
Biofeedback Applied to Interactive Serious Games to Monitor Frailty in an Elderly Population


 , and
, and
Abstract
:1. Introduction
2. Literature Review
3. Materials and Methods
3.1. Materials
3.1.1. Hardware Used
3.1.2. Inclusion and Exclusion Criteria
- The user must have a personal computer or laptop and a webcam
- The user must be between the ages of 12 and 85
- The user must be in a spacious room during the game to avoid hitting their surroundings
- The playing room should be well lit with natural or voluminous artificial light
- It is desirable that there be at least one other person next to the user while they are playing
- People with vestibular problems and those who are sensitive to light should only use the system in the presence of others
- People who currently have minor musculoskeletal problems or have had them before.
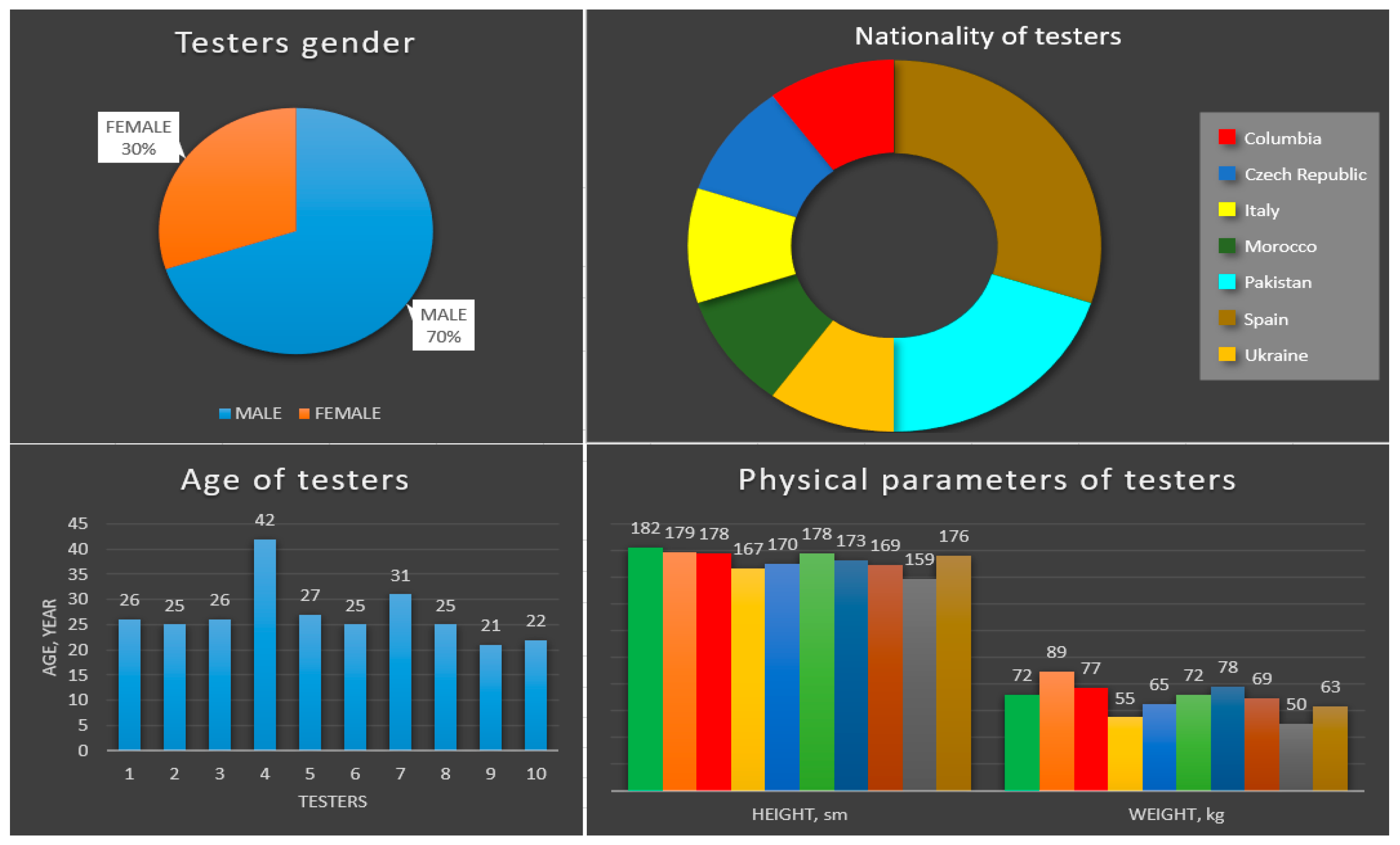
3.1.3. Experimental Features
- (a)
- Information about testers
- (b)
- Testing plan and regulations
3.2. Methods
3.2.1. Overall View
- (a)
- Gaming platform
- Levels of settings
- Levels for the upper body
- Levels for the lower body.
- (b)
- Exercises used
- (1)
- “The sign of infinity”. This exercise is a simple activity for the upper extremities. The task involves putting your hands with the palms in front of you, bending your hands at the elbows, and describing the “sign of infinity” in the air. This exercise should be repeated 10 times for each hand, keeping in mind that the right hand moves clockwise and the left counterclockwise. The purpose of this exercise is to assess the player’s motor skills and coordination.
- (2)
- “Rope Pull”. This level is a movement that is exactly the same as a top-down rope pull, repeated 10 times overall. The goal is to assess the overall mobility of the upper extremities, as well as the accuracy and simultaneity of the movements.
