
Geometric–Statistical Model for Middle-Ear Anatomy and Ventilation

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
- -
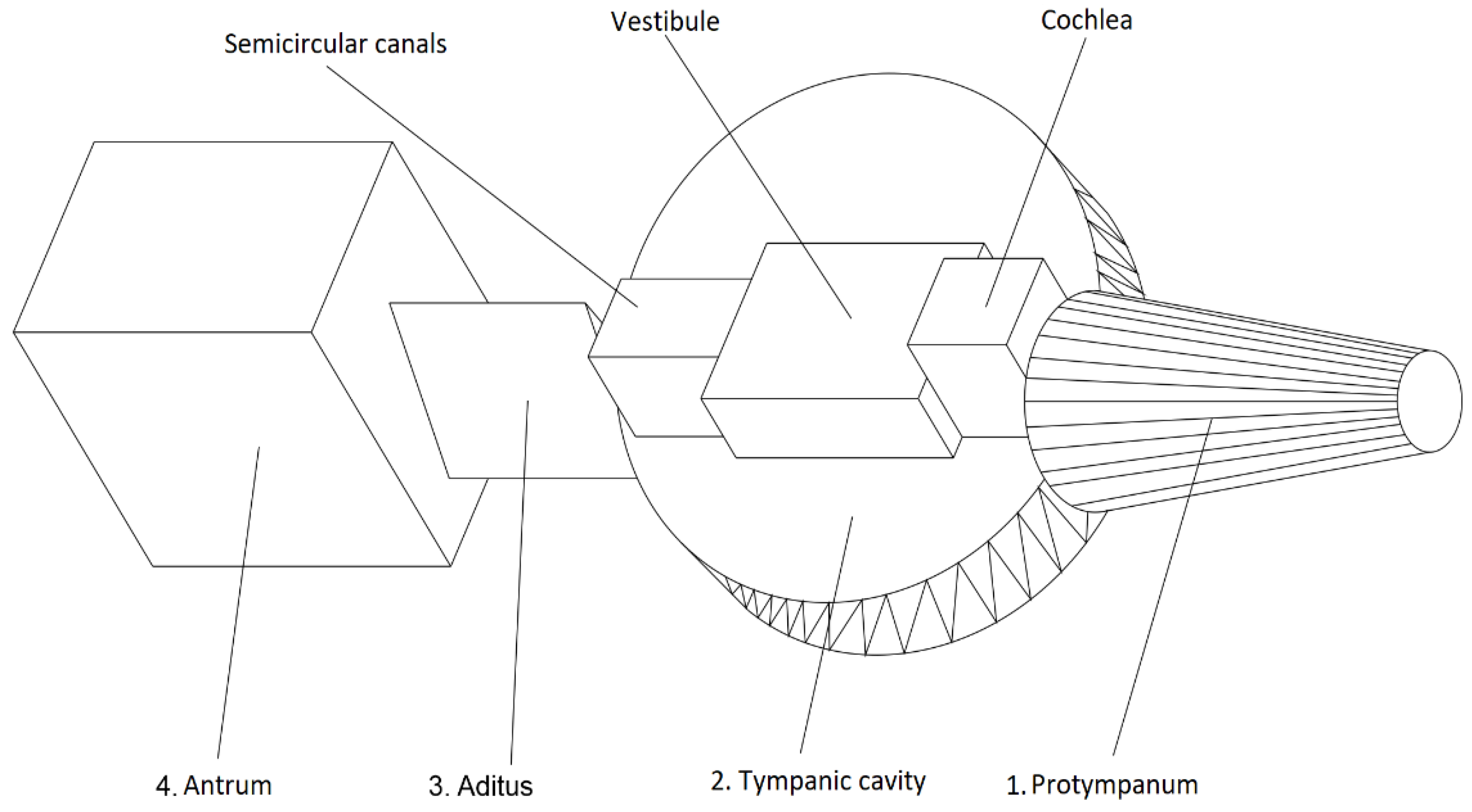
- The ME with constant geometry (invariable; immutable; fixed) includes the Protympanum, Tympanic cavity*, Aditus and Antrum. All these segments have the same dimensions* throughout post-natal life starting from the 7th month of fetal life; (this statement assumes the calculated error—[7]):E*: E* = −5.1%
- -
- The ME with variable geometry includes mastoid and petrous cavities.
