
Effect of COVID-19 on Selected Characteristics of Life Satisfaction Reflected in a Fuzzy Model


Abstract
:Featured Application
Abstract
1. Introduction
- -
- general opinion about one’s own well-being and satisfaction;
- -
- physical condition—physical everyday issues;
- -
- satisfaction with work and its results.
- They observed that the overall prevalence of
- -
- emotional exhaustion was 34.1%;
- -
- depersonalization was 12.6%;
- -
- lack of personal accomplishment was 15.2%.
- The main risk factors were found to be
- -
- younger age;
- -
- less social support;
- -
- low family and co-worker preparedness to cope with the COVID-19 outbreak;
- -
- increased sense of threat of COVID-19 virus;
- -
- longer time working in quarantined areas;
- -
- working in a high-risk environment;
- -
- working in hospitals with inadequate and insufficient material and human resources;
- -
- higher workload;
- -
- lower level of specialized COVID-19 training [22].
- Several factors significantly increased the likelihood of at-risk well-being:
- -
- lower levels of resilience;
- -
- use of support resources;
- -
- lack of organization understanding of the emotional support needs of healthcare workers;
- -
- increased workload;
- -
- insufficient personal protective equipment;
- -
- staff was insufficient to safely care for patients;
- -
- lower levels of psychological safety.
- Several factors were found to be significantly associated with higher levels of resilience:
- -
- positive perceptions of the organization’s understanding of the emotional support needs;
- -
- belief that sufficient educational resources were available regarding COVID-19 patient care;
- -
- positive perceptions of support from direct supervisors;
- -
- positive perceptions of staff redeployment policies;
- -
- -
- definition of the task and how it can be accomplished using fuzzy sets;
- -
- definition of linguistic variables and their fuzzy equivalents;
- -
- definition of membership functions;
- -
- definition of a set of fuzzy rules for these variables;
- -
- choice of defuzzification method.
2. Materials and Methods
2.1. Materials
2.2. Methods
2.3. Statistical Analysis
2.4. Computational Methods
- aggregation of premises in the rules—PROD;
- implication—MIN;
- aggregation of results from the rules (accumulation)—MAX;
- defuzzification—center of gravity (COG).
- -
- PSS10—Perceived Stress Score
- range of values XPSS = (0;40);
- general interpretation: the higher value means the worse situation;
- specificity of the interpretation suggests three potential output states.
- -
- SWLS
- range of values XSWLS = (5;35);
- general interpretation: a lower value means a worse situation;
- specificity of the interpretation suggests six potential output states; however, as the numerical interval is narrow, we paired the context of the outputs, obtaining finally three potential output states.
- -
- NMQ—Nordic Musculoskeletal Questionnaire
- range of values XNMQ = (0;40);
- general interpretation: ahigher value means aworse situation;
- there is no specific number of output interpretations.
- -
- “Emotional exhaustion” Xem
- range of values Xem = (0;54);
- general interpretation: a higher value means a worse psychological condition.
- -
- “Depersonalization” Xdep
- range of values Xdep = (0;30);
- general interpretation: a higher value means a worse psychological condition.
- -
- “Lack of personal achievements” Xachiev
- range of values Xachiev = (0;48);
- general interpretation: a lower value means a worse psychological condition—note that it is opposite to the other MBI factors.
- (a)
- PSS10 and SWLS—the respondent’s general opinion about their own life.
- (b)
- NMQ—physical state.
- (c)
- MBI factors—job burnout.
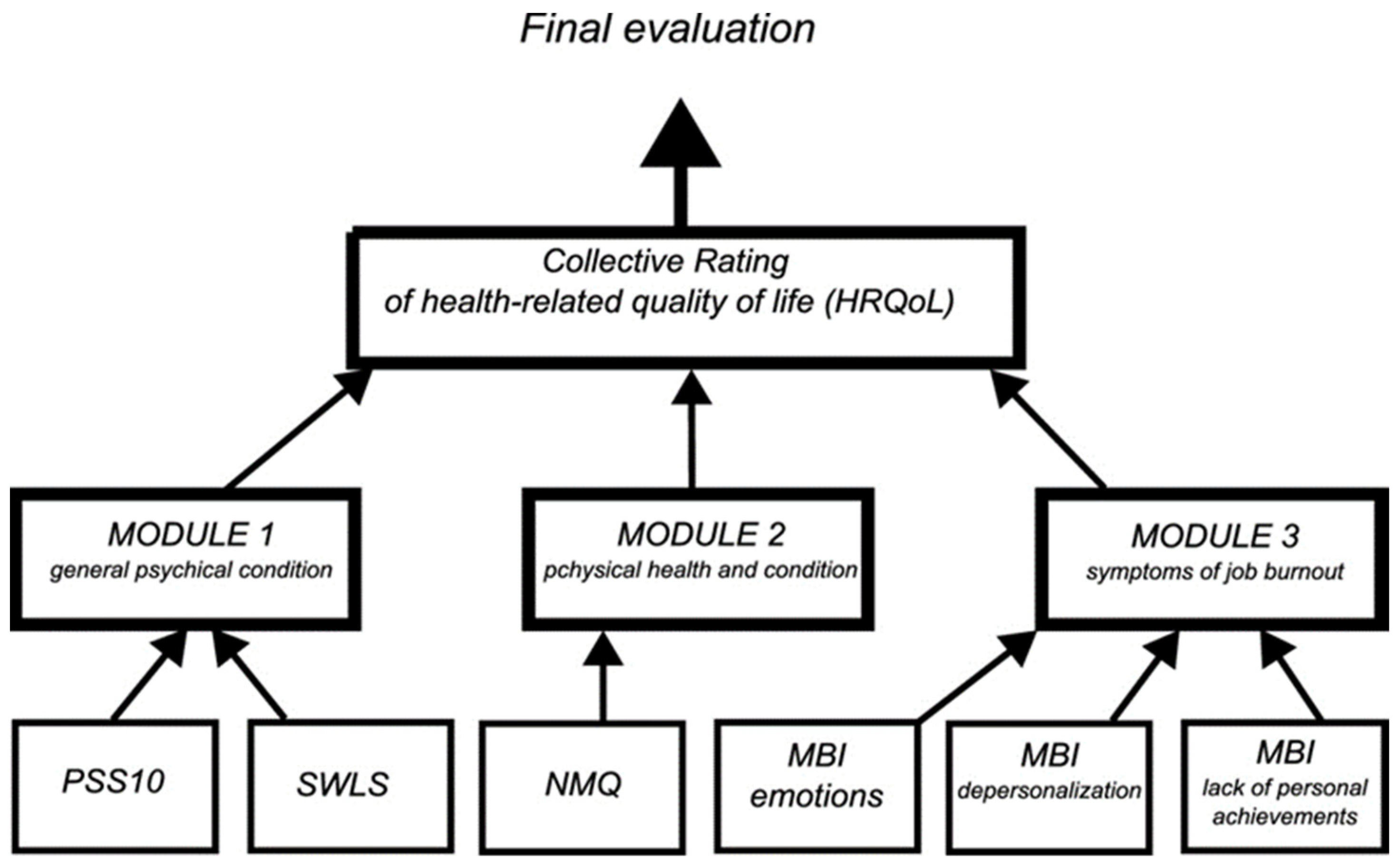
- Proposition 0
- Proposition 1
- -
- mental state assessment module—a system that collects data from the PSS10 (three linguistic values) and SWLS;
- -
- physical state assessment module—a system collecting data from the NMQ survey questionnaires;
- -
- burnout assessment module—based on MBI, but divided into 3 features: emotions, depersonalization, and lack of achievements; this was a simplified structure of the approach given inthe work of Prokopowicz and Mikołajewski [11].
