

Simvastatin Embedded into Poly(Lactic-Co-Glycolic Acid)-Based Scaffolds in Promoting Preclinical Bone Regeneration: A Systematic Review
 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Information Sources
2.5. Study Selection
2.6. Data Collection Process
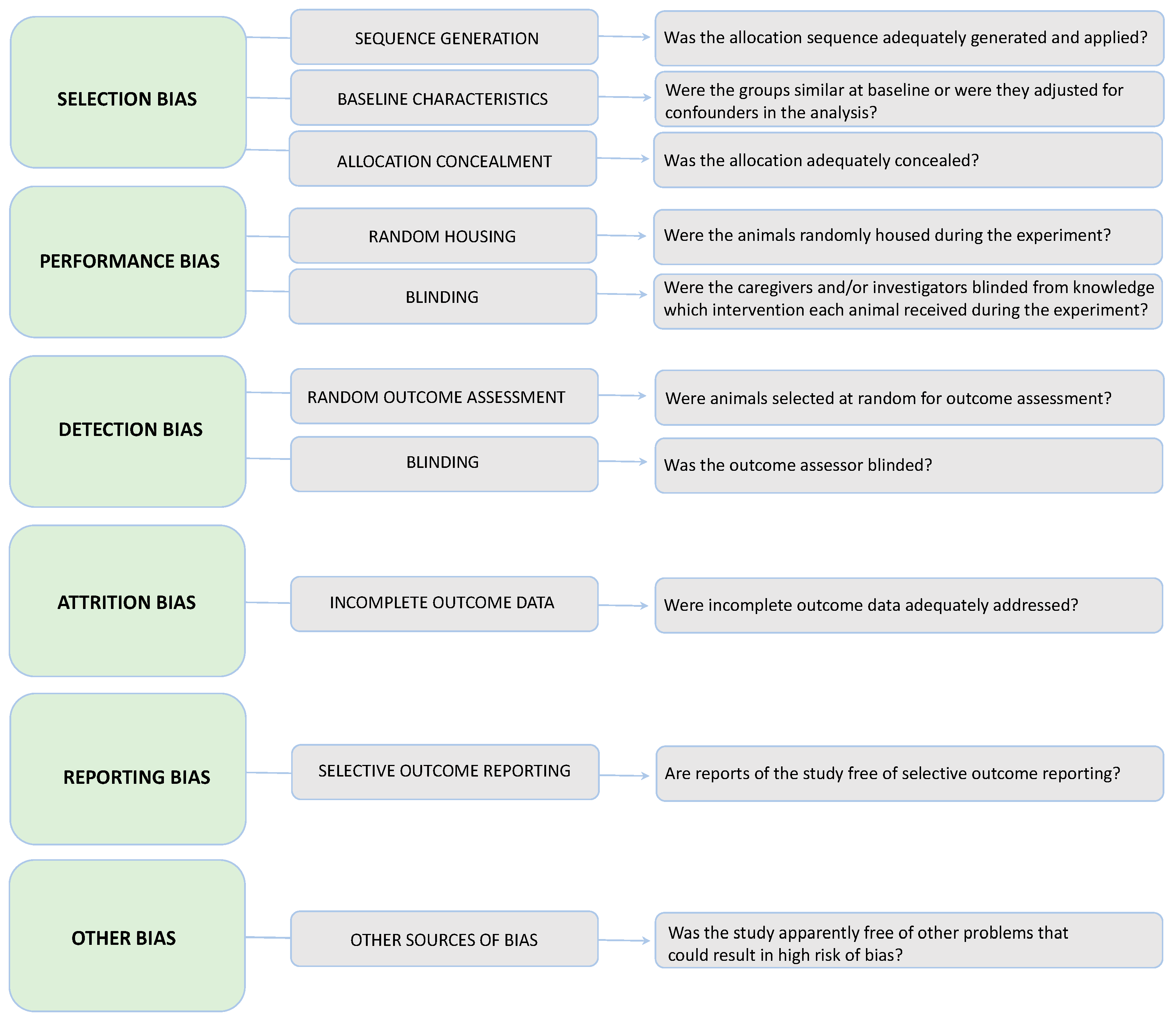
2.7. Quality and Risk of Bias Assessment
2.8. Summary Measures
2.9. Synthesis of Results
3. Results
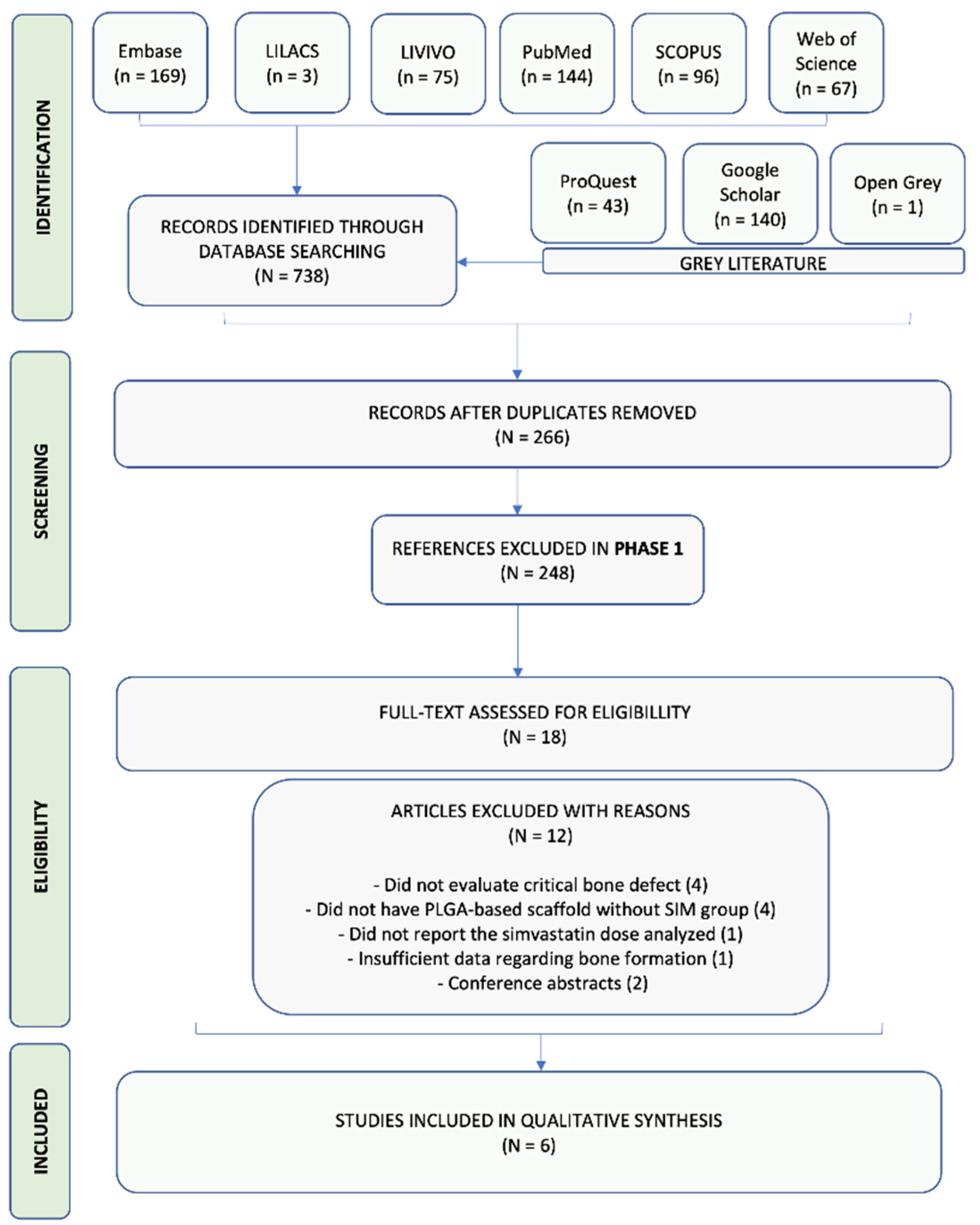
3.1. Study Selection
3.2. Study Characteristics
- (1)
- Sequence generation (Was the allocation sequence adequately generated and applied?).
- (2)
- Baseline characteristics (Were all the animals similar at baseline [age, sex, weight]?).
- (3)
- Allocation concealment (Was the allocation adequately concealed?).
- (4)
- Random housing (Were the animals randomly housed during the experiment?).
- (5)
- Blinding (Were the caregivers and/or investigators blinded from knowledge which intervention each animal received during the experiment?).
- (6)
- Random outcome assessment (Were animals selected at random for outcome assessment?).
- (7)
- Blinding (Was the outcome assessor blinded?).
- (8)
- Incomplete outcome data (Were incomplete outcome data adequately addressed?).
- (9)
- Selective outcome reporting (Are reports of the study free of selective outcome reporting?).
- (10)
- Other sources of bias (Was the study apparently free of other problems that could result in high risk of bias?).