- -
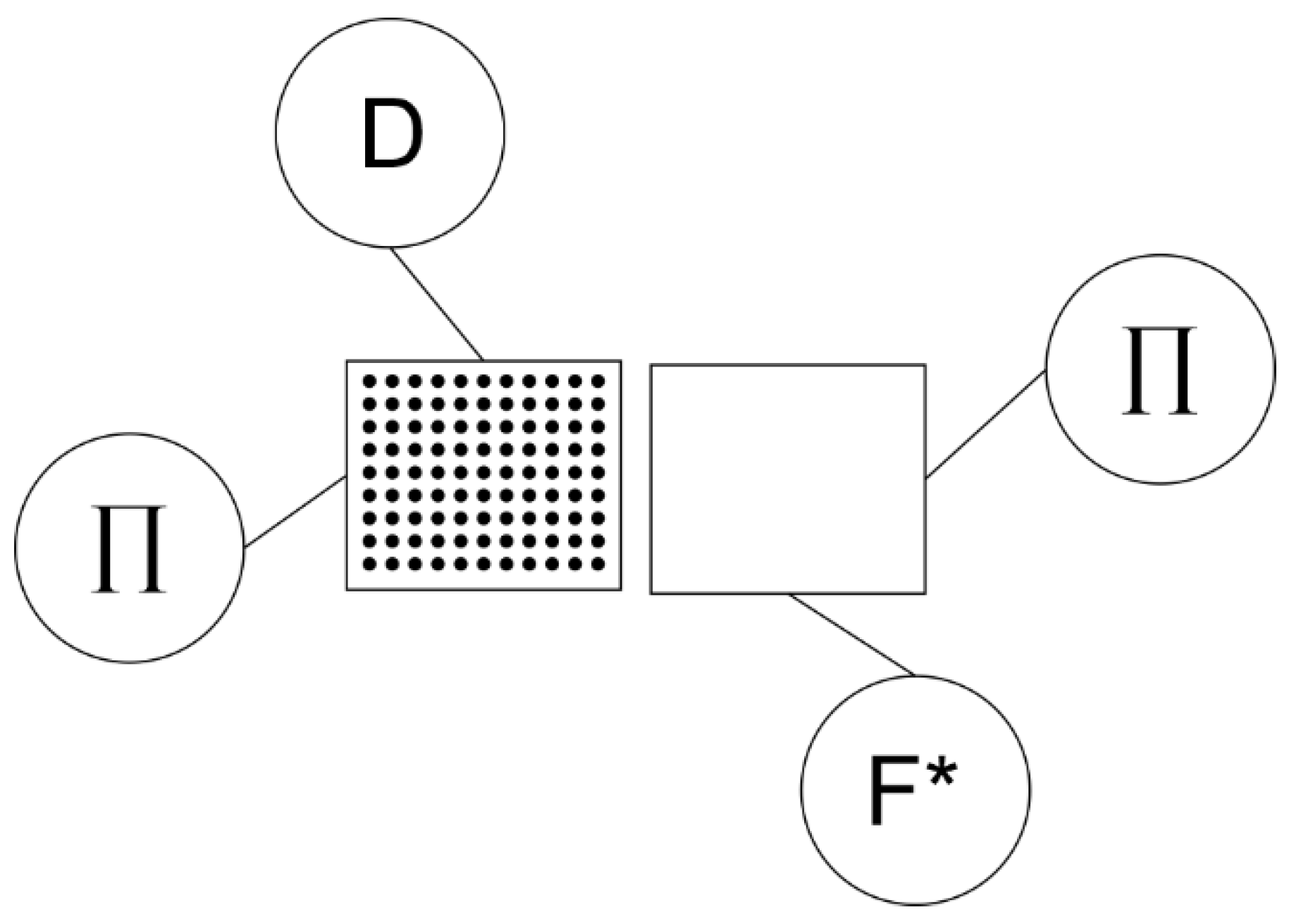
- Pseudo-unistratified heterogenous epithelium and unistratified but with a pattern of prism-shaped cell of dominant variable dimension hF, perpendicular to the basal membrane (Figure 1). This type of epithelium can be found in most of the mucosa with immutable geometry (Protympanum; Tympanic cavity, Aditus). The value of the height hF is at a maximum in the Protympanum, minimum in the Aditus and has mean values in the Tympanic cavity;
- -
- Homogenous unistratified epithelium made up of pavement cells of dominant dimension parallel to the basal membrane and constant minimal dimension hD perpendicular to the basal membrane (Figure 1). This is the epithelium of the mucosa covering the Antrum (central cavity of fixed geometry), and the peripheral cavities of the ME (mastoid and petrous)—ME of variable geometry.
