The general problem is scheduling a high throughput of in- and out-patient surgeries over a certain time period to minimize the OR overtime while bounding the likelihood of exceeding the limited downstream ward bed capacity. Patient priorities are included in the model as hard constraints, i.e., if a patient requires scheduling within one week, it will be done. We do not consider optimizing the flow of the emergency arrivals as they are treated in a separate flow, in downtime and after hours. Further, we do not consider optimizing the total number of patients scheduled since this requires discriminating between patients and should be the responsibility of the hospital. If the ward beds and ORs are underutilized, the hospital can add more patients to the list of patients to be scheduled.
2.1. Operating Room Day Schedule Generation
For a given MSS, we assume that each surgical specialty is assigned one or more ORs on each day for the planning horizon D, where the available surgery time for each block is given the capacity parameter . Note that can be of any size, and different values can be specified for each block. These values are determined by the hospital. Further, we assume that the surgical specialties allocate their blocks to its operators where each operator has at least one assignment in D per week. A patient then belongs to an operator’s list of patients () and can be assigned to one of the operator’s blocks.
For each operator’s block, we generate a set of feasible ORDS of patients to be scheduled. The feasibility of the ORDS is determined, on the one hand, by practical rules set by the hospital and, on the other hand, by limits on overtime. The ORDS are all feasible combinations of patients within the operator’s waiting list. The number of combinations will grow exponentially. However, in real life, hospitals have a diverse set of practical rules [
29,
31,
32] that determine which ORDS are permitted. The application of these rules significantly reduces the number of feasible combinations. Here, we make use of two rules. First, we pose an upper bound on the number of patients assigned to an ORDS. Second, we pose an upper bound on the number of ICU patients assigned to an ORDS. However, these ORDS may not be feasible towards restrictions on overtime and are eliminated using Monte Carlo sampling.
Let
be the maximum number of surgeries assigned to an ORDS and
be a binary decision variable taking the value 1 if patient
i is assigned to ORDS
p; otherwise, it is 0. Then, one may pose an upper limit on the number of patients assigned to an ORDS using the following constraint:
Second, one may pose an upper bound on the number of ICU patients (
) for each ORDS by
where
is a binary parameter taking the value 1 if patient
i requires ICU admission; otherwise, it is 0. It is assumed that a patient’s need for ICU admission is known in advance.
As the block length of each block (
) is finite and surgery duration differs significantly across surgical types, only a subset of ORDS is feasible. That is to say, a set of patients is considered a feasible ORDS
p when the probability of exceeding
is no more than
; that is,
where
is a random variable denoting the surgery duration of patient
i, including overhead such as preparation and cleaning. Note that only unique values for
need to be considered. To make sure that all patients can be assigned to at least one ORDS, an exception to this rule must be given to single surgeries. This is important since some surgeries may span the entire block and exceed the limit of
.
When generating the ORDS, a limit (
) is set on the probability that the sum of surgery duration in an ORDS surpasses the available surgery time
as posed by constraint (
3). For each ORDS, the expected value of this probability is calculated for regular overtime
and extended overtime
, as
where
is the time added to extend the block length. Our MIP model uses these values to estimate the number of days resulting in regular and extended overtime along with the set of feasible ORDS
P.
2.2. Ward Combination Optimization
From historical data, for the different surgery types, it is possible to estimate the probability that a specific patient is in the ward on any given day. If one discretizes these probabilities (
) and counts (
) how many within each bin or class interval
k, then it is possible to approximate the number of patients in the ward by the sum of binomial distributions, or
where
l is an index to a particular combination of patient numbers in each interval class, defined by
which is a base-
encoding where
is a set of available staffed ward beds and
.
Indeed, the number of such combinations will grow exponentially in terms of the number of staffed ward beds and the number of class intervals. However, not all are feasible since those that exceed the number of available staffed ward beds with probability
can be disregarded. That is, the feasibility of patients in ward combination
l for a given number of available staffed ward beds
a must satisfy
Monte Carlo sampling can be used to verify each combination resulting in a binary parameter , denoting its feasibility. This parameter is utilized by a constraint in our model to bound the likelihood of exceeding the staffed ward beds.