- (3)
- “Inflating the lifejacket”. This exercise is similar to the previous one, but also involves the shoulder girdle. The activity is also aimed at assessing the synchronicity of actions and the general condition of the upper body.
- (4)
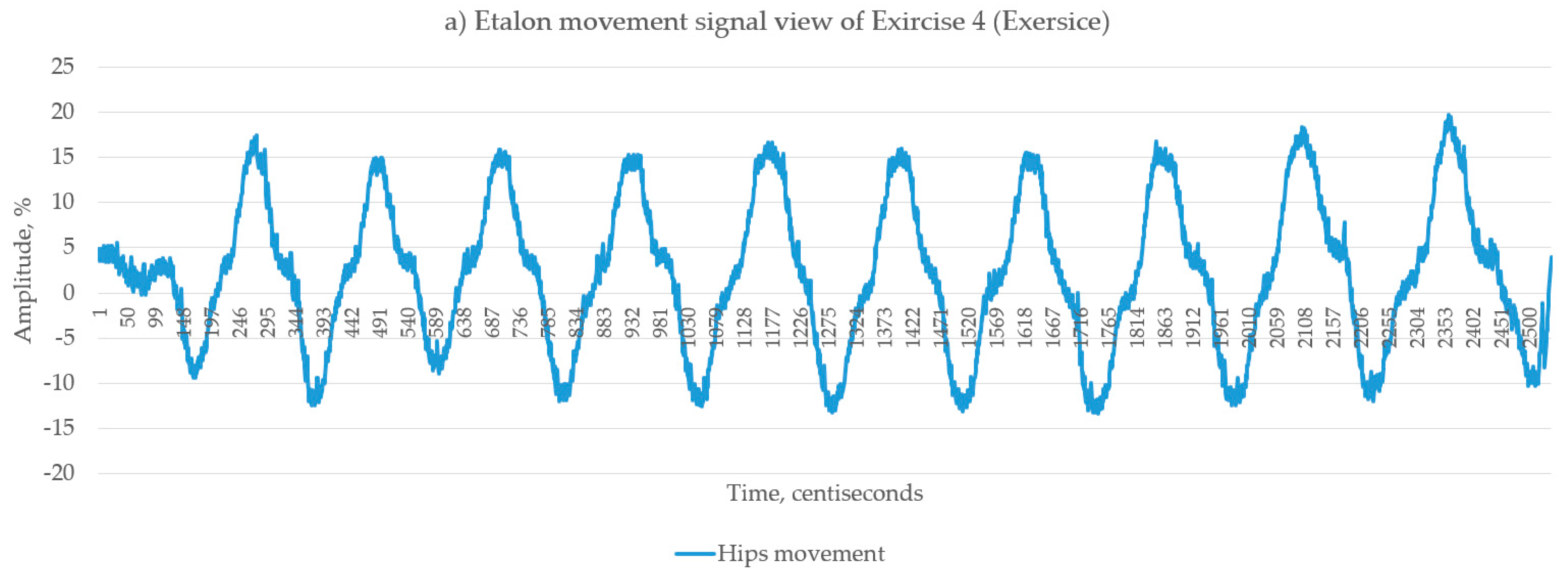
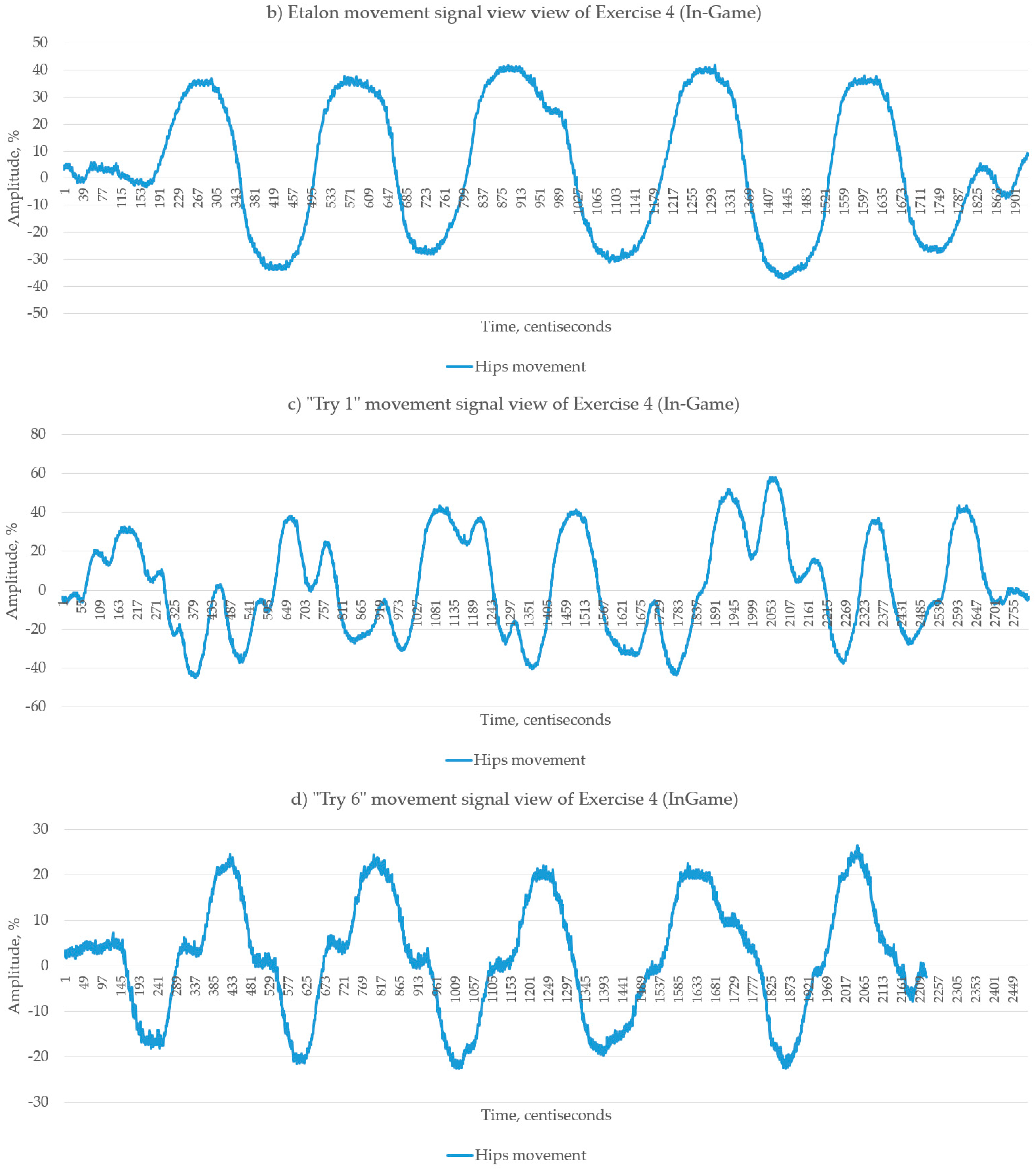
- “Sailing on a yacht”. The essence of this exercise is to steer the boat and pass through 10 control points, by moving the hips left and right. It is necessary to perform 10 repetitions in each direction. The purpose is to assess the general mobility of