- Proposition 2
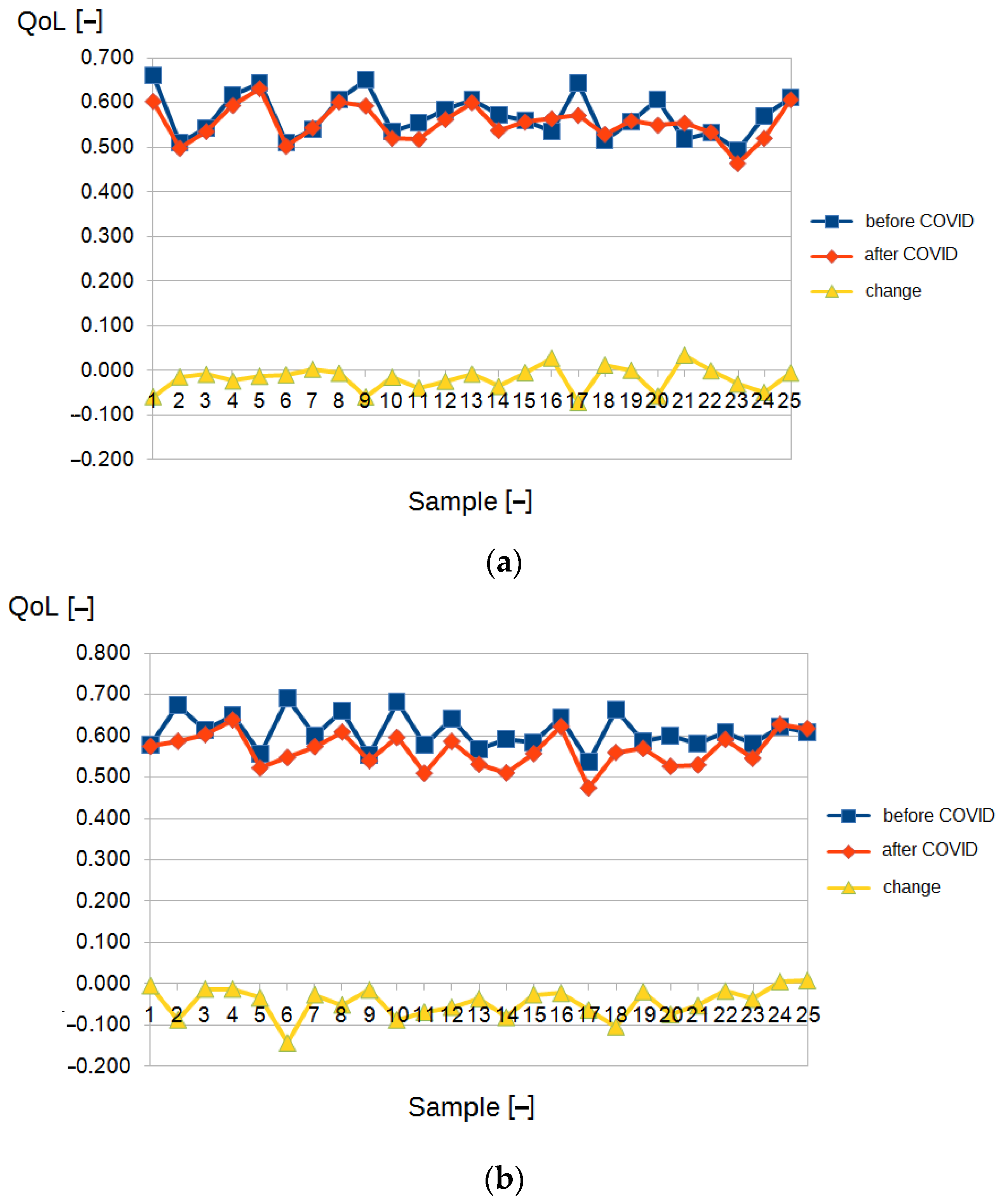
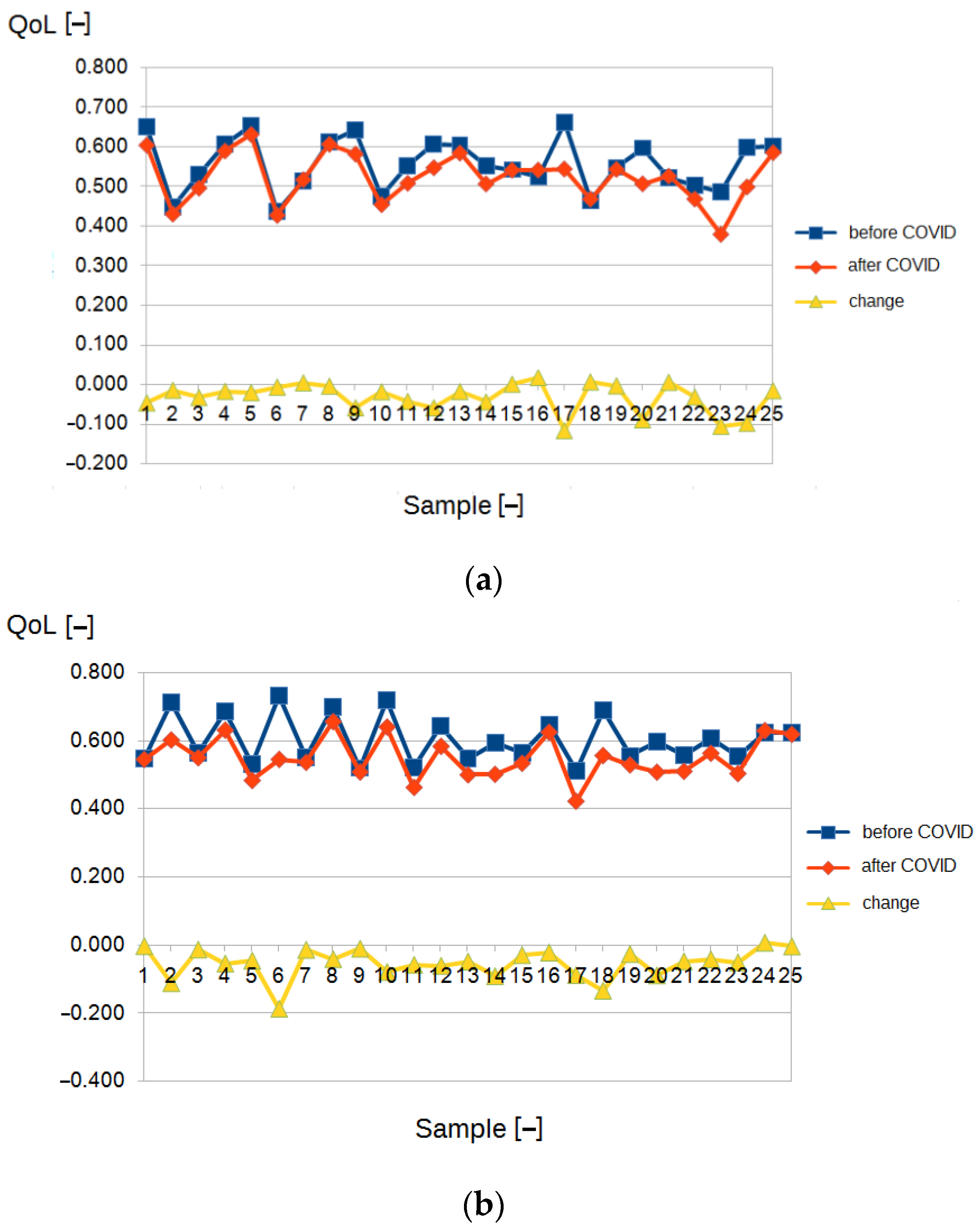
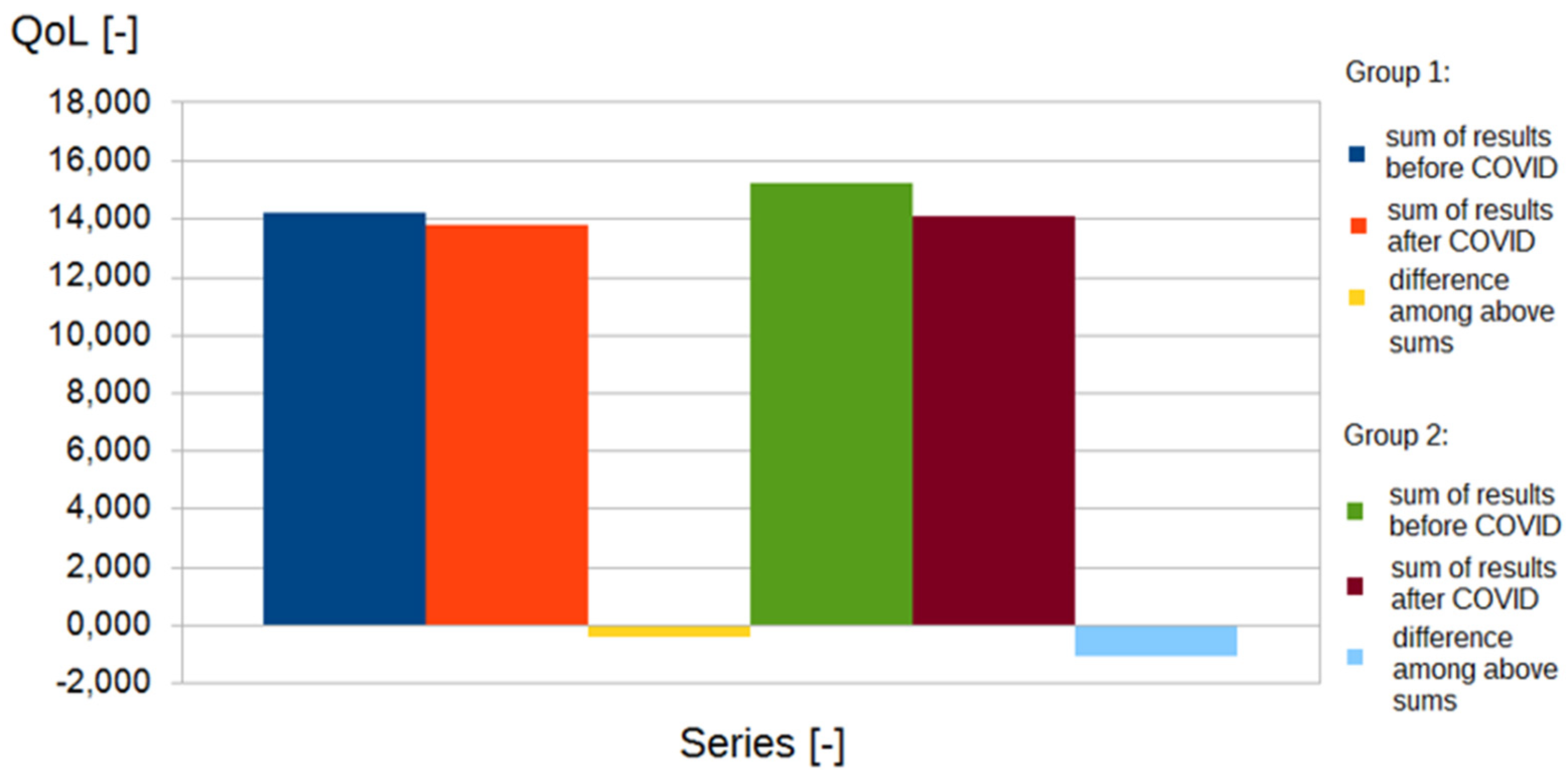
3. Results
3.1. General Results
3.2. Fuzzy Evaluation Models Summary
- -
- mental state assessment module—a system that collects data from the PSS10 and SWLS;
- -
- physical state assessment module—a system collecting data from the NMQ survey questionnaires;
- -
4. Discussion
- -
- fuzzy set theory (45%);
- -
- deterministic sensitivity analysis (31%);
- -
- probabilistic sensitivity analysis (15%);
- -
- Bayesian framework (6%);
- -
- grey theory (3%) [41].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | artificial intelligence |
| CADx | computer-aided diagnosis |
| CADe | computer-aided detection |
| CI | computational intelligence |
| COG | center of gravity |
| COVID-19 | corona virus disease 2019 |
| GDP | gross domestic product |
| HRQoL | Health-Related Quality of Life |
| NMQ | Nordic Musculoskeletal Questionnaire |
| MBI | Maslach Burnout Inventory |
| OFN | Ordered Fuzzy Numbers |
| PLUS | personal life usual satisfaction |
| PSS10 | Perceived Stress Score |
| Q1 | lower quartile |
| Q3 | upper quartile |
| QoL | Quality of Life |
| SD | standard deviation |
| SWLS | Satisfaction with Life Scale |
| TOPSIS | The Technique for Order of Preference by Similarity to Ideal Solution |
References
- Proto, E.; Rustichini, A. A Reassessment of the Relationship between GDP and Life Satisfaction. PLoS ONE 2013, 8, e79358. [Google Scholar] [CrossRef] [Green Version]
- Easterlin, R.A.; Angelescu, L. Happiness and growth the world over: Time series evidence on the happiness-income paradox. IZA Discuss. Papers 2009, 4060, 31. [Google Scholar] [CrossRef]
- Zhou, M.; Lin, W. Adaptability and Life Satisfaction: The Moderating Role of Social Support. Front. Psychol. 2016, 7, 1134. [Google Scholar] [CrossRef] [Green Version]
- Ruggeri, K.; Garcia-Garzon, E.; Maguire, Á.; Matz, S.; Huppert, F.A. Well-being is more than happiness and life satisfaction: A multidimensional analysis of 21 countries. Health Qual. Life Outcomes 2020, 18, 192. [Google Scholar] [CrossRef]
- Krys, K.; Park, J.; Kocimska-Zych, A.; Kosiarczyk, A.; Selim, H.A.; Wojtczuk-Turek, A.; Haas, B.W.; Uchida, Y.; Torres, C.; Capaldi, C.A.; et al. Personal Life Satisfaction as a Measure of Societal Happiness is an Individualistic Presumption: Evidence from Fifty Countries. J. Happiness Stud. 2021, 22, 2197–2214. [Google Scholar] [CrossRef]
- Zadeh, L. Fuzzy sets. Inf. Control 1965, 8, 338–353. [Google Scholar] [CrossRef] [Green Version]
- Zadeh, L. From computing with numbers to computing with words—from manipulation of measurements to manipulation of perceptions. Int. J. Appl. Math. Comput. Sci. 2002, 12, 307–324. [Google Scholar]
- Prokopowicz, P. The use of Ordered Fuzzy Numbers for modeling changes in dynamic processes. Inf. Sci. 2019, 470, 1–14. [Google Scholar] [CrossRef]
- Prokopowicz, P.; Mikołajewski, D.; Tyburek, K.; Mikołajewska, E. Computational gait analysis for post-stroke rehabilitation purposes using fuzzy numbers, fractal dimension and neural networks. Bull. Pol. Acad. Sci. Tech. Sci. 2020, 68, 191–198. [Google Scholar]
- Mikołajewska, E.; Prokopowicz, P.; Mikołajewski, D. Computational gait analysis using fuzzy logic for everyday clinical purposes—preliminary findings. Bio-Algorithms Med.-Syst. 2017, 13, 37–42. [Google Scholar] [CrossRef]
- Prokopowicz, P.; Mikołajewski, D. Fuzzy Approach to Computational Classification of Burnout—Preliminary Findings. Appl. Sci. 2022, 12, 3767. [Google Scholar] [CrossRef]
