
Evaluation of Lip Morphology and Nasolabial Angle in Non-Syndromic Cleft Lip and/Palate and Non-Cleft Individuals

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
- Subjects had undergone their cleft lip and palate surgery during their childhood.
- No orthodontic treatment has been done for any participants.
- All clinical records and radiographs (Late. Ceph. and OPG) were taken by a Saudi board-certified dental resident.
- Late. Ceph. must show all of the landmarks planned to be used in the study.
- Lips should close smoothly.
- Bite should be registered in centric occlusion.
- Late. Ceph. that had any artefacts in the area of interest.
- Radiographs that were of poor quality due to exposure parameters.
- Radiographs that were blurred due to movement of patients.
2.2. Measurements
2.3. Statistical Analyses
3. Results
3.1. LM/Esthetic Plane Analysis
3.2. Nasolabial Angle Analysis (NLA)
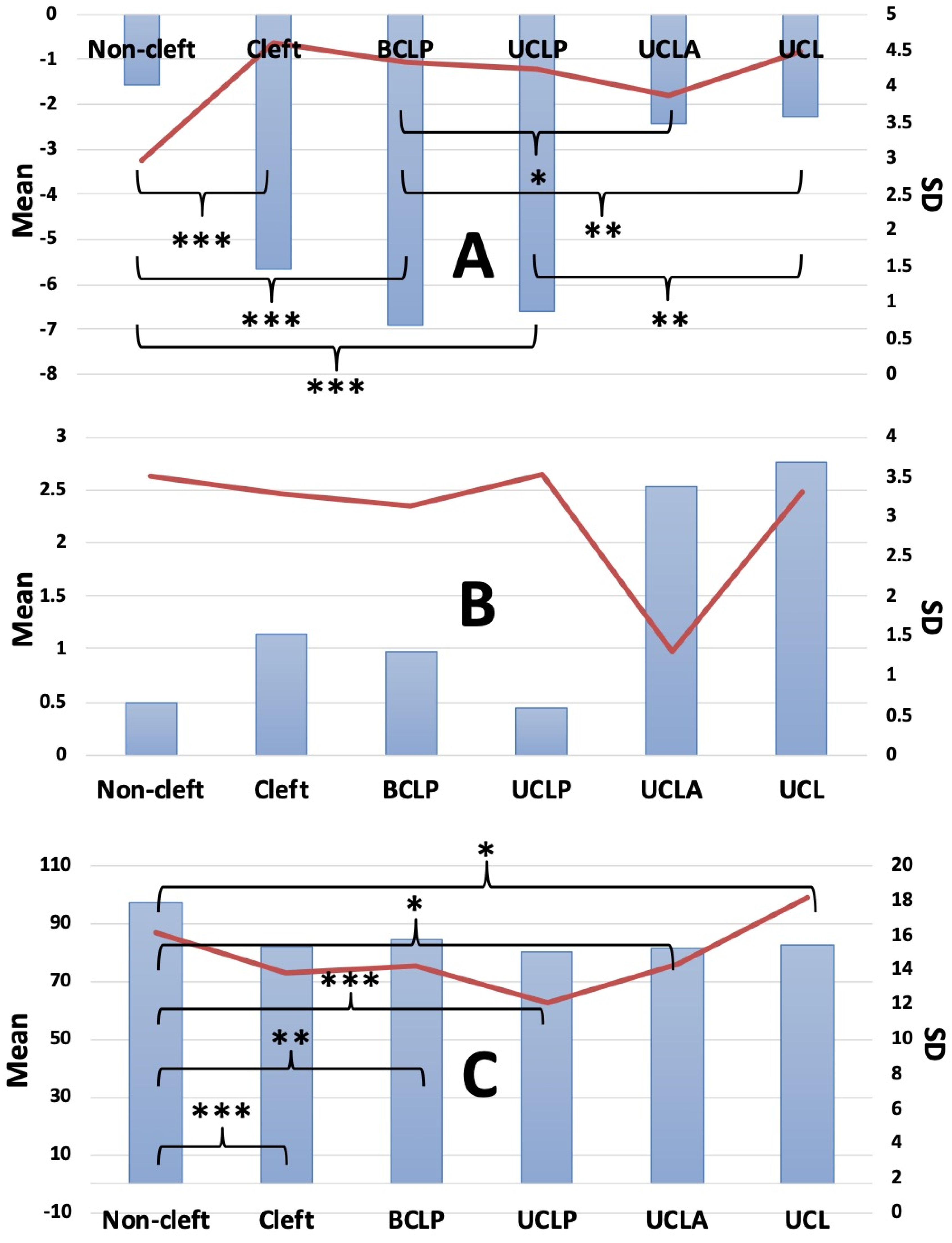
- The NLA angle formed from the columella, subnasale, and labiale superius of the subjects were 97.199 (NC), 84.492 (BCLP), 79.893 (UCLP), 81.166 (UCLA), and 82.515 (UCL), respectively (Figure 2).
