
CPAP Adherence Assessment via Gaussian Mixture Modeling of Telemonitored Apnea Therapy

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Related Work
3. The CPAP Use Dataset
4. Methodology
4.1. Detecting Summarization Patterns
4.2. Features Extraction and Selection
4.3. Selection
5. Gaussian Mixture Modeling
5.1. Rationale for Using Gaussian Mixture Modeling
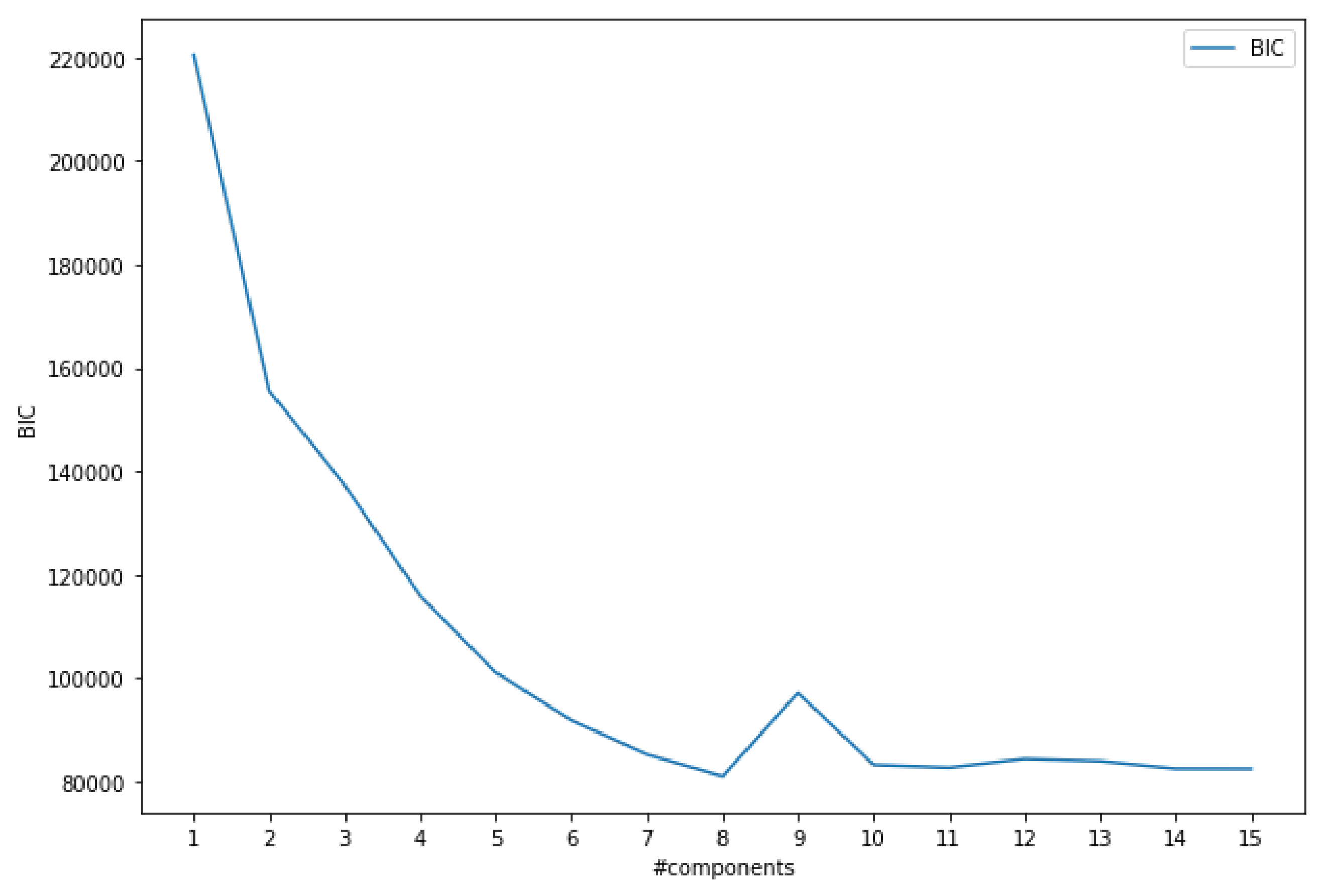
5.2. Bayesian Information Criterion
5.3. Further Supporting Statistics
5.4. Gaussian Components
5.5. LDA-Based Visualization
5.6. GMM-Based Patient Characterization
6. Discussion
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Franco, P.; Bourdin, H.; Braun, F.; Briffod, J.; Pin, I.; Challamel, M.J. Diagnostic du syndrome d’apnée obstructive du sommeil chez l’enfant (2–18 ans): Place de la polysomnographie et de la polygraphie ventilatoire. Syndrome d’apnée obstructive du sommeil de l’enfant (SAOS) Recommandations de la Société Française de Recherche et Médecine du Sommeil. Arch. PéDiatrie 2017, 24, S16–S27. [Google Scholar] [CrossRef] [PubMed]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pepin, J.L. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [Green Version]
- Watson, N.F. Health Care Savings: The Economic Value of Diagnostic and Therapeutic Care for Obstructive Sleep Apnea. J. Clin. Sleep Med. 2016, 12, 1075–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilat, H.; Vinker, S.; Buda, I.; Soudry, E.; Shani, M.; Bachar, G. Obstructive sleep apnea and cardiovascular comorbidities: A large epidemiologic study. Medicine 2014, 93, e45. [Google Scholar] [CrossRef] [PubMed]
- DiMatteo, M.R. Variations in patients’ adherence to medical recommendations: A quantitative review of 50 years of research. Med. Care 2004, 42, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Iannella, G.; Lechien, J.R.; Perrone, T.; Meccariello, G.; Cammaroto, G.; Cannavicci, A.; Burgio, L.; Maniaci, A.; Cocuzza, S.; Di Luca, M.; et al. Barbed reposition pharyngoplasty (BRP) in obstructive sleep apnea treatment: State of the art. Am. J. Otolaryngol. 2022, 43, 103197. [Google Scholar] [CrossRef]
- Wang, D.; Tang, Y.; Chen, Y.; Zhang, S.; Ma, D.; Luo, Y.; Li, S.; Su, X.; Wang, X.; Liu, C.; et al. The effect of non-benzodiazepine sedative hypnotics on CPAP adherence in patients with OSA: A systematic review and meta-analysis. Sleep 2021, 44, zsab077. [Google Scholar] [CrossRef]
