1. Introduction
Deep Bite
A deep bite is characterized by excessive vertical overlap of the lower incisors by the upper incisors in maximum intercuspation. A deep bite is a feature of malocclusion that can be dental, skeletal or a combination of both [
1]. A deep bite is often associated with a retroclination and extrusion of the upper and lower front teeth, a loss of vertical posterior dimension or a combination of both. A skeletal deep bite is characterized by a counterclockwise rotation of the mandible [
2,
3,
4,
5,
6,
7,
8,
9].
Orthodontic treatment has the objective to level the curve of Spee with the intrusion of the upper/lower anterior teeth and the extrusion of the posterior teeth, or both. It is advisable to understand which is the best approach according to the exposure of the incisors in the smile [
10]. In particular, if a patient has a deep bite associated with a gingival smile (
Figure 1), it will be advisable to program the intrusion of the upper incisors. On the contrary, as it often happens, if the patient has good exposure of the upper incisors to the smile and a deep bite, it will be necessary to project a greater intrusion of the lower incisors and an extrusion of the posterior teeth (
Figure 2) [
11,
12].
The development of orthodontic therapies with transparent aligners has prompted many clinicians to investigate their effectiveness and efficiency in detail [
13,
14,
15,
16,
17,
18,
19]. Several companies entered the orthodontic aligner market over the years, and Invisalign established itself as the industry leader in the number of patients treated, the number of service providers and technological advancement. This also allowed for greater scientific production [
20,
21,
22,
23,
24,
25].
Fixed orthodontic multibracket appliance (
Figure 3) may be useful to level the curve of Spee more than aligners because aligners’ “bite block” effect can produce posterior teeth intrusion or not allow posterior teeth extrusion. This effect can be reduced by the application of precision bite ramps on palatal upper anterior teeth [
26,
27,
28,
29]. If a deep bite can be solved just with upper and lower anterior teeth proclination and relative intrusion, aligners can perform like fixed appliances. If the treatment has the objective to intrude lower incisors and extrude posterior teeth, aligners have some difficulty making it possible [
30,
31].
The aim of this paper is to present two clinical cases of deep bite treatment and to propose a novel deep bite treatment protocol with Invisalign orthodontic aligners.
2. Materials and Methods: Deep Bite Protocol with Aligners
2.1. Attachments
Since aligners need retention to express vertical movements, such as extrusion or intrusion of posterior teeth, it is useful that the application of retention by conventional horizontal rectangular attachments are 4 mm large on premolars and, if possible, 5 mm on canines (
Figure 4). If extrusion of the premolars is desired, the attachment design is modified from horizontal rectangular to gingival beveled (
Figure 5). The attachments of this shape and dimension are necessary to improve the surface of force application to premolars and canines and to prevent dislodgement of aligners during an anterior intrusion.
2.2. Working Setup
In fixed multibracket therapies, deep bite correction may require the use of reverse curve archwires that determine an overcorrection of the deep bite to obtain more intrusion of anterior teeth and extrusion of posterior teeth. With aligners, it is not possible to add a reverse curve arch, but it can be possible to design a virtual setup in order to overcorrect the position of the teeth such as the shape of a reverse curve archwire (
Figure 6). Virtual setup is composed of a series of overcorrected dental final positions (
Figure 7).
2.3. Staging
Staging is the sequence of movements generated by the virtual setup. Staging is represented by a diagram showing each aligner and which corresponding teeth are moved. Staging can involve simultaneous movements of all teeth or only of some teeth for some aligners, and of other teeth on other aligners, such as working with a segmented orthodontic technique. In deep bite correction, orthodontic movements are provided with the sequence called “frog staging” (
Figure 8) for the intrusion movement of the anterior sector. In particular, the intrusion is programmed first on lower canines, then on incisors, again on canines, subsequently again on incisors and so on. In this way, the number of aligners increases and, consequently, the treatment duration increases, but the predictability of the movement is improved. In fact, movements are directed on some teeth while the other teeth, not moving, act as anchoring units.
3. Case Report Number 1
The first case reported was an adult male patient who had already undergone orthodontic treatment in the past with the extraction of the four first premolars. The orthodontic situation (
Figure 9,
Figure 10 and
Figure 11 and
Table 1) showed a dentoskeletal class II malocclusion, upper and lower crowding, severe deep bite with impingement of the lower incisors on the palate, retroclination of the upper and lower incisors, and convex and biretruded profile. The patient was strongly brachyfacial, and therefore, a deep bite was not only dental but also skeletal. The patient showed good exposure of the upper incisors; therefore, in the resolution of the deep bite, it was preferable not to intrude upper incisors in order not to worsen the patient’s aesthetics.
The treatment was conducted exclusively with clear aligners and followed the protocol for the resolution of the deep bite that was described above. It lasted approximately 18 months, with only one little refinement. At the end of the treatment, the resolution of the deep bite and an important leveling of the patient’s curve of Spee was clearly evident, as can be seen in the comparison between the initial and final orthopantomography.
The exposure of the lower incisors at the end of the treatment was normal, the upper and lower crowding was resolved, and the dental class was corrected. In fact, at the end of the treatment, the patient was in molar and canine class I. Cephalometric analysis (
Table 2) showed skeletal deep bite, skeletal class II, and better inclination of upper and lower incisors. At the end of the treatment, intra- and extra-oral photos of the patient and X-rays were taken (
Figure 12 and
Figure 13) and, after few days, a removable Essix for long-term retention was delivered. Final cephalometric tracing is showed in
Figure 14.
4. Case Report Number 2
The second case was concerned with the orthodontic treatment with transparent aligners of a growing patient with dentoskeletal class II malocclusion, scissor bite of the first right upper premolar, a slight contraction of the upper and lower arches, lower dental crowding and an interincisive diastema.
The patient also had good exposure to their smile and deep bite, so it was indicated to correct the deep bite by leveling the lower arch with the intrusion of the canines and incisors (
Figure 15 and
Figure 16).
The patient presented a skeletal class II malocclusion, a normodivergent growth pattern, excessive proclination of the upper incisors and a normoinclination of the lower incisors (
Figure 17 and
Table 3).
An orthodontic therapy with transparent aligners was performed with all components of the protocol just described: horizontal rectangular attachments on the posterior teeth and lower canines, frog staging and over-correction of the final setup.
Furthermore, when the lower leveling and upper expansion phases were completed, the patient was asked to wear class II intermaxillary elastics.
Thanks to the patient’s excellent collaboration, the optimal biomechanical control of the aligners and the patient’s growth, the treatment was successfully carried out in 18 months, reaching a dental class I, a resolution of crowding, a median diastema closure and deep bite resolution.