- Prokopowicz, P.; Mikołajewski, D.; Tyburek, K.; Mikołajewska, E.; Kotlarz, P. AI-Based Analysis of SelectedGaitParameters in Post-strokePatients. In Image Processing and Communications: Techniques, Algorithms and Applications, Advances in Intelligent Systems and Computing Book Series; Choraś, M., Ryszard, S.C., Eds.; Springer: Cham, Switzerland, 2020; Volume 1062, pp. 197–205. [Google Scholar] [CrossRef]
- Prokopowicz, P.; Mikołajewski, D.; Mikołajewska, E.; Kotlarz, P. Fuzzy System as an Assessment Tool for Analysis of the Health-Related Quality of Life for the People After Stroke. In Lecture Notes in Artificial Intelligence Book Series, Proceedings of the Artificial Intelligence and Soft Computing: 16th International Conference, ICAISC 2017, Zakopane, Poland, 11–15 June 2017; Rutkowski, L., Korytkowski, M., Scherer, R., Tadeusiewicz, R., Zadeh, L.A., Zurada, J.M., Eds.; Springer: Cham, Switzerland, 2017; pp. 710–721. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E. The Measurement of Experienced Burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Crawford, J.O. The Nordic Musculoskeletal Questionnaire. Occup. Med. 2007, 57, 300–301. [Google Scholar] [CrossRef] [Green Version]
- Baik, S.H.; Fox, R.S.; Mills, S.D.; Roesch, S.C.; Sadler, G.R.; Klonoff, E.A.; Malcarne, V.L. Reliability and validity of the Perceived Stress Scale-10 in Hispanic Americans with English or Spanish language preference. J. Health Psychol. 2019, 24, 628–639. [Google Scholar] [CrossRef]
- Wickramasinghe, N.D.; Dissanayake, D.S.; Abeywardena, G.S. Validity and reliability of the Maslach Burnout Inventory-Student Survey in Sri Lanka. BMC Psychol. 2018, 6, 52. [Google Scholar] [CrossRef]
- Descatha, A.; Roquelaure, Y.; Chastang, J.F.; Evanoff, B.; Melchior, M.; Mariot, C.; Ha, C.; Imbernon, E.; Goldberg, M.; Leclerc, A. Validity of Nordic-style questionnaires in the surveillance of upper-limb work-related musculoskeletal disorders. Scand. J. Work Environ. Health 2007, 33, 58–65. [Google Scholar] [CrossRef] [Green Version]
- García, G.M.; Calvo, J.C.A. The threat of COVID-19 and its influence on nursing staff burnout. J. Adv. Nurs. 2021, 77, 832–844. [Google Scholar] [CrossRef]
- Ruiz-Fernández, M.D.; Ramos-Pichardo, J.D.; Ibáñez-Masero, O.; Cabrera-Troya, J.; Carmona-Rega, M.I.; Ortega-Galán, Á.M. Compassion fatigue, burnout, compassion satisfaction and perceived stress in healthcare professionals during the COVID-19 health crisis in Spain. J. Clin. Nurs. 2020, 29, 4321–4330. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Nurses’ burnout and associated risk factors during the COVID-19 pandemic: A systematic review and meta-analysis. J. Adv. Nurs. 2021, 77, 3286–3302. [Google Scholar] [CrossRef]
- Jácome, C.; Seixas, A.; Serrão, C.; Teixeira, A.; Castro, L.; Duarte, I. Burnout in Portuguese physiotherapists during COVID-19 pandemic. Physiother. Res. Int. 2021, 26, e1915. [Google Scholar] [CrossRef]
- De Sire, A.; Marotta, N.; Raimo, S.; Lippi, L.; Inzitari, M.T.; Tasselli, A.; Gimigliano, A.; Palermo, L.; Invernizzi, M.; Ammendolia, A. Psychological distress and work environment perception by physical therapists from southern Italy during COVID-19 pandemic: The CALABRIA study. Int. J. Environ. Res. Public Health 2021, 18, 9676. [Google Scholar] [CrossRef]
- Munn, L.T.; Liu, T.L.; Swick, M.; Rose, R.; Broyhill, B.; New, L.; Gibbs, M. Original Research: Well-Being and Resilience Among Health Care Workers During the COVID-19 Pandemic: A Cross-Sectional Study. Am. J. Nurs. 2021, 121, 24–34. [Google Scholar] [CrossRef]