- Engleman, H.M.; Wild, M.R. Improving CPAP use by patients with the sleep apnoea/hypopnoea syndrome (SAHS). Sleep Med. Rev. 2003, 7, 81–99. [Google Scholar] [CrossRef]
- Pépin, J.L.; Tamisier, R.; Hwang, D.; Mereddy, S.; Parthasarathy, S. Does remote monitoring change OSA management and CPAP adherence? Respirology 2017, 22, 1508–1517. [Google Scholar] [CrossRef]
- Varma, N.; Ricci, R.P. Telemedicine and cardiac implants: What is the benefit? Eur. Heart J. 2013, 34, 1885–1895. [Google Scholar] [CrossRef] [Green Version]
- Mendelson, M.; Vivodtzev, I.; Tamisier, R.; Laplaud, D.; Dias-Domingos, S.; Baguet, J.P.; Moreau, L.; Koltes, C.; Chavez, L.; De Lamberterie, G.; et al. CPAP treatment supported by telemedicine does not improve blood pressure in high cardiovascular risk OSA patients: A randomized, controlled trial. Sleep 2014, 37, 1863–1870. [Google Scholar] [CrossRef]
- Chang, J.; Derose, S.; Benjafield, A.; Crocker, M.; Kim, J.; Becker, K.; Woodrum, R.; Arguelles, J.; Hwang, D. Acceptance and Impact of Telemedicine in Patient Sub-Groups with Obstructive Sleep Apnea: Analysis from the Tele-Osa Randomized Clinical Trial; Sleep. Oxford University Press Inc. Journals Dept.: Cary, NC, USA, 2017; Volume 40, pp. A201–A202. [Google Scholar]
- Stepnowsky, C.; Palau, J.; Marler, M.; Gifford, A. Pilot randomized trial of the effect of wireless telemonitoring on compliance and treatment efficacy in obstructive sleep apnea. J. Med. Internet Res. 2007, 9, e14. [Google Scholar] [CrossRef]
- Stepnowsky, C.J.; Marler, M.R.; Ancoli-Israel, S. Determinants of nasal CPAP compliance. Sleep Med. 2002, 3, 239–247. [Google Scholar] [CrossRef]
- McKee, G.J.; Miljkovic, D. Data Aggregation and Information Loss; Technical Report 9843; American Agricultural Economics Association: Ames, IA, USA, 2007. [Google Scholar]
- Orcutt, G.H.; Watts, H.W.; Edwards, J.B. Data Aggregation and Information Loss. Am. Econ. Rev. 1968, 58, 773–787. [Google Scholar]
- Ye, L.; Pien, G.W.; Ratcliffe, S.J.; Björnsdottir, E.; Arnardottir, E.S.; Pack, A.I.; Benediktsdottir, B.; Gislason, T. The different clinical faces of obstructive sleep apnoea: A cluster analysis. Eur. Respir. J. 2014, 44, 1600–1607. [Google Scholar] [CrossRef] [Green Version]
- Gagnadoux, F.; Le Vaillant, M.; Paris, A.; Pigeanne, T.; Leclair-Visonneau, L.; Bizieux-Thaminy, A.; Alizon, C.; Humeau, M.P.; Nguyen, X.L.; Rouault, B. Relationship between OSA clinical phenotypes and CPAP treatment outcomes. Chest 2016, 149, 288–290. [Google Scholar] [CrossRef] [Green Version]