- Compared to NC and all 4 cleft groups, NLA showed significant disparities. Among NSCLP no significant disparities were found.
- No significant gender disparities among all groups were found (Table 3).
- No significant side disparities were found (Table 4).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mohammad-Rahimi, H.; Nadimi, M.; Rohban, M.H.; Shamsoddin, E.; Lee, V.Y.; Motamedian, S.R. Machine Learning and Orthodontics, Current Trends and the Future Opportunities: A Scoping Review. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 170–192.e4. [Google Scholar] [CrossRef]
- Chaudhari, P.K.; Alam, M.K. Current Applications of Artificial Intelligence in Cleft Care: A Scoping Review. Front. Med. 2021, 8, 14. [Google Scholar]
- Oh, K.; Oh, I.-S.; Le, V.N.T.; Lee, D.-W. Deep Anatomical Context Feature Learning for Cephalometric Landmark Detection. IEEE J. Biomed. Health Inform. 2021, 25, 806–817. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Qiao, X.; Iwamoto, Y.; Chen, Y. Automatic Cephalometric Landmark Detection on X-Ray Images Using a Deep-Learning Method. Appl. Sci. 2020, 10, 2547. [Google Scholar] [CrossRef] [Green Version]
- Amasya, H.; Yildirim, D.; Aydogan, T.; Kemaloglu, N.; Orhan, K. Cervical Vertebral Maturation Assessment on Lateral Cephalometric Radiographs Using Artificial Intelligence: Comparison of Machine Learning Classifier Models. Dentomaxillofac. Radiol. 2020, 49, 20190441. [Google Scholar] [CrossRef]
- Yu, H.J.; Cho, S.R.; Kim, M.J.; Kim, W.H.; Kim, J.W.; Choi, J. Automated Skeletal Classification with Lateral Cephalometry Based on Artificial Intelligence. J. Dent. Res. 2020, 99, 249–256. [Google Scholar] [CrossRef]
- Kunz, F.; Stellzig-Eisenhauer, A.; Zeman, F.; Boldt, J. Artificial Intelligence in Orthodontics: Evaluation of a Fully Automated Cephalometric Analysis Using a Customized Convolutional Neural Network. J. Orofac. Orthop. 2020, 81, 52–68. [Google Scholar] [CrossRef]
- Lee, K.-S.; Ryu, J.-J.; Jang, H.S.; Lee, D.-Y.; Jung, S.-K. Deep Convolutional Neural Networks Based Analysis of Cephalometric Radiographs for Differential Diagnosis of Orthognathic Surgery Indications. Appl. Sci. 2020, 10, 2124. [Google Scholar] [CrossRef] [Green Version]
- Vial, A.; Stirling, D.; Field, M.; Ros, M.; Ritz, C.; Carolan, M.; Holloway, L.; Miller, A.A. The Role of Deep Learning and Radiomic Feature Extraction in Cancer-Specific Predictive Modelling: A Review. Transl. Cancer Res. 2018, 7, 803–816. [Google Scholar] [CrossRef]
