
Reciprocating System for Secondary Root Canal Treatment of Oval Canals: CBCT, X-rays for Remnant Detection and Their Identification with ESEM and EDX


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection and Preparation
2.2. First Root Canal Treatment
2.3. Root Canal Filling Procedures
2.4. Secondary Root Canal Treatment
2.5. Radiographic Evaluation
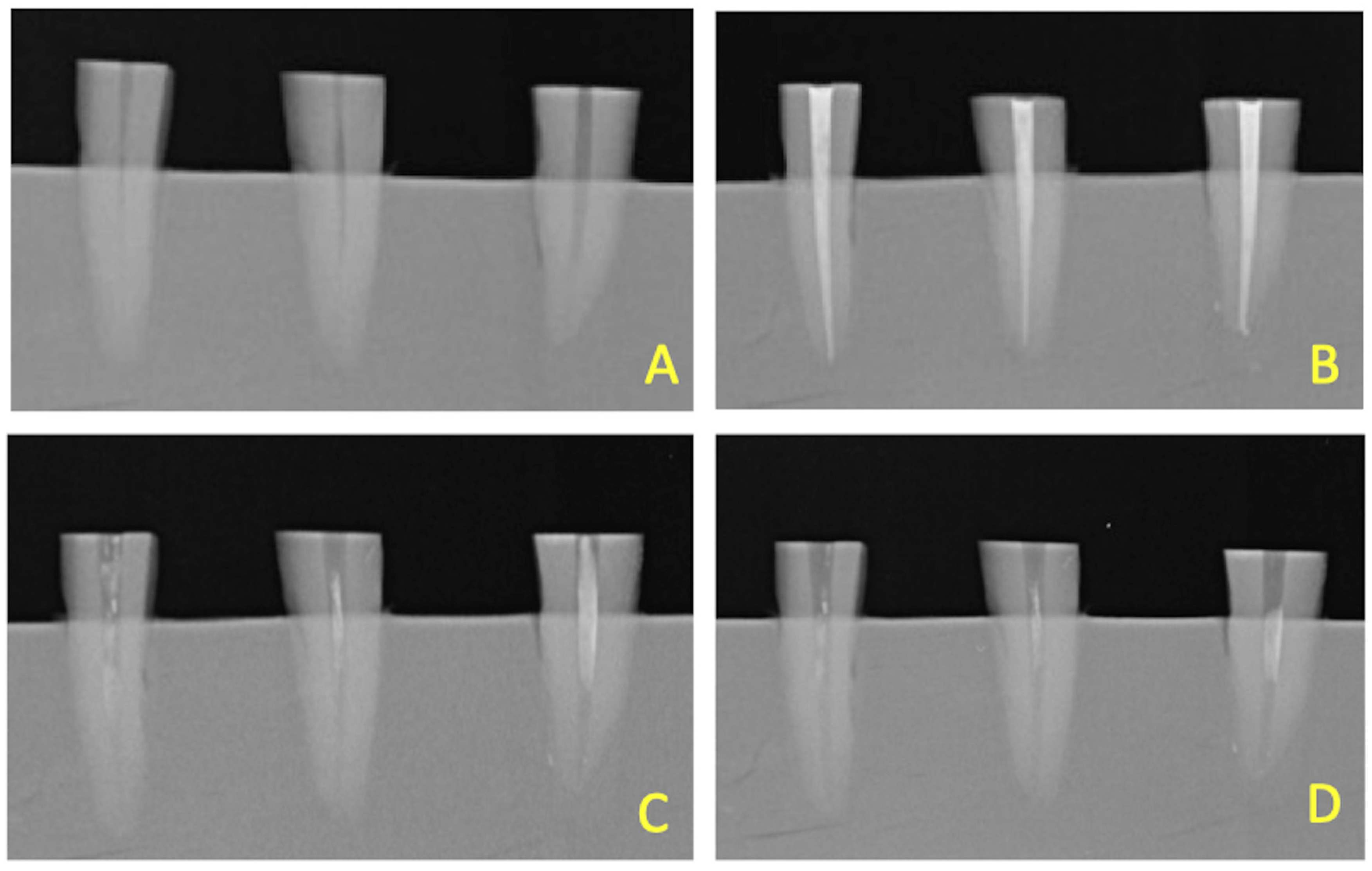
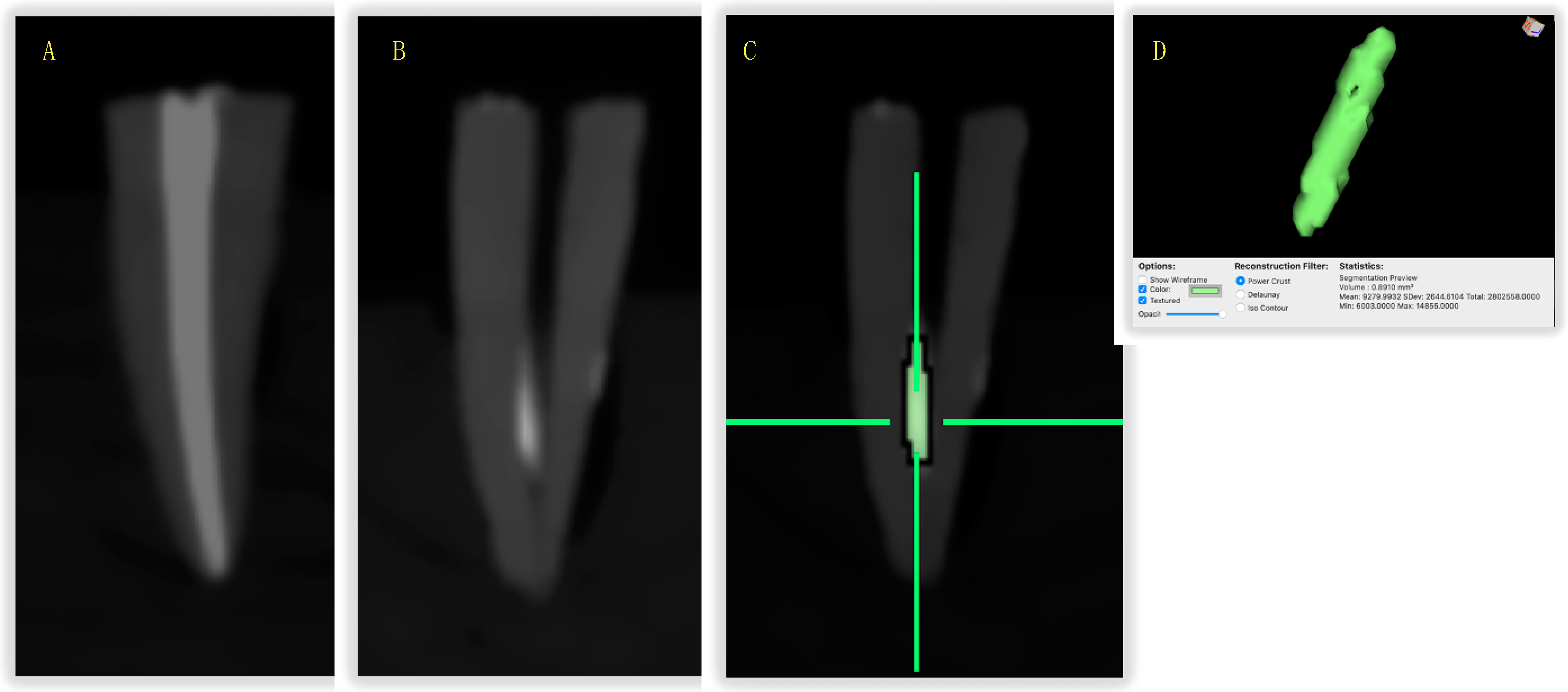
2.6. CBCT Evaluation
2.7. ESEM-EDX Evaluation
2.8. Statistical Analysis
3. Results
3.1. Time to Complete SRCTs
3.2. Assessment of Intracanal Remnants: X-rays and CBCT
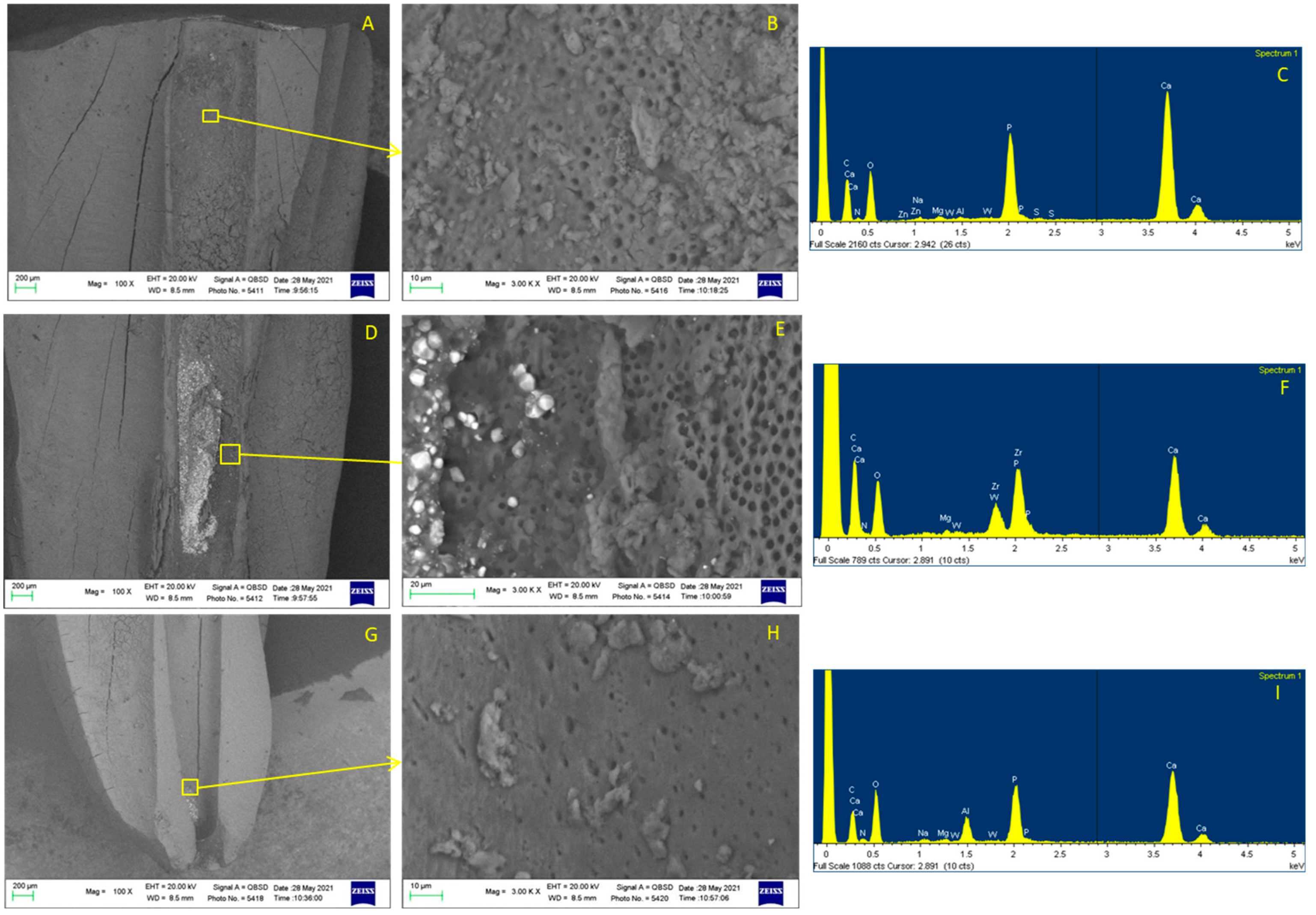
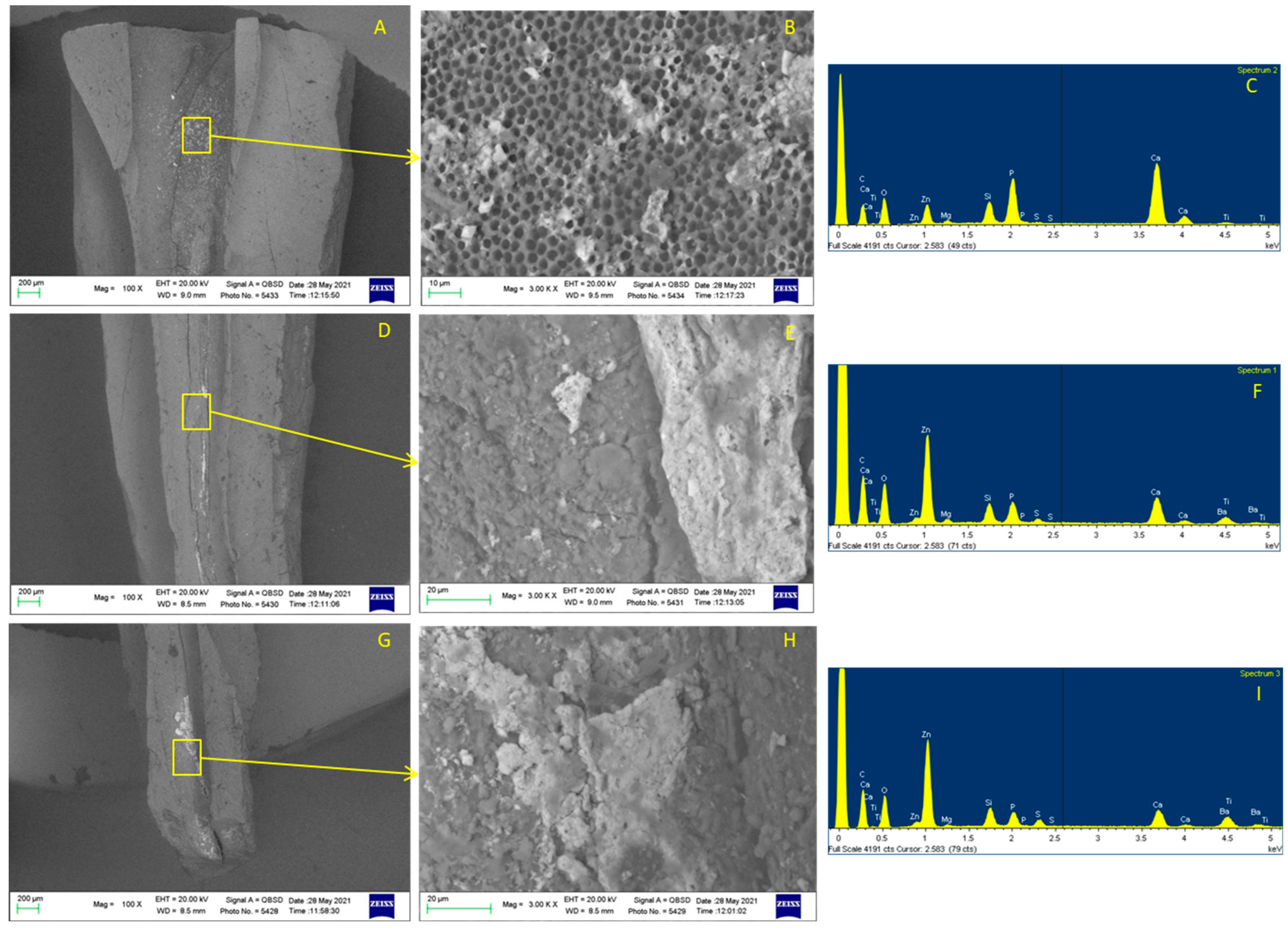
3.3. ESEM-EDX Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nair, P.N.R. On the causes of persistent apical periodontitis: A review. Int. Endod. J. 2006, 39, 249–281. [Google Scholar] [CrossRef]
- Rôças, I.N.; Hülsmann, M.; Siqueira, J.F., Jr. Microorganisms in Root Canal-treated Teeth from a German Population. J. Endod. 2008, 34, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D.; Siqueira, J.F., Jr. Biofilms and apical periodontitis: Study of prevalence and association with clinical and histopathologic findings. J. Endod. 2010, 36, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr. Aetiology of root canal treatment failure: Why well-treated teeth can fail. Int. Endod. J. 2001, 34, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, Y.L.; Mann, V.; Gulabivala, K. Outcome of secondary root canal treatment: A systematic review of the literature. Int. Endod. J. 2008, 41, 1026–1046. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Alves, F.R.; Almeida, B.M.; de Oliveira, J.C.M.; Rôças, I.N. Ability of chemomechanical preparation with either rotary instruments or self-adjusting file to disinfect oval-shaped root canals. J. Endod. 2010, 36, 1860–1865. [Google Scholar] [CrossRef]
- Hülsmann, M.; Bluhm, V. Efficacy, cleaning ability and safety of different rotary NiTi instruments in root canal retreatment. Int. Endod. J. 2004, 37, 468–476. [Google Scholar] [CrossRef]
- Somma, F.; Cammarota, G.; Plotino, G.; Grande, N.M.; Pameijer, C.H. The Effectiveness of Manual and Mechanical Instrumentation for the Retreatment of Three Different Root Canal Filling Materials. J. Endod. 2008, 34, 466–469. [Google Scholar] [CrossRef]
- Kfir, A.; Tsesis, I.; Yakirevich, E.; Matalon, S.; Abramovitz, I. The efficacy of five techniques for removing root filling material: Microscopic versus radiographic evaluation. Int. Endod. J. 2012, 45, 35–41. [Google Scholar] [CrossRef]
- Prati, C.; Zamparini, F.; Spinelli, A.; Pelliccioni, G.A.; Pirani, C.; Gandolfi, M.G. Secondary Root Canal Treatment with Reciproc Blue and K-File: Radiographic and ESEM-EDX Analysis of Dentin and Root Canal Filling Remnants. J. Clin. Med. 2020, 9, 1902. [Google Scholar] [CrossRef]
- Peters, O.A. Current challenges and concepts in the preparation of root canal systems: A review. J. Endod. 2004, 30, 559–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, M.P.; Duarte, M.A.; Cavenago, B.C.; Kato, A.S.; da Silveira Bueno, C.E. Effectiveness of the ProTaper Next and Reciproc Systems in Removing Root Canal Filling Material with Sonic or Ultrasonic Irrigation: A Micro-computed Tomographic Study. J. Endod. 