
Influence and Control of SARS-CoV-2 Transmission under Two Different Models
Abstract
:1. Introduction
2. Model
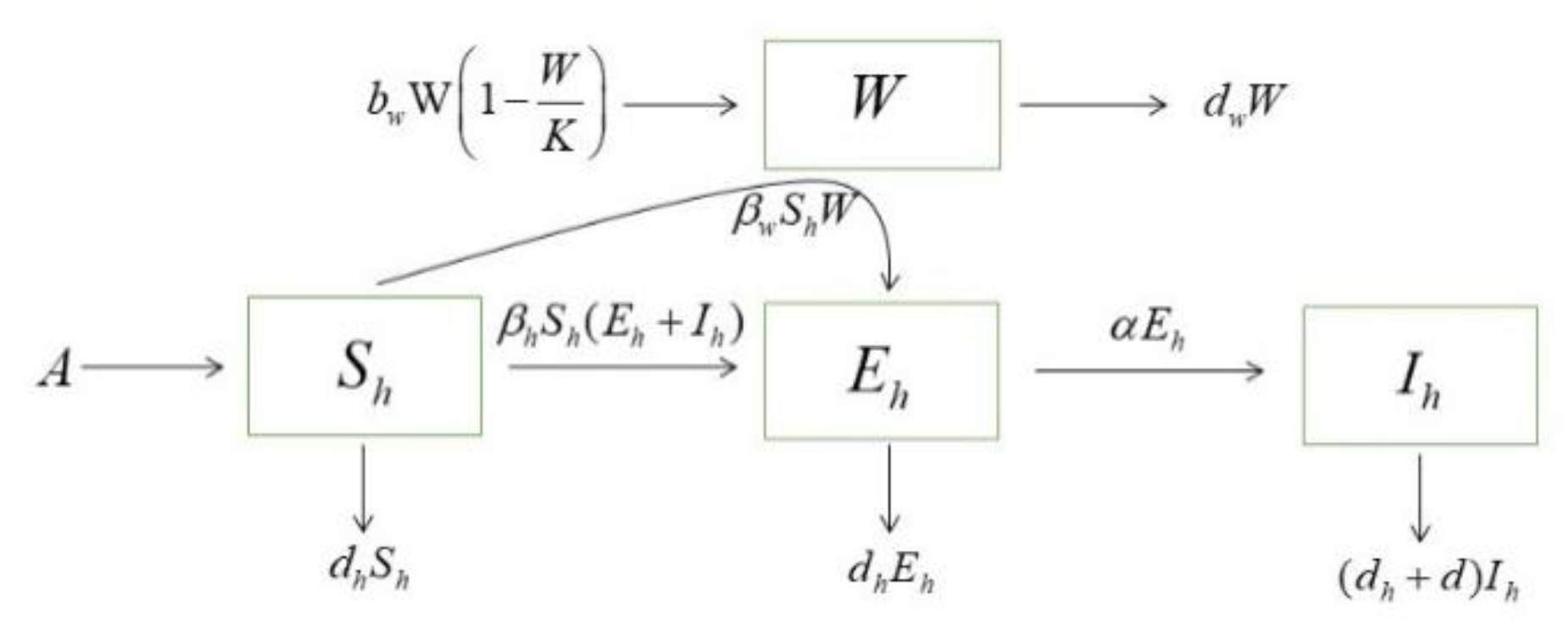
2.1. Direct Transmission Model
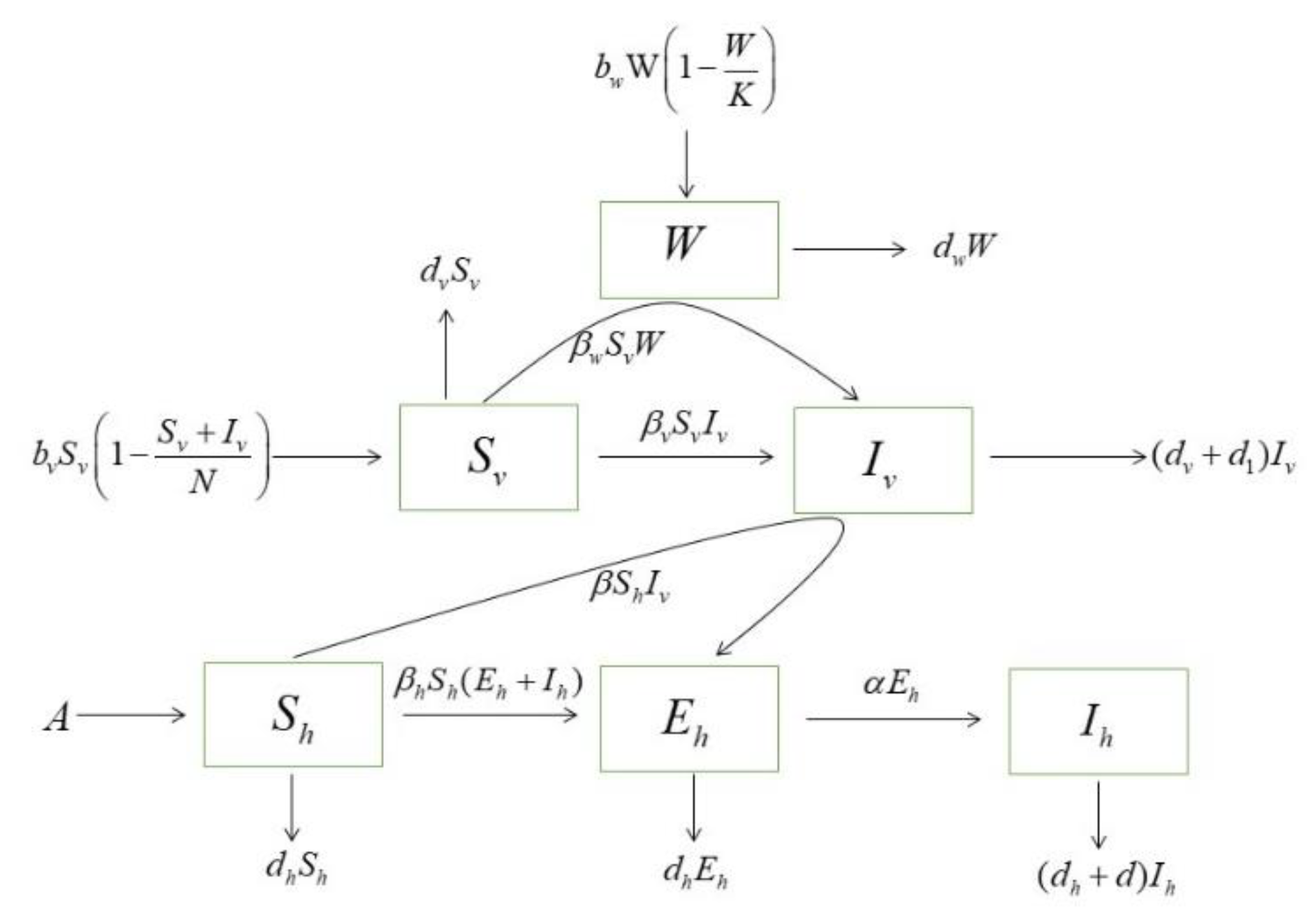
2.2. Indirect Transmission Model
3. Results
3.1. Equilibrium Stability and Basic Reproduction Number
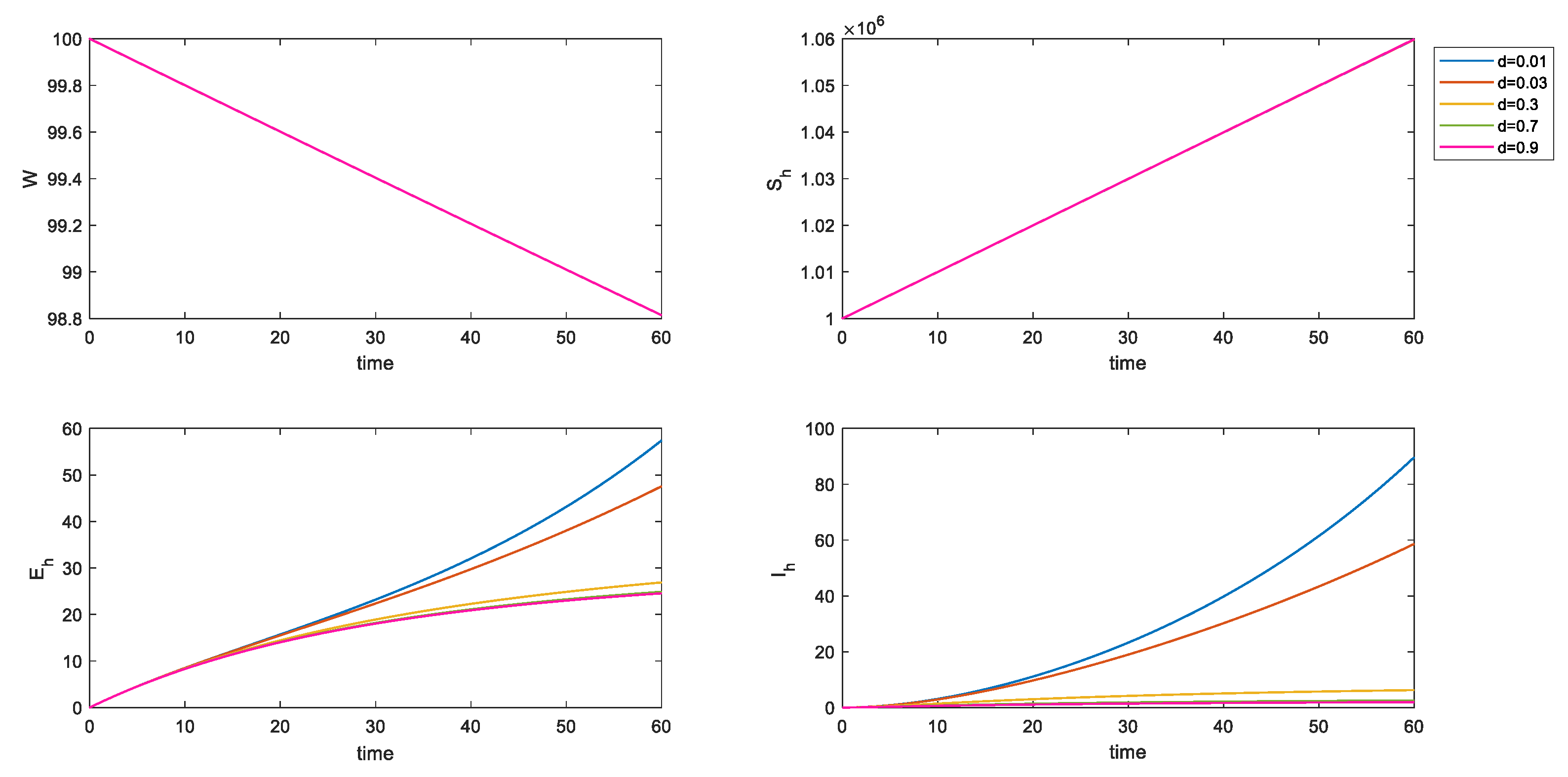
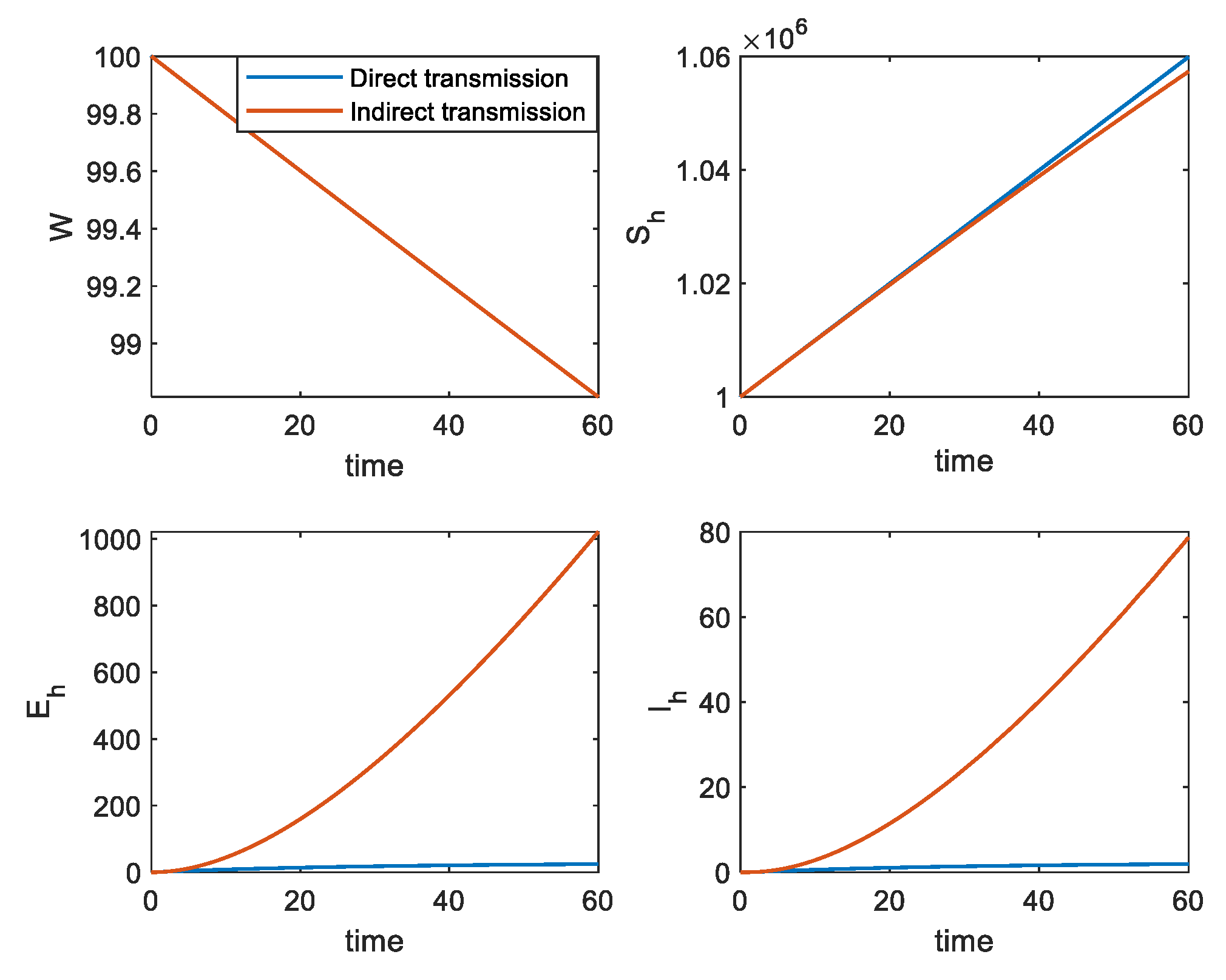
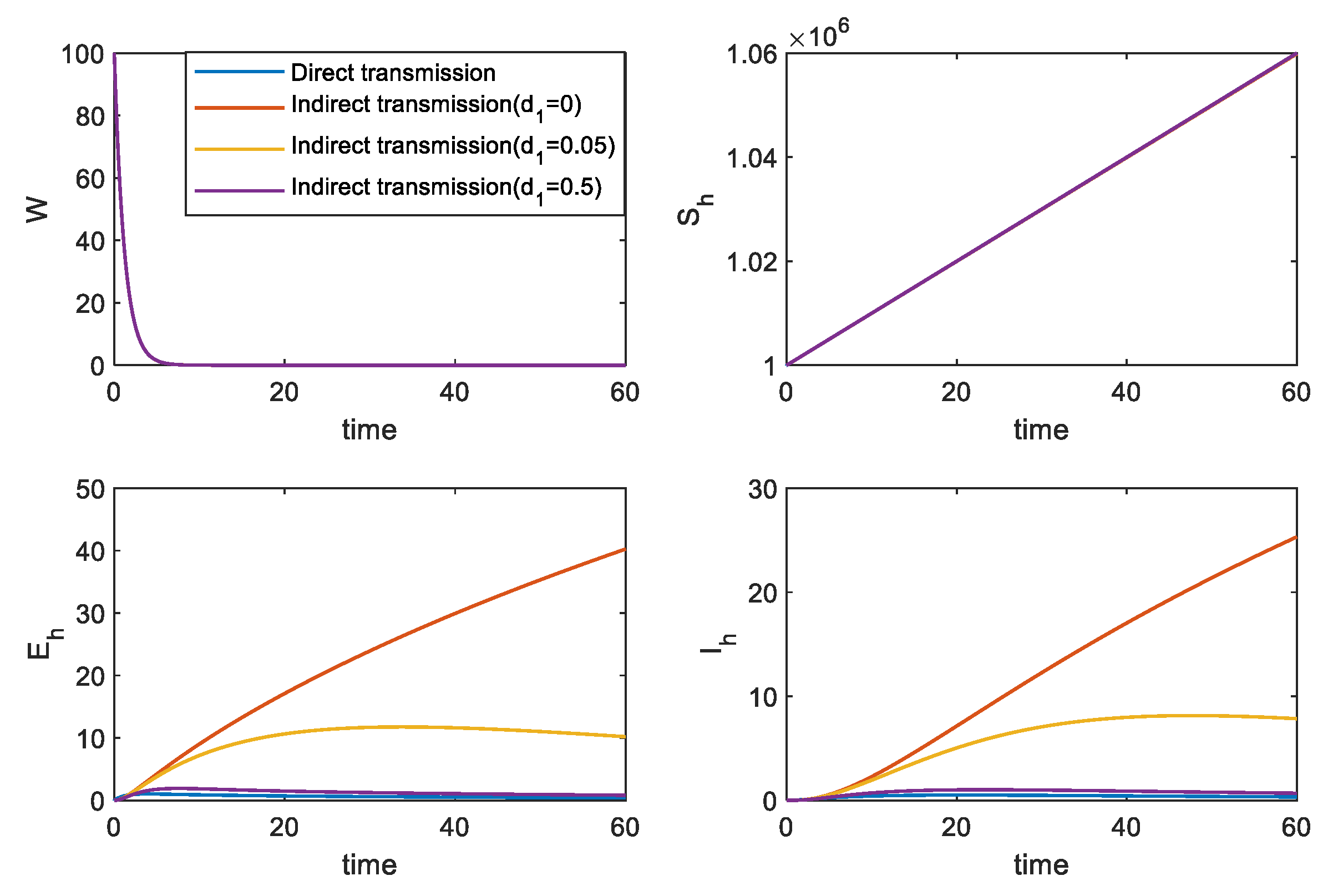
3.2. Numerical Simulation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Cummings, B.E. Potted plants do A review and analysis Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar]
- Abubakr, N.; Salem, Z.A.; Kamel, A.H.M. Oral manifestations in mild-to-moderate cases of COVID-19 viral infection in the adult population. Dent. Med. Probl. 2021, 58, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Han, B.; Wang, J. COVID-19: Gastrointestinal manifestations and potential fecal–oral transmission. Gastroenterology 2020, 158, 1518–1519. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Zhu, J.; Zhang, Z.; Han, Y. A familial cluster of infection associated with the 2019 novel coronavirus indicating possible person-to-person transmission during the incubation period. J. Infect. Dis. 2020, 221, 1757–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.C.; Liao, C.H.; Chang, C.F.; Chou, C.C.; Lin, Y.R. A Locally Transmitted Case of SARS-CoV-2 Infection in Taiwan. N. Engl. J. Med. 2020, 382, 1070–1072. [Google Scholar] [CrossRef] [Green Version]
