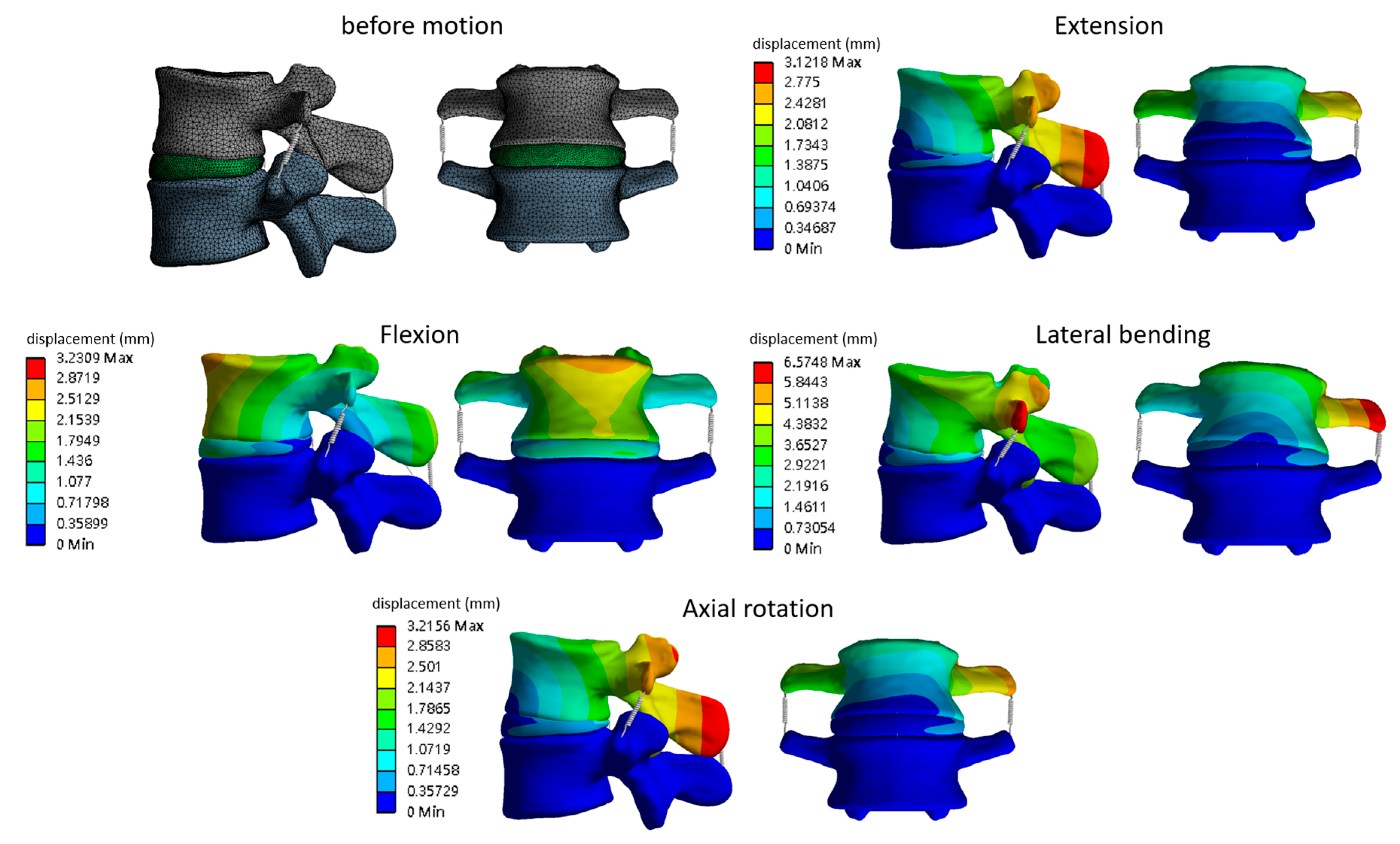
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fjeld, O.R.; Grøvle, L.; Helgeland, J.; Småstuen, M.C.; Solberg, T.K.; Zwart, J.A.; Grotle, M. Complications, Reoperations, Readmissions, and Length of Hospital Stay in 34,639 Surgical Cases of Lumbar Disc Herniation. Bone Joint J. 2019, 101-B, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Gugliotta, M.; da Costa, B.R.; Dabis, E.; Theiler, R.; Jüni, P.; Reichenbach, S.; Landolt, H.; Hasler, P. Surgical versus Conservative Treatment for Lumbar Disc Herniation: A Prospective Cohort Study. BMJ Open 2016, 6, e012938. [Google Scholar] [CrossRef] [Green Version]
- Demirel, A.; Yorubulut, M.; Ergun, N. Regression of Lumbar Disc Herniation by Physiotherapy. Does Non-Surgical Spinal Decompression Therapy Make a Difference? Double-Blind Randomized Controlled Trial. J. Back Musculoskelet Rehabil. 2017, 30, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Choi, Y.; Chung, C.K.; Kim, K.J.; Shin, D.A.; Park, Y.K.; Kwon, W.K.; Yang, S.H.; Lee, C.H.; Park, S.B.; et al. Nonsurgical Treatment Outcomes for Surgical Candidates with Lumbar Disc Herniation: A Comprehensive Cohort Study. Sci. Rep. 2021, 11, 3931. [Google Scholar] [CrossRef] [PubMed]
- Harper, R.; Klineberg, E. The Evidence-Based Approach for Surgical Complications in the Treatment of Lumbar Disc Herniation. Int. Orthop. 2019, 43, 975–980. [Google Scholar] [CrossRef]
- Carragee, E.J.; Spinnickie, A.O.; Alamin, T.F.; Paragioudakis, S. A Prospective Controlled Study of Limited versus Subtotal Posterior Discectomy: Short-Term Outcomes in Patients with Herniated Lumbar Intervertebral Discs and Large Posterior Anular Defect. Spine 2006, 31, 653–657. [Google Scholar] [CrossRef] [PubMed]
- McGirt, M.J.; Eustacchio, S.; Varga, P.; Vilendecic, M.; Trummer, M.; Gorensek, M.; Ledic, D.; Carragee, E.J. A Prospective Cohort Study of Close Interval Computed Tomography and Magnetic Resonance Imaging after Primary Lumbar Discectomy: Factors Associated with Recurrent Disc Herniation and Disc Height Loss. Spine 2009, 34, 2044–2051. [Google Scholar] [CrossRef] [PubMed]
- Lequin, M.B.; Barth, M.; Thomė, C.; Bouma, G.J. Primary Limited Lumbar Discectomy with an Annulus Closure Device: One-Year Clinical and Radiographic Results from a Prospective, Multi-Center Study. Korean J. Spine 2012, 9, 340. [Google Scholar] [CrossRef] [PubMed]
- Ledic, D.; Vukas, D.; Grahovac, G.; Barth, M.; Bouma, G.J.; Vilendecic, M. Effect of Anular Closure on Disk Height Maintenance and Reoperated Recurrent Herniation Following Lumbar Diskectomy: Two-Year Data. J. Neurol. Surg. A Cent Eur. Neurosurg. 2015, 76, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Prado, M.; Mascoli, C.; Giambini, H. Discectomy Decreases Facet Joint Distance and Increases the Instability of the Spine: A Finite Element Study. Comput. Biol. Med. 2022, 143, 105278. [Google Scholar] [CrossRef] [PubMed]