- -
- An anatomic macroscopic support, of constant geometry (immutable) throughout the course of life, for a F heterogenous epithelium, pseudo-unistratified and unistratified, but with a prism-shaped pattern and completely defined mean sizes (see the geometric modeling that follows). This represents an epithelial surface AF of constant size throughout life, of mean thickness hF, also constant throughout life.
- -
- An anatomic macroscopic support, of variable geometry (increasing size in all three dimensions, with a completely defined growth rate), for a D homogenous epithelium, of constant thickness hD. This represents an epithelial surface AD of constant thickness hD, increasing surface with a completely defined growth rate. We will define the growth rate as an analytic function of the growth rate of total body mass of an individual and also of the state of the D-cell population state of health expressed in statistical terms.
- -
- Why is the area AF constant throughout life?
- -
- Why is the area AD increasing simultaneously to the increase in body mass?
- -
- Why are there circumstances when AD stops growing?
- -
- Why does the inequality hF > hD even exist?
3. Results
- -
- The constant numerical value of epithelial area AF ((15) and (17));
- -
- The growth of epithelial area AD, expressed by the inequation ADa/ADnb > 1;
- -
- The uneven thickness of epithelium F and D, expressed by the inequality hF > hD.
- -
- The D-Organ is the epithelium of the mucosa covering the Antrum (central cavity of the ME) and the peripheral cavities (mastoid and petrous);
- -
- The F-Organ is the epithelium of the mucosa covering the Protympanum, Tympanic cavity and Additus (central cavities of the ME).
4. Discussions
- -
- nSD is the total number of D-Cells according to (21);
- -
- VΔ is the volume corresponding to the mas mΔ or to the number of mols νΔ which is the object of simultaneous transfer between the two thermodynamic systems εT and MT via exchange of useful mechanical work within the time interval τ [4]:
- -
- Growth of the peripheral cavitary system of the ME (mastoid) (40), (32), (16), (18);
- -
- Constant value (invariability) of the other segments of the ME (17).
- -
- Useful (decreases the cell energy consumption); or
- -
- Useless, (does not decrease the cell energy consumption) at which point there is a process cessation.
- Determines the numeric values of the ratio xj of healthy D-cells within the D-cell population:
- Determines the numeric values of the ratio yj of afflicted D-cells:
- The determinations above are based on the sufficiently substantiated expression:
- -
- For which numeric value of Π*, the ratio of metabolic energy consumption QDUit1 and QDUit2 of the D-cell, measured at two different moments t1 and t2, becomes equal to 1 (one) (QDUit1 = QDUit2) (QDUit1/QDUit2 = 1) (no decrease in energy consumption), and during the considered interval the area AD increased by one unit [1 cm2] (AD + 1)?
- -
- For which numeric value of Π*, the increase in the D-cell population (AD + 1) {(12), (14), (21) and (22)} becomes useless since it determines no decrease in energy consumption for each D-cell separately or no decrease in installed power for the whole of the D-Organ?
- One truncated cone (Protympanum);
- One cylinder (Tympanic cavity);
- One right prism with a triangular base (Aditus);
- One cube (Antrum);
- -
- All these solids share a symmetry axis;
- -
- This axis is identical to the line representing the collinear heights of the pyramid and the spherical crown (also constituting the symmetry axis of the thumbtack);
- -
- Thus, the fixed geometry ME (F-Organ) is a cavity with shape described above, a cavity within the thumbtack (the temporal bone) (Figure 2).
- On the exterior by the lateral total surface of the thumbtack.
- On the interior by the lateral total surface of the fixed geometry ME (central or axial cavities of the ME).
- The segment around the Protimpanum represents 7% of the D-cell population;
- The segment around the Tympanic cavity represents 18% of the D-cell population;
- The segment around the Aditus represents 10% of the D-cell population;
- The segment around the Antrum represents 65% of the D-cell population.
5. Conclusions
- An increase in D-cell numbers (mastoid growth);
- A decrease in metabolic energy consumption of the D-cell for performing the D-function;
- The optimal function, independent of time, of the D-Organ and of each healthy D-cell (no risk of malfunction, reliability R, R(t) = 1).