the joints of the pelvic area, and condition of the lumbar spine, as well as to train balance.
- (5)
- “Dinghy Control”. Conceptually, this exercise is similar to the previous one. The only difference is that this time, the movement is not with the hips but with the shoulder girdle. In this case, the main purpose of the exercise is to support and warm up the spine and examine its condition.
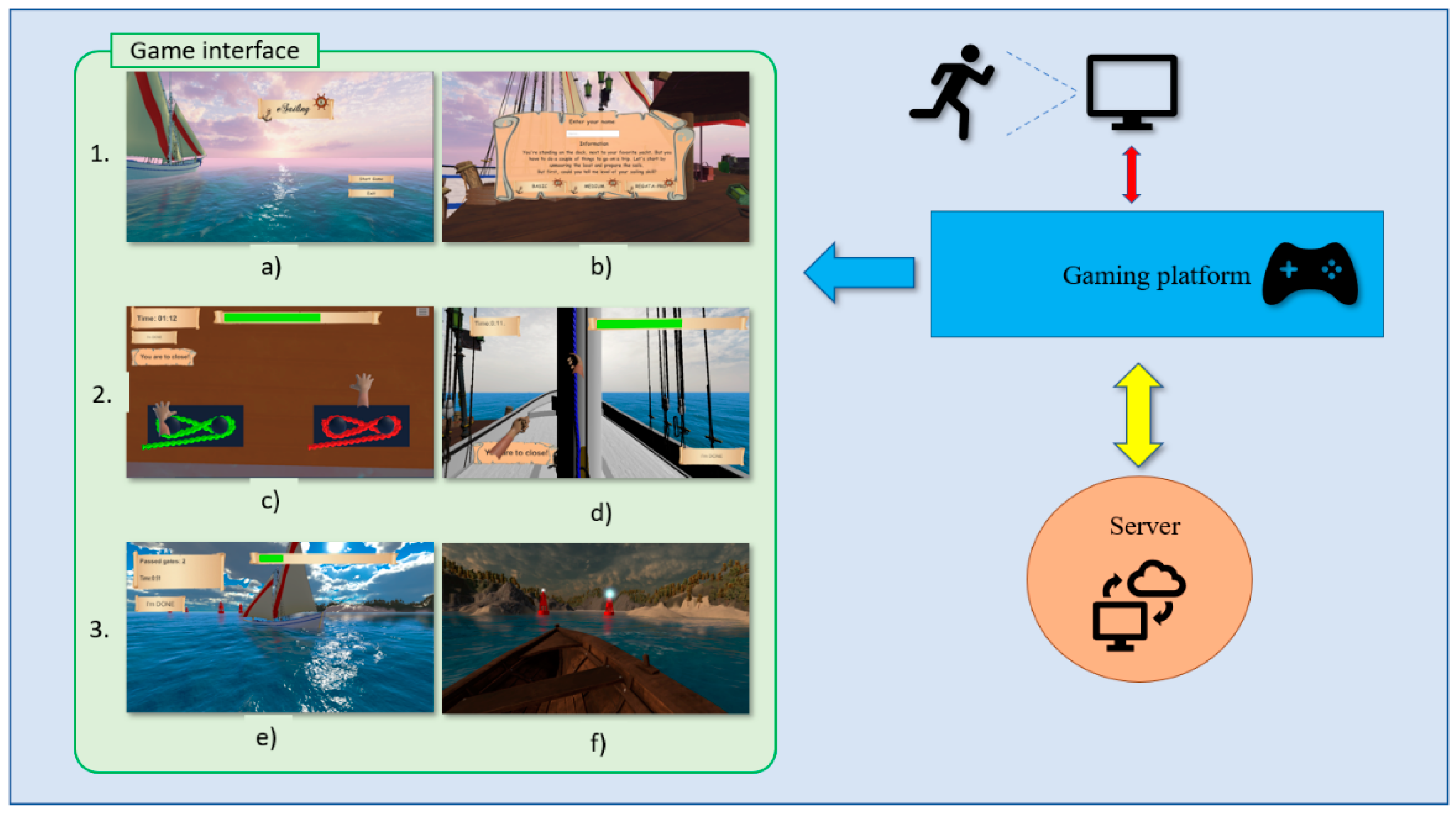
- (c)
- Game Interface
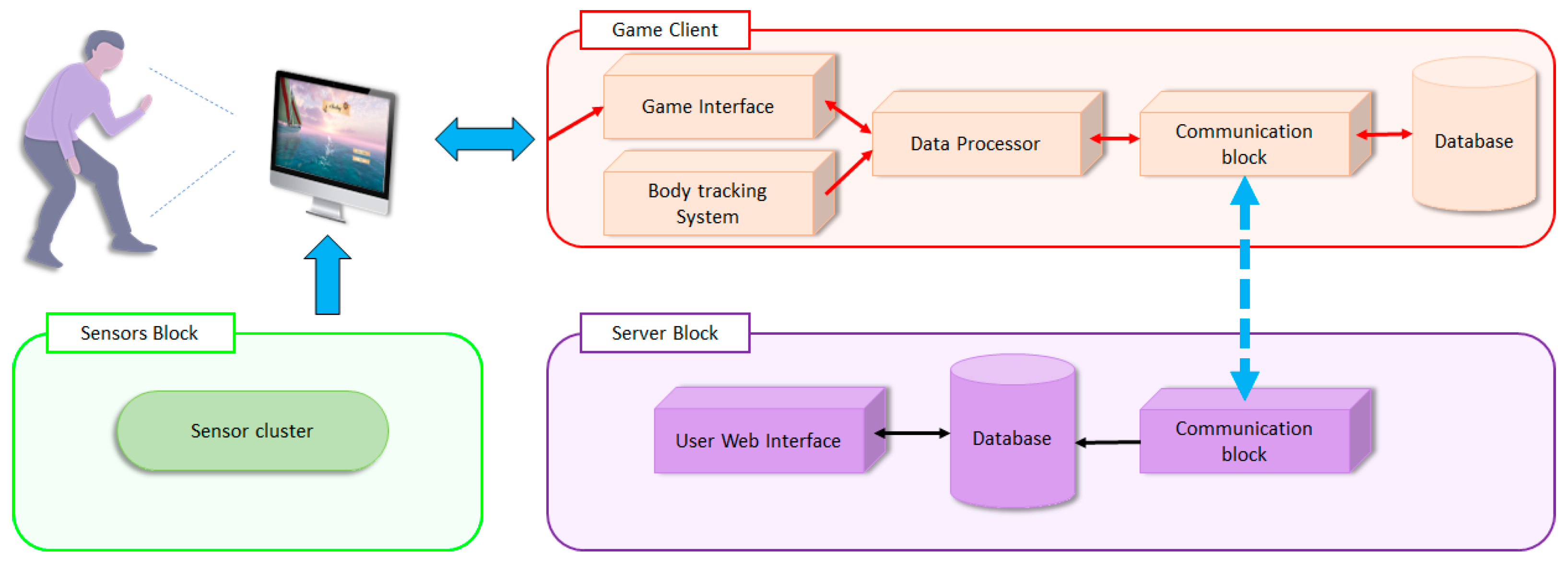
3.2.2. Architecture Explanation
3.2.3. Body Tracking System Description
- The hand recognition module has been reduced (fingers, palm).
- The face recognition module (eyes, mouth, nose, ears, eyebrows) was reduced.
- The storyboarding process was optimized, which allowed a stable 30 fps to be obtained (in the original state the rate was 18–24 fps).
3.2.4. Game Structure
- A level guide with a description of the task, and a demonstration of the movement to be performed by the player
- The actual playing process (performing the exercise)
- The result window, where the player sees how well they did, and the transition window to the next activity (level).