- Ding, Y.; Sohn, J.H.; Kawczynski, M.G.; Trivedi, H.; Harnish, R.; Jenkins, N.W.; Lituiev, D.; Copeland, T.P.; Aboian, M.S.; Mari Aparici, C. A Deep Learning Model to Predict a Diagnosis of Alzheimer Disease by Using 18F-FDG PET of the Brain. Radiology 2019, 290, 456–464. [Google Scholar] [CrossRef]
- Kim, H.; Shim, E.; Park, J.; Kim, Y.-J.; Lee, U.; Kim, Y. Web-Based Fully Automated Cephalometric Analysis by Deep Learning. Comput. Methods Programs Biomed. 2020, 194, 105513. [Google Scholar] [CrossRef]
- Arık, S.Ö.; Ibragimov, B.; Xing, L. Fully Automated Quantitative Cephalometry Using Convolutional Neural Networks. J. Med. Imaging 2017, 4, 014501. [Google Scholar] [CrossRef]
- Tolarova, M.M. Global Health Issues Related to Cleft Lip and Palate: Prevention and Treatment Need to Team Together. Indian J. Dent. Res. 2016, 27, 455. [Google Scholar] [CrossRef]
- Mossey, P.A.; Little, J.; Munger, R.G.; Dixon, M.J.; Shaw, W.C. Cleft Lip and Palate. Lancet 2009, 374, 1773–1785. [Google Scholar] [CrossRef]
- Alam, M.K.; Iida, J.; Sato, Y.; Kajii, T.S. Postnatal Treatment Factors Affecting Craniofacial Morphology of Unilateral Cleft Lip and Palate (UCLP) Patients in a Japanese Population. Br. J. Oral. Maxillofac. Surg. 2013, 51, e205–e210. [Google Scholar] [CrossRef] [PubMed]
- Haque, S.; Alam, M.K. Common Dental Anomalies in Cleft Lip and Palate Patients. Malays. J. Med. Sci. 2015, 22, 55–60. [Google Scholar]
- De Lauris, R.C.M.C.; Capelozza, L.; Calil, L.R.; Lauris, J.R.P.; Janson, G.; Garib, D.G. Facial Profile Esthetics in Operated Children with Bilateral Cleft Lip and Palate. Dent. Press J. Orthod. 2017, 22, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Tole, N.; Lajnert, V.; Kovacevic Pavicic, D.; Spalj, S. Gender, Age, and Psychosocial Context of the Perception of Facial Esthetics. J. Esthet. Restor. Dent. 2014, 26, 119–130. [Google Scholar] [CrossRef]
- Phillips, G.S.A.; Swan, M.C.; Sawyer, A.R.; Goodacre, T.E.E.; Cadier, M. A Comparative Study of the Aesthetic Outcome of Two Techniques for Unilateral Complete Cleft Lip Repair. Plast. Reconstr. Surg. 2017, 140, 757–764. [Google Scholar] [CrossRef]
- Nahai, F.R.; Williams, J.K.; Burstein, F.D.; Martin, J.; Thomas, J. The Management of Cleft Lip and Palate: Pathways for Treatment and Longitudinal Assessment. Semin. Plast. Surg. 2005, 19, 275–285. [Google Scholar] [CrossRef] [Green Version]
- Alam, M.K.; Alfawzan, A.A. Evaluation of Sella Turcica Bridging and Morphology in Different Types of Cleft Patients. Front. Cell Dev. Biol. 2020, 8, 656. [Google Scholar] [CrossRef]