- Paradowska-Stolarz, A.M. Oral manifestations of COVID-19: Brief review. Dent. Med. Probl. 2021, 58, 123–126. [Google Scholar] [CrossRef]
- Torul, D.; Omezli, M.M. Is saliva a reliable biofluid for the detection of COVID-19? Dent. Med. Probl. 2021, 58, 229–235. [Google Scholar] [CrossRef]
- Rubulotta, F.; Soliman-Aboumarie, H.; Filbey, K. Technologies to optimize the care of severe coronavirus disease 2019 patients for health care providers challenged by limited resources. Anesth. Analgesia. 2020, 131, 351–364. [Google Scholar] [CrossRef]
- Riggioni, C.; Comberiati, P.; Giovannini, M.; Agache, I.; Akdis, M.; Alves-Correia, M.; Antó, J.M.; Arcolaci, A.; Azkur, A.K.; Azkur, D.; et al. A compendium answering 150 questions on COVID-19 and SARS-CoV-2. Allergy 2020, 75, 2503–2541. [Google Scholar] [CrossRef]
- Voinsky, I.; Baristaite, G.; Gurwitz, D. Effects of age and sex on recovery from COVID-19: Analysis of 5769 Israeli patients. J. Infect. 2020, 81, e102–e103. [Google Scholar] [CrossRef]
- Martynowicz, H.; Jodkowska, A.; Poręba, R.; Mazur, G.; Więckiewicz, M. Demographic, clinical, laboratory, and genetic risk factors associated with COVID-19 severity in adults: A narrative review. Dent. Med. Probl. 2021, 58, 115–121. [Google Scholar] [CrossRef]
- Salgotra, R.; Gandomi, M.; Gandomi, A.H. Time series analysis and forecast of the COVID-19 pandemic in India using genetic programming. Chaos Solitons Fractals 2020, 138, 109945. [Google Scholar] [CrossRef]