- Bailly, S.; Destors, M.; Grillet, Y.; Richard, P.; Stach, B.; Vivodtzev, I.; Timsit, J.F.; Lévy, P.; Tamisier, R.; Pépin, J.L.; et al. Obstructive sleep apnea: A cluster analysis at time of diagnosis. PLoS ONE 2016, 11, e0157318. [Google Scholar] [CrossRef] [Green Version]
- Subramani, Y.; Singh, M.; Wong, J.; Kushida, C.A.; Malhotra, A.; Chung, F. Understanding phenotypes of obstructive sleep apnea: Applications in anesthesia, surgery, and perioperative medicine. Anesth. Analg. 2017, 124, 179. [Google Scholar] [CrossRef]
- Smith, I.; Lasserson, T.; Haniffa, M. Interventions to improve use of continuous positive airway pressure for obstructive sleep apnoea. Cochrane Database Syst. Rev. 2004, 18. [Google Scholar] [CrossRef]
- Babbin, S.F.; Velicer, W.F.; Aloia, M.S.; Kushida, C.A. Identifying longitudinal patterns for individuals and subgroups: An example with adherence to treatment for obstructive sleep apnea. Multivar. Behav. Res. 2015, 50, 91–108. [Google Scholar] [CrossRef]
- Hoeppner, B.B.; Goodwin, M.S.; Velicer, W.F.; Mooney, M.E.; Hatsukami, D.K. Detecting longitudinal patterns of daily smoking following drastic cigarette reduction. Addict. Behav. 2008, 33, 623–639. [Google Scholar] [CrossRef] [Green Version]
- Aloia, M.S.; Goodwin, M.S.; Velicer, W.F.; Arnedt, J.T.; Zimmerman, M.; Skrekas, J.; Harris, S.; Millman, R.P. Time series analysis of treatment adherence patterns in individuals with obstructive sleep apnea. Ann. Behav. Med. 2008, 36, 44–53. [Google Scholar] [CrossRef]
- Drake, C.L.; Roehrs, T.; Roth, T. Insomnia causes, consequences, and therapeutics: An overview. Depress. Anxiety 2003, 18, 163–176. [Google Scholar] [CrossRef]
- Imani, S.; Madrid, F.; Ding, W.; Crouter, S.; Keogh, E. Matrix Profile XIII: Time Series Snippets: A New Primitive for Time Series Data Mining. In Proceedings of the 2018 IEEE International Conference on Big Knowledge (ICBK), Singapore, 17–18 November 2018; pp. 382–389. [Google Scholar]
- Gharghabi, S.; Imani, S.; Bagnall, A.; Darvishzadeh, A.; Keogh, E. An Ultra-Fast Time Series Distance Measure to Allow Data Mining in More Complex Real-World Deployments; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Barandas, M.; Folgado, D.; Fernandes, L.; Santos, S.; Abreu, M.; Bota, P.; Liu, H.; Schultz, T.; Gamboa, H. TSFEL: Time Series Feature Extraction Library. SoftwareX 2020, 11, 100456. [Google Scholar] [CrossRef]
- Taskesen, E. pca. 2019. Available online: https://github.com/erdogant/pca (accessed on 21 April 2022).