- Alam, M.K.; Alfawzan, A.A. Dental Characteristics of Different Types of Cleft and Non-Cleft Individuals. Front. Cell Dev. Biol. 2020, 8, 789. [Google Scholar] [CrossRef]
- Alam, M.K.; Alfawzan, A.A.; Haque, S.; Mok, P.L.; Marya, A.; Venugopal, A.; Jamayet, N.B.; Siddiqui, A.A. Sagittal Jaw Relationship of Different Types of Cleft and Non-Cleft Individuals. Front. Pediatr. 2021, 9, 651951. [Google Scholar] [CrossRef]
- Ricketts, R.M. Esthetics, Environment, and the Law of Lip Relation. Am. J. Orthod 1968, 54, 272–289. [Google Scholar] [CrossRef]
- Armijo, B.S.; Brown, M.; Guyuron, B. Defining the ideal nasolabial angle. Plast. Reconstr. Surg. 2012, 129, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Smahel, Z.; Polivková, H.; Skvarilová, B.; Horák, I. Configuration of Facial Profile in Adults with Cleft Lip with or without Cleft Palate. Acta Chir. Plast. 1992, 34, 190–203. [Google Scholar] [PubMed]
- Celikoglu, M.; Buyuk, S.K.; Sekerci, A.E.; Ersoz, M.; Celik, S.; Sisman, Y. Facial Soft-Tissue Thickness in Patients Affected by Bilateral Cleft Lip and Palate: A Retrospective Cone-Beam Computed Tomography Study. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 573–578. [Google Scholar] [CrossRef] [PubMed]
- Kocadereli, I. Changes in Soft Tissue Profile after Orthodontic Treatment with and without Extractions. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 67–72. [Google Scholar] [CrossRef]
- Satravaha, S.; Schlegel, K.D. The Significance of the Integumentary Profile. Am. J. Orthod. Dentofac. Orthop. 1987, 92, 422–426. [Google Scholar] [CrossRef]
- Alcalde, R.E.; Jinno, T.; Orsini, M.G.; Sasaki, A.; Sugiyama, R.M.; Matsumura, T. Soft Tissue Cephalometric Norms in Japanese Adults. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 84–89. [Google Scholar] [CrossRef]
- Paradowska-Stolarz, A.M.; Kawala, B. The Nasolabial Angle Among Patients with Total Cleft Lip and Palate. Adv. Clin. Exp. Med. 2015, 24, 481–485. [Google Scholar] [CrossRef] [Green Version]
- Rhee, S.C.; Kang, S.R.; Park, H.S. Balanced Angular Profile Analysis. Plast. Reconstr. Surg. 2004, 114, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Almoammar, K.A.; Almarhoon, H.A.; Batwa, W.; Alqahtani, N.; Al-Jewair, T.; Albarakati, S. Cephalometric Soft Tissue Characteristics of Unilateral Cleft Lip and Palate Patients in Relation to Missing Teeth. BioMed Res. Int. 2017, 2017, 2392808. [Google Scholar] [CrossRef] [Green Version]