- Mikołajewska, E. Work-related musculoskeletal injuries in physiotherapists. Med. Pr. 2013, 64, 681–687. [Google Scholar] [CrossRef] [Green Version]
- Mikołajewska, E. Strategies of prevention of the work-related injuries in physiotherapists. Med. Pr. 2016, 67, 673–679. (In Polish) [Google Scholar] [CrossRef] [Green Version]
- Merlo, G.; Rippe, J. Physician Burnout: A Lifestyle Medicine Perspective. Am. J. Lifestyle Med. 2020, 15, 148–157. [Google Scholar] [CrossRef]
- Thukral, S.; Rana, V. Versatility of fuzzy logic in chronic diseases: A review. Med. Hypotheses 2019, 122, 150–156. [Google Scholar] [CrossRef]
- Azar, A.T.; Hassanien, A.E. Scientific Research Group in Egypt (SRGE). Editorial on: Fuzzy Logic in Biomedicine. Comput Biol. Med. 2015, 64, 321–322. [Google Scholar] [CrossRef]
- Barbounaki, S.; Vivilaki, V.G. A fuzzy intelligent system to assess midwives’ burnout conditions. Eur. J. Midwifery 2021, 6, 7. [Google Scholar] [CrossRef]
- Kosiński, W.; Prokopowicz, P.; Rosa, A. Defuzzification Functionals of Ordered Fuzzy Numbers. IEEE Trans. Fuzzy Syst. 2013, 21, 1163–1169. [Google Scholar] [CrossRef]
- Ahmadi, H.; Gholamzadeh, M.; Shahmoradi, L.; Nilashi, M.; Rashvand, P. Diseases diagnosis using fuzzy logic methods: A systematic and meta-analysis review. Comput. Methods Programs Biomed. 2018, 161, 145–172. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Julio, Y.F.; Prieto-Guevara, M.J.; Nieto-Bernal, W.; Meriño-Fuentes, I.; Guerrero-Avendaño, A. Framework for the Development of Data-Driven Mamdani-Type Fuzzy Clinical Decision Support Systems. Diagnostics 2019, 2, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farzandipour, M.; Nabovati, E.; Saeedi, S.; Fakharian, E. Fuzzy decision support systems to diagnose musculoskeletal disorders: A systematic literature review. Comput. Methods Programs Biomed. 2018, 163, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Rojek, I.; Mikołajewski, D.; Dostatni, E. Digital twins in product lifecycle for sustainability in manufacturing and maintenance. Appl. Sci. 2021, 11, 31. [Google Scholar] [CrossRef]
- Rojek, I.; Mikołajewski, D.; Dostatni, E.; Macko, M. AI-optimized technological aspects of the material used in 3D printing processes for selected medical applications. Materials 2020, 13, 5437. [Google Scholar] [CrossRef]
- Dubois, D.; Prade, H. Fuzzy Sets and Systems Theory and Applications; Academic Press: Boston, MA, USA, 1980. [Google Scholar]
- Clemente-Suárez, V.J.; Navarro-Jiménez, E.; Ruisoto, P.; Dalamitros, A.A.; Beltran-Velasco, A.I.; Hormeño-Holgado, A.; Laborde-Cárdenas, C.C.; Tornero-Aguilera, J.F. Performance of Fuzzy Multi-Criteria Decision Analysis of Emergency System in COVID-19 Pandemic. An Extensive Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 5208. [Google Scholar] [CrossRef]
- Zaidan, A.A.; Zaidan, B.B.; Al-Haiqi, A.; Kiah, M.L.; Hussain, M.; Abdulnabi, M. Evaluation and selection of open-source EMR software packages based on integrated AHP and TOPSIS. J.Biomed. Inform. 2015, 53, 390–404. [Google Scholar] [CrossRef] [Green Version]
- Broekhuizen, H.; Groothuis-Oudshoorn, C.G.; van Til, J.A.; Hummel, J.M.; IJzerman, M.J. A review and classification of approaches for dealing with uncertainty in multi-criteria decision analysis for healthcare decisions. Pharmacoeconomics 2015, 33, 445–455. [Google Scholar] [CrossRef] [Green Version]