3.3. Risk of Bias (RoB) in Individual Studies
3.4. Results of Individual Studies
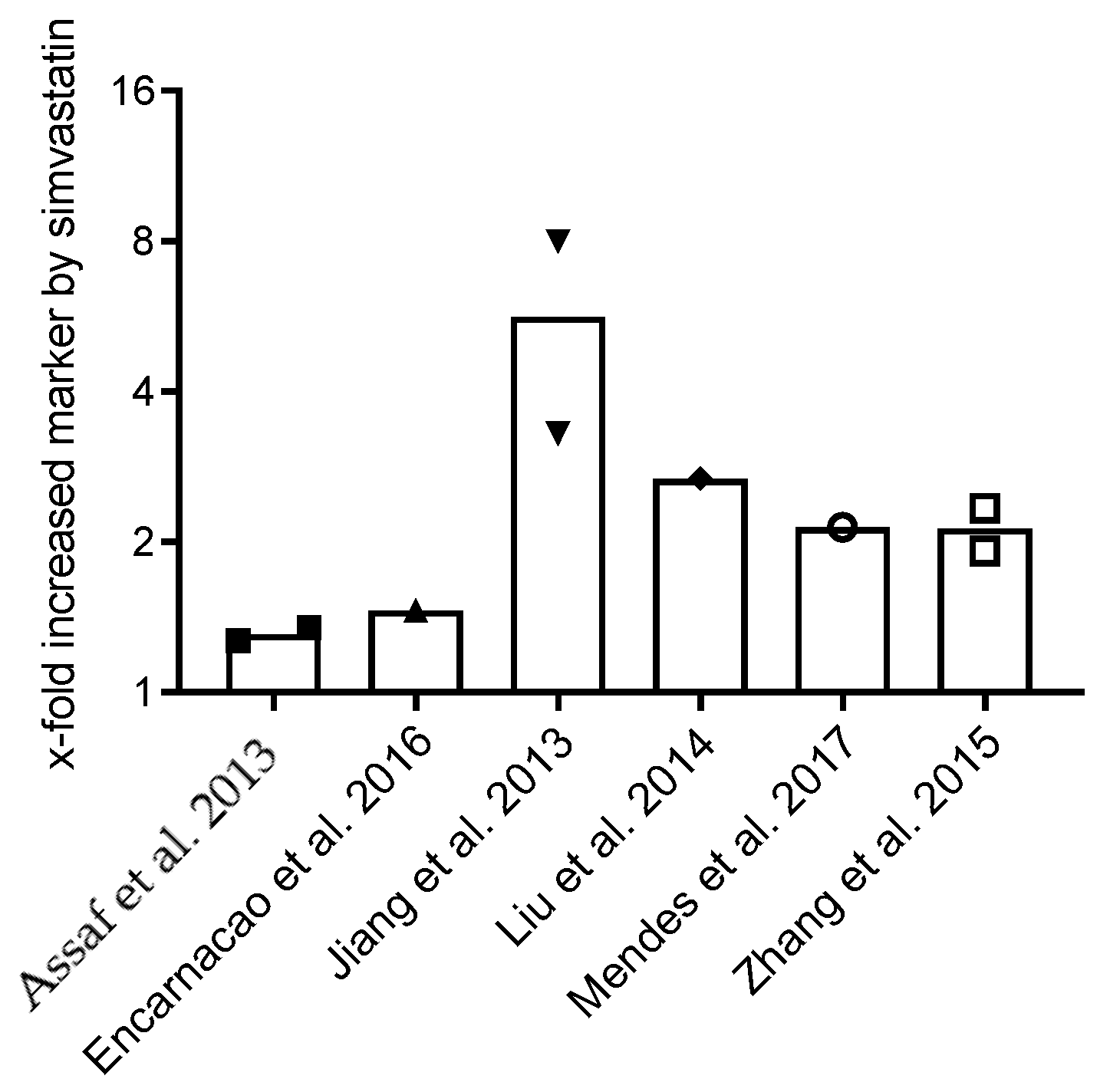
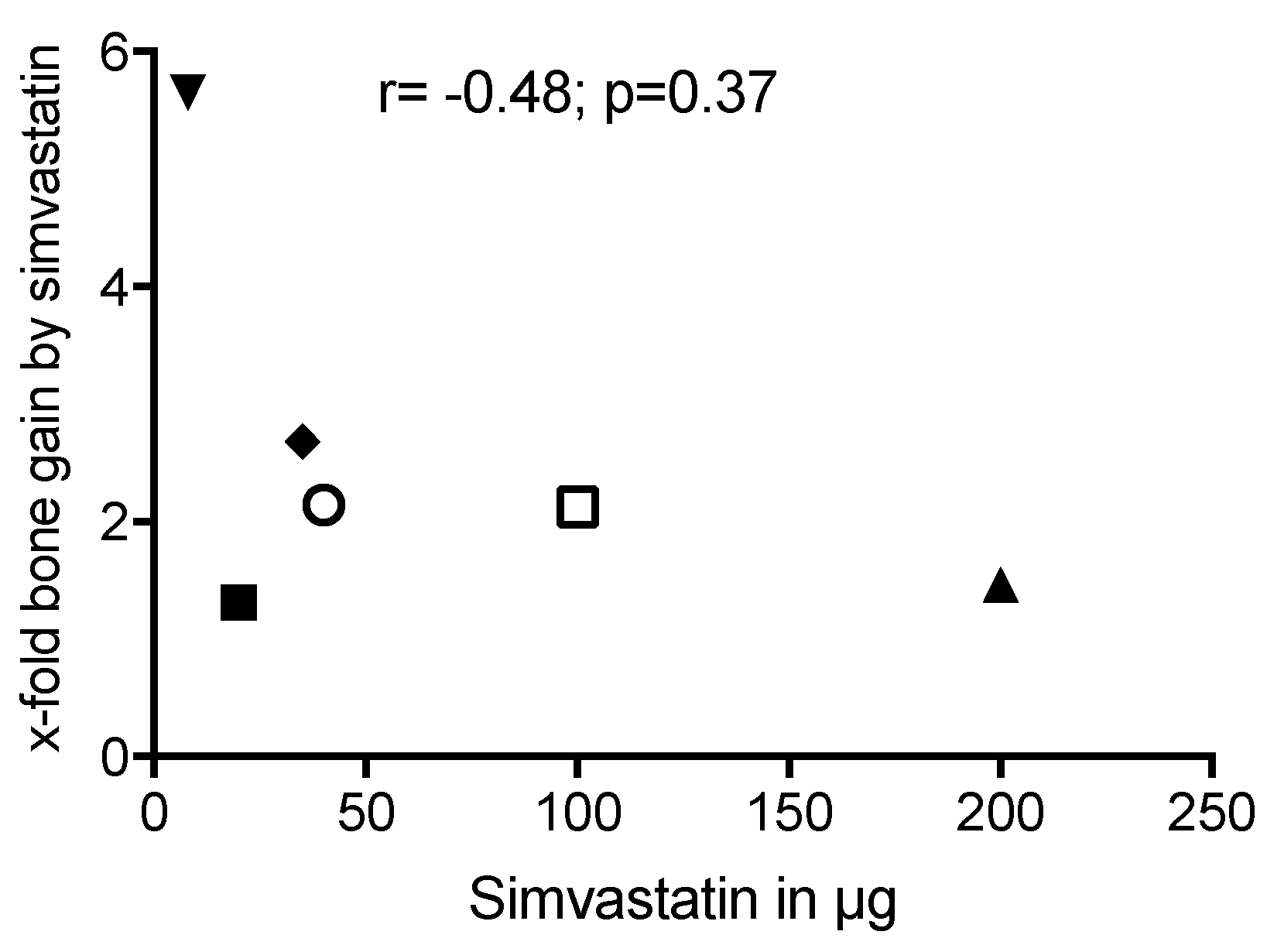
3.5. Synthesys of Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Author | Reasons For Exclusion * |
|---|---|---|
| (1) | CHANG et al., 2013 | 1 |
| (2) | CHANG et al., 2020 | 1 |
| (3) | FU et al., 2015 | 3 |
| (4) | LEE et al., 2018 | 2 |
| (5) | TAI et al., 2010 | 5 |
| (6) | MASAELI et al., 2016 | 2 |
| (7) | NAITO et al., 2014 | 2 |
| (8) | SENON et al., 2015 | 5 |
| (9) | TERUKINA et al., 2016 | 2 |
| (10) | VENKATESAN et al., 2019 | 1 |
| (11) | ZHANG et al., 2019 | 1 |
| (12) | FERREIRA et al., 2015 | 4 |
References
- Araújo, M.G.; Lindhe, J. Dimensional Ridge Alterations Following Tooth Extraction. An Experimental Study in the Dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Kim, S.; Sándor, G.K.Y. Comparison of Platet-Rich Plasma (PRP), Platet -Rich Ribrin (PRF), and Concentrated Growth Factor (CGF) in Rabbit—Skull Defect Healing. Arch. Oral Biol. 2014, 59, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, S.; Aleksic, Z.; Klokkevold, P.; Lekovic, V.; Dimitrijevic, B.; Kenney, E.B.; Camargo, P. Use of Platelet-Rich Fibrin Membrane Following Treatment of Gingival Recession: A Randomized Clinical Trial. Int. J. Periodontics Restor. Dent. 2012, 32, e41–e50. [Google Scholar]
- Puisys, A.; Linkevicius, T. The Influence of Mucosal Tissue Thickening on Crestal Bone Stability around Bone-Level Implants. A Prospective Controlled Clinical Trial. Clin. Oral. Implant. Res. 2015, 26, 123–129. [Google Scholar] [CrossRef]
- Landsberg, C.; Bender, O.; Weinreb, M.; Wigler, R.; Chackartchi, T.; Weinberg, E.; Matalon, S. Postextraction Ridge Width Alterations Following Socket Seal Surgery—A Retrospective Study. Appl. Sci. 2021, 11, 525832. [Google Scholar] [CrossRef]
- Virlan, M.J.R.; Miricescu, D.; Totan, A.; Greabu, M.; Tanase, C.; Sabliov, C.M.; Caruntu, C.; Calenic, B. Current Uses of Poly (Lactic-Co-Glycolic Acid) in the Dental Field: A Comprehensive Review. J. Chem. 2015, 2015, 525832. [Google Scholar] [CrossRef] [Green Version]
- Makadia, H.K.; Siegel, S.J. Poly Lactic-Co-Glycolic Acid (PLGA) as Biodegradable Controlled Drug Delivery Carrier. Polymers 2011, 3, 1377–1397. [Google Scholar] [CrossRef]