- Skomorac, R.; Delić, J.; Bečulić, H.; Jusić, A. Radiological evaluation of lumbosacral spine for post discectomy segmental instability. Medicinski Glasnik 2016, 13, 142–147. [Google Scholar] [PubMed]
- Tibrewal, S.; Pearcy, M.; Portek, I.; Spivey, J. A Prospective Study of Lumbar Spinal Movements before and after Discectomy Using Biplanar Radiography. Correlation of Clinical and Radiographic Findings. Spine 1985, 10, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.; Tu, K.; Xu, Y.; Zhang, W.; Wang, H.; Wang, D. Effect of Partial Discectomy on the Stability of the Lumbar Spine. A Study of Kinematics. Chin. Med. J. 1990, 103, 396–399. [Google Scholar]
- Guardado, A.A.; Baker, A.; Weightman, A.; Hoyland, J.A.; Cooper, G. Lumbar Intervertebral Disc Herniation: Annular Closure Devices and Key Design Requirements. Bioengineering 2022, 9, 47. [Google Scholar] [CrossRef] [PubMed]
- Cho, P.G.; Shin, D.A.; Park, S.H.; Ji, G.Y. Efficacy of a Novel Annular Closure Device after Lumbar Discectomy in Korean Patients: A 24-Month Follow-Up of a Randomized Controlled Trial. J. Korean Neurosurg. Soc. 2019, 62, 691–699. [Google Scholar] [CrossRef] [Green Version]
- Bailey, A.; Araghi, A.; Blumenthal, S.; Huffmon, G.v. Prospective, Multicenter, Randomized, Controlled Study of Anular Repair in Lumbar Discectomy: Two-Year Follow-Up. Spine 2013, 38, 1161–1169. [Google Scholar] [CrossRef]
- Berlemann, U.; Schwarzenbach, O. An Injectable Nucleus Replacement as an Adjunct to Microdiscectomy: 2 Year Follow-up in a Pilot Clinical Study. Eur. Spine J. 2009, 18, 1706–1712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartlett, A.; Wales, L.; Houfburg, R.; Durfee, W.K.; Griffith, S.L.; Bentley, I. Optimizing the Effectiveness of a Mechanical Suture-Based Anulus Fibrosus Repair Construct in an Acute Failure Laboratory Simulation. J. Spinal Disord. Tech. 2013, 26, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Qi, C.; Yan, X.; Huang, C.; Melerzanov, A.; Du, Y. Biomaterials as carrier, barrier and reactor for cell-based regenerative medicine. Protein Cell 2015, 6, 638–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsantrizos, A.; Ordway, N.R.; Myint, K.; Martz, E.; Yuan, H.A. Mechanical and biomechanical characterization of a polyurethane nucleus replacement device injected and cured in situ within a balloon. SAS J. 2008, 2, 28–39. [Google Scholar] [CrossRef] [Green Version]