- Coronavirus WHO. Available online: https://COVID19.who.int/ (accessed on 15 March 2021).
- Lam, S.K.; Kwong, E.W.; Hung, M.S.; Chien, W.T. Investigating the strategies adopted by emergency nurses to address uncertainty and change in the event of emerging infectious diseases: A grounded theory study. Int. J. Environ. Res. Public Health 2020, 17, 2490. [Google Scholar] [CrossRef] [Green Version]
- Cupertino, M.C.; Resende, M.B.; Mayer, N.A.; Carvalho, L.M.; Siqueira-Batista, R. Emerging and re-emerging human infectious diseases: A systematic review of the role of wild animals with a focus on public health impact. Asian Pac. J. Trop. Med. 2020, 13, 99. [Google Scholar] [CrossRef]
- Ambat, A.S.; Vyas, N. Assessment of preparedness against emerging infectious disease among private hospitals in a district of South India. Med. J. Armed Forces India 2022, 78, 42–46. [Google Scholar] [CrossRef]
- Wu, Z.; Yang, L.; Ren, X.; He, G.; Zhang, J.; Yang, J.; Qian, Z.; Dong, J.; Sun, L.; Zhu, Y.; et al. Deciphering the bat virome catalog to better understand the ecological diversity of bat viruses and the bat origin of emerging infectious diseases. ISME J. 2016, 10, 609–620. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Lu, L.; Du, J.; Yang, L.; Ren, X.; Liu, B.; Jiang, J.; Jiang, Y.; Dong, J.; Sun, L.; et al. Comparative analysis of rodent and small mammal viromes to better understand the wildlife origin of emerging infectious diseases. Microbiome 2018, 6, 1–14. [Google Scholar] [CrossRef]