2017, 43, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, L.S.; Gomes, C.C.; Marceliano-Alves, M.F.; Cunha, R.S.; Provenzano, J.C.; Siqueira, J.F., Jr. Preparation of Oval-shaped Canals with TRUShape and Reciproc Systems: A Micro-Computed Tomography Study Using Contralateral Premolars. J. Endod. 2017, 43, 1018–1022. [Google Scholar] [CrossRef]
- Ferreira, F.; Adeodato, C.; Barbosa, I.; Aboud, L.; Scelza, P.; Zaccaro Scelza, M. Movement kinematics and cyclic fatigue of NiTi rotary instruments: A systematic review. Int. Endod. J. 2017, 50, 143–152. [Google Scholar] [CrossRef]
- Ball, R.L.; Barbizam, J.V.; Cohenca, N. Intraoperative endodontic applications of cone beam computed tomography. J. Endod. 2013, 39, 548–557. [Google Scholar] [CrossRef]
- Schropp, L.; Kirkevang, L.L. Accuracy and Reliability of Intraoral Radiographs in Determining the Cleanliness of Root Canals after Endodontic Retreatment. Eur. Endod. J. 2017, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Baxter, S.; Schöler, C.; Dullin, C.; Hülsmann, M. Sensitivity of conventional radiographs and cone-beam computed tomography in detecting the remaining root-canal filling material. J. Oral. Sci. 2020, 62, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, E.; Schrenker, C.; Zupanc, J.; Bürklein, S. Percentage of Gutta-percha Filled Areas in Canals Obturated with Cross-linked Gutta-percha Core-carrier Systems, Single-Cone and Lateral Compaction Technique. J. Endod. 2016, 42, 294–298. [Google Scholar] [CrossRef]