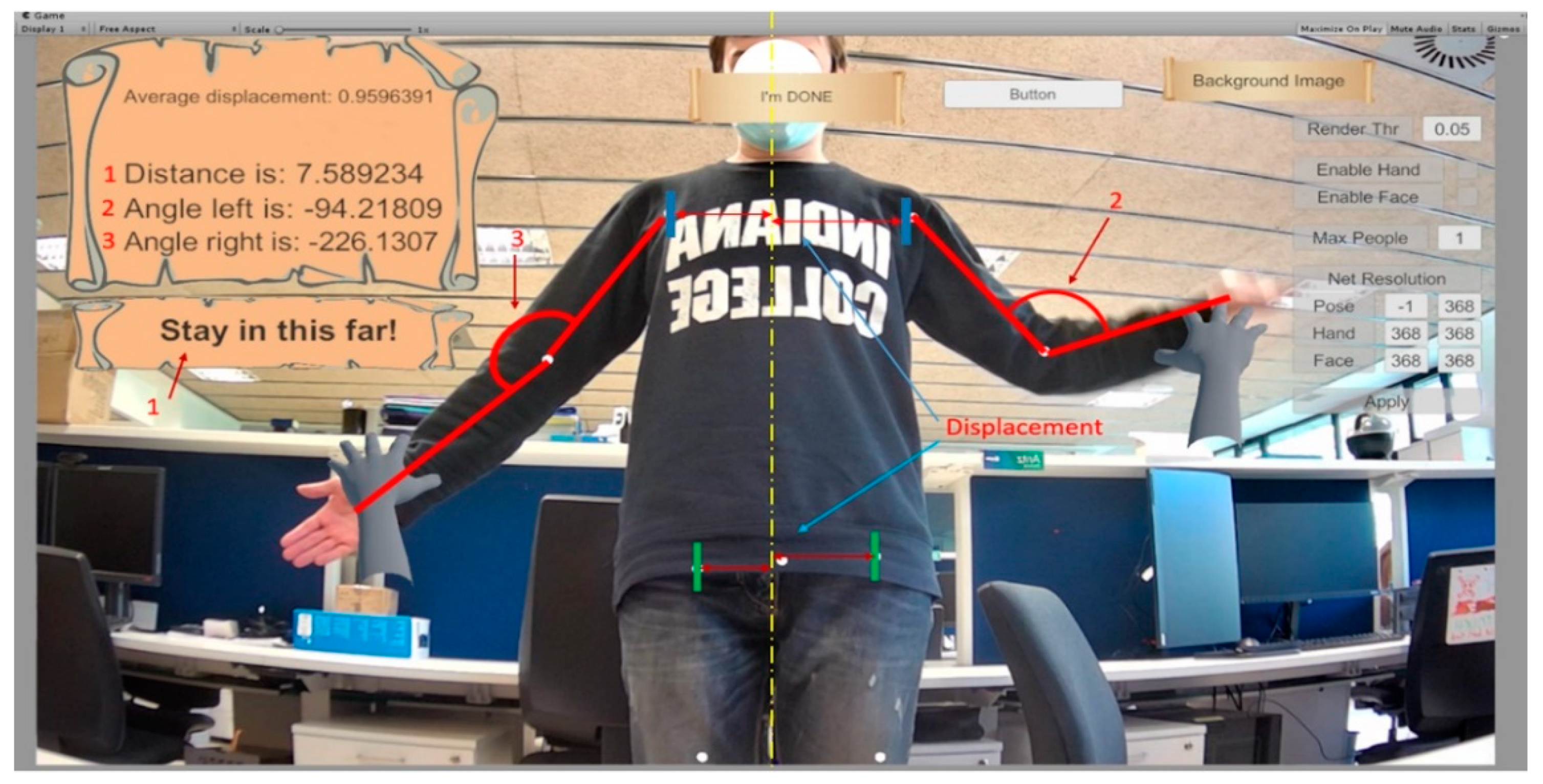
3.2.5. Data Collection Method
- Angle between shoulder and left hand forearm
- Angle between shoulder and right hand forearm
- Left hand position
- Right arm position
- Hip position
- Shoulder position
- Head position
- Head rotation angle.
- The timing of the player’s movements, both the total number and each repetition individually
- The maximum value of the deviation amplitude, which indicates the intensity of the exercise
- The activity as a whole, based on the number of peak values of the deviation amplitude
- The evaluative characteristic of motor skills, based on the direction in which there is a greater number of peak values of the deviation amplitude.
3.2.6. Data Saving and Interpretation
- Right- and left-hand angle data—information that allows you to assess the overall movement activity of the player when performing upper limb exercises
- Head angle and head displacement data—allow tracking the degree of rotation of the player’s head. Useful for understanding the approximate direction of the player’s gaze, as well as problems with general motor skills (for problems with the cervical spine
- Range data—show the general dynamics of the player’s position in space. Useful for evaluating general activity, as well as for evaluating the player’s movement during game activities
- Hips and shoulders displacement data—show the dynamic displacement of the player’s shoulders and hips, as well as the degree of this displacement
- Left and right arm displacement data—the activity of the player’s hand movement. Characteristics of upper and lower maximum deflection, smoothness, and accuracy of the movements
- Average arm, hip, and shoulder movements—characteristics that allow the average position of the body to be estimated, as well as individual areas of the body. Useful when researching into temporary or permanent partial atrophy, palsy, or dysfunction of the muscles of a particular area of the body.