- Rachowicz, L.J.; Hero, J.M.; Alford, R.A.; Taylor, J.W.; Morgan, J.A.T.; Vredenburg, V.T.; Collins, J.P.; Briggs, C.J. The novel and endemic pathogen hypotheses: Competing explanations for the origin of emerging infectious diseases of wildlife. Conserv. Biol. 2005, 19, 1441–1448. [Google Scholar] [CrossRef]
- Oei, W.; Janssen, M.P.; van der Poel, C.L.; van Steenbergen, J.E.; Rehmet, S.; Kretzschmar, M.E. Modeling the transmission risk of emerging infectious diseases through blood transfusion. Transfusion 2013, 53, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- McBryde, E. The value of early transmission dynamic studies in emerging infectious diseases. Lancet Infect. Dis. 2020, 20, 512–513. [Google Scholar] [CrossRef] [Green Version]
- Sarkar, K.; Khajanchi, S.; Nieto, J.J. Modeling and forecasting the COVID-19 pandemic in India. Chaos Solitons Fractals 2020, 139, 110049. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Zeng, Z.; Wang, K.; Wong, S.-S.; Liang, W.; Zanin, M.; Liu, P.; Cao, X.; Gao, Z.; Mai, Z.; et al. Modified SEIR and AI prediction of the epidemics trend of COVID-19 in China under public health interventions. J. Thorac. Dis. 2020, 12, 165. [Google Scholar] [CrossRef]
- Tang, B.; Wang, X.; Li, Q.; Bragazzi, N.L.; Tang, S.; Xiao, Y.; Wu, J. Estimation of the transmission risk of the 2019-nCoV and its implication for public health interventions. J. Clin. Med. 2020, 9, 462. [Google Scholar] [CrossRef] [Green Version]