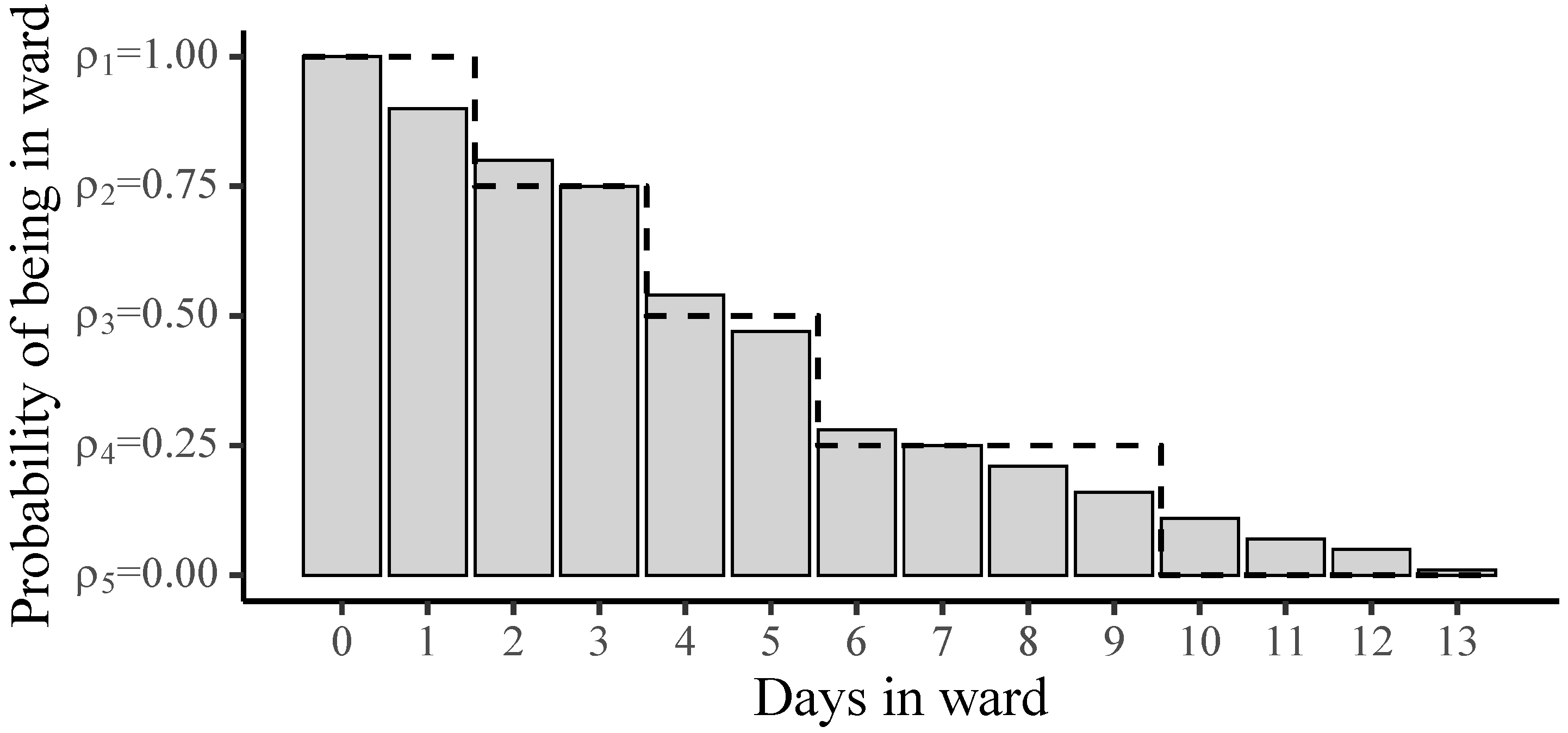
In
Figure 1, one can see how a distribution for an arbitrary surgery type has been discretized to 5 levels, as illustrated by the dashed line. In this example, the discretization assumes that for the day of the surgery and the day after (0 and 1), the patient will be in the ward with probability
. After the ninth day, the patient has left the ward and the probability is
. We are only interested in the levels between the first and the last, which is, in this example,
. The number of patients in the first level
are used to calculate the number of available staffed ward beds
, where
is the total number of staffed ward beds.
Once all feasible ORDS and ward combinations have been generated, the scheduling problem is reduced to allocating ORDS to days and rooms subject to the feasibility of the resulting ward combination. Let us introduce a binary decision variable taking the value 1 if an ORDS p is assigned on day and room . There are, however, a number of restrictions on which ORDS can be assigned to any given day. These usually center around the availability of the operators and the patients. Additionally, the ORDS’s feasibility depends on the OR’s capacity for that day, . As a result, the reduced set is generated taking the following restrictions into account:
The availability of the operators for a given day,
The patients’ availability and priority,
ORDS feasibility for a given day and room, dependent on and .
Patient priorities are implemented in practice as a strict number of days that patients can be on the waiting list.
As each ORDS spans the whole day, only one ORDS can be assigned to a room and a day,
Similarly, any patient
i can only be scheduled once,
where
is the set of patients included in ORDS
p. It is assumed that all patients must be scheduled, so the throughput is fixed. Additionally, each operator is only permitted to work according to a single ORDS per day,
where
are the ORDS containing the patients of operator
o. Finally, we assume a quota system for ICU admission as proposed by [
31]; that is to say, for each day, no more than
patients can be admitted to the ICU,
where
denotes the number of ICU patients in ORDS
p.