- Moreno-Calderón, A.; Tong, T.S.; Thokala, P. Multi-criteria Decision Analysis Software in Healthcare Priority Setting: A Systematic Review. Pharmacoeconomics 2020, 38, 269–283. [Google Scholar] [CrossRef]
- Maija, K.; Katri, K. The moral orders of work and health: A case of sick leave due to burnout. Sociol. Health Illn. 2019, 41, 219–233. [Google Scholar] [CrossRef]
- Grensman, A.; Acharya, B.D.; Wändell, P.; Nilsson, G.; Werner, S. Health-related quality of life in patients with Burnout on sick leave: Descriptive and comparative results from a clinical study. Int. Arch. Occup. Environ. Health 2016, 89, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Mather, L.; Bergström, G.; Blom, V.; Svedberg, P. The covariation between burnout and sick leave due to mental disorders is explained by a shared genetic liability: A prospective swedish twin study with a five-year follow-up. Twin Res. Hum. Genet. 2014, 17, 535–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kärkkäinen, R.; Saaranen, T.; Hiltunen, S.; Ryynänen, O.P.; Räsänen, K. Systematic review: Factors associated with return to work in burnout. Occup. Med. 2017, 67, 461–468. [Google Scholar] [CrossRef] [Green Version]
- Byeon, H. Influence of the COVID-19 Pandemic on the Subjective Life Satisfaction of SouthKoreanAdults: Bayesian Nomogram Approach. Diagnostics 2022, 12, 761. [Google Scholar] [CrossRef]
- Kosinski, W.; Prokopowicz, P. Fuzziness–Representation of Dynamic Changes. In New Dimensions In FuzzyLogic And Related Technologies, Vol I, Proceedings; Stepnicka, M., Novak, V., Bodenhofer, U., Eds.; EuropeanSocFuzzy Log &Technol: Barcellona, Spain, 2007; pp. 449–456. [Google Scholar]
- Prokopowicz, P.; Golsefid, S.M.M. Aggregation Operator for Ordered Fuzzy Numbers Concerning the Direction. In Artificial Intelligence and Soft Computing. ICAISC 2014. Lecture Notes in Computer Science; Rutkowski, L., Korytkowski, M., Scherer, R., Tadeusiewicz, R., Zadeh, L.A., Zurada, J.M., Eds.; Springer: Cham, Switzerland, 2014; Volume 8467. [Google Scholar] [CrossRef]
- Prokopowicz, P.; Czerniak, J.; Mikołajewski, D.; Apiecionek, Ł.; Slezak, D. Theory and Applications of Ordered Fuzzy Number: A Tribute to Professor Witold Kosiński. In Studies in Fuzziness and Soft Computing; Springer: Berlin/Heidelberg, Germany, 2017; Volume 356. [Google Scholar]
- Vilela, M.; Oluyemi, G.; Petrovski, A. A holistic approach to assessment of value of information (VOI) with fuzzy data and decisioncriteria. Decis. Appl. Manag. Eng. 2020, 3, 97–118. [Google Scholar] [CrossRef]
- Pamucar, D.; Bozanic, D.; Puska, A.; Marinkovic, D. Application of neuro-fuzzy system for predicting the success of a company in public procurement. Decis. Appl. Manag. Eng. 2022, 5, 135–153. [Google Scholar] [CrossRef]
- Precup, R.-E.; Preitl, S.; Petriu, E.; Bojan-Dragos, C.-A.; Szedlak-Stinean, A.-I.; Roman, R.-C.; Hedrea, E.-L. Model-BasedFuzzy Control Results for Networked Control Systems. Rep. Mech. Eng. 2020, 1, 10–25. [Google Scholar] [CrossRef]
- Bozanic, D.; Tesic, D.; Marinkovic, D.; Milic, A. Modeling of neuro-fuzzy system as a support in decision-making processes. Rep. Mech. Eng. 2021, 2, 222–234. [Google Scholar] [CrossRef]
- Li, M.; Xiao, P. Network Blockchain Security Sharing Model Based on Fuzzy Logic. Comput. Intell Neurosci. 2022, 2022, 1509000. [Google Scholar] [CrossRef]
- Khan, S.; Iqbal, W.; Waheed, A.; Mehmood, G.; Khan, S.; Zareei, M.; Biswal, R.R. An Efficient and Secure Revocation-Enabled Attribute-Based Access Control for eHealth in Smart Society. Sensors 2022, 22, 336. [Google Scholar] [CrossRef]