The leveling of the lower arch and the coordination of the arches made it possible to treat the dental class II using intermaxillary elastics (
Figure 18,
Figure 19 and
Figure 20 and
Table 4). At the end of the treatment, the patient was asked to wear removable Essix for long-term retention.
5. Discussion
Most papers agree that a deep bite is difficult to treat with aligners, and anterior intrusion and posterior extrusion are difficult to achieve, but not all papers share the same opinion.
Although the patients had different malocclusions (the patient in case number 1 had undergone an extractive treatment in the past and had a relapse, while the patient in case number 2 had a class II malocclusion with complete dentition), the same protocol to treat their deep bite malocclusion was effective. It is also important to report that both cases had dental arch contraction and crowding. The resolution of these two features of malocclusion helped with the correction of the deep bite because it was in part corrected with the relative intrusion of the anterior lower teeth. Relative intrusion is a combination of intrusion and labial tipping.
Krieger et al., stated that the vertical movements of intrusion and extrusion are more difficult with the aligners [
30].
From the systematic review by Galan-Lopez et al., knowledge emerged that the least predictable movements with Invisalign are rotations and vertical movements [
32].
According to a recent review of the literature conducted by Papadimitriou on the efficacy of Invisalign therapy on different types of malocclusions, Invisalign was found to be effective for tipping and rotation movements. Moreover, the results of Invisalign therapies may be comparable with those of fixed multibracket therapies in the case of little or medium crowdings in adult patients who do not require extractions [
33,
34].
Invisalign was found not to be very effective in arch expansions through a bodily movement of the teeth, in the closure of the extraction spaces, in the correction of vertical occlusal contacts and in the resolution of major malocclusions. It has been found that some malocclusions, such as minor dental misalignments or anterior dental open bites, can be treated with more prediction using aligners [
29,
35].
On the contrary, malocclusions characterized by a deep bite are more complex to treat [
36]. A study by Douglas Henik et al. analyzed patients with skeletal deep bites treated with Invisalign G5 and virtual bite ramps versus patients treated with fixed orthodontic devices. This study showed that there is no difference in the effectiveness of treatment between fixed and Invisalign equipment [
31].
Additionally, according to Yang Liu and Wei Hu, the correction of a deep bite was difficult with the transparent aligners. Deep bite correction involves the extrusion of the posterior teeth and the intrusion of the anterior or both movements. The choice depends on some factors, such as the exposure of the gum of the incisors during a smile and the vertical dimension. The intrusion of the incisors was simple to obtain, while the extrusion of the posterior teeth was not favored by the Invisalign because covering the occlusal surface prevented their extrusion [
36,
37]. Roozbeh Khosravi et al. agreed that the resolution of a deep bite with the Invisalign aligners occurred only through an intrusion movement of the incisors and not also an extrusion of the posterior sectors [
38].
The purpose of these case reports is to show the clinical results of an orthodontic treatment protocol with transparent aligners to solve malocclusion associated with severe deep bites. Anchorage attachments are very important for transfering the pressure desired to intrude anteriors without disengaging the aligners on posterior teeth and favour posterior extrusion. If the intrusion of anterior teeth is associated with proclination, then a deep bite is easier to solve. Moving teeth with frog staging increase the number of aligners than traditional methods and may improve predictability. Finally, overengineering the dental final setup is an attempt to exceed the limits of the amount of vertical movements performed with aligners. In case number 1, anterior teeth were proclined and intruded at the same time without excessing lower incisor proclination, and the arches were expanded with uprighting of posterior segments and improvement in the vertical dimension. In case number 2, a deep bite was associated with class II skeletal malocclusion. The patient had favourable growth of the mandible that helped the correction of deep bites.
6. Conclusions
The treatment of deep bites with transparent aligners can be approached with good predictability using the protocol described in these two clinical cases. However, a more in-depth analysis and larger case histories with the same protocol are needed.
Author Contributions
Conceptualization, G.C., E.P., A.D.I., A.P. and S.C.; methodology, A.D.I., D.D.V. and G.D. software, I.R.B. and S.C.; validation, E.P. and D.D.V.; formal analysis, F.C., A.P. and S.C.; investigation, G.C. and E.P., resources, I.R.B. and F.I.; data curation, G.C., F.C. and E.P.; writing—original draft preparation, G.C., A.P. and S.C.; writing—review and editing, F.I. and G.D.; visualization, F.I. and I.R.B.; supervision, G.D., D.D.V. and F.I.; project administration, G.D., E.P. and A.D.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The present clinical study was based at the University of Bari (Italy), in full accordance with ethical principles, including the World Medical Association Declaration of Helsinki and the additional requirements of Italian law. Furthermore, the University of Bari, Italy, classified the study as exempt from ethical review as it carries only negligible risk and involves the use of existing data that contain only non-identifiable data about human beings. The patient signed a written informed consent form.
Informed Consent Statement
Informed consent was obtained from the subjects involved in the study. Written informed consent was obtained from the patients to publish this paper.
Data Availability Statement
All experimental data to support the findings of this study are available by contacting the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Danz, J.C.; Greuter, C.; Sifakakis, I.; Fayed, M.; Pandis, N.; Katsaros, C. Stability and Relapse after Orthodontic Treatment of Deep Bite Cases-a Long-Term Follow-up Study. Eur. J. Orthod. 2014, 36, 522–530. [Google Scholar] [CrossRef]
- Fattahi, H.; Pakshir, H.; Afzali Baghdadabadi, N.; Shahian Jahromi, S. Skeletal and Dentoalveolar Features in Patients with Deep Overbite Malocclusion. J. Dent. (Tehran) 2014, 11, 629–638. [Google Scholar]
- Cantore, S.; Ballini, A.; Farronato, D.; Malcangi, G.; Dipalma, G.; Assandri, F.; Garagiola, U.; Inchingolo, F.; De Vito, D.; Cirulli, N. Evaluation of an Oral Appliance in Patients with Mild to Moderate Obstructive Sleep Apnea Syndrome Intolerant to Continuous Positive Airway Pressure Use: Preliminary Results. Int. J. Immunopathol. Pharm. 2016, 29, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Coloccia, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Montenegro, V.; Patano, A.; Marinelli, G.; Laudadio, C.; Limongelli, L.; Di Venere, D.; et al. Effectiveness of Dental and Maxillary Transverse Changes in Tooth-Borne, Bone-Borne, and Hybrid Palatal Expansion through Cone-Beam Tomography: A Systematic Review of the Literature. Medicina 2021, 57, 288. [Google Scholar] [CrossRef]
- Elastodontic Therapy Un Nuovo Approccio Alla Terapia Ortodontica Funzionale. Available online: https://www.ildentistamoderno.com/elastodontic-therapy-un-nuovo-approccio-alla-terapia-ortodontica-funzionale/ (accessed on 12 January 2022).