- Pérez-Alfayate, R.; Mercade, M.; Algar-Pinilla, J.; Cisneros-Cabello, R.; Foschi, F.; Cohen, S. Root Canal Filling Quality Comparison of a Premixed Calcium Silicate Endodontic Sealer and Different Carrier-Based Obturation Systems. J. Clin. Med. 2021, 10, 1271. [Google Scholar] [CrossRef]
- Nagendrababu, V.; Murray, P.E.; Ordinola-Zapata, R.; Peters, O.A.; Rôças, I.N.; Siqueira, J.F., Jr.; Priya, E.; Jayaraman, J.; Pulikkotil, S.J.; Camilleri, J.; et al. PRILE 2021 guidelines for reporting laboratory studies in Endodontology: A consensus-based development. Int. Endod. J. 2021, 54, 1482–1490. [Google Scholar] [CrossRef]
- Pirani, C.; Pelliccioni, G.A.; Marchionni, S.; Montebugnoli, L.; Piana, G.; Prati, C. Effectiveness of Three Different Retreatment Techniques in Canals Filled With Compacted Gutta-Percha or Thermafil: A Scanning Electron Microscope Study. J. Endod. 2009, 35, 1433–1440. [Google Scholar] [CrossRef] [PubMed]
- Rödig, T.; Reicherts, P.; Konietschke, F.; Dullin, C.; Hahn, W.; Hülsmann, M. Efficacy of reciprocating and rotary NiTi instruments for retreatment of curved root canals assessed by micro-CT. Int. Endod. J. 2014, 47, 942–948. [Google Scholar] [CrossRef]
- Bago, I.; Plotino, G.; Katić, M.; Ročan, M.; Batinić, M.; Anić, I. Evaluation of filling material remnants after basic preparation, apical enlargement and final irrigation in retreatment of severely curved root canals in extracted teeth. Int. Endod. J 2020, 53, 962–973. [Google Scholar] [CrossRef] [PubMed]
- Alves, F.R.F.; Rôças, I.N.; Provenzano, J.C.; Siqueira, J.F., Jr. Removal of the Previous Root Canal Filling Material for Retreatment: Implications and Techniques. Appl. Sci. 2022, 12, 10217. [Google Scholar] [CrossRef]