- Medici, V.; Czlonkowska, A.; Litwin, T.; Giulivi, C. Diagnosis of Wilson Disease and Its Phenotypes by Using Artificial Intelligence. Biomolecules 2021, 11, 1243. [Google Scholar] [CrossRef] [PubMed]
- Luvizutto, G.J.; Silva, G.F.; Nascimento, M.R.; Sousa Santos, K.C.; Appelt, P.A.; de Moura Neto, E.; de Souza, J.T.; Wincker, F.C.; Miranda, L.A.; Hamamoto Filho, P.T.; et al. Use of artificial intelligence as an instrument of evaluation after stroke: A scoping review based on international classification of functioning, disability and health concept. Top. Stroke Rehabil. 2022, 29, 331–346. [Google Scholar] [CrossRef] [PubMed]
- Fleck, D.E.; Ernest, N.; Asch, R.; Adler, C.M.; Cohen, K.; Yuan, W.; Kunkel, B.; Krikorian, R.; Wade, S.L.; Babcock, L. Predicting Post-Concussion Symptom Recovery in Adolescents Using a Novel Artificial Intelligence. J. Neurotrauma 2021, 38, 830–836. [Google Scholar] [CrossRef]
- Berman, A.L.; Silverman, M.M. A Call to Clarify Fuzzy Sets. Crisis 2021, 42, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Ruotsalainen, P.; Blobel, B. Health Information Systems in the Digital Health Ecosystem-Problems and Solutions for Ethics, Trust and Privacy. Int. J. Environ. Res. Public Health 2020, 17, 3006. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group (n = 25, 100%) | Reference Group (n = 25, 100%) | |
|---|---|---|
| Age (years) | ||
| Mean | 26.92 | 26.12 |
| SD | 3.97 | 3.94 |
| Min | 22 | 22 |
| Q1 | 24 | 23 |
| Median | 25 | 25 |
| Q3 | 29 | 27 |
| Max | 34 | 35 |
| Seniority (years) | ||
| Mean | 3.2 | 3.36 |
| SD | 2.61 | 2.53 |
| Min | 1 | 1 |
| Q1 | 1 | 1.5 |
| Median | 2 | 3 |
| Q3 | 5 | 4 |
| Max | 8 | 9 |
| Gender: | ||
| Females (F) | 10 (40%) | 11 (44%) |
| Males (M) | 15 (60%) | 14 (56%) |
| Scale | PSS10 | MBI | SWLS | NMQ |
|---|---|---|---|---|
| Direction of change | the higher the score, the higher the stress | the higher the score, the higher the stress | the higher the score, the higher quality of living | the higher the score, the higher number of problems |
| Scoring | 1–4: low 7–10: high | three component scales: emotional exhaustion (9 items), depersonalization (5 items), and personal achievement (8 items), are measured separately | range of scores is 5–35, where 5–9 extremely dissatisfied with life, 20 neutral, 31–35 extremely satisfied with life | whether someone has problems with their locomotion and how often |
| Scale | PSS10 | MBI | SWLS | NMQ |
|---|---|---|---|---|
| Direction of change in group 1 (physiotherapists) after COVID-19 | higher stress | higher stress | lower quality of living | higher number of problems |
| Direction of change in group 2 (informaticians) after COVID-19 | lower stress | lower stress | higher quality of living | no change |
| Scale | PSS10 | MBI | SWLS | NMQ |
|---|---|---|---|---|
| Mean | 29.16 | 48.76 | 16.6 | 0.72 |
| SD | 2.43 | 14.68 | 4.06 | 0.73 |
| Min | 25 | 32 | 10 | 0 |
| Q1 | 28 | 38 | 14 | 1 |
| Median | 28 | 46 | 16 | 1 |
| Q3 | 31 | 52 | 18 | 1 |
| Max | 34 | 79 | 15 | 2 |
| Distribution | data are not normally distributed | data are not normally distributed | data are not normally distributed | data are not normally distributed |
| Mean | 30.6 | 57.24 | 14.96 | 0.73 |
| SD | 2.12 | 13.14 | 3.75 | 0.74 |
| Min | 27 | 39 | 8 | 0 |
| Q1 | 29.5 | 44.5 | 13 | 1 |
| Median | 30 | 55 | 14 | 1 |
| Q3 | 32 | 72 | 16 | 1 |
| Max | 35 | 79 | 25 | 2 |