- d’Apuzzo, F.; Minervini, G.; Grassia, V.; Rotolo, R.P.; Perillo, L.; Nucci, L. Mandibular Coronoid Process Hypertrophy: Diagnosis and 20-Year Follow-Up with CBCT, MRI and EMG Evaluations. Appl. Sci. 2021, 11, 4504. [Google Scholar] [CrossRef]
- d’Apuzzo, F.; Nucci, L.; Strangio, B.M.; Inchingolo, A.D.; Dipalma, G.; Minervini, G.; Perillo, L.; Grassia, V. Dento-Skeletal Class III Treatment with Mixed Anchored Palatal Expander: A Systematic Review. Appl. Sci. 2022, 12, 4646. [Google Scholar] [CrossRef]
- Di Venere, D.; CORSALINI, M.; NARDI, G.M.; LAFORGIA, A.; GRASSI, F.R.; RAPONE, B.; PETTINI, F. Obstructive Site Localization in Patients with Obstructive Sleep Apnea Syndrome: A Comparison between Otolaryngologic Data and Cephalometric Values. Oral Implant. (Rome) 2017, 10, 295–310. [Google Scholar] [CrossRef]
- de Praeter, J.; Dermaut, L.; Martens, G.D.M.; Kuijpers-Jagtman, A.M. Long-term stability of the leveling of the curve of Spee. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 266–272. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina (Kaunas) 2021, 57, 1350. [Google Scholar] [CrossRef]
- Sarver, D.M. The Importance of Incisor Positioning in the Esthetic Smile: The Smile Arc. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 98–111. [Google Scholar] [CrossRef] [Green Version]
- Di Venere, D.; Rapone, B.; Corsalini, M. Dental Trauma in the Anterior Sector: An Analysis of the Predisposing Factors in a Group of Orthodontic Patients. Clin. Therap. 2020, 171, e481–e485. [Google Scholar] [CrossRef]
- Rosvall, M.D.; Fields, H.W.; Ziuchkovski, J.; Rosenstiel, S.F.; Johnston, W.M. Attractiveness, Acceptability, and Value of Orthodontic Appliances. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 276.e1–276.e12; discussion 276–277. [Google Scholar] [CrossRef]
- Ziuchkovski, J.P.; Fields, H.W.; Johnston, W.M.; Lindsey, D.T. Assessment of Perceived Orthodontic Appliance Attractiveness. Am. J. Orthod. Dentofac. Orthop. 2008, 133, S68–S78. [Google Scholar] [CrossRef]
- Marinelli, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Limongelli, L.; Montenegro, V.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; et al. White Spot Lesions in Orthodontics: Prevention and Treatment. A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 227–240. [Google Scholar] [CrossRef]
- Patano, A.; Cirulli, N.; Beretta, M.; Plantamura, P.; Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Marinelli, G.; Scarano, A.; et al. Education Technology in Orthodontics and Paediatric Dentistry during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6056. [Google Scholar] [CrossRef]
- Adina, S.; Dipalma, G.; Bordea, I.R.; Lucaciu, O.; Feurdean, C.; Inchingolo, A.D.; Septimiu, R.; Malcangi, G.; Cantore, S.; Martin, D.; et al. Orthopedic Joint Stability Influences Growth and Maxillary Development: Clinical Aspects. J. Biol. Regul. Homeost. Agents 2020, 34, 747–756. [Google Scholar] [CrossRef]
- Di Venere, D. Correlation between Parodontal Indexes and Orthodontic Retainers: Prospective Study in a Group of 16 Patients. ORL 2017, 10, 78. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Pede, C.D.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef]
- Adobes-Martin, M.; Montoya-Morcillo, M.-L.; Zhou-Wu, A.; Garcovich, D. Invisalign Treatment from the Patient Perspective: A Twitter Content Analyses. J. Clin. Exp. Dent. 2021, 13, e376–e382. [Google Scholar] [CrossRef]
- Caruso, S.; Darvizeh, A.; Zema, S.; Gatto, R.; Nota, A. Management of a Facilitated Aesthetic Orthodontic Treatment with Clear Aligners and Minimally Invasive Corticotomy. Dent. J. 2020, 8, 19. [Google Scholar] [CrossRef] [Green Version]
- Nota, A.; Caruso, S.; Ehsani, S.; Ferrazzano, G.F.; Gatto, R.; Tecco, S. Short-Term Effect of Orthodontic Treatment with Clear Aligners on Pain and SEMG Activity of Masticatory Muscles. Medicina 2021, 57, 178. [Google Scholar] [CrossRef]
- El-Bialy, T. The Use of High Frequency Vibration and Clear Aligners in Management of an Adult Patient with Class III Skeletal Malocclusion with Open Bite and Severe Bimaxillary Protrusion: Case Report. Dent. J. 2020, 8, 75. [Google Scholar] [CrossRef]
- Timm, L.H.; Farrag, G.; Baxmann, M.; Schwendicke, F. Factors Influencing Patient Compliance during Clear Aligner Therapy: A Retrospective Cohort Study. J. Clin. Med. 2021, 10, 3103. [Google Scholar] [CrossRef]