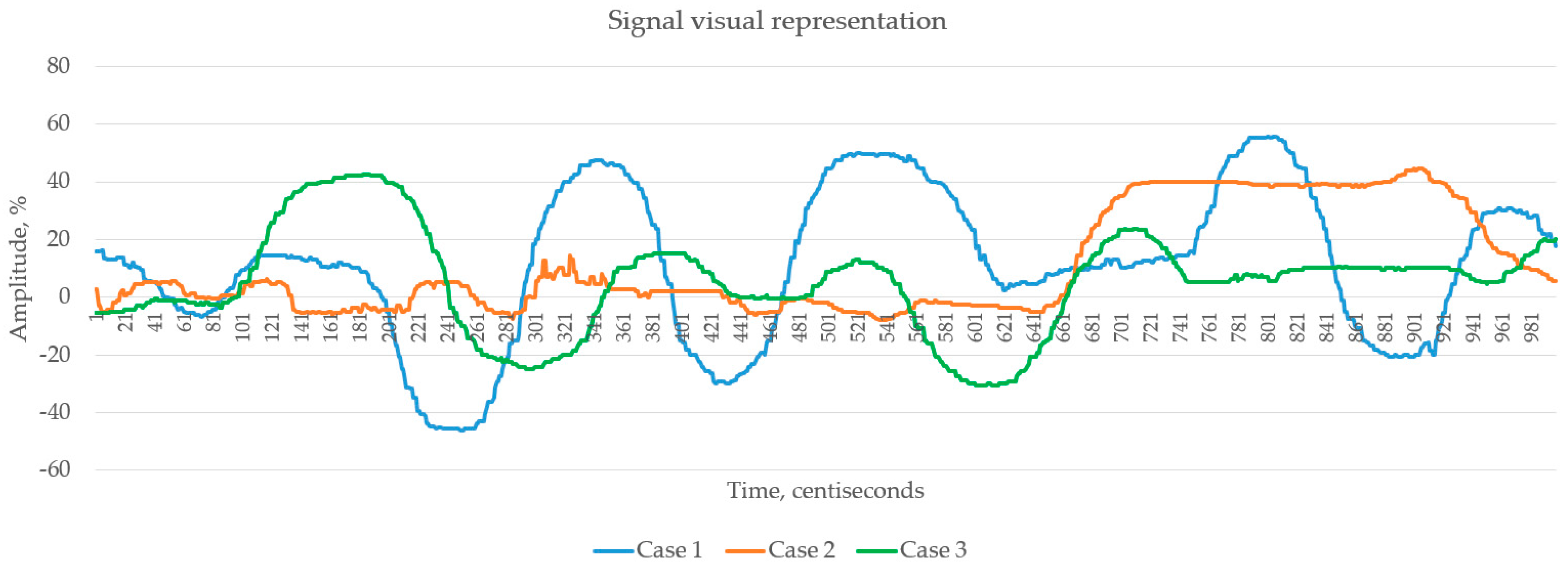
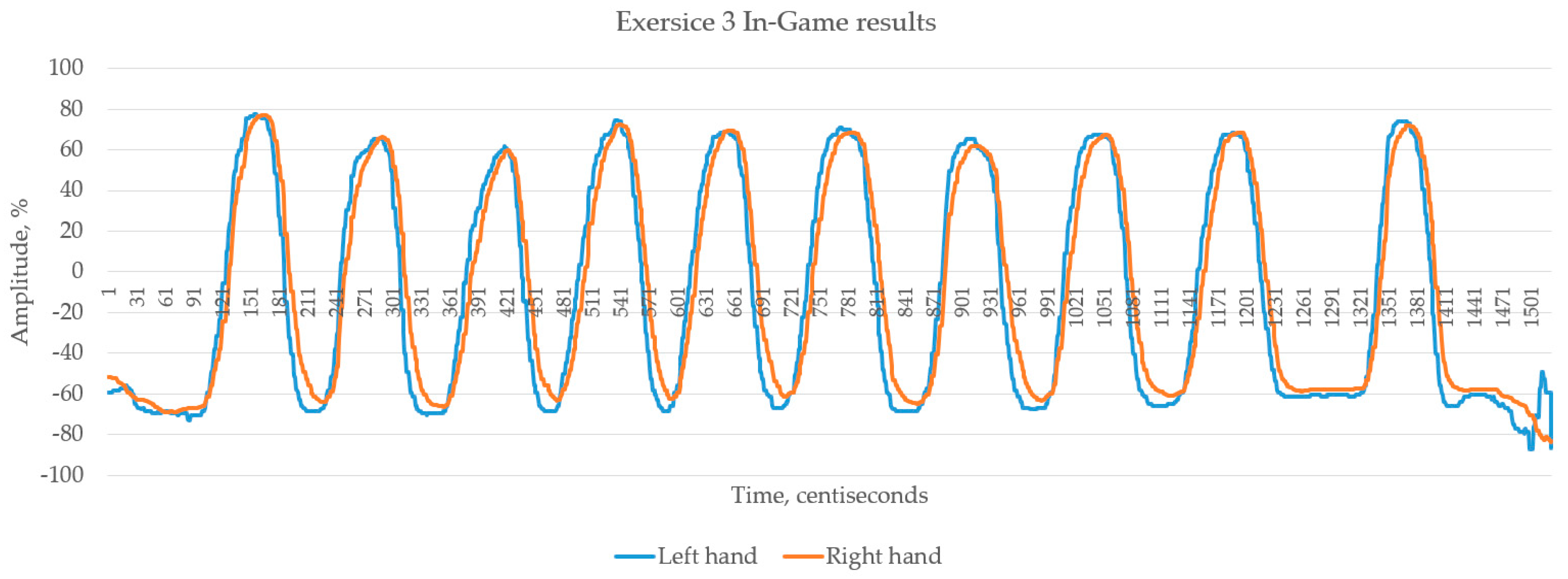
3.2.7. Data Visualization
- Time to complete each task