- The stopping of mastoid growth (stopping the increase in D-cell population);
- An increase in metabolic energy consumption of the healthy D-cells for performing the D-function;
- Fatigue or aging of the D-function of healthy D-cells as the subject grows older [rick of malfunction, reliability R, R(t) → 0)]. The attrition finally leads to abolishing the D-function of all the initially healthy D-cells. In other words, the disease status of the D-Organ is evolving (gets worst in time) and this process ends when all D-cells become diseased (defective-D-function abolished) and the entire D-Organ will be non-functional or defective. The ultimate physiological expression of this process is the abolishment of the ventilation function of the ME.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guyton, A.C. Textbook of Medical Physiology, 8th ed.; WB Saunders Company: Philadelphia, PN, USA; Harcourt Brace Jovanovich Inc.: San Diego, CA, USA, 1991; pp. 2, 274, 433–437, 744, 792. [Google Scholar]
- Best, C.H.; Taylor, N.B. The Physiological Basis of Medical Practice, A Text in Applied Physiology, 6th ed.; The Williams & Williams Company: Baltimore, MD, USA, 1955; Part III, Chapter 31. [Google Scholar]
- Piiper, J. Physiological Equilibria of Gas Cavities in the Body. In Respiration, Handbook of Physiologie, A Critical Comprehensive Presentation of Physiological Knowledge and Concepts; Fenn, W.O., Rahn, H., Eds.; American Physiological Society: Washington, DC, USA, 1965; Volume 2, pp. 1205–1218. [Google Scholar]
- Radulescu, M.; Mocanu, H.; Nechifor, A.; Mocanu, A.I. Thermodynamic Model for Middle-Ear Ventilation—Defining The D-Organ by Comparison to The Eustachian Tube (Re-Interpretation of A Classic Experiment and Review of Literature). Acta Tech. Napoc. Ser. Appl. Mat. Mec. Eng. 2022, 65, 69–78. [Google Scholar]
- Yee, A.L.; Cantekin, E.I. Effect of Changes in Systemic Oxygen Tension on Middle Ear Gas Exchange. Ann. Otol. Rhinol. Laryngol. 1986, 95, 369–372. [Google Scholar] [CrossRef] [PubMed]
- Eby, T.L.; Nadol, J.B. Postnatal Growth of the Human Temporal Bone—Implication for Cochlear Implants in Children. Ann. Otol. Rhinol. Laryngol. 1986, 95, 356–364. [Google Scholar] [CrossRef]
- Almour, R.X. The Practical Application of Wittmaack’s Theory of Pneumatization. Ann. Otol. Rhinol. Laryngol. 1933, 42, 112–125. [Google Scholar] [CrossRef]
- Diamant, M. Otitis and Pneumatization of the Mastoid Bone; Hakon Olsons Boktryckeri: Lund, Sweden, 1940; pp. 1–149. [Google Scholar]
- Tumarkin, A. On the Nature and Significance of Hypocellularity of the Mastoid. J. Laryngol. Otol. 1959, 73, 33–34. [Google Scholar] [CrossRef] [PubMed]
- Palva, T.; Palva, A. Size of the Human Mastoid System. Acta. Otolaryngol. Stockh. 1966, 62, 237–251. [Google Scholar] [CrossRef]
- Tos, M.; Stangerup, S.E.; Andreassen, U.K. Size of the Mastoid Air Cells and Otitis Media. Ann. Otol. Rhinol. Laryngol. 1985, 94, 386–392. [Google Scholar] [CrossRef]
- Junqueira, L.C.; Carneiro, J.; Long, J.A. Basic Histology, Lange Medical Publications; Appleton-Century-Crofts: Norwalk, CT, USA; Los Altos, CA, USA, 1986; pp. 64–76, 80–82, 140–165, 227, 380–386. [Google Scholar]
- Shimada, T.; Lim, D.J. Distribution of Cilliated Cells in the Human Middle Ear. Ann. Otol. Rhinol. Laryngol. 1972, 81, 203. [Google Scholar] [CrossRef] [PubMed]
- Sammut, J.J. Disposition of the Middle Ear Mucosa. J. Laryngol. 1968, 82, 238. [Google Scholar] [CrossRef] [PubMed]
- Hentzer, E. Ultrastructure of the Normal Mucosa in the Human Middle Ear, Mastoid Cavities and Eustachian Tube. Ann. Otol. Rhinol. Laryngol. 1970, 79, 1143. [Google Scholar] [CrossRef]