- Tachiki, C.; Nishii, Y.; Yamamoto, M.; Takaki, T. Treatment Option Criteria for Open Bite with Receiver Operating Characteristic Analysis—A Retrospective Study. Appl. Sci. 2021, 11, 8736. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Ceci, S.; Patano, A.; Inchingolo, A.M.; Montenegro, V.; Di Pede, C.; Malcangi, G.; Marinelli, G.; Coloccia, G.; Garibaldi, M.; et al. Elastodontic Therapy of Hyperdivergent Class II Patients Using AMCOP® Devices: A Retrospective Study. Appl. Sci. 2022, 12, 3259. [Google Scholar] [CrossRef]
- De Felice, M.E.; Nucci, L.; Fiori, A.; Flores-Mir, C.; Perillo, L.; Grassia, V. Accuracy of Interproximal Enamel Reduction during Clear Aligner Treatment. Prog. Orthod. 2020, 21, 28. [Google Scholar] [CrossRef]
- Greco, M.; Rombolà, A. Precision Bite Ramps and Aligners: An Elective Choice for Deep Bite Treatment. J. Orthod. 2021, 14653125211034180. [Google Scholar] [CrossRef]
- Harris, K.; Ojima, K.; Dan, C.; Upadhyay, M.; Alshehri, A.; Kuo, C.-L.; Mu, J.; Uribe, F.; Nanda, R. Evaluation of Open Bite Closure Using Clear Aligners: A Retrospective Study. Prog. Orthod. 2020, 21, 23. [Google Scholar] [CrossRef]
- Krieger, E.; Seiferth, J.; Marinello, I.; Jung, B.A.; Wriedt, S.; Jacobs, C.; Wehrbein, H. Invisalign® Treatment in the Anterior Region. J. Orofac. Orthop./Fortschr. Kieferorthopädie 2012, 73, 365–376. [Google Scholar] [CrossRef]
- Henick, D.; Dayan, W.; Dunford, R.; Warunek, S.; Al-Jewair, T. Effects of Invisalign (G5) with Virtual Bite Ramps for Skeletal Deep Overbite Malocclusion Correction in Adults. Angle Orthod. 2021, 91, 164–170. [Google Scholar] [CrossRef]
- Galan-Lopez, L.; Barcia-Gonzalez, J.; Plasencia, E. A Systematic Review of the Accuracy and Efficiency of Dental Movements with Invisalign®. Korean J. Orthod. 2019, 49, 140–149. [Google Scholar] [CrossRef]
- Papadimitriou, A.; Mousoulea, S.; Gkantidis, N.; Kloukos, D. Clinical Effectiveness of Invisalign® Orthodontic Treatment: A Systematic Review. Prog. Orthod. 2018, 19, 37. [Google Scholar] [CrossRef] [Green Version]
- Malcangi, G.; Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Garibaldi, M.; Inchingolo, A.M.; Piras, F.; Cardarelli, F.; Settanni, V.; et al. Impacted Central Incisors in the Upper Jaw in an Adolescent Patient: Orthodontic-Surgical Treatment—A Case Report. Appl. Sci. 2022, 12, 2657. [Google Scholar] [CrossRef]
- Laudadio, C.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Montenegro, V.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Management of Anterior Open-Bite in the Deciduous, Mixed and Permanent Dentition Stage: A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 271–281. [Google Scholar] [CrossRef]
- Liu, Y.; Hu, W. Force Changes Associated with Different Intrusion Strategies for Deep-Bite Correction by Clear Aligners. Angle Orthod. 2018, 88, 771–778. [Google Scholar] [CrossRef] [Green Version]
- Montenegro, V.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Compliance of Children with Removable Functional Appliance with Microchip Integrated during Covid-19 Pandemic: A Systematic Review. J. Biol. Regul. Homeost. Agents 2021, 35, 365–377. [Google Scholar] [CrossRef]
- Khosravi, R.; Cohanim, B.; Hujoel, P.; Daher, S.; Neal, M.; Liu, W.; Huang, G. Management of Overbite with the Invisalign Appliance. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 691–699.e2. [Google Scholar] [CrossRef]
Figure 1.
Gingival smile and deep bite.
Figure 1.
Gingival smile and deep bite.
Figure 2.
Deep bite with good exposure of the upper incisors.
Figure 2.
Deep bite with good exposure of the upper incisors.
Figure 3.
Multibracket appliance during curve of Spee leveling: (A) at the beginning of the treatment; (B) at the end of the treatment.
Figure 3.
Multibracket appliance during curve of Spee leveling: (A) at the beginning of the treatment; (B) at the end of the treatment.
Figure 4.
Conventional horizontal rectangular attachments.
Figure 4.
Conventional horizontal rectangular attachments.
Figure 5.
Different designs of lower premolars attachments.
Figure 5.
Different designs of lower premolars attachments.
Figure 6.
Working setup in a deep bite: (A) deep curve of Spee; (B) reverse curve of Spee archwire; (C) overengineered setup.
Figure 6.
Working setup in a deep bite: (A) deep curve of Spee; (B) reverse curve of Spee archwire; (C) overengineered setup.
Figure 7.
Overcorrection of the digital setup.
Figure 7.
Overcorrection of the digital setup.
Figure 9.
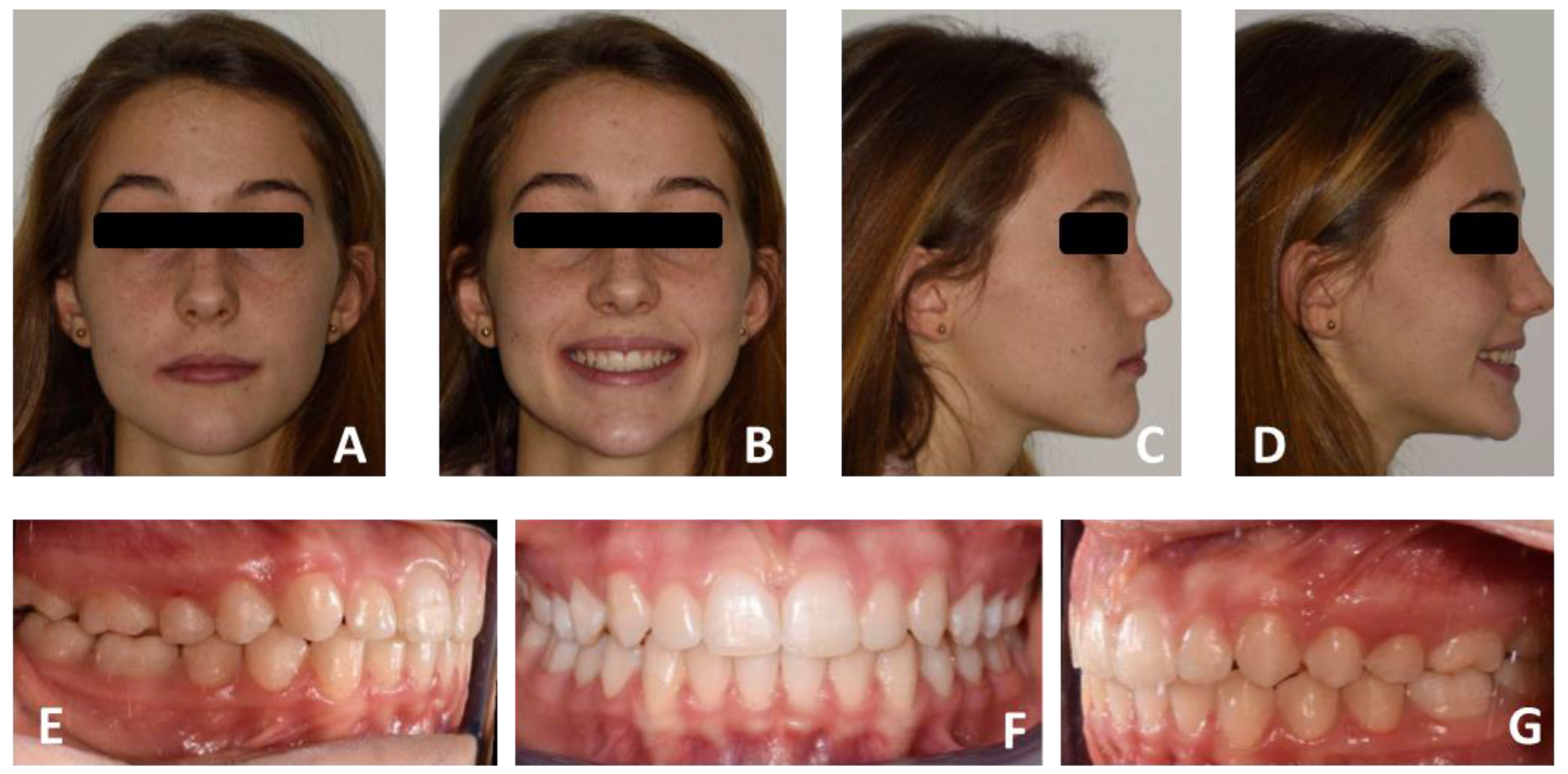
Pre-treatment intraoral and extraoral photos of case number 1: frontal facial view (A); frontal facial view smiling (B); right facial view (C); right facial view smiling (D); Right arches view (E); Frontal arches view (F); Left arches view (G); upper arch occlusal view (H); lower arch occlusal view (I).