- Amplitude of the received signal (by means of direct Fourier transform);
- Frequency of repetitions
- Repetition period
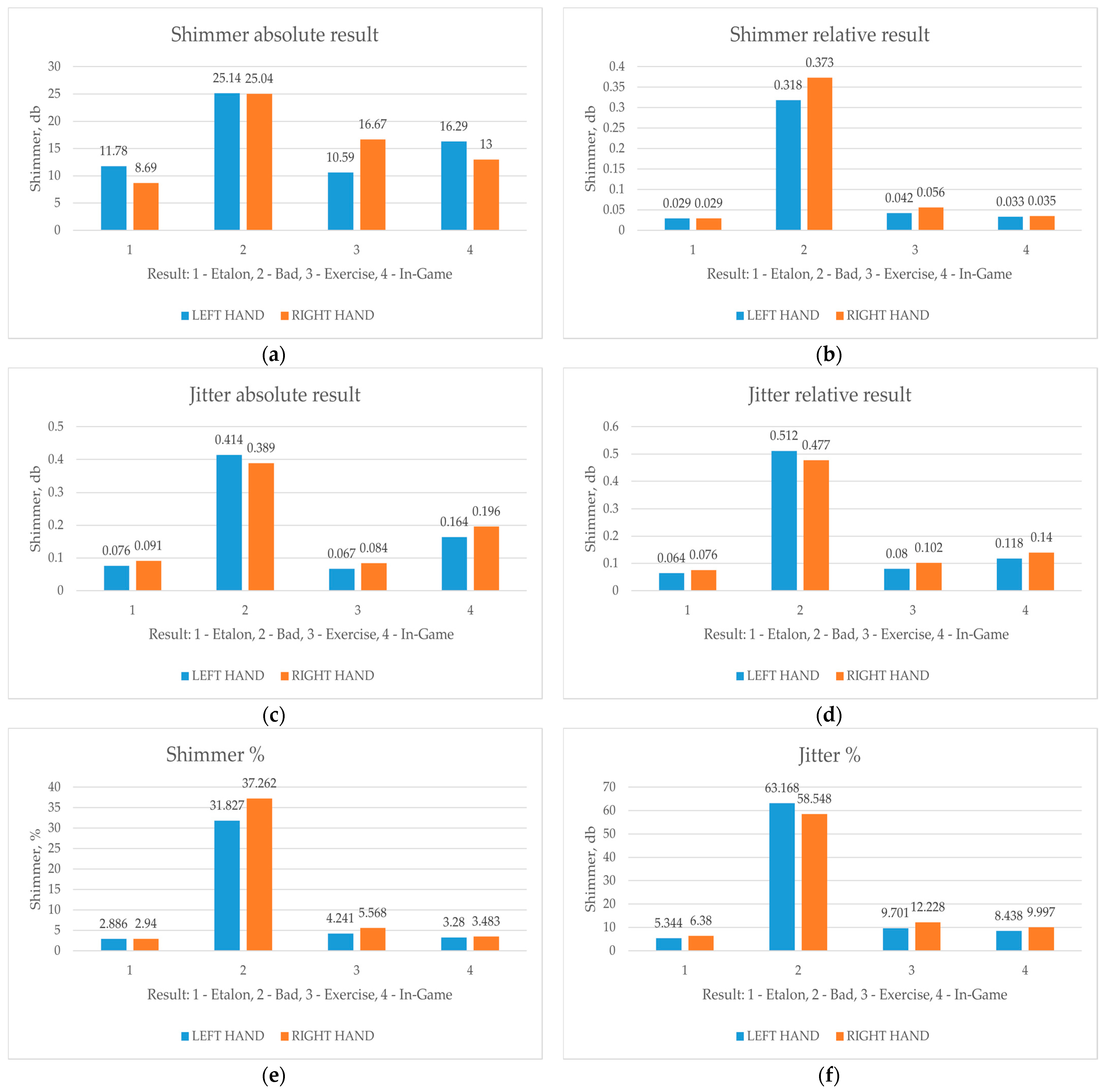