- Oh, H.S.; Korn, E.L.; Zhang, X.; Liu, Y.; Xu, T.; Boyd, R.; Baumrind, S. Correlations between Cephalometric and Photographic Measurements of Facial Attractiveness in Chinese and US Patients after Orthodontic Treatment. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 762–763. [Google Scholar] [CrossRef]
- Russell, K.A.; Orthod, D.; Tompson, B.; Orthod, D.; Paedo, D. Correlation between Facial Morphology and Esthetics in Patients with Repaired Complete Unilateral Cleft Lip and Palate. Cleft Palate Craniofac. J. 2009, 46, 319–325. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
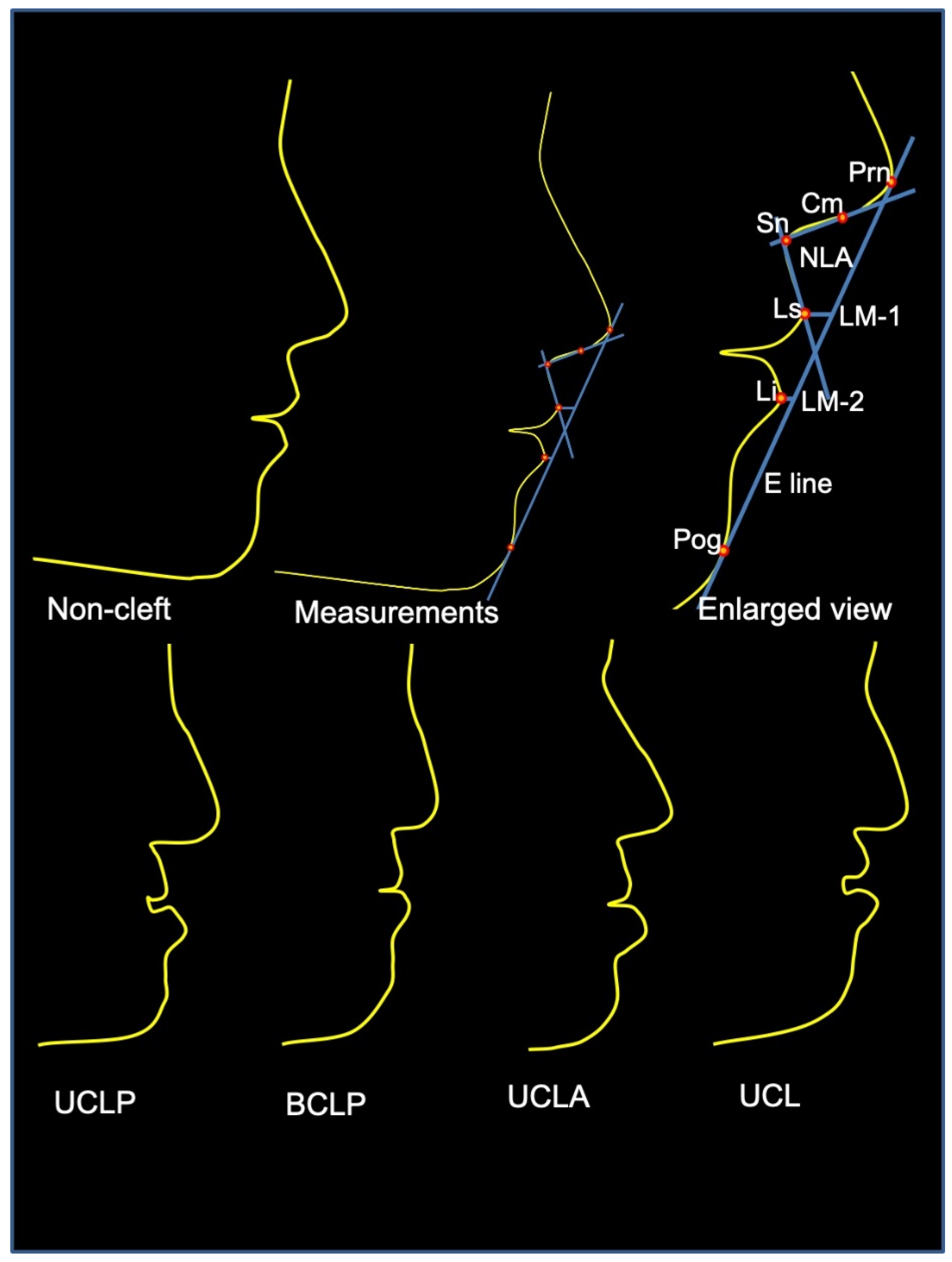
| Prn (pronasale) | the most prominent point of the nose. |
| Cm (Highest point of columella) | the most anterior and highest part of the columella. |
| Sn (subnasale) | the point at which the columella merges with the upper lip in the midsagittal plane. |
| Ls (labiale superius) | the most anterior point on the upper lip. |
| Li (labiale inferius) | the most anterior point on the lower lip. |
| Pog (soft tissue pogonion) | the most anterior point on the soft tissue chin. |
| Nasolabial angle (NLA) | the acute angle formed by profile points highest point of columella, subnasale, and labiale superius. |
| Upper lip to E plane (LM-1) | distance between the Ls and a line from the Prn to the pog. |
| Lower lip to E plane (LM-2) | distance between the Li and a line from the Prn to the pog. |
| SN | Non-Cleft | BCLP | UCLP | UCLA | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LM-1 | LM-2 | NLA | LM-1 | LM-2 | NLA | LM-1 | LM-2 | NLA | LM-1 | LM-2 | NLA | |
| 1 | 0.52 | 2.09 | 90.21 | −2.74 | −0.12 | 87.77 | −5.83 | 0.61 | 69.68 | 1.17 | 3.64 | 82.28 |
| 2 | −3.04 | −1.57 | 95.12 | −6.71 | 3.20 | 43.10 | −11.49 | −0.09 | 95.43 | −5.70 | 0.97 | 86.80 |
| 3 | −8.21 | −4.75 | 116.33 | −1.74 | 4.34 | 102.57 | −4.57 | −1.36 | 89.20 | 0.19 | 3.83 | 85.17 |
| 4 | 3.00 | 3.53 | 89.54 | −5.83 | −0.54 | 84.63 | −1.87 | 5.22 | 58.79 | −6.74 | 0.87 | 66.45 |
| 5 | −3.80 | −1.60 | 74.36 | −4.90 | 1.55 | 97.38 | −3.45 | 2.49 | 79.37 | 0.21 | 2.93 | 86.38 |
| 6 | −1.96 | 1.56 | 83.91 | −4.88 | 0.80 | 94.13 | −2.11 | 3.55 | 81.77 | 2.86 | 3.11 | 102.06 |
| 7 | 1.54 | 5.54 | 91.30 | −4.49 | 1.01 | 89.37 | −0.60 | 4.58 | 90.35 | −2.03 | 3.05 | 90.88 |
| 8 | 1.35 | 5.62 | 83.00 | −6.71 | 1.59 | 102.79 | −2.89 | 3.30 | 89.00 | −8.31 | 0.70 | 53.00 |
| 9 | 2.30 | 5.79 | 89.04 | −6.97 | 3.14 | 108.71 | −3.20 | 2.65 | 70.24 | −3.44 | 3.62 | 77.47 |
| 10 | −2.42 | −3.01 | 77.24 | −6.00 | −1.43 | 75.69 | −3.42 | 1.49 | 79.04 | |||