Figure 9.
Pre-treatment intraoral and extraoral photos of case number 1: frontal facial view (A); frontal facial view smiling (B); right facial view (C); right facial view smiling (D); Right arches view (E); Frontal arches view (F); Left arches view (G); upper arch occlusal view (H); lower arch occlusal view (I).
Figure 10.
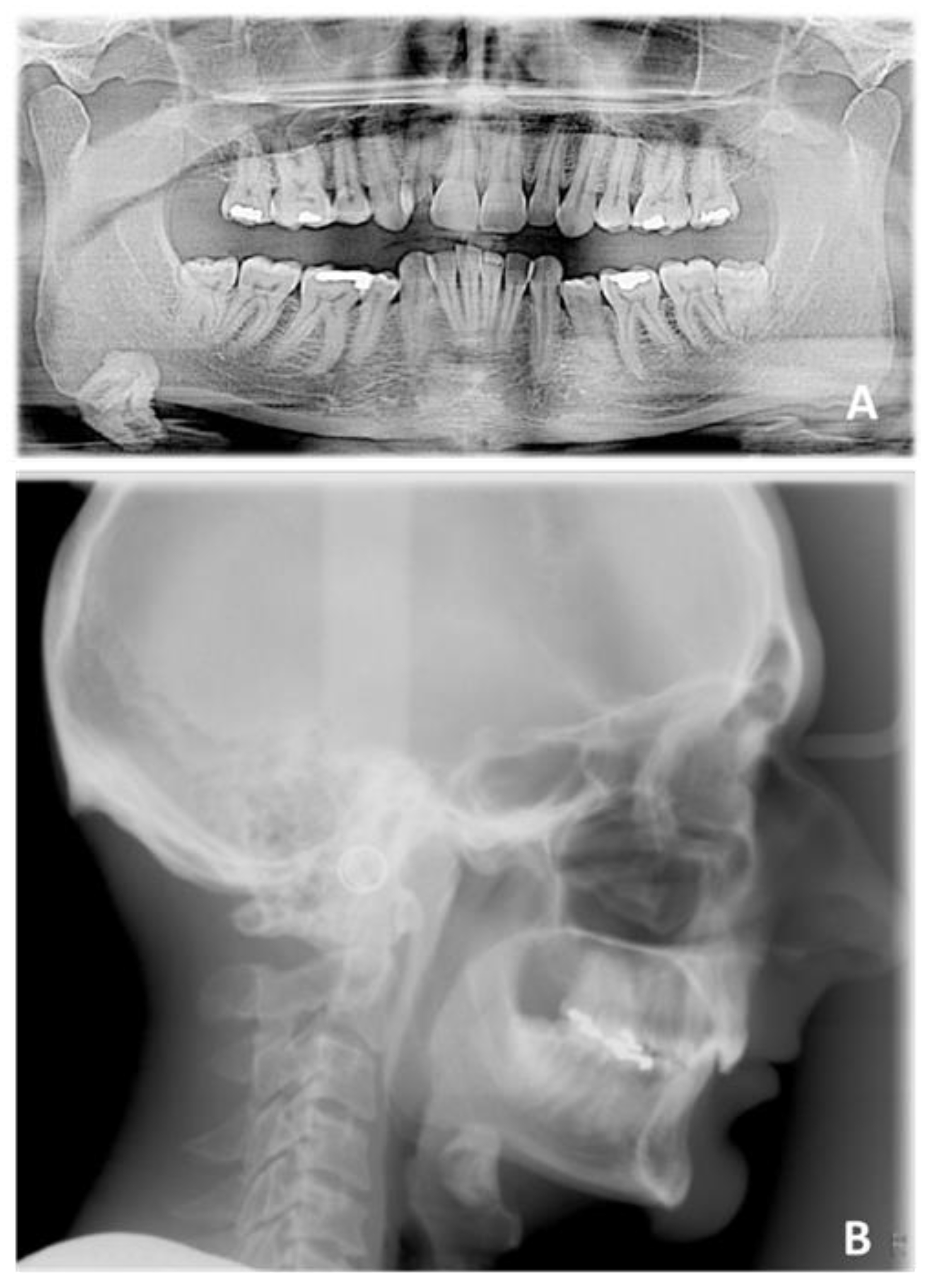
Pre-treatment radiographic of case number 1: (A) orthopantomography; (B) lateral cephalogram.
Figure 10.
Pre-treatment radiographic of case number 1: (A) orthopantomography; (B) lateral cephalogram.
Figure 11.
Pre-treatment cephalometric tracing.
Figure 11.
Pre-treatment cephalometric tracing.
Figure 12.
Post-treatment extraoral and intraoral photos of case number 1: frontal facial view (A); frontal facial view smiling (B); right facial view (C); right facial view smiling (D); right arches view (E); frontal arches view (F); left arches view (G); upper arch occlusal view (H); lower arch occlusal view (I).
Figure 12.
Post-treatment extraoral and intraoral photos of case number 1: frontal facial view (A); frontal facial view smiling (B); right facial view (C); right facial view smiling (D); right arches view (E); frontal arches view (F); left arches view (G); upper arch occlusal view (H); lower arch occlusal view (I).
Figure 13.