- Jitter and shimmer.
3.2.8. Data Comparison
- (a)
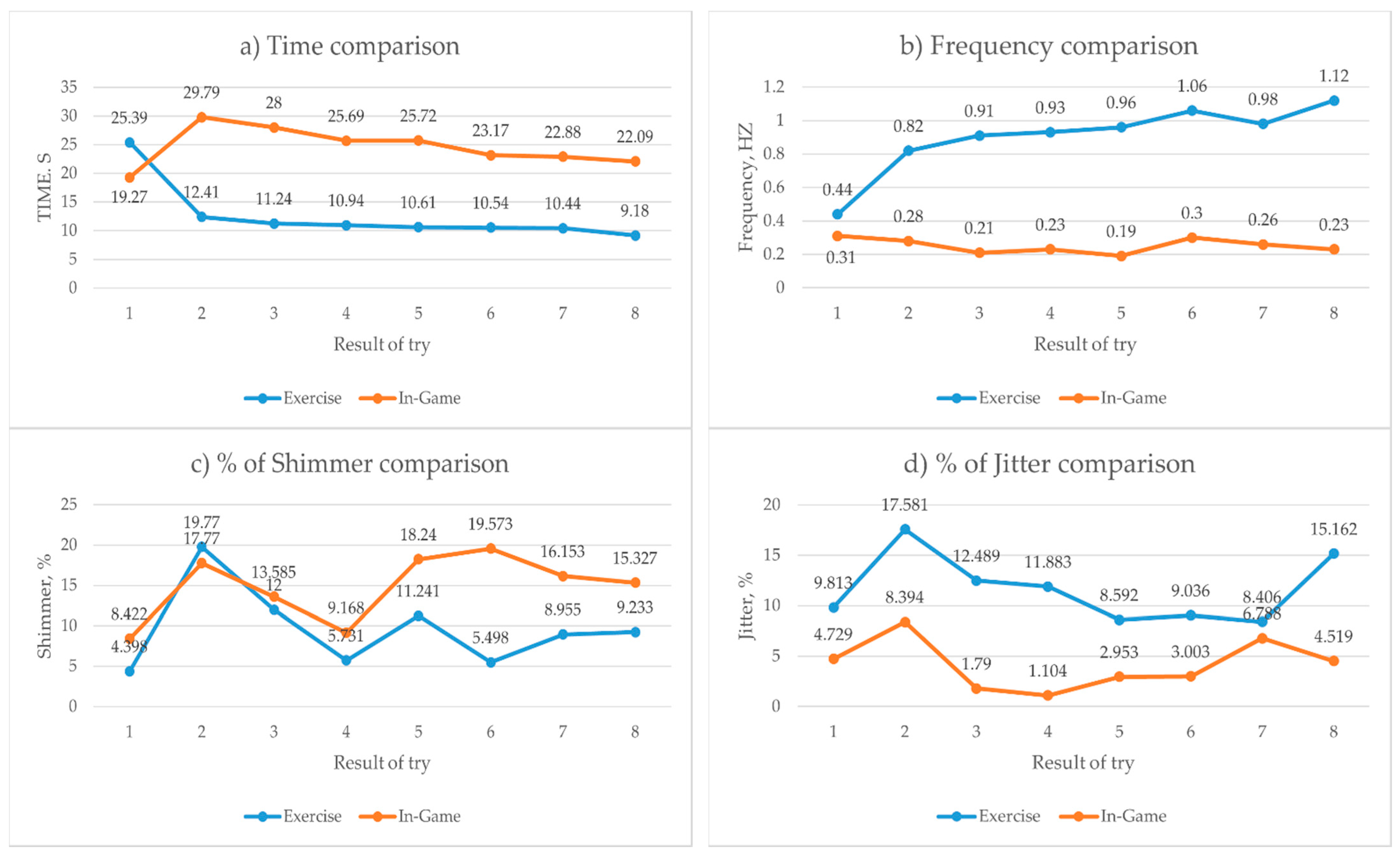
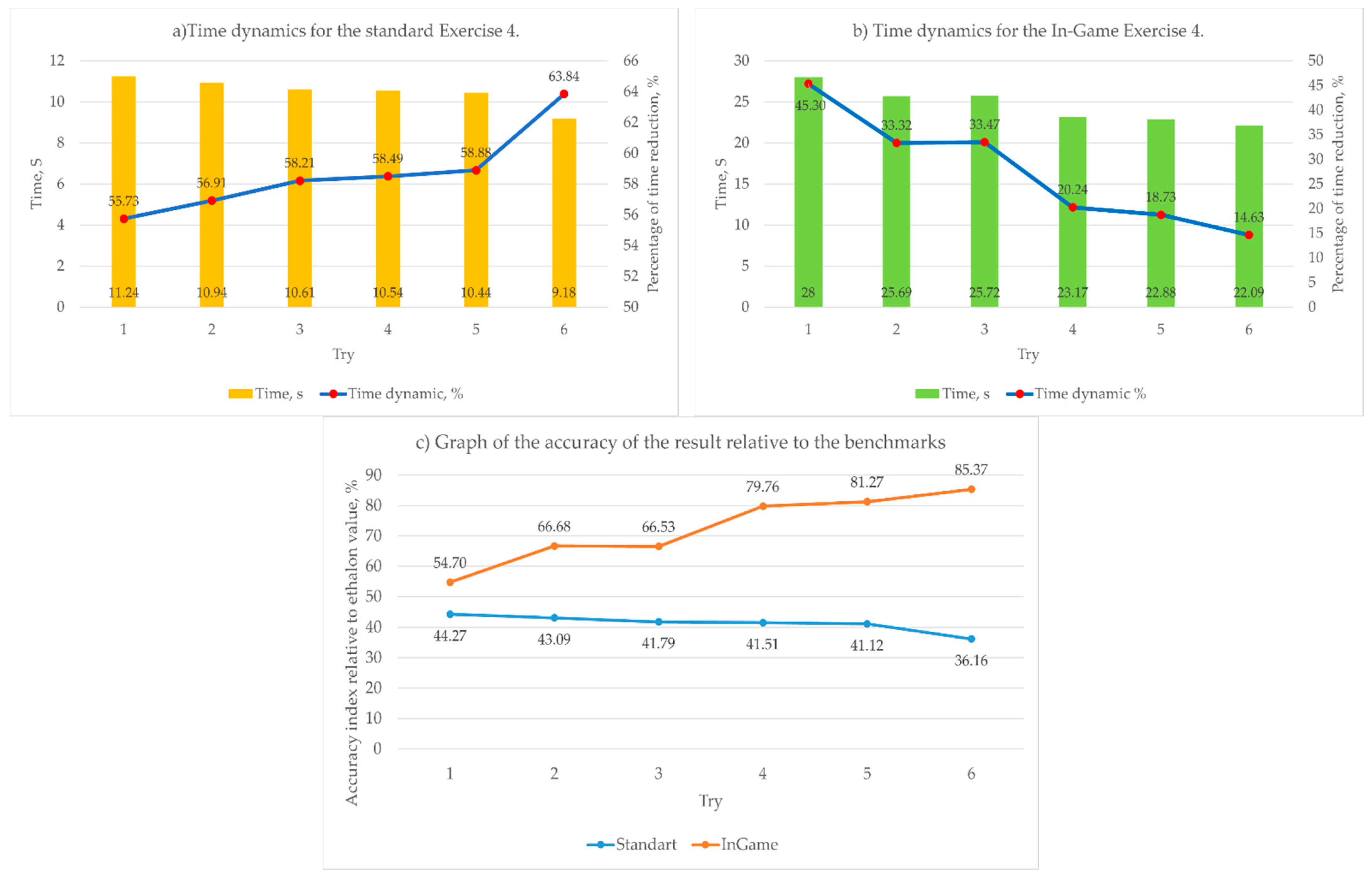
- Time parameter:
- (b)