| Distribution | data are not normally distributed | data are not normally distributed | data are not normally distributed | data are not normally distributed |
| Scale | PSS10 | MBI | SWLS | NMQ |
|---|---|---|---|---|
| Mean | 18.76 | 17.2 | 54.16 | 0.44 |
| SD | 3.38 | 2.72 | 16.67 | 0.51 |
| Min | 10 | 14 | 25 | 0 |
| Q1 | 17.5 | 15 | 44.5 | 0 |
| Median | 19 | 17 | 53 | 0 |
| Q3 | 21 | 18 | 69 | 1 |
| Max | 24 | 24 | 77 | 1 |
| Distribution | data are not normally distributed | data are not normally distributed | data are not normally distributed | data are not normally distributed |
| Mean | 16.24 | 13.88 | 63.6 | 0.48 |
| SD | 2.85 | 2.35 | 15.07 | 0.51 |
| Min | 10 | 10 | 41 | 0 |
| Q1 | 15 | 12.5 | 51 | 0 |
| Median | 16 | 14 | 64 | 0 |
| Q3 | 18 | 15 | 76 | 1 |
| Max | 21 | 20 | 87 | 1 |
| Distribution | data are not normally distributed | data are not normally distributed | data are not normally distributed | data are not normally distributed |
| Group 1 (Physical Therapists)—before COVID-19 | ||||
|---|---|---|---|---|
| Scale | PSS10 | MBI | SWLS | NMQ |
| PSS10 | - | 0.473 p = 0.016 | n.s. | n.s. |
| MBI | 0.473 p = 0.016 | - | n.s. | 0.440 p = 0.028 |
| SWLS | n.s. | n.s. | - | n.s. |
| NMQ | n.s. | 0.440 p = 0.028 | n.s. | - |
| Group 1 (Physical Therapists)—after COVID-19 | ||||
| PSS10 | - | 0.430 p = 0.032 | n.s. | n.s. |
| MBI | 0.430 p = 0.032 | - | −0.483 p = 0.015 | n.s. |
| SWLS | n.s. | −0.483 p = 0.015 | - | n.s. |
| NMQ | n.s. | n.s. | n.s. | - |
| Group 2 (Informaticians)—before COVID-19 | ||||
| PSS10 | - | n.s. | n.s. | n.s. |
| MBI | n.s. | - | n.s. | n.s. |
| SWLS | n.s. | n.s. | - | 0.805 p = 0.000 |
| NMQ | n.s. | n.s. | 0.805 p = 0.000 | - |
| Group 2 (Informaticians)—after COVID-19 | ||||
| PSS10 | - | n.s. | n.s. | n.s. |
| MBI | n.s. | - | n.s. | n.s. |
| SWLS | n.s. | n.s. | - | 0.528 p = 0.007 |
| NMQ | n.s. | n.s. | 0.528 p = 0.007 | - |
| No. | Physical Therapists | Informaticians | ||||
|---|---|---|---|---|---|---|
| Before COVID-19 | After COVID-19 | Change | Before COVID-19 | After COVID-19 | Change | |
| 1 | 0.660 | 0.603 | −0.058 | 0.579 | 0.574 | −0.004 |
| 2 | 0.511 | 0.498 | −0.014 | 0.674 | 0.587 | −0.087 |
| 3 | 0.543 | 0.535 | −0.008 | 0.615 | 0.603 | −0.012 |
| 4 | 0.616 | 0.594 | −0.023 | 0.650 | 0.638 | −0.012 |
| 5 | 0.643 | 0.631 | −0.012 | 0.556 | 0.522 | −0.034 |
| 6 | 0.511 | 0.502 | −0.009 | 0.691 | 0.547 | −0.144 |
| 7 | 0.540 | 0.543 | 0.004 | 0.600 | 0.574 | −0.026 |
| 8 | 0.607 | 0.601 | −0.005 | 0.660 | 0.609 | −0.051 |
| 9 | 0.651 | 0.593 | −0.058 | 0.554 | 0.540 | −0.014 |
| 10 | 0.534 | 0.520 | −0.014 | 0.684 | 0.596 | −0.088 |
| 11 | 0.556 | 0.518 | −0.038 | 0.578 | 0.509 | −0.069 |
| 12 | 0.585 | 0.562 | −0.023 | 0.643 | 0.586 | −0.057 |
| 13 | 0.607 | 0.600 | −0.007 | 0.567 | 0.531 | −0.036 |
| 14 | 0.572 | 0.538 | −0.035 | 0.591 | 0.510 | −0.081 |
| 15 | 0.560 | 0.557 | −0.004 | 0.583 | 0.557 | −0.026 |
| 16 | 0.535 | 0.564 | 0.029 | 0.645 | 0.622 | −0.023 |
| 17 | 0.642 | 0.571 | −0.071 | 0.537 | 0.474 | −0.064 |
| 18 | 0.516 | 0.529 | 0.013 | 0.664 | 0.559 | −0.104 |
| 19 | 0.557 | 0.559 | 0.002 | 0.588 | 0.569 | −0.019 |
| 20 | 0.606 | 0.549 | −0.056 | 0.600 | 0.526 | −0.074 |
| 21 | 0.519 | 0.554 | 0.035 | 0.582 | 0.529 | −0.053 |
| 22 | 0.533 | 0.533 | 0.000 | 0.608 | 0.591 | −0.017 |
| 23 | 0.493 | 0.464 | −0.030 | 0.582 | 0.545 | −0.037 |
| 24 | 0.568 | 0.520 | −0.048 | 0.621 | 0.627 | 0.006 |
| 25 | 0.611 | 0.607 | −0.004 | 0.608 | 0.617 | 0.009 |
| Min | 0.493 | 0.464 | −0.071 | 0.537 | 0.474 | −0.144 |