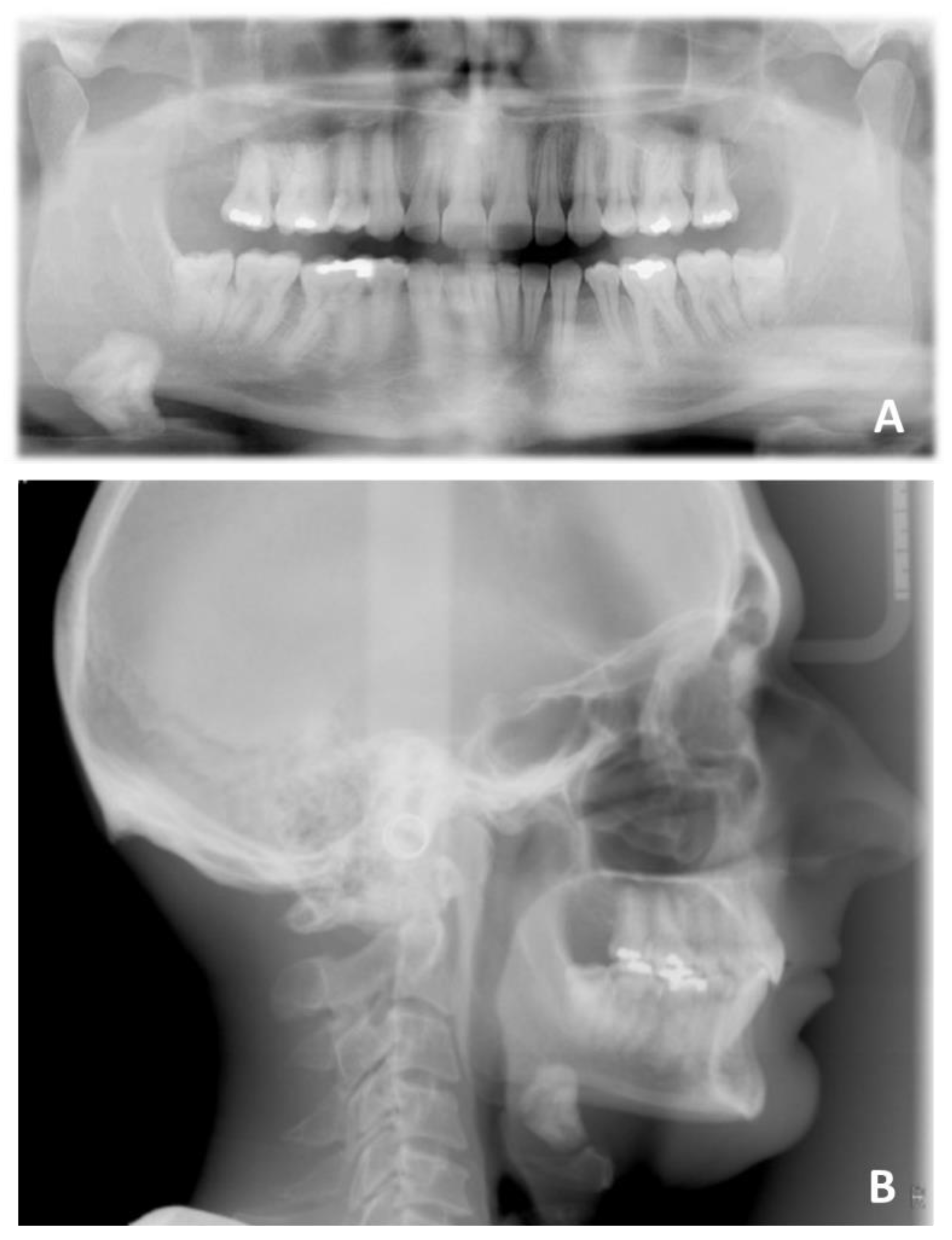
Post-treatment radiographic of case number 1: (A) orthopantomography; (B) lateral cephalogram.
Figure 13.
Post-treatment radiographic of case number 1: (A) orthopantomography; (B) lateral cephalogram.
Figure 14.
Post-treatment cephalometric tracing.
Figure 14.
Post-treatment cephalometric tracing.
Figure 15.
Pre-treatment intraoral and extraoral photos of case number 2: frontal facial view (A); frontal facial view smiling (B); right facial view (C); right facial view smiling (D); right arches view (E); frontal arches view (F); left arches view (G); upper arch occlusal view (H); lower arch occlusal view (I).
Figure 15.
Pre-treatment intraoral and extraoral photos of case number 2: frontal facial view (A); frontal facial view smiling (B); right facial view (C); right facial view smiling (D); right arches view (E); frontal arches view (F); left arches view (G); upper arch occlusal view (H); lower arch occlusal view (I).
Figure 16.