- Pirani, C.; Iacono, F.; Chersoni, S.; Sword, J.; Pashley, D.H.; Tay, F.R.; Looney, S.; Gandolfi, M.G.; Prati, C. The effect of ultrasonic removal of various root-end filling materials. Int. Endod. J. 2009, 42, 1015–1025. [Google Scholar] [CrossRef]
- Keleş, A.; Şimşek, N.; Alçin, H.; Ahmetoglu, F.; Yologlu, S. Retreatment of flat-oval root canals with a self-adjusting file: An SEM study. Dent. Mater J. 2014, 33, 786–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scelza, M.F.; Coil, J.M.; Maciel, A.C.; Oliveira, L.R.; Scelza, P. Comparative SEM evaluation of three solvents used in endodontic retreatment: An ex vivo study. J. Appl. Oral. Sci. 2008, 16, 24–29. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, I.; Pina-Vaz, I. The Novel Role of Solvents in Non-Surgical Endodontic Retreatment. Appl. Sci. 2022, 12, 5492. [Google Scholar] [CrossRef]
- Hülsmann, M.; Rümmelin, C.; Schäfers, F. Root canal cleanliness after preparation with different endodontic handpieces and hand instruments: A comparative SEM investigation. J. Endod. 1997, 23, 301–306. [Google Scholar] [CrossRef]
- Prati, C.; Foschi, F.; Nucci, C.; Montebugnoli, L.; Marchionni, S. Appearance of the root canal walls after preparation with NiTi rotary instruments: A comparative SEM investigation. Clin. Oral. Investig. 2004, 8, 102–110. [Google Scholar] [CrossRef]
- Love, R.M. Bacterial adhesins--their role in tubule invasion and endodontic disease. Austral. Endod. J. 2002, 28, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.R.; Siqueira, J.F., Jr.; Ricucci, D.; Lopes, W.S. Dentinal tubule infection as the cause of recurrent disease and late endodontic treatment failure: A case report. J. Endod. 