| 11 | 0.13 | 1.10 | 93.49 | −13.68 | 4.97 | 70.79 | −2.92 | 5.11 | 79.36 | UCL | ||
| 12 | −3.67 | −0.75 | 100.03 | −6.39 | 1.53 | 83.85 | −5.92 | −0.91 | 86.72 | |||
| 13 | −2.87 | −2.23 | 90.58 | −11.87 | 2.91 | 85.81 | −8.57 | −4.04 | 81.10 | −6.34 | 1.93 | 80.57 |
| 14 | −0.63 | −0.04 | 94.99 | −8.53 | −1.61 | 80.94 | −2.99 | 4.86 | 80.61 | −2.47 | 0.73 | 83.13 |
| 15 | 3.48 | 5.11 | 90.69 | 0.42 | 8.04 | 87.55 | −11.28 | −0.58 | 75.13 | −3.15 | 0.43 | 91.10 |
| 16 | 1.76 | 5.46 | 78.34 | −5.41 | −0.33 | 80.91 | −2.91 | 1.40 | 56.34 | 1.75 | 2.41 | 85.56 |
| 17 | −4.81 | −3.68 | 87.10 | −14.88 | −6.49 | 66.24 | −6.07 | 2.78 | 82.52 | 4.93 | 9.12 | 94.25 |
| 18 | 2.74 | 6.42 | 103.18 | −4.47 | −1.55 | 73.86 | −4.61 | 2.30 | 51.65 | −0.97 | 3.99 | 68.11 |
| 19 | −5.15 | −0.53 | 80.02 | −4.85 | 1.30 | 95.22 | −8.25 | 1.10 | 86.54 | −3.07 | 5.40 | 72.82 |
| 20 | −3.34 | −0.47 | 117.40 | −3.87 | 4.84 | 61.53 | −7.29 | −0.42 | 78.20 | 0.39 | 3.40 | 82.28 |
| 21 | −5.19 | −1.79 | 89.61 | −4.64 | 2.29 | 89.29 | −7.63 | −0.70 | 88.34 | −6.21 | −0.52 | 123.10 |
| 22 | −4.14 | −5.32 | 138.23 | −1.43 | −0.70 | 96.05 | −12.36 | −4.65 | 88.54 | −4.52 | −0.85 | 86.24 |
| 23 | −2.23 | −1.34 | 99.96 | −14.01 | 3.36 | 87.27 | −10.89 | −1.44 | 109.05 | −1.33 | 4.00 | 67.87 |
| 24 | −3.77 | −2.00 | 106.37 | −11.01 | −0.72 | 71.34 | −11.11 | −3.01 | 61.64 | −11.85 | −1.90 | 44.72 |
| 25 | −2.55 | −1.05 | 126.48 | −10.18 | −1.01 | 95.55 | −15.03 | −3.20 | 87.27 | 3.48 | 7.69 | 92.95 |
| 26 | −4.99 | 0.53 | 133.19 | −4.52 | 3.80 | 76.53 | −9.79 | −1.83 | 77.84 | |||
| 27 | −1.78 | −3.71 | 116.57 | −2.65 | 1.80 | 71.15 | −12.63 | −6.13 | 84.47 | |||
| 28 | 2.91 | 6.16 | 93.82 | −11.26 | −0.58 | 90.24 | −4.19 | 2.00 | 78.32 | |||
| 29 | −3.10 | −3.07 | 101.43 | −16.82 | −6.89 | 100.01 | −3.47 | 1.44 | 89.50 | |||
| 30 | −0.75 | 0.52 | 83.12 | −3.05 | 3.53 | 72.21 | ||||||
| 31 | 0.31 | 2.61 | 98.54 | 0.58 | 3.64 | 66.85 | ||||||
| 32 | −5.62 | 3.40 | 91.36 | |||||||||
| 33 | −6.98 | 0.89 | 77.51 | |||||||||
| 34 | −6.27 | 1.04 | 69.71 | |||||||||
| 35 | −16.18 | −11.76 | 103.45 | |||||||||
| 36 | −5.10 | 2.74 | 78.32 | |||||||||
| 37 | −16.86 | −6.93 | 99.97 | |||||||||
| 38 | −4.45 | 0.48 | 70.93 | |||||||||
| 39 | −9.37 | 2.30 | 76.10 | |||||||||
| 40 | −6.62 | 0.69 | 75.34 | |||||||||
| 41 | −3.01 | 1.84 | 67.85 | |||||||||
| Grouping | Variables | Gender | Mean | SD | 95% CI | p-Value | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Non-cleft | LM-1 | M | −1.355 | 2.366 | −1.859 | 2.606 | 0.734 |