Given a schedule defined by the decision variables
, a constraint is posed to bound the likelihood of exceeding the staffed ward beds by a given probability. This is important as exceeding the staffed ward beds may result in cancellations. To start with, one must establish the daily availability of the staffed ward beds for any given surgery schedule. For each schedule, the number of patients that will occupy a ward bed with 100% certainty (
) is assumed to be known for any given day. The number of staffed wards beds that are available each day (
) can be calculated as follows:
where
is the upper bound on LOS in the ward. The parameter
denotes the number of patients still in the ward from previous weeks (prior to the start of our planning horizon) with 100% (
) certainty of occupying a staffed ward bed on the day
j. This evaluation may be carried out with a Monte Carlo sampling using the previous week’s known schedule. The parameter
denotes the number of ward patients on the day
j after a surgery, belonging to ORDS
p, with
, or a 100% chance of being in the ward that day. By multiplying the decision variable
by this parameter for each day, we can calculate the total number of patients within each scheduled ORDS that are in the ward on the day
d after their surgery, conducted on the day
. The daily availability of staffed ward beds is bounded by the maximum number of staffed ward beds (
), so
The number of patients
with the probability
, where
, of being in the ward at given day
d may be calculated as follows:
where
denotes the number of patients in ward with probability
on the day
j after the surgery belonging to ORDS
p.
is number of patients from the previous planning period with the probability of
of occupying the staffed ward beds on day
d.
As a final step in bounding the likelihood of exceeding the staffed ward beds that are available, one must make sure that the combination of ward admission probabilities, associated with the schedule defined by the decision variables
, is feasible. That means connecting the available staffed ward beds each day
, the number of patients
, with the probability
of being in the ward at a given day and the set of feasible ward combinations specified by
. We may now introduce the binary decision variable
that takes the value 1 if ward combination
l is realized on day
d; otherwise, it is 0. There can be only one ward combination realized each day
In order to discover which ward combination resulted from the scheduled ORDS, a base-
decoder is constructed in the form of the following constraint:
This constraint may be thought of as searching for a specific row in a table. The right-hand side decodes the combinations of into a specific row number, which corresponds to the settings of ward combination l.
To make the connection from a certain ward combination to the available staffed ward beds each day, a binary variable
is introduced, taking the value 1 if on the day
there are
staffed ward beds available; otherwise, it is 0. This variable is linked to the actual number of available staffed ward beds using the following constraint:
where
can only take one value each day
Now, one can force the selection of a feasible ward combinations as follows:
where
is a binary parameter value taking the value 1 if a ward combination
l is feasible with respect to the risk of ward overflow specified by
; otherwise, it is 0 for a given number of available staffed ward beds
. As explained at the start of this section, the parameter
is calculated by Monte Carlo sampling prior to the start of the optimization. The purpose of constraints (
14) to (
19) is to guide the ORDS assignments so that each day’s resulting ward combination is feasible.
Having specified the constraints that hedge against the risk of ward overflow, we now turn to the objective function. The problem considered in this paper is to schedule a given set of patients (fixed throughput) over the period D so that both overtime and the likelihood of exceeding the limited number of staffed ward beds are minimized. As we have already set bounds to the likelihood of exceeding the limited number of staffed ward beds with the parameter , the focus in the objective function is on minimizing the OR overtime and the amount of overtime.
Let us introduce the binary variable
, taking the value 1 if
and otherwise taking the value of 0, as forced by the following constraint:
and similarly, the binary variable
taking the value 1 if
and otherwise taking the value of 0, as posed by the following constraint:
The former binary variable (
) determines the number of times that the probabilities of the selected ORDSs surpass the accepted risk (
) of entering regular overtime, while the latter (
) determines the number of times that the probabilities of the ORDSs surpass the accepted risk (
) of entering extended overtime. The objective function minimizes the total number of times a selected ORDS results in overtime, but with more weight
on the extended overtime. A further penalty is added for the degree of surpassing the accepted risk limits by minimizing the squared probabilities
and
, again with more weight on extended overtime, resulting in the following objective function:
2.3. Robust Ward Optimization
In robust optimization, distributional information about the LOS is ignored [
2]. Instead, constraints that reflect the worst-case realization of uncertainty are added. The difficulty of describing the worst-case realization, the so-called uncertainty set, is the challenge remaining. The subject matter experts, knowing the patients’ conditions, may be able to estimate the worst-case scenario. Depending on the risk-attitude of the hospital, a probabilistic guarantee for the feasibility can be made.