2012, 38, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Brown, J.; Semper, M.; Abella, F.; Mannocci, F. European Society of Endodontology position statement: Use of cone beam computed tomography in Endodontics: European Society of Endodontology (ESE) developed by. Int. Endod. J. 2019, 52, 1675–1678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohenca, N.; Shemesh, H. Clinical applications of cone beam computed tomography in endodontics: A comprehensive review. Quintessence Int. 2015, 46, 657–668. [Google Scholar] [PubMed]
- Di Nardo, D.; Zanza, A.; Pagnoni, F.; Xhajanka, E.; Testarelli, L. An Update on Advanced Diagnostic Imaging in Dentistry. Diagnostics 2022, 12, 1041. [Google Scholar] [CrossRef]
- Bago, I.; Suk, M.; Katic, M.; Gabric, D.; Anic, I. Comparison of the effectiveness of various rotary and reciprocating systems with different surface treatments to remove gutta-percha and an epoxy resin-based sealer from straight root canals. Int. Endod. J. 2019, 52, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Keleş, A.; Arslan, H.; Kamalak, A.; Akçay, M.; Sousa-Neto, M.D.; Versiani, M.A. Removal of filling materials from oval-shaped canals using laser irradiation: A micro-computed tomographic study. J. Endod. 2015, 41, 219–224. [Google Scholar] [CrossRef]
- Ajina, M.A.; Shah, P.K.; Chong, B.S. Critical analysis of research methods and experimental models to study removal of root filling materials. Int. Endod. J. 2022, 55, 119–152. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | SRCT #25 Time | SRCT #40 Time |