- Vanaclocha-Saiz, A.; Vanaclocha, V.; Atienza, C.M.; Clavel, P.; Jorda-Gomez, P.; Barrios, C.; Vanaclocha, L. Finite Element Analysis of a Bionate Ring-Shaped Customized Lumbar Disc Nucleus Prosthesis. ACS Appl. Bio Mater. 2022, 5, 172–182. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Chen, C.H.; Tsuang, F.Y.; Lin, Y.C.; Chiang, C.J.; Kuo, Y.J. The Stability of Long-Segment and Short-Segment Fixation for Treating Severe Burst Fractures at the Thoracolumbar Junction in Osteoporotic Bone: A Finite Element Analysis. PLoS ONE 2019, 14, e0211676. [Google Scholar] [CrossRef] [Green Version]
- Goel, V.K.; Monroe, B.T.; Gilbertson, L.G.; Brinckmann, P. Interlaminar Shear Stresses and Laminae Separation in a Disc: Finite Element Analysis of the L3-L4 Motion Segment Subjected to Axial Compressive Loads. Spine 1995, 20, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.F.; Bayraktar, H.H.; Keaveny, T.M. Trabecular Bone Modulus-Density Relationships Depend on Anatomic Site. J. Biomech. 2003, 36, 897–904. [Google Scholar] [CrossRef]
- Schmidt, H.; Heuer, F.; Drumm, J.; Klezl, Z.; Claes, L.; Wilke, H.J. Application of a Calibration Method Provides More Realistic Results for a Finite Element Model of a Lumbar Spinal Segment. Clin. Biomech. 2007, 22, 377–384. [Google Scholar] [CrossRef]
- Kanyanta, V.; Ivankovic, A. Mechanical Characterisation of Polyurethane Elastomer for Biomedical Applications. J. Mech. Behav. Biomed. Mater. 2010, 3, 51–62. [Google Scholar] [CrossRef]
- Silva, P.; Crozier, S.; Veidt, M.; Pearcy, M.J. An Experimental and Finite Element Poroelastic Creep Response Analysis of an Intervertebral Hydrogel Disc Model in Axial Compression. J. Mater. Sci. Mater. Med. 2005, 16, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.J.; Cheng, C.K.; Sun, J.S.; Liao, C.J.; Wang, Y.H.; Tsuang, Y.H. The Effect of a New Anular Repair after Discectomy in Intervertebral Disc Degeneration: An Experimental Study Using a Porcine Spine Model. Spine 2011, 36, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Dreischarf, M.; Zander, T.; Shirazi-Adl, A.; Puttlitz, C.M.; Adam, C.J.; Chen, C.S.; Goel, V.K.; Kiapour, A.; Kim, Y.H.; Labus, K.M.; et al. Comparison of Eight Published Static Finite Element Models of the Intact Lumbar Spine: Predictive Power of Models Improves When Combined Together. J. Biomech. 2014, 47, 1757–1766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Illien-Jünger, S.; Lu, Y.; Purmessur, D.; Mayer, J.E.; Walter, B.A.; Roughley, P.J.; Qureshi, S.A.; Hecht, A.C.; Iatridis, J.C. Detrimental Effects of Discectomy on Intervertebral Disc Biology Can Be Decelerated by Growth Factor Treatment during Surgery: A Large Animal Organ Culture Model. Spine J. 2014, 14, 2724–2732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariconda, M.; Galasso, O.; Attingenti, P.; Federico, G.; Milano, C. Frequency and Clinical Meaning of Long-Term Degenerative Changes after Lumbar