| F | −1.729 | 3.469 | |||||
| LM-2 | M | 0.648 | 3.434 | −2.340 | 2.923 | 0.822 | |
| F | 0.357 | 3.668 | |||||
| NLA | M | 100.752 | 20.096 | −5.357 | 18.313 | 0.272 | |
| F | 94.274 | 11.739 | |||||
| BCLP | LM-1 | M | −6.533 | 4.513 | −2.277 | 5.165 | 0.433 |
| F | −7.978 | 3.913 | |||||
| LM-2 | M | 0.780 | 3.540 | −3.447 | 1.977 | 0.583 | |
| F | 1.515 | 1.799 | |||||
| NLA | M | 87.195 | 12.135 | −1.876 | 21.474 | 0.096 | |
| F | 77.396 | 17.400 | |||||
| UCLP | LM-1 | M | −6.785 | 4.749 | −3.113 | 2.321 | 0.770 |
| F | −6.389 | 3.768 | |||||
| LM-2 | M | 0.190 | 4.005 | −2.780 | 1.721 | 0.637 | |
| F | 0.720 | 3.026 | |||||
| NLA | M | 81.572 | 9.908 | −4.211 | 11.095 | 0.369 | |
| F | 78.130 | 14.060 | |||||
| UCLA | LM-1 | M | −1.943 | 3.916 | −5.364 | 8.231 | 0.633 |
| F | −3.377 | 4.417 | |||||
| LM-2 | M | 2.673 | 1.379 | −1.833 | 2.727 | 0.657 | |
| F | 2.227 | 1.323 | |||||
| NLA | M | 83.372 | 11.718 | −18.207 | 31.443 | 0.548 | |
| F | 76.753 | 20.694 | |||||
| UCL | LM-1 | M | −1.917 | 5.005 | −4.972 | 6.451 | 0.781 |
| F | −2.657 | 4.219 | |||||
| LM-2 | M | 3.060 | 3.158 | −3.546 | 4.862 | 0.737 | |
| F | 2.402 | 3.737 | |||||
| NLA | M | 76.791 | 16.796 | −34.064 | 9.260 | 0.234 | |
| F | 89.193 | 18.707 | |||||
| Variables | Side | Mean | SD | 95% CI | p-Value | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| LM-1 | Right | −5.208 | 4.706 | −2.575 | 2.203 | 0.877 |
| Left | −5.022 | 4.683 | ||||
| LM-2 | Right | 0.480 | 3.734 | −3.005 | 0.410 | 0.134 |
| Left | 1.777 | 3.043 | ||||
| NLA | Right | 82.949 | 13.428 | −2.823 | 10.988 | 0.242 |
| Left | 78.866 | 13.665 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alam, M.K.; Alfawzan, A.A.; Akhter, F.; Alswairki, H.J.; Chaudhari, P.K. Evaluation of Lip Morphology and Nasolabial Angle in Non-Syndromic Cleft Lip and/Palate and Non-Cleft Individuals. Appl. Sci. 2022, 12, 357. https://doi.org/10.3390/app12010357
Alam MK, Alfawzan AA, Akhter F, Alswairki HJ, Chaudhari PK. Evaluation of Lip Morphology and Nasolabial Angle in Non-Syndromic Cleft Lip and/Palate and Non-Cleft Individuals. Applied Sciences. 2022; 12(1):357. https://doi.org/10.3390/app12010357
Chicago/Turabian StyleAlam, Mohammad Khursheed, Ahmed Ali Alfawzan, Fatema Akhter, Haytham Jamil Alswairki, and Prabhat Kumar Chaudhari. 2022. "Evaluation of Lip Morphology and Nasolabial Angle in Non-Syndromic Cleft Lip and/Palate and Non-Cleft Individuals" Applied Sciences 12, no. 1: 357. https://doi.org/10.3390/app12010357