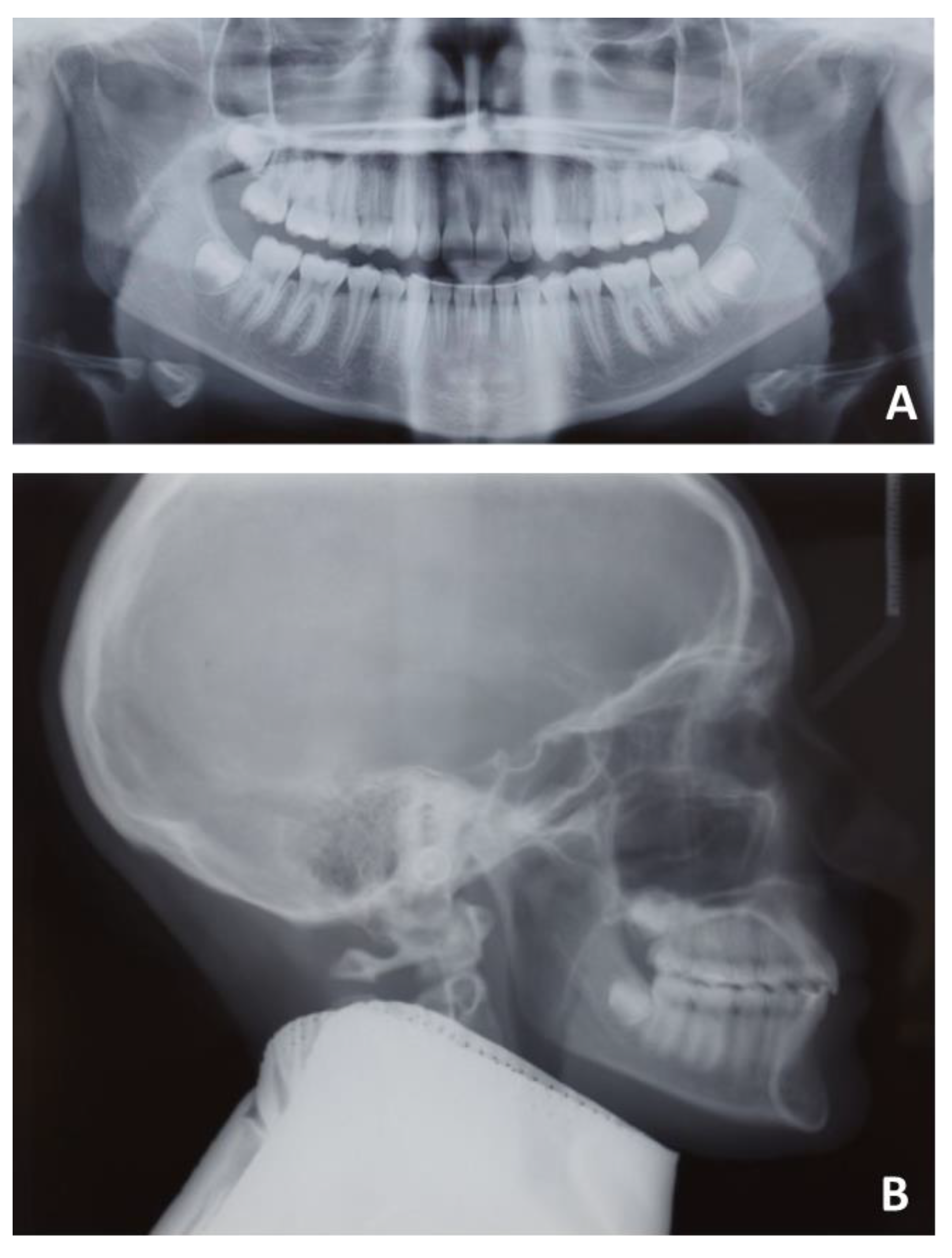
Pre-treatment radiographic of case number 2: (A) orthopantomography; (B) lateral cephalogram.
Figure 16.
Pre-treatment radiographic of case number 2: (A) orthopantomography; (B) lateral cephalogram.
Figure 17.
Pre-treatment cephalometric tracing of case number 2.
Figure 17.
Pre-treatment cephalometric tracing of case number 2.
Figure 18.
Post-treatment intraoral and extraoral photos of case number 2: frontal facial view (A); frontal facial view smiling (B); right facial view (C); right facial view smiling (D); right arches view (E); frontal arches view (F); left arches view (G); upper arch occlusal view (H); lower arch occlusal view (I).
Figure 18.
Post-treatment intraoral and extraoral photos of case number 2: frontal facial view (A); frontal facial view smiling (B); right facial view (C); right facial view smiling (D); right arches view (E); frontal arches view (F); left arches view (G); upper arch occlusal view (H); lower arch occlusal view (I).
Figure 19.
Post-treatment radiographic of case number 2: (A) orthopantomography; (B) lateral cephalogram.
Figure 19.
Post-treatment radiographic of case number 2: (A) orthopantomography; (B) lateral cephalogram.
Figure 20.
Post-treatment cephalometric tracing of case number 2.
Figure 20.
Post-treatment cephalometric tracing of case number 2.
Table 1.
Pre-treatment cephalometric values of case number 1.
Table 1.
Pre-treatment cephalometric values of case number 1.
| Measurements | Result | Mean | S.D. | Severity |
|---|
| SNA | 79.83 | 81.77 | 6.0 | |
| SNB | 74.62 | 80.42 | 5.3 | * |
| ANB | 5.21 | 2.05 | 1.8 | * |
| Bjork sum | 382.11 | 393.97 | 3.7 | *** |
| FMA | 11.29 | 25 | 4.0 | *** |
| Gonial angle | 102.95 | 122.38 | 4.9 | *** |
| APDI | 75.80 | 85.98 | 4.0 | ** |
| ODI | 90.55 | 73.35 | 5.9 | ** |
| Combination factor | 166.35 | 159.3 | 7.1 | |
| A to N-Perp (FH) | 0.70 | 1.1 | 2.7 | |
| B to N-Perp (FH) | −7.89 | −3.5 | 2.0 | ** |
| Pog to N-Perp (FH) | −6.01 | −0.3 | 2.5 | ** |
| FH to AB | 76.98 | 81 | 3.0 | * |
| A-B to mandibular plane | 91.73 | 69.3 | 2.5 | *** |
| Wits appraisal | 8.97 | −2.24 | 0.3 | *** |
| Overjet | 3.72 | 2 | 2.0 | |
| Overbite | 8.62 | 2 | 2.0 | *** |
| U1 to FH | 92.22 | 116.52 | 6.0 | *** |
| U1 to SN | 81.40 | 109.31 | 6.0 | *** |
| U1 to UOP | 76.49 | 55 | 4.0 | *** |
| IMPA | 96.76 | 95 | 5.5 | |
| L1 to LOP | 56.94 | 66 | 5.0 | * |
| Interincisal angle | 159.74 | 128 | 5.3 | *** |
| Cant of occlusal plane | −0.59 | 9.3 | 3.8 | ** |
| U1 to NA (mm) | 3.24 | 4 | 3.0 | |
| U1 to NA (deg) | 1.57 | 22 | 5.0 | *** |
| L1 to NB (mm) | 0.04 | 4 | 2.0 | * |
| L1 to NB (deg) | 13.49 | 25 | 5.0 | ** |
| Upper incisal display | 4.02 | 3 | 1.5 | |
| Upper lip to E-plane | −8.53 | 0 | 2.0 | *** |
| Lower lip to E-plane | −8.50 | 0 | 2.0 | *** |
| Nasolabial angle | 102.08 | 95 | 5.0 | * |
Table 2.
Post-treatment cephalometric values of case number 1.
Table 2.