Discectomy Visualized on Imaging Tests. Eur. Spine J. 2009, 19, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Stadelmann, M.A.; Stocker, R.; Maquer, G.; Hoppe, S.; Vermathen, P.; Alkalay, R.N.; Zysset, P.K. Finite Element Models Can Reproduce the Effect of Nucleotomy on the Multi-Axial Compliance of Human Intervertebral Discs. Comput. Methods Biomech. Biomed. Eng. 2020, 23, 934–944. [Google Scholar] [CrossRef]
- Wilke, H.J.; Kavanagh, S.; Neller, S.; Haid, C.; Claes, L.E. Effect of a Prosthetic Disc Nucleus on the Mobility and Disc Height of the L4–5 Intervertebral Disc Postnucleotomy. J. Neurosurg. Spine 2001, 95, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Goel, V.; Goyal, S.; Clark, C.; Nishiyama, K.; Nye, T. Kinematics of the Whole Lumbar Spine: Effect of Discectomy. Spine 1985, 10, 543–554. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Yan, H.; Jian, F.; Wang, X.; Li, H. Numerical Analysis of the Influence of Nucleus Pulposus Removal on the Biomechanical Behavior of a Lumbar Motion Segment. Comput. Methods Biomech. Biomed. Eng. 2015, 18, 1516–1524. [Google Scholar] [CrossRef]
- Cannella, M.; Isaacs, J.L.; Allen, S.; Orana, A.; Vresilovic, E.; Marcolongo, M. Nucleus Implantation: The Biomechanics of Augmentation versus Replacement with Varying Degrees of Nucleotomy. J. Biomech. Eng. 2014, 136, 051001. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Property | Modulus (MPa) | ν | References |
|---|---|---|---|
| Cortical bone | 12,000 | 0.2 | Goel et al., 1995 [23] |
| Cancellous bone | 300 | 0.2 | Morgan et al., 2003 [24] |
| Annulus fibrosus | Mooney-Rivlin c1 = 0.18, c2 = 0.045 | NA | Schmidt et al., 2007 [25] |
| Nucleus pulposus | Mooney-Rivlin c1 = 0.12, c2 = 0.03 | NA | |
| Ligaments | Hyperelastic | NA | |
| Polyurethane elastomer | 4.7 MPa | 0.499 | Kanyanta et al. [26] |
| Hydrogel | 0.45 MPa | 0.2 | Silva et al. [27] |
| Body Position | Compressive Force (N) | Moment (Nm) |
|---|---|---|
| Flexion | 1175 | 7.5 |
| Extension | 500 | 7.5 |
| Lateral bending | 700 | 7.8 |
| Axial rotation | 720 | 5.5 |
| Body Position | Flexion | |||
| ROM about the | ||||
| x-Axis (Degree), ML Direction [% #] | y-Axis (Degree), AP Direction [% #] | z-Axis (Degree) [% #] | FJ Gap * | |
| model a (intact) | −0.7 [undefined] | 3.6 [−21.7%] | 0.0 [0%] | - |
| model b (conservative) | −6.7 [undefined] | 5.1 [10.9%] | 0.0 [0%] | −11.5% |
| model c (aggressive) | −6.7 [undefined] | 5.1 [10.9%] | 0.0 [0%] | −90.5% |
| model d (aggressive with annular repair) | 1.1 [undefined] | 3.4 [−26.1%] | 0.2 [undefined] | −89.4% |
| model e (PU) | −4.5 [undefined] | 4.6 [0%] | 0.3 [undefined] | −40.5% |
| model e (Hydrogel) | −0.7 [undefined] | 3.6 [−21.7%] | 0.0 [0%] | −73.1% |
| Body Position | Extension | |||