| Max | 0.660 | 0.631 | 0.035 | 0.691 | 0.638 | 0.009 |
| Mean | 0.571 | 0.554 | −0.017 | 0.610 | 0.566 | −0.045 |
| SD | 0.049 | 0.040 | 0.027 | 0.043 | 0.042 | 0.037 |
| Median | 0.564 | 0.555 | −0.013 | 0.604 | 0.571 | −0.036 |
| Q1 | 0.534 | 0.529 | −0.035 | 0.582 | 0.531 | −0.069 |
| Q3 | 0.607 | 0.593 | −0.004 | 0.645 | 0.596 | −0.017 |
| No. | Physical Therapists | Informaticians | ||||
|---|---|---|---|---|---|---|
| Before COVID-19 | After COVID-19 | Change | Before COVID-19 | After COVID-19 | Change | |
| 1 | 0.656 | 0.599 | −0.057 | 0.574 | 0.570 | −0.004 |
| 2 | 0.489 | 0.471 | −0.018 | 0.669 | 0.587 | −0.082 |
| 3 | 0.537 | 0.507 | −0.030 | 0.611 | 0.595 | −0.016 |
| 4 | 0.607 | 0.589 | −0.018 | 0.650 | 0.629 | −0.021 |
| 5 | 0.639 | 0.631 | −0.008 | 0.552 | 0.513 | −0.039 |
| 6 | 0.490 | 0.490 | 0.000 | 0.682 | 0.544 | −0.138 |
| 7 | 0.523 | 0.528 | 0.006 | 0.596 | 0.570 | −0.026 |
| 8 | 0.580 | 0.580 | 0.000 | 0.660 | 0.609 | −0.051 |
| 9 | 0.646 | 0.581 | −0.065 | 0.550 | 0.540 | −0.010 |
| 10 | 0.525 | 0.501 | −0.023 | 0.670 | 0.591 | −0.079 |
| 11 | 0.560 | 0.515 | −0.044 | 0.569 | 0.494 | −0.075 |
| 12 | 0.576 | 0.553 | −0.023 | 0.643 | 0.586 | −0.057 |
| 13 | 0.603 | 0.584 | −0.019 | 0,556 | 0.521 | −0.035 |
| 14 | 0.558 | 0.507 | −0.051 | 0.591 | 0.506 | −0.085 |
| 15 | 0.549 | 0.547 | −0.002 | 0.579 | 0.547 | −0.032 |
| 16 | 0.531 | 0.553 | 0.022 | 0.650 | 0.628 | −0.022 |
| 17 | 0.628 | 0.544 | −0.084 | 0.526 | 0.464 | −0.062 |
| 18 | 0.500 | 0.517 | 0.016 | 0.659 | 0.555 | −0.104 |
| 19 | 0.551 | 0.547 | −0.004 | 0.584 | 0.565 | −0.018 |
| 20 | 0.597 | 0.512 | −0.085 | 0.596 | 0.515 | −0.081 |
| 21 | 0.521 | 0.546 | 0.025 | 0.578 | 0.524 | −0.054 |
| 22 | 0.523 | 0.508 | −0.016 | 0.608 | 0.581 | −0.027 |
| 23 | 0.486 | 0.448 | −0.038 | 0.578 | 0.535 | −0.043 |
| 24 | 0.564 | 0.504 | −0.060 | 0.621 | 0.628 | 0.006 |
| 25 | 0.597 | 0.580 | −0.017 | 0.613 | 0.617 | 0.004 |
| Min | 0.486 | 0.448 | −0.085 | 0.526 | 0.464 | −0.138 |
| Max | 0.656 | 0.631 | 0.025 | 0.682 | 0.629 | 0.006 |
| Mean | 0.561 | 0.538 | −0.024 | 0.607 | 0.561 | −0.046 |
| SD | 0.050 | 0.043 | 0.030 | 0.044 | 0.045 | 0.036 |
| Median | 0.559 | 0.545 | −0.019 | 0.602 | 0.568 | −0.041 |
| Q1 | 0.523 | 0.507 | −0.044 | 0.578 | 0.524 | −0.075 |
| Q3 | 0.597 | 0.580 | −0.002 | 0.650 | 0.591 | −0.021 |
| Group 1 (Physical Therapists) | ||
|---|---|---|
| Scale | Model 1 | Model 2 |
| Change in PSS10 | −0.493 p = 0.012 | −0.484 p = 0.014 |
| Change in MBI | n.s. | −0.161 p = 0.044 |
| Change in SWLS | 0.278 p = 0.001 | 0.369 p = 0.069 |
| Change in NMQ | n.s. | 0.039 p = 0.049 |
| Group 2 (Informaticians) | ||
| Change in PSS10 | n.s. | 0.157 p = 0.009 |
| Change in MBI | n.s. | 0.390 p = 0.009 |
| Change in SWLS | −0.322 p = 0.012 | −0.283 p = 0.016 |
| Change in NMQ | −0.350 p = 0.046 | −0.390 p = 0.044 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mikołajewski, D.; Prokopowicz, P. Effect of COVID-19 on Selected Characteristics of Life Satisfaction Reflected in a Fuzzy Model. Appl. Sci. 2022, 12, 7376. https://doi.org/10.3390/app12157376
Mikołajewski D, Prokopowicz P. Effect of COVID-19 on Selected Characteristics of Life Satisfaction Reflected in a Fuzzy Model. Applied Sciences. 2022; 12(15):7376. https://doi.org/10.3390/app12157376
Chicago/Turabian StyleMikołajewski, Dariusz, and Piotr Prokopowicz. 2022. "Effect of COVID-19 on Selected Characteristics of Life Satisfaction Reflected in a Fuzzy Model" Applied Sciences 12, no. 15: 7376. https://doi.org/10.3390/app12157376