- Lohninger, H. Fundamentals of Statistics; Epina Bookshelf; Harvard University Press: Cambridge, MA, USA, 2010; Volume 5. [Google Scholar]
- Fabozzi, F.J.; Focardi, S.M.; Rachev, S.T.; Arshanapalli, B.G. The Basics of Financial Econometrics: Tools, Concepts, and Asset Management Applications; John Wiley & Sons: Hoboken, NJ, USA, 2014. [Google Scholar]
- Reynolds, D.A. Gaussian Mixture Models. Encycl. Biom. 2009, 741, 659–663. [Google Scholar]
- Povinelli, R.J.; Johnson, M.T.; Lindgren, A.C.; Ye, J. Time series classification using Gaussian mixture models of reconstructed phase spaces. IEEE Trans. Knowl. Data Eng. 2004, 16, 779–783. [Google Scholar] [CrossRef] [Green Version]
- Eirola, E.; Lendasse, A. Gaussian mixture models for time series modelling, forecasting, and interpolation. In International Symposium on Intelligent Data Analysis; Springer: Berlin/Heidelberg, Germany, 2013; pp. 162–173. [Google Scholar]
- Krishnan Nair, K.; Kiremidjian, A.S. Time Series Based Structural Damage Detection Algorithm Using Gaussian Mixtures Modeling. J. Dyn. Syst. Meas. Control 2006, 129, 285–293. [Google Scholar] [CrossRef]
- Reddy, A.; Ordway-West, M.; Lee, M.; Dugan, M.; Whitney, J.; Kahana, R.; Ford, B.; Muedsam, J.; Henslee, A.; Rao, M. Using Gaussian Mixture Models to Detect Outliers in Seasonal Univariate Network Traffic. In Proceedings of the 2017 IEEE Security and Privacy Workshops (SPW), San Jose, CA, USA, 25 May 2017; pp. 229–234. [Google Scholar]
- Le, T.Q.; Cheng, C.; Sangasoongsong, A.; Bukkapatnam, S.T.S. Prediction of sleep apnea episodes from a wireless wearable multisensor suite. In Proceedings of the 2013 IEEE Point-of-Care Healthcare Technologies (PHT), Bangalore, India, 16–18 January 2013; pp. 152–155. [Google Scholar]
- MacQueen, J. Some methods for classification and analysis of multivariate observations. In Proceedings of the Fifth Berkeley Symposium on Mathematical Statistics and Probability, Oakland, CA, USA, 21 June 1967; Volume 1, pp. 281–297. [Google Scholar]
- Akogul, S.; Erisoglu, M. A Comparison of Information Criteria in Clustering Based on Mixture of Multivariate Normal Distributions. Math. Comput. Appl. 2016, 21, 34. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, J.M.; Beymer, P.N.; Anderson, D.J.; van Lissa, C.; Schmidt, J.A. tidyLPA: An R Package to Easily Carry Out Latent Profile Analysis (LPA) Using Open-Source or Commercial Software. J. Open Source Softw. 2018, 3, 978. [Google Scholar] [CrossRef] [Green Version]
- Banfield, J.D.; Raftery, A.E. Model-Based Gaussian and Non-Gaussian Clustering. Biometrics 1993, 49, 803–821. [Google Scholar] [CrossRef]
- Seghouane, A.K.; Bekara, M. A small sample model selection criterion based on Kullback’s symmetric divergence. IEEE Trans. Signal Process. 2004, 52, 3314–3323. [Google Scholar] [CrossRef]
- Sclove, S.L. Application of model-selection criteria to some problems in multivariate analysis. Psychometrika 1987, 52, 333–343. [Google Scholar] [CrossRef]
- Biernacki, C.; Celeux, G.; Govaert, G. Assessing a Mixture Model for Clustering with the Integrated Classification Likelihood. IEEE Trans. Pattern Anal. Mach. Intell.—PAMI 1997, 22, 719–725. [Google Scholar] [CrossRef]