|---|---|---|
| SC Group (n = 32) | 7.02 ± 1.10 | 1.18 ± 0.53 |
| GF Group (n = 32) | 8.22 ± 1.20 | 2.00 ± 1.10 |
| Group | Preoperative | Post-Treatment | SRCT #25 | SRCT #40 |
|---|---|---|---|---|
| AHPlus/SingleCone (n = 32) | 4.87 ± 0.65 | 7.11 ± 0.78 (+46%) | 7.94 ± 0.63 (+12%) | 8.53 ± 0.65 (+8%) |
| AHPlus/GuttaFusion (n = 32) | 4.82 ± 0.61 | 6.97 ± 0.81 (+45%) | 7.98 ± 0.60 (+14%) | 8.61 ± 0.61 (+8%) |
| SC Group (n = 32) | GF Group (n = 32) | |||
|---|---|---|---|---|
| Canal Third | Area (mm2) | Volume (mm3) | Area (mm2) | Volume (mm3) |
| Coronal | 0.17 ± 0.29 a | 0.21 ± 0.25 a | 0.14 ± 0.21 a | 0.17 ± 0.35 a |
| Middle | 0.44 ± 0.38 b | 0.46 ± 0.61 b | 0.62 ± 0.49 b | 0.56 ± 0.78 b |
| Apical | 0.23 ± 0.20 a | 0.17 ± 0.28 a | 0.28 ± 0.25 a | 0.23 ± 0.36 a |
| Total | 0.83 ± 0.66 | 0.85 ± 0.85 | 1.03 ± 0.70 | 0.97 ± 1.19 |
| Apical Third Area | Middle Third Area | Coronal Third Area | Total Area | ||
|---|---|---|---|---|---|
| Apical Third Volume | Pearson correlation | 0.516 | 0.404 | 0.137 | 0.493 |
| p value | 0.0001 | 0.002 | 0.172 | 0.0001 | |
| N | 32 | 32 | 32 | 32 | |
| Middle Third Volume | Pearson correlation | 0.270 | 0.586 | 0.322 | 0.594 |
| p value | 0.028 | 0.0001 | 0.014 | 0.0001 | |
| N | 32 | 32 | 32 | 32 | |
| Coronal Third Volume | Pearson correlation | −0.087 | 0.133 | 0.651 | 0.262 |
| p value | 0.277 | 0.182 | 0.0001 | 0.034 | |
| N | 32 | 32 | 32 | 32 | |
| Total Volume | Pearson correlation | 0.290 | 0.575 | 0.473 | 0.678 |
| p value | 0.018 | 0.0001 | 0.0001 | 0.0001 | |
| N | 32 | 32 | 32 | 32 | |
| Apical Third Area | Middle Third Area | Coronal Third Area | Total Area | ||