- Maki, D.G. SARS revisited: The challenge of controlling emerging infectious diseases at the local, regional, federal, and global levels. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2004; Volume 79, pp. 1359–1366. [Google Scholar]
- Brug, J.; Aro, A.R.; Richardus, J.H. Risk Perceptions and Behaviour: Towards Pandemic Control of Emerging Infectious Diseases. Int. J. Behav. Med. 2009, 16, 3–6. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Dong, Y. Dynamic modelling of the impact of public health education on the control of emerging infectious disease. J. Biol. Dyn. 2019, 13, 502–517. [Google Scholar] [CrossRef]
- Pan, Q.; Gao, T.; He, M. Influence of isolation measures for patients with mild symptoms on the spread of COVID-19. Chaos Solitons Fractals 2020, 139, 110022. [Google Scholar] [CrossRef]
- Kumar, S.; Thakur, K.; Sharma, B.; Bhardwaj, T.R.; Prasad, D.N.; Singh, R.K. Recent Advances in Vaccine Development for the Treatment of Emerging Infectious Diseases. Indian J. Pharm. Educ. Res. 2019, 53, 343–354. [Google Scholar] [CrossRef] [Green Version]
- Krause, R.M.; Dimmock, N.J.; Morens, D.M. Summary of antibody workshop: The role of humoral immunity in the treatment and prevention of emerging and extant infectious diseases. J. Infect. Dis. 1997, 176, 549–559. [Google Scholar] [CrossRef] [Green Version]
- Wood, C.S.; Thomas, M.R.; Budd, J.; Mashamba-Thompson, T.; Herbst, K.; Pillay, D.; Peeling, R.W.; Johnson, A.M.; McKendry, R.A.; Stevens, M.M. Taking connected mobile-health diagnostics of infectious diseases to the field. Nature 2019, 566, 467–474. [Google Scholar] [CrossRef]