- Gasa, M.; Tamisier, R.; Launois, S.H.; Sapene, M.; Martin, F.; Stach, B.; Grillet, Y.; Levy, P.; Pepin, J.L. Residual sleepiness in sleep apnea patients treated by continuous positive airway pressure. J. Sleep Res. 2013, 22, 389–397. [Google Scholar] [CrossRef]
- Balakrishnama, S.; Ganapathiraju, A. Linear Discriminant Analysis—A Brief Tutorial. Inst. Signal Inf. Process. 1998, 18, 1–8. [Google Scholar]
- Pollicina, I.; Maniaci, A.; Lechien, J.R.; Iannella, G.; Vicini, C.; Cammaroto, G.; Cannavicci, A.; Magliulo, G.; Pace, A.; Cocuzza, S.; et al. Neurocognitive Performance Improvement after Obstructive Sleep Apnea Treatment: State of the Art. Behav. Sci. 2021, 11, 180. [Google Scholar] [CrossRef]
- Yeghiazarians, Y.; Jneid, H.; Tietjens, J.R.; Redline, S.; Brown, D.L.; El-Sherif, N.; Mehra, R.; Bozkurt, B.; Ndumele, C.E.; Somers, V.K.; et al. Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e56–e67. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| #Comps | LL | AIC | AWE | CAIC | KIC | SABIC | ICL |
|---|---|---|---|---|---|---|---|
| 1 | −331,566 | 663,173 | 663,594 | 663,355 | 663,196 | 663,271 | −663,335 |
| 2 | −323,953 | 647,988 | 648,855 | 648,361 | 648,032 | 648,189 | −654,536 |
| 3 | −319,721 | 639,567 | 640,878 | 640,130 | 639,632 | 639,871 | −648,605 |
| 4 | −318,231 | 636,627 | 638,383 | 637,381 | 636,713 | 637,035 | −649,319 |
| 5 | −317,349 | 634,907 | 637,108 | 635,852 | 635,014 | 635,417 | −650,038 |
| 6 | −316,502 | 633,254 | 635,899 | 634,390 | 633,382 | 633,867 | −650,552 |
| 7 | −315,985 | 632,261 | 635,351 | 633,588 | 632,410 | 632,978 | −650,243 |
| 8 | −315,801 | 631,936 | 635,470 | 633,453 | 632,106 | 632,756 | −653,016 |
| Comp | % Elements | avg (h/Night) | std | std*2 | Energy | avg/std | Status |
|---|---|---|---|---|---|---|---|
| 1 | 6.85% | 3.69 | 1.64 | 3.29 | 110.61 | 2.24 | Struggling |
| 2 | 7.30% | 6.87 | 3.02 | 6.05 | 206.17 | 2.27 | Unstable |
| 3 | 8.29% | 4.85 | 1.69 | 3.37 | 145.63 | 2.88 | Pre-adaptation |
| 4 | 17.51% | 6.21 | 1.96 | 3.93 | 186.20 | 3.16 | Adapted |
| 5 | 13.76% | 5.56 | 1.47 | 2.94 | 166.82 | 3.79 | Highly adapted |
| 6 | 13.15% | 7.90 | 1.75 | 3.50 | 236.90 | 4.52 | Good |
| 7 | 20.68% | 7.07 | 1.05 | 2.10 | 212.10 | 6.72 | Ideal |
| 8 | 12.46% | 8.55 | 1.14 | 2.27 | 256.54 | 7.52 | Plain |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, J.F., Jr.; Bailly, S.; Pepin, J.-L.; Goeuriot, L.; Spadon, G.; Amer-Yahia, S. CPAP Adherence Assessment via Gaussian Mixture Modeling of Telemonitored Apnea Therapy. Appl. Sci. 2022, 12, 7618. https://doi.org/10.3390/app12157618
Rodrigues JF Jr., Bailly S, Pepin J-L, Goeuriot L, Spadon G, Amer-Yahia S. CPAP Adherence Assessment via Gaussian Mixture Modeling of Telemonitored Apnea Therapy. Applied Sciences. 2022; 12(15):7618. https://doi.org/10.3390/app12157618
Chicago/Turabian StyleRodrigues, Jose F., Jr., Sebastien Bailly, Jean-Louis Pepin, Lorraine Goeuriot, Gabriel Spadon, and Sihem Amer-Yahia. 2022. "CPAP Adherence Assessment via Gaussian Mixture Modeling of Telemonitored Apnea Therapy" Applied Sciences 12, no. 15: 7618. https://doi.org/10.3390/app12157618