- Sadé, J. Middle Ear Mucosa. Arch. Otolaryngol. Head Neck Surg. 1966, 84, 131. [Google Scholar] [CrossRef] [PubMed]
- Hilding, D.A. Ultrastructure of Middle Ear Mucosa and Organisation of Cilliary Matrix. Ann. Otol. Rhinol. Laryngol. 1971, 80, 306. [Google Scholar] [CrossRef] [PubMed]
- Hentzer, E. Histologic Studies of the Normal Mucosa in the Middle Ear, Mastoid Cavities and Eustachian Tube. Ann. Otol. Rhinol. Laryngol. 1970, 79, 825. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Isano, M.; Azuma, H.; Ito, A.; Kimura, H. Computerized Assessment of Pneumatization in Temporal Bone. In Proceedings of the Abstract Book, XVI World Congress of Otorhinolaryngology Head and Neck Surgery, Sydney, Australia, 2–7 March 1997; pp. 254–255. [Google Scholar]
- Azuma, H.; Isano, M.; Murata, K.; Ito, A.; Tanaka, H.; Kawamoto, M. Morphological Characterization of Air Cells in Temporal Bone by Digital Processing of C.T. Images. In Proceedings of the Abstract Book, XVI World Congress of Otorhinolaryngology Head and Neck Surgery, Sydney, Australia, 2–7 March 1997; Volume 317. [Google Scholar]
- Zhao, P.; Ding, H.; Lv, H.; Li, J.; Liu, X.; Yang, Z.; Wang, Z. Growth pattern of temporal bone pneumatization: A computed tomography study with consecutive age groups. Surg. Radiol. Anat. 2018, 41, 221–225. [Google Scholar] [CrossRef]
- Munhoz, L.; Hiroshi Iida, C.; Abdala, R., Jr.; Abdala, R.; Arita, E.S. Mastoid Air Cell System: Hounsfield Density by Multislice Computed Tomography. J. Clin. Diagn. Res. 2018, 12, TC01–TC03. [Google Scholar] [CrossRef]
- Lima, M.A.R.; Farage, L.; Cury, M.C.L.; Bahmad, F., Jr. Mastoid surface area-to-volume ratios in adult brazilian individuals. Braz. J. Otolaryngol. 2013, 9, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Byun, S.W.; Lee, S.S.; Park, J.Y.; Yoo, J.H. Normal Mastoid Air Cell System Geometry: Has Surface Area Been Overestimated? Clin. Exp. Otolaryngol. 2016, 9, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Csakanyi, Z.; Katona, G.; Josvai, E.; Mohos, F.; Sziklai, I. Volume and Surface of the Mastoid Cell System in Otitis Media with Effusion in Children: A Case-Control Study by Three-Dimensional Reconstruction of Computed Tomographic Images. Otol. Neurotol. 2011, 32, 64–70. [Google Scholar] [CrossRef]
- Neagu, A.; Mocanu, A.I.; Bonciu, A.; Coadă, G.; Mocanu, H. Prevalence of GJB2 gene mutations correlated to presence of clinical and environmental risk factors in the etiology of congenital sensorineural hearing loss of the Romanian population. Exp. Ther. Med. 2021, 21, 612. [Google Scholar] [CrossRef] [PubMed]
- Mocanu, H.; Mocanu, A.I.; Bonciu, A.; Coada, G.; Schipor, M.A.; Radulescu, M. Analysis of long-term functional results of radical mastoidectomy. Exp. Ther. Med. 2021, 22, 1216. [Google Scholar] [CrossRef] [PubMed]
- Mocanu, H.; Mocanu, A.I.; Coada, G.; Bonciu, A.; Schipor, M.A.; Radulescu, M. Analysis of long-term anatomic results of radical mastoidectomy. Exp. Ther. Med. 2022, 23, 156. [Google Scholar] [CrossRef] [PubMed]
- Park, M.S.; Yoo, S.H.; Lee, D.H. Measurement of surface area in human mastoid air cell system. J. Laryngol. Otol. 2000, 114, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Koc, A.; Ekinci, G.; Bilgili, A.M.; Akpinar, I.N.; Yakut, H.; Han, T. Evaluation of the mastoid air cell system by high resolution computed tomography: Three-dimensional multiplanar volume rendering technique. J. Laryngol. Otol. 2003, 117, 595–598. [Google Scholar] [CrossRef] [PubMed]
- Valtonen, H.J.; Dietz, A.; Qvarnberg, Y.H.; Nuutinen, J. Development of mastoid air cell system in children treated with ventilation tubes for early-onset otitis media: A prospective radiographic 5-year follow-up study. Laryngoscope 2005, 115, 268–273. [Google Scholar] [CrossRef]