| Apical Third Volume | Pearson correlation | 0.145 | 0.420 | 0.352 | 0.458 |
| p value | 0.226 | 0.012 | 0.030 | 0.006 | |
| N | 32 | 32 | 32 | 32 | |
| Middle Third Volume | Pearson correlation | 0.021 | 0.619 | 0.597 | 0.629 |
| p value | 0.457 | 0.0001 | 0.0001 | 0.0001 | |
| N | 32 | 32 | 32 | 32 | |
| Coronal Third Volume | Pearson correlation | −0.125 | 0.199 | 0.595 | 0.280 |
| p value | 0.260 | 0.150 | 0.0001 | 0.071 | |
| N | 32 | 32 | 32 | 32 | |
| Total (Volume) | Pearson correlation | 0.022 | 0.591 | 0.670 | 0.631 |
| p value | 0.456 | 0.000 | 0.000 | 0.0001 | |
| N | 32 | 32 | 32 | 32 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spinelli, A.; Zamparini, F.; Buonavoglia, A.; Pisi, P.; Gandolfi, M.G.; Prati, C. Reciprocating System for Secondary Root Canal Treatment of Oval Canals: CBCT, X-rays for Remnant Detection and Their Identification with ESEM and EDX. Appl. Sci. 2022, 12, 11671. https://doi.org/10.3390/app122211671
Spinelli A, Zamparini F, Buonavoglia A, Pisi P, Gandolfi MG, Prati C. Reciprocating System for Secondary Root Canal Treatment of Oval Canals: CBCT, X-rays for Remnant Detection and Their Identification with ESEM and EDX. Applied Sciences. 2022; 12(22):11671. https://doi.org/10.3390/app122211671
Chicago/Turabian StyleSpinelli, Andrea, Fausto Zamparini, Alessio Buonavoglia, Paolo Pisi, Maria Giovanna Gandolfi, and Carlo Prati. 2022. "Reciprocating System for Secondary Root Canal Treatment of Oval Canals: CBCT, X-rays for Remnant Detection and Their Identification with ESEM and EDX" Applied Sciences 12, no. 22: 11671. https://doi.org/10.3390/app122211671