- Han, P.; Ivanovski, S. Saliva—Friend and foe in the COVID-19 outbreak. Diagnostics 2020, 10, 290. [Google Scholar] [CrossRef]
- Manzar, S.; Kazmi, F.; Shahzad, H.B.; Qureshi, F.A.; Shahbaz, M.; Rashid, S. Estimation of the risk of COVID-19 transmission through aerosol-generating procedures. Dent. Med. Probl. 2022; published ahead of print. [Google Scholar] [CrossRef]
- Meyerowitz, E.A.; Richterman, A.; Gandhi, R.T.; Sax, P.E. Transmission of SARS-CoV-2: A review of viral, host, and environmental factors. Ann. Intern. Med. 2021, 174, 69–79. [Google Scholar] [CrossRef]
- Sun, H.; Lau, A.; Heo, Y.C.; Lin, L.; DeLong, R.; Fok, A. Relationships between tissue properties and operational parameters of a dental handpiece during simulated cavity preparation. J. Dent. Biomech. 2013, 4, 1758736013483747. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.A.; Atangana, A. Modeling the dynamics of novel coronavirus (2019-nCov) with fractional derivative. Alex. Eng. J. 2020, 59, 2379–2389. [Google Scholar] [CrossRef]
- Pei, S.; Kandula, S.; Yang, W.; Shaman, J. Forecasting the spatial transmission of influenza in the United States. Proc. Natl. Acad. Sci. USA 2018, 115, 2752–2757. [Google Scholar] [CrossRef] [Green Version]
- Zhou, D.; Gao, L.; Pan, Q.; He, M. The Impacts of Medical Resources on Emerging Self-Limiting Infectious Diseases. Appl. Sci. 2022, 12, 4255. [Google Scholar] [CrossRef]