Let us assume that the decision-maker is very conservative and requires an
level of certainty that the number of staffed ward beds occupied in the ward are kept below their capacity
. Let the probability of patient
i being in the ward on day
d be denoted by
. Then, the worst-case realization should satisfy the following condition:
where
are the patients with certainty
in the ward from the previous plan and
takes the value 1 when
; otherwise, it is 0. Constraint (
24) replaces constraints (
12)–(
19) described in the previous section; all other details of the MIP model remain the same.
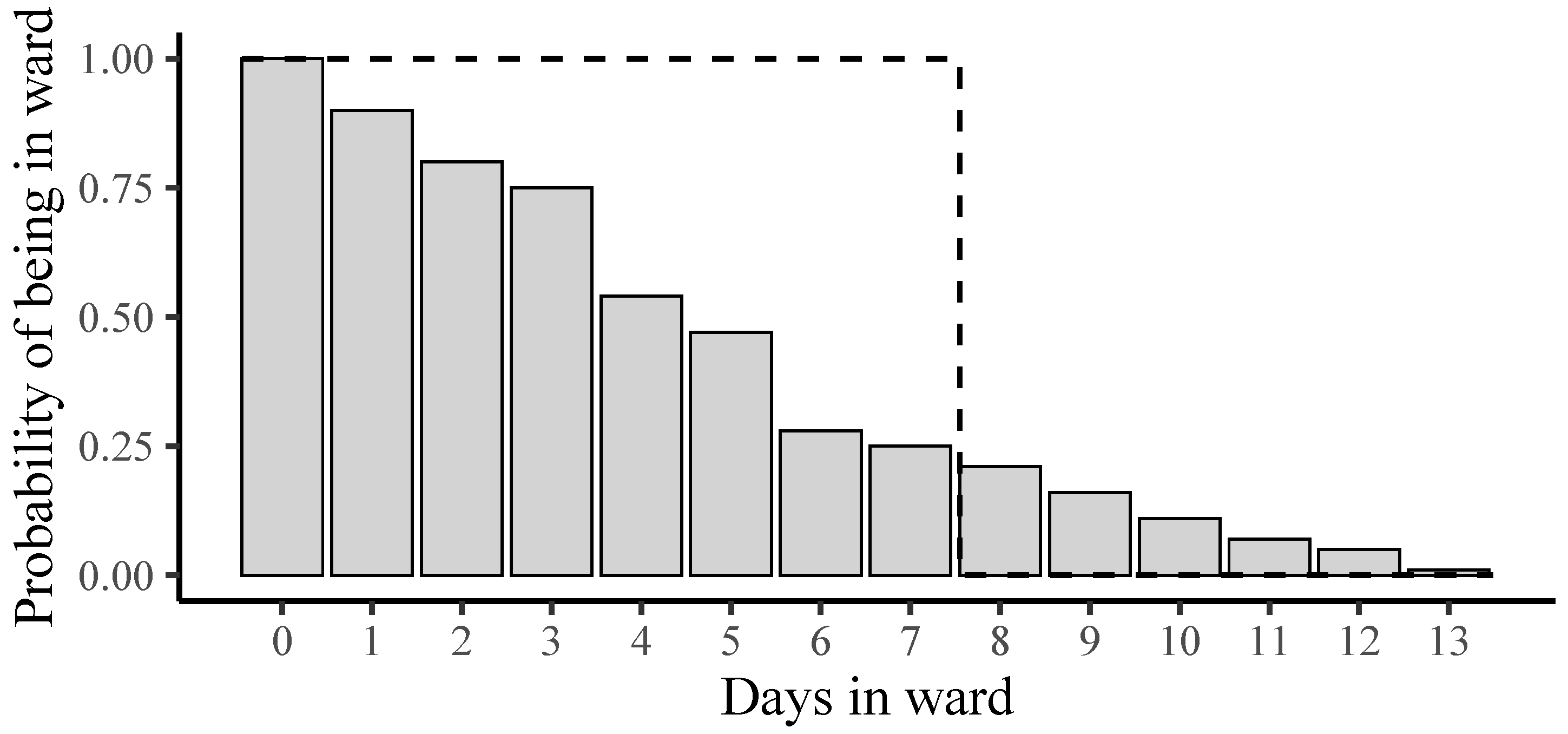
In
Figure 2, one can see the distribution for the same surgery type as presented in
Figure 1, but now, for the worst-case LOS using
, as illustrated by the dashed-line. In this example, the patient is in ward from days 0 to 7 (
) but has left the ward on day 8 (
). The figure shows that the approach is conservative and may reduce the number of scheduling possibilities.
Although the worst case for the LOS for a single patient is used, there is still the chance that we will exceed the staffed ward beds with a high probability when there are many patients in the ward. In the implementation of this constraint in [
2], a slack is introduced to allow for additional ward beds and thus guarantee feasibility. We do not consider this an option and suggest that the strategy in practice would be to increase the value of
until feasibility is met.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}