- Cinamon, U. The growth rate and size of the mastoid air cell system and mastoid bone: A review and reference. Eur. Arch. Otorhinolaryngol. 2009, 266, 781–786. [Google Scholar] [CrossRef]
- Hug, J.E.; Pfaltz, C.R. Temporal bone pneumatization. A planimetric study. Arch. Otorhinolaryngol. 1981, 233, 145–156. [Google Scholar] [CrossRef]
- Flisberg, K.; Zsigmond, M. The size of the mastoid air cell system. Planimetry-direct volume determination. Acta Otolaryngol. 1965, 60, 23–29. [Google Scholar] [CrossRef]
- Todd, N.W.; Pitts, R.B.; Braun, I.F.; Heindel, H. Mastoid size determined with lateral radiographs and computerized tomography. Acta Otolaryngol. 1987, 103, 226–231. [Google Scholar] [CrossRef]
- Vrabec, J.T.; Champion, S.W.; Gomez, J.D.; Johnson, R.F., Jr.; Chaljub, G. 3D CT imaging method for measuring temporal bone aeration. Acta. Otolaryngol. 2002, 122, 831–835. [Google Scholar] [CrossRef]
- Lee, D.H.; Jun, B.C.; Kim, D.G.; Jung, M.K.; Yeo, S.W. Volume variation of mastoid pneumatization in different age groups: A study by three-dimensional reconstruction based on computed tomography images. Surg. Radiol. Anat. 2005, 27, 37–42. [Google Scholar] [CrossRef]
- Sadé, J.; Fuchs, C. A comparison of mastoid pneumatization in adults and children with cholesteatoma. Eur. Arch. Otorhinolaryngol. 1994, 251, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Derlacki, E.L. Etiological aspects in congenital cholesteatoma. In Cholesteatoma. First International Conference; McCabe, B., Sadé, J., Abramson, M., Eds.; Aesculapius: Birmingham, AL, USA, 1977; pp. 208–211. [Google Scholar]
- Schillinger, R. Pneumatization of the mastoid. Radiology 1939, 33, 54–67. [Google Scholar] [CrossRef]
- Zollikofer, C.P.; Weissmann, J.D. A morphogenetic model of cranial pneumatization based on the invasive tissue hypothesis. Anat. Rec. 2008, 291, 1446–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatterjee, D.; Ghosh, T.B.; Ghosh, B.B. Size variation of mastoid air cell system in Indian people at different age groups: A radiographic planimetric study. J. Laryngol. Otol. 1990, 104, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Isono, M.; Ito, A.; Nakayama, K.; Miyashita, H.; Saito, K.; Murata, K. Computerized assessment of developmental changes in the mastoid air cell system. Int. Congr. Ser. 2003, 1254, 487–491. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gas Type | Diffusion Time [seconds] | |||
|---|---|---|---|---|
| O2 | CO2 | N2 | Gas Mix | |
| Diffusion time | τO2 | τCO2 | τN2 | τamestec = (τO2⋅VOF∗O2/VOF∗) + (τCO2⋅VOF∗CO2/VOF∗) + (τN2⋅VOF∗N2/VOF∗) |
| Newborn | 6.61 | 0.365 | 12.36 | 3.71 |
| Adult | 178.78 | 9.87 | 334.3 | 100.344 |
| Volume Flow [cm3/24 h] | ||||
|---|---|---|---|---|
| Gas Type | O2 | CO2 | N2 | Total Gas Mix |
| Newborn | 110.87 | 2317.97 | 858.87 | 3287.71 |
| Adult | 102.67 | 2146.44 | 795.31 | 2254.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rădulescu, M.; Mocanu, A.-I.; Dascălu, I.T.; Schipor, M.-A.; Mocanu, H. Geometric–Statistical Model for Middle-Ear Anatomy and Ventilation. Appl. Sci. 2022, 12, 11287. https://doi.org/10.3390/app122111287
Rădulescu M, Mocanu A-I, Dascălu IT, Schipor M-A, Mocanu H. Geometric–Statistical Model for Middle-Ear Anatomy and Ventilation. Applied Sciences. 2022; 12(21):11287. https://doi.org/10.3390/app122111287
Chicago/Turabian StyleRădulescu, Marian, Adela-Ioana Mocanu, Ionela Teodora Dascălu, Mihai-Adrian Schipor, and Horia Mocanu. 2022. "Geometric–Statistical Model for Middle-Ear Anatomy and Ventilation" Applied Sciences 12, no. 21: 11287. https://doi.org/10.3390/app122111287