Post-treatment cephalometric values of case number 1.
| Measurements | Result | Mean | S.D. | Severity |
|---|
| SNA | 79.13 | 81.77 | 6.0 | |
| SNB | 75.37 | 80.42 | 5.3 | |
| ANB | 3.76 | 2.05 | 1.8 | |
| Bjork sum | 382.04 | 393.97 | 3.7 | *** |
| FMA | 10.85 | 25 | 4.0 | *** |
| Gonial angle | 104.36 | 122.38 | 4.9 | *** |
| APDI | 79.77 | 85.98 | 4.0 | * |
| ODI | 88.72 | 73.35 | 5.9 | ** |
| Combination factor | 168.49 | 159.3 | 7.1 | * |
| A to N-Perp (FH) | 0.36 | 1.1 | 2.7 | |
| B to N-Perp (FH) | −6.03 | −3.5 | 2.0 | * |
| Pog to N-Perp (FH) | −2.98 | −0.3 | 2.5 | * |
| FH to AB | 80.10 | 81 | 3.0 | |
| A-B to mandibular plane | 89.05 | 69.3 | 2.5 | *** |
| Wits appraisal | 3.54 | −2.24 | 0.3 | *** |
| Overjet | 3.39 | 2 | 2.0 | |
| Overbite | 2.92 | 2 | 2.0 | |
| U1 to FH | 105.32 | 116.52 | 6.0 | * |
| U1 to SN | 94.12 | 109.31 | 6.0 | ** |
| U1 to UOP | 66.26 | 55 | 4.0 | ** |
| IMPA | 102.70 | 95 | 5.5 | * |
| L1 to LOP | 66.13 | 66 | 5.0 | |
| Interincisal angle | 141.13 | 128 | 5.3 | ** |
| Cant of occlusal plane | 4.44 | 9.3 | 3.8 | * |
| U1 to NA (mm) | 0.42 | 4 | 3.0 | * |
| U1 to NA (deg) | 14.99 | 22 | 5.0 | * |
| L1 to NB (mm) | 1.91 | 4 | 2.0 | * |
| L1 to NB (deg) | 20.12 | 25 | 5.0 | |
| Upper incisal display | 4.11 | 3 | 1.5 | |
| Upper lip to E-plane | −9.54 | 0 | 2.0 | *** |
| Lower lip to E-plane | −7.88 | 0 | 2.0 | *** |
| Nasolabial angle | 129.11 | 95 | 5.0 | *** |
Table 3.
Pre-treatment cephalometric values of case number 2.
Table 3.
Pre-treatment cephalometric values of case number 2.
| Measurements | Result | Mean | S.D. | Severity |
|---|
| SNA | 85.76 | 81.77 | 6.0 | |
| SNB | 79.54 | 80.42 | 5.3 | |
| ANB | 6.22 | 2.05 | 1.8 | ** |
| Bjork sum | 391.96 | 393.97 | 3.7 | |
| FMA | 22.50 | 25 | 4.0 | |
| Gonial angle | 122.28 | 122.38 | 4.9 | |
| APDI | 77.07 | 85.98 | 4.0 | ** |
| ODI | 75.83 | 73.35 | 5.9 | |
| Combination factor | 152.90 | 159.3 | 7.1 | |
| A to N-Perp (FH) | 5.03 | 1.1 | 2.7 | * |
| B to N-Perp (FH) | −1.58 | −3.5 | 2.0 | |
| Pog to N-Perp (FH) | 0.36 | −0.3 | 2.5 | |
| FH to AB | 79.38 | 81 | 3.0 | |
| A-B to mandibular plane | 78.13 | 69.3 | 2.5 | *** |
| Wits appraisal | 3.80 | −2.24 | 0.3 | *** |
| Overjet | 6.03 | 2 | 2.0 | ** |
| Overbite | 5.30 | 2 | 2.0 | * |
| U1 to FH | 113.00 | 116.52 | 6.0 | |
| U1 to SN | 103.54 | 109.31 | 6.0 | |
| U1 to UOP | 57.39 | 55 | 4.0 | |
| IMPA | 101.75 | 95 | 5.5 | * |
| L1 to LOP | 53.91 | 66 | 5.0 | ** |
| Interincisal angle | 122.75 | 128 | 5.3 | |
| Cant of occlusal plane | 4.53 | 9.3 | 3.8 | * |
| U1 to NA (mm) | 2.45 | 4 | 3.0 | |
| U1 to NA (deg) | 17.78 | 22 | 5.0 | |
| L1 to NB (mm) | 5.32 | 4 | 2.0 | |
| L1 to NB (deg) | 33.25 | 25 | 5.0 | * |
| Upper incisal display | 4.64 | 3 | 1.5 | * |
| Upper lip to E-plane | −2.73 | 0 | 2.0 | * |
| Lower lip to E-plane | −1.56 | 0 | 2.0 | |
| Nasolabial angle | 92.06 | 95 | 5.0 | |
Table 4.
Post-treatment cephalometric values of case number 2.
Table 4.
Post-treatment cephalometric values of case number 2.
| Measurements | Result | Mean | S.D. | Severity |
|---|
| SNA | 82.68 | 81.77 | 6.0 | |
| SNB | 79.04 | 80.42 | 5.3 | |
| ANB | 3.64 | 2.05 | 1.8 | |
| Bjork sum | 393.11 | 393.97 | 3.7 | |
| FMA | 22.58 | 25 | 4.0 | |
| Gonial angle | 129.98 | 122.38 | 4.9 | * |
| APDI | 81.92 | 85.98 | 4.0 | * |
| ODI | 71.74 | 73.35 | 5.9 | |
| Combination factor | 153.66 | 159.3 | 7.1 | |
| A to N-Perp (FH) | 3.26 | 1.1 | 2.7 | |
| B to N-Perp (FH) | −0.71 | −3.5 | 2.0 | * |
| Pog to N-Perp (FH) | 2.95 | −0.3 | 2.5 | * |
| FH to AB | 83.80 | 81 | 3.0 | |
| A-B to mandibular plane | 73.62 | 69.3 | 2.5 | * |
| Wits appraisal | 1.39 | −2.24 | 0.3 | *** |
| Overjet | 3.11 | 2 | 2.0 | |
| Overbite | 1.81 | 2 | 2.0 | |
| U1 to FH | 110.99 | 116.52 | 6.0 | |
| U1 to SN | 100.46 | 109.31 | 6.0 | * |
| U1 to UOP | 62.99 | 55 | 4.0 | * |
| IMPA | 94.70 | 95 | 5.5 | |
| L1 to LOP | 64.50 | 66 | 5.0 | |
| Interincisal angle | 131.73 | 128 | 5.3 | |
| Cant of occlusal plane | 4.04 | 9.3 | 3.8 | * |
| U1 to NA (mm) | 2.32 | 4 | 3.0 | |
| U1 to NA (deg) | 17.78 | 22 | 5.0 | |
| L1 to NB (mm) | 4.32 | 4 | 2.0 | |
| L1 to NB (deg) | 26.85 | 25 | 5.0 | |
| Upper incisal display | 2.77 | 3 | 1.5 | |
| Upper lip to E-plane | −8.01 | 0 | 2.0 | *** |
| Lower lip to E-plane | −5.83 | 0 | 2.0 | ** |
| Nasolabial angle | 109.41 | 95 | 5.0 | ** |
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 



























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}