- Viana, R.; Moyo, S.; Amoako, D.G.; Tegally, H.; Scheepers, C.; Althaus, C.L.; Anyaneji, U.J.; Bester, P.A.; Boni, M.F.; Chand, M.; et al. Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in southern Africa. Nature 2022, 603, 679–686. [Google Scholar] [CrossRef]
- Shuai, H.; Chan, J.F.W.; Hu, B.; Chai, Y.; Yuen, T.; Yin, F.; Huang, X.; Yoon, C.; Ju, J.-C.; Liu, H.; et al. Attenuated replication and pathogenicity of SARS-CoV-2 B.1.1.529 Omicron. Nature 2022, 603, 693–699. [Google Scholar] [CrossRef]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2). Science 2020, 16, eabb3221. [Google Scholar] [CrossRef]
- Blavatska, V.; Holovatch, Y. Spreading processes in post-epidemic environments. Phys. A Stat. Mech. Appl. 2021, 573, 125980. [Google Scholar] [CrossRef]
- Lu, L.; Quintela, I.; Lin, C.; Lin, T.-C.; Lin, C.-H.; Wu, V.C.H.; Lin, C.-S. A review of epidemic investigation on cold-chain food-mediated SARS-CoV-2 transmission and food safety consideration during COVID-19 pandemic. J. Food Saf. 2021, 41, e12932. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.I.P.; Hsu, L.Y.; Cook, A.R.; Yap, J.C.H. COVID-19 Containment Measures. In Uncovering the Science Of COVID-19; World Scientific: Singapore, 2022; pp. 147–203. [Google Scholar]
- Checchi, V.; Bellini, P.; Bencivenni, D.; Consolo, U. COVID-19 dentistry-related aspects: A literature overview. Int. Dent. J. 2021, 71, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Dziedzic, A.; Wojtyczka, R. The impact of coronavirus infectious disease 19 (COVID-19) on oral health. Oral Dis. 2021, 27, 703–706. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Definitions | Value | Unit |