- Mendes, D.; Domingues, J.A.; Hausen, M.A.; Cattani, S.M.M.; Aragones, A.; Oliveira, A.L.R.; Inácio, R.F.; Barbo, M.L.P.; Duek, E.A.R. Study of Mesenchymal Stem Cells Cultured on a Poly(Lactic-Co-Glycolic Acid) Scaffold Containing Simvastatin for Bone Healing. J. Appl. Biomater. Funct. Mater. 2017, 15, e133–e141. [Google Scholar] [CrossRef] [Green Version]
- Danhier, F.; Ansorena, E.; Silva, J.M.; Coco, R.; Le Breton, A.; Préat, V. PLGA-Based Nanoparticles: An Overview of Biomedical Applications. J. Control. Release 2012, 161, 505–522. [Google Scholar] [CrossRef]
- Zhang, Z.Z.; Zhang, H.Z.; Zhang, Z.Y. 3D Printed Poly(ε-Caprolactone) Scaffolds Function with Simvastatin-Loaded Poly(Lactic-Co-Glycolic Acid) Microspheres to Repair Load-Bearing Segmental Bone Defects. Exp. Med. 2019, 17, 79–90. [Google Scholar] [CrossRef] [Green Version]
- Tai, I.C.; Fu, Y.C.; Wang, C.K.; Chang, J.K.; Ho, M.L. Local Delivery of Controlled-Release Simvastatin/PLGA /HA p Microspheres Enhances Bone Repair. Int. J. Nanomed. 2013, 8, 3895–3905. [Google Scholar] [CrossRef]
- Littuma, G.J.S.; Sordi, M.B.; Borges Curtarelli, R.; Aragonês, Á.; da Cruz, A.C.C.; Magini, R.S. Titanium Coated with Poly(Lactic-Co-Glycolic) Acid Incorporating Simvastatin: Biofunctionalization of Dental Prosthetic Abutments. J. Periodontal. Res. 2020, 55, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Özeç, I.; Kiliç, E.; Gümüş, C.; Göze, F. Effect of Local Simvastatin Application on Mandibular Defects. J. Craniofacial Surg. 2007, 18, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, K.; Karkavelas, G.; Vouros, I.; Kessopoulou, E.; Konstantinidis, A. Effects of Local Application of Simvastatin on Bone Regeneration in Femoral Bone Defects in Rabbit. J. Cranio-Maxillofac. Surg. 2015, 43, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Schmid, M.J.; Marx, D.B.; Beatty, M.W.; Cullen, D.M.; Collins, M.E.; Reinhardt, R.A. The Effect of Local Simvastatin Delivery Strategies on Mandibular Bone Formation In Vivo. Biomaterials 2008, 29, 1940–1949. [Google Scholar] [CrossRef] [Green Version]
- Oryan, A.; Kamali, A.; Moshiri, A. Potential Mechanisms and Applications of Statins on Osteogenesis: Current Modalities, Conflicts and Future Directions. J. Control. Release 2015, 215, 12–24. [Google Scholar] [CrossRef]