| x-Axis (Degree), ML Direction [% #] | y-Axis (Degree), AP Direction [% #] | z-Axis (Degree) [% #] | FJ Gap * | |
| model a (intact) | 0.0 | −2.4 | 0.0 | - |
| model b (conservative) | −0.5 [undefined] | −1.3 [45.8%] | 0.0 [0%] | −13.1% |
| model c (aggressive) | −2.1 [undefined] | −2.1 [12.5%] | 0.0 [0%] | −38.6% |
| model d (aggressive with annular repair) | −2.1 [undefined] | −2.0 [16.7%] | 0.0 [0%] | −37.8% |
| model e (PU) | 0.9 [undefined] | −1.4 [41.7%] | 0.2 [undefined] | −48.0% |
| model e (Hydrogel) | −1.5 [undefined] | −1.8 [25%] | 0.3 [undefined] | −50.5% |
| Body Position | Axial Rotation | |||
| x-Axis (Degree), ML Direction [% #] | y-Axis (Degree), AP Direction [% #] | z-Axis (Degree) [% #] | FJ Gap * | |
| model a (intact) | 0.0 | 0.1 | −1.5 | - |
| model b (conservative) | −0.7 [undefined] | −1.3 [1400%] | −1.6 [−6.7%] | −12.3% |
| model c (aggressive) | −4.2 [undefined] | −0.8 [−900%] | −1.6 [−6.7%] | −90.1% |
| model d (aggressive with annular repair) | −4.2 [undefined] | −0.8 [−900%] | −1.6 [−6.7%] | −89.0% |
| model e (PU) | 0.8 [undefined] | 0.0 [−100%] | −1.4 [6.7%] | −84.5% |
| model e (Hydrogel) | −2.6 [undefined] | −1.0 [−1100%] | −1.2 [20%] | −88.9% |
| Body Position | Lateral Bending | |||
| x-Axis (Degree), ML Direction [% #] | y-Axis (Degree), AP Direction [% #] | z-Axis (Degree) [% #] | FJ Gap * | |
| model a (intact) | −3.3 | −0.2 | −1.2 | - |
| model b (conservative) | −4.6 [−39.4%] | −1.7 [−750%] | −1.2 [0%] | −13.1% |
| model c (aggressive) | −6.4 [−93.9%] | −2.0 [−900%] | −1.2 [0%] | −44.2% |
| model d (aggressive with annular repair) | −6.4 [−93.9%] | −2.0 [−900%] | −1.2 [0%] | −43.3% |
| model e (PU) | −1.2 [63.6%] | 0.2 [200%] | −1.0 [16.7%] | −27.7% |
| model e (Hydrogel) | −5.4 [−63.6%] | −1.7 [−750%] | −0.9 [25%] | −42.6% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, C.-J.; Hsieh, Y.-Y.; Tsuang, F.-Y.; Chiang, Y.-F.; Wu, L.-C. Assessment of Spinal Stability after Discectomy Followed by Annulus Fibrosus Repair and Augmentation of the Nucleus Pulposus: A Finite Element Study. Appl. Sci. 2022, 12, 11906. https://doi.org/10.3390/app122311906
Chiang C-J, Hsieh Y-Y, Tsuang F-Y, Chiang Y-F, Wu L-C. Assessment of Spinal Stability after Discectomy Followed by Annulus Fibrosus Repair and Augmentation of the Nucleus Pulposus: A Finite Element Study. Applied Sciences. 2022; 12(23):11906. https://doi.org/10.3390/app122311906
Chicago/Turabian StyleChiang, Chang-Jung, Yueh-Ying Hsieh, Fon-Yih Tsuang, Yueh-Feng Chiang, and Lien-Chen Wu. 2022. "Assessment of Spinal Stability after Discectomy Followed by Annulus Fibrosus Repair and Augmentation of the Nucleus Pulposus: A Finite Element Study" Applied Sciences 12, no. 23: 11906. https://doi.org/10.3390/app122311906