|---|---|---|---|
| Carrying capacity of pathogenic population | Quantity | ||
| Incidence rate of pathogenic population | Day−1 | ||
| Removal rate of pathogenic population | Day−1 | ||
| Recruitment rate of human | Quantity | ||
| Removal rate of humans | Day−1 | ||
| Transmission rate among human | Day−1 | ||
| Transmission rate from pathogenic population to human | Day−1 | ||
| Average latency period | Dimensionless | ||
| Removal rate of infected human | Day−1 | ||
| Carrying capacity of inanimate-mediated | Quantity | ||
| Transmission rate among inanimate-mediated | Day−1 | ||
| The growth rate of inanimate-mediated | Day−1 | ||
| Removal rate of inanimate-mediated | Day−1 | ||
| Disinfection rate | Day−1 | ||
| Transmission rate from inanimate-mediated to human | Day−1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, X.; Chen, S.; Pan, Q.; He, M.; Qu, L. Influence and Control of SARS-CoV-2 Transmission under Two Different Models. Appl. Sci. 2022, 12, 11849. https://doi.org/10.3390/app122211849
Gao X, Chen S, Pan Q, He M, Qu L. Influence and Control of SARS-CoV-2 Transmission under Two Different Models. Applied Sciences. 2022; 12(22):11849. https://doi.org/10.3390/app122211849
Chicago/Turabian StyleGao, Xubin, Shuang Chen, Qiuhui Pan, Mingfeng He, and Leilei Qu. 2022. "Influence and Control of SARS-CoV-2 Transmission under Two Different Models" Applied Sciences 12, no. 22: 11849. https://doi.org/10.3390/app122211849