- Mundy, G.; Garrett, R.; Harris, S.; Chan, J.; Chen, D.; Rossini, G.; Boyce, B.; Zhao, M.; Gutierrez, G. Stimulation of Bone Formation in Vitro and in Rodents by Statins. Science 1999, 286, 1946–1949. [Google Scholar] [CrossRef]
- Jiang, L.; Sun, H.; Yuan, A.; Zhang, K.; Li, D.; Li, C.; Shi, C.; Li, X.; Gao, K.; Zheng, C.; et al. Enhancement of Osteoinduction by Continual Simvastatin Release from Poly(Lactic-Co-Glycolic Acid)-Hydroxyapatite-Simvastatin Nano-Fibrous Scaffold. J. Biomed. Nanotechnol. 2013, 9, 1921–1928. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Grp, P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 89, 873–880. [Google Scholar] [CrossRef] [Green Version]
- Greenhalgh, T.; Peacock, R. Effectiveness and Efficiency of Search Methods in Systematic Reviews of Complex Evidence: Audit of Primary Sources. Br. Med. J. 2005, 331, 1064–1065. [Google Scholar] [CrossRef] [Green Version]
- Hooijmans, C.R.; Rovers, M.M.; De Vries, R.B.M.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s Risk of Bias Tool for Animal Studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef] [PubMed]
- Encarnação, I.C.; Ferreira Xavier, C.C.; Bobinski, F.; Dos Santos, A.R.S.; Corrêa, M.; De Freitas, S.F.T.; Aragonez, A.; Goldfeder, E.M.; Cordeiro, M.M.R. Analysis of Bone Repair and Inflammatory Process Caused by Simvastatin Combined with PLGA+HA+βTCP Scaffold. Implant Dent. 2016, 25, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Assaf, K.; De Rezende Duek, E.A.; Oliveira, N.M. Efficacy of a Combination of Simvastatin and Poly(DL-Lactic-Co-Glycolic Acid) in Stimulating the Regeneration of Bone Defects. Mater. Res. 2013, 16, 215–220. [Google Scholar] [CrossRef]
- Liu, Y.S.; Ou, M.E.; Liu, H.; Gu, M.; Lv, L.W.; Fan, C.; Chen, T.; Zhao, X.H.; Jin, C.Y.; Zhang, X.; et al. The Effect of Simvastatin on Chemotactic Capability of SDF-1α and the Promotion of Bone Regeneration. Biomaterials 2014, 35, 4489–4498. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.X.; Xiao, G.Y.; Wang, X.; Dong, Z.G.; Ma, Z.Y.; Li, L.; Li, Y.H.; Pan, X.; Nie, L. Biocompatibility and Osteogenesis of Calcium Phosphate Composite Scaffolds Containing Simvastatin-Loaded PLGA Microspheres for Bone Tissue Engineering. J. Biomed. Mater. Res. A 2015, 103, 3250–3258. [Google Scholar] [CrossRef]
- Wang, W.; Yeung, K.W.K. Bone Grafts and Biomaterials Substitutes for Bone Defect Repair: A Review. Bioact. Mater. 2017, 2, 224–247. [Google Scholar] [CrossRef]
- Sordi, M.B.; da Cruz, A.C.C.; Aragones, Á.; Rodríguez Cordeiro, M.M.; de Souza Magini, R. PLGA+HA/ΒTCP Scaffold Incorporating Simvastatin: A Promising Biomaterial for Bone Tissue Engineering. J. Oral. Implantol. 2021, 47, 93–101. [Google Scholar] [CrossRef]
- Ferreira, L.B.; Bradaschia-Correa, V.; Moreira, M.M.; Marques, N.D.M.; Arana-Chavez, V.E. Evaluation of Bone Repair of Critical Size Defects Treated with Simvastatin-Loaded Poly(Lactic-Co-Glycolic Acid) Microspheres in Rat Calvaria. J. Biomater. Appl. 2015, 29, 965–976. [Google Scholar] [CrossRef]
- Wu, Z.; Liu, C.; Zang, G.; Sun, H. The Effect of Simvastatin on Remodelling of the Alveolar Bone Following Tooth Extraction. Int. J. Oral Maxillofac. Surg. 2008, 37, 170–176. [Google Scholar] [CrossRef]
- Lee, C.T.; Lee, Y. Der Preparation of Porous Biodegradable Poly(Lactide-Co-Glycolide)/ Hyaluronic Acid Blend Scaffolds: Characterization, in Vitro Cells Culture and Degradation Behaviors. J. Mater. Sci. Mater. Med. 2006, 17, 1411–1420. [Google Scholar] [CrossRef]
- Grayson, W.L.; Fröhlich, M.; Yeager, K.; Bhumiratana, S.; Chan, M.E.; Cannizzaro, C.; Wan, L.Q.; Liu, X.S.; Guo, X.E.; Vunjak-Novakovic, G. Engineering Anatomically Shaped Human Bone Grafts. Proc. Natl. Acad. Sci. USA 2010, 107, 3299–3304. [Google Scholar] [CrossRef] [PubMed]
- Lebourg, M.; Suay Antón, J.; Gomez Ribelles, J.L. Characterization of Calcium Phosphate Layers Grown on Polycaprolactone for Tissue Engineering Purposes. Compos. Sci. Technol. 2010, 70, 1796–1804. [Google Scholar] [CrossRef] [Green Version]
- Jain, R.A. The Manufacturing Techniques of Various Drug Loaded Biodegradable Poly(Lactide-Co-Glycolide) (PLGA) Devices. Biomaterials 2000, 21, 2475–2490. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. Chin. J. Evid. -Based Med. 2009, 9, 8–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouxsein, M.L.; Boyd, S.K.; Christiansen, B.A.; Guldberg, R.E.; Jepsen, K.J.; Müller, R. Guidelines for Assessment of Bone Microstructure in Rodents Using Micro-Computed Tomography. J. Bone Miner. Res. 2010, 25, 1468–1486. [Google Scholar] [CrossRef] [PubMed]
- Burghardt, A.J.; Link, T.M.; Majumdar, S. High-Resolution Computed Tomography for Clinical Imaging of Bone Microarchitecture. Clin. Orthop. Relat. Res. 2011, 469, 2179–2193. [Google Scholar] [CrossRef]
- Narayan, R.J. Monitoring and Evaluation of Biomaterials and Their Performance In Vivo; Woodhead Publishing: Suston, UK, 2016. [Google Scholar]





| Study | Population | Scaffold | Outcome Measures | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Author (Year); Country | Total Animals/Defects (n/n) | Control Group (n) | Test Group (n) | Animal Model/Bone | Bone Defect Dimension | SIM Dose per Scaffold | PLA/PGA Ratio (m:m) | Analysis Methods/Experimental Time | Main Findings (p Value) |
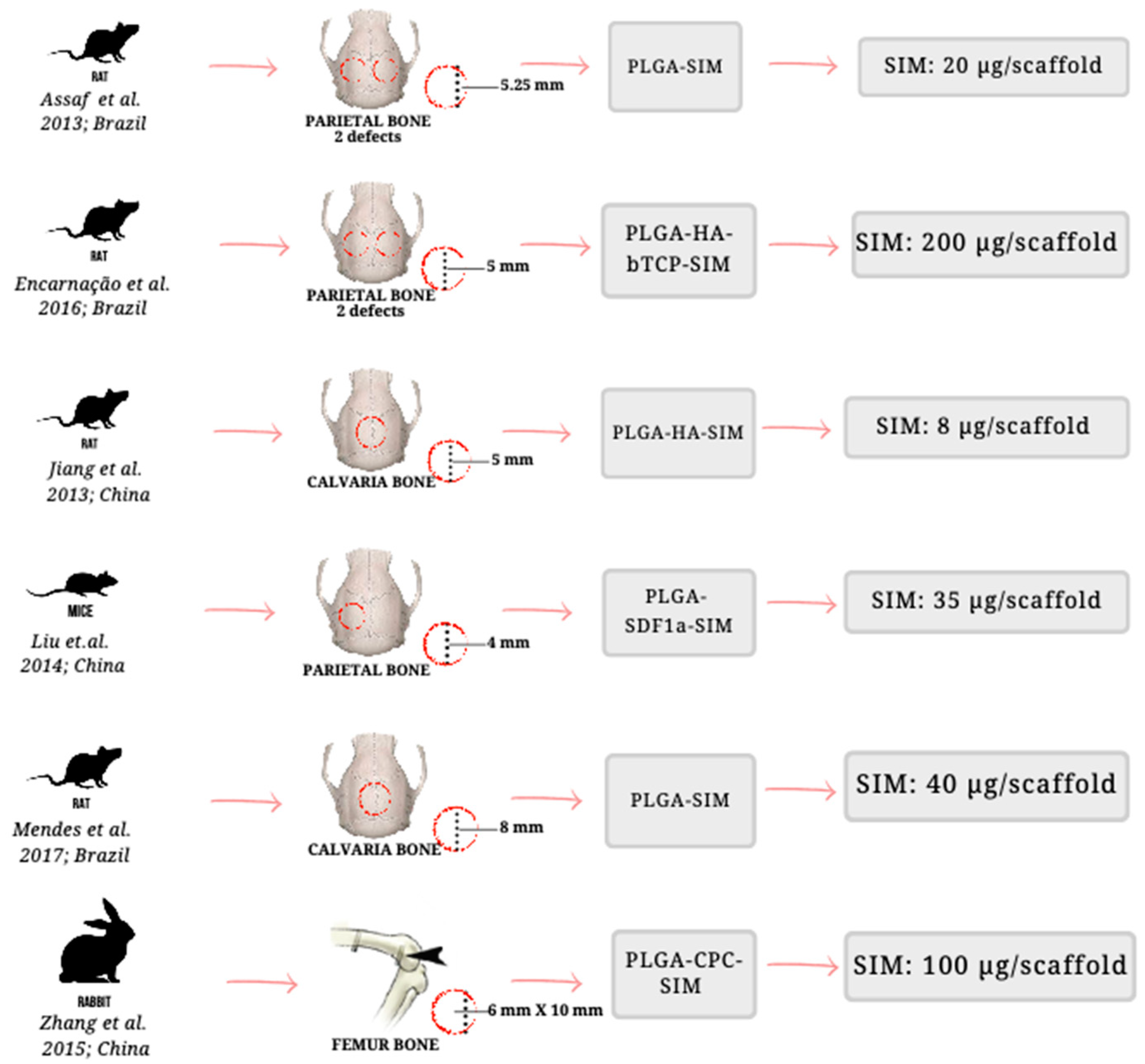
| Assaf K. et al. (2013) [23]; Brazil | 32/64 | Blank control (n = 32) | PLGA (n = 16) PLGA-SIM (n = 16) | Wistar Rats/Parietal bone | 5.25 mm diameter | 20 µg/scaffold | 50:50 | Histological analysis/28 and 56 days. | PLGA-SIM promoted more bone formation than PLGA or blank control groups on 28 and 56 days (p < 0.05). |
| Encarnação I.C. et al. (2016) [22]; Brazil | 180/360 | Naive (n = 6) Blank control (n = 6) | PLGA-HA-βTCP-SIM (n = 6) PLGA-HA-βTCP (n = 6) SIM (n = 6) Vehicle (ethyl alcohol + phosphate-buffered saline) (n = 6) | Wistar Rats/Parietal Bone | 5 mm diameter | 200 µg/scaffold | 82:18 | Radiographical analysis/1, 7, 15, 30, and 60 days. | SIM incorporated into PLGA-HA-βTCP scaffold did lead to bone formation (p < 0.05). |
| Jiang L. et al. (2013) [18]; China | 24/24 | Blank control (n = 8) | PLGA-HA (n = 8) PLGA-HA-SIM (n = 8) | Wistar Rats/Calvaria bone | 5 mm diameter | 8 µg/scaffold | 85:15 | Micro-computed tomography/28 and 56 days | PLGA-HA-SIM group stimulated more bone formation than PLGA-HA or Blank control on 28 and 56 days (p < 0.05). |
| Liu Y.S. et al. (2014) [24]; China | 32/32 | PLGA (n = 8) | PLGA-SIM (n = 8) PLGA-SDF1a (n = 8) PLGA-SDF1a-SIM (n = 8) | Mice/Calvaria bone | 4 mm diameter | 35 µg/scaffold | 75:25 | Micro-computed tomography/56 days | PLGA-SDF1α-SIM promoted more bone formation than PLGA, PLGA-SDF1, or PLGA-SIM on day 56 (p < 0.05). |
| Mendes J.D. et al. (2017) [8]; Brazil | 35/35 | Blank control (n = 7) | PLGA (n = 7) PLGA-SIM (n = 7) PLGA-MSC (n = 7) PLGA-SIM-MSC (n = 7) | Wistar Rats/Calvaria bone | 8 mm diameter | 40 µg/scaffold | Not reported | Histological analysis/56 days | PLGA-SIM promoted more bone formation than PLGA, PLGA-MSC, or PLGA-SIM-MSC (p < 0.05). |
| Zhang H.X. et al. (2015) [25]; China | 30/30 | Blank Control (n = 10) | PLGA-CPC (n = 10) PLGA-CPC-SIM (n = 10) | Rabbits/Femur | 6 mm diameter × 10 mm length | 100 µg/scaffold | 50:50 | Micro-computed tomography analysis/42 and 84 days | PLGA-CPC-SIM scaffolds promoted more bone formation than PLGA-CPC or blank control on days 42 and 84 (p < 0.05). |
| SYRCLE’S Quality Assessment of the Reviewed Papers Item | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | Item | |||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| Assaf K. et al. (2013) [23] | No | Yes | Yes | Yes | No | Unclear | No | Yes | Yes | Yes |
| Encarnação I.C. et al. (2016) [22] | No | Unclear | Unclear | Unclear | No | Unclear | No | Yes | Yes | No |
| Jiang L. et al. (2013) [18] | No | Yes | Yes | Unclear | No | Unclear | No | Yes | Yes | Yes |
| Liu Y.S. et al. (2014) [24] | No | Yes | Unclear | Unclear | No | Unclear | No | Yes | Yes | Yes |
| Mendes J.D. et al. (2017) [8] | No | Yes | Unclear | Unclear | No | Unclear | No | Yes | Yes | Yes |
| Zhang H.X. et al. (2015) [25] | No | Yes | Unclear | Unclear | No | Unclear | No | Yes | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magini, E.B.; Matos, L.d.O.; Curtarelli, R.B.; Sordi, M.B.; Magrin, G.L.; Flores-Mir, C.; Gruber, R.; Cruz, A.C.C. Simvastatin Embedded into Poly(Lactic-Co-Glycolic Acid)-Based Scaffolds in Promoting Preclinical Bone Regeneration: A Systematic Review. Appl. Sci. 2022, 12, 11623. https://doi.org/10.3390/app122211623
Magini EB, Matos LdO, Curtarelli RB, Sordi MB, Magrin GL, Flores-Mir C, Gruber R, Cruz ACC. Simvastatin Embedded into Poly(Lactic-Co-Glycolic Acid)-Based Scaffolds in Promoting Preclinical Bone Regeneration: A Systematic Review. Applied Sciences. 2022; 12(22):11623. https://doi.org/10.3390/app122211623
Chicago/Turabian StyleMagini, Eduarda Blasi, Luiza de Oliveira Matos, Raissa Borges Curtarelli, Mariane Beatriz Sordi, Gabriel Leonardo Magrin, Carlos Flores-Mir, Reinhard Gruber, and Ariadne Cristiane Cabral Cruz. 2022. "Simvastatin Embedded into Poly(Lactic-Co-Glycolic Acid)-Based Scaffolds in Promoting Preclinical Bone Regeneration: A Systematic Review" Applied Sciences 12, no. 22: 11623. https://doi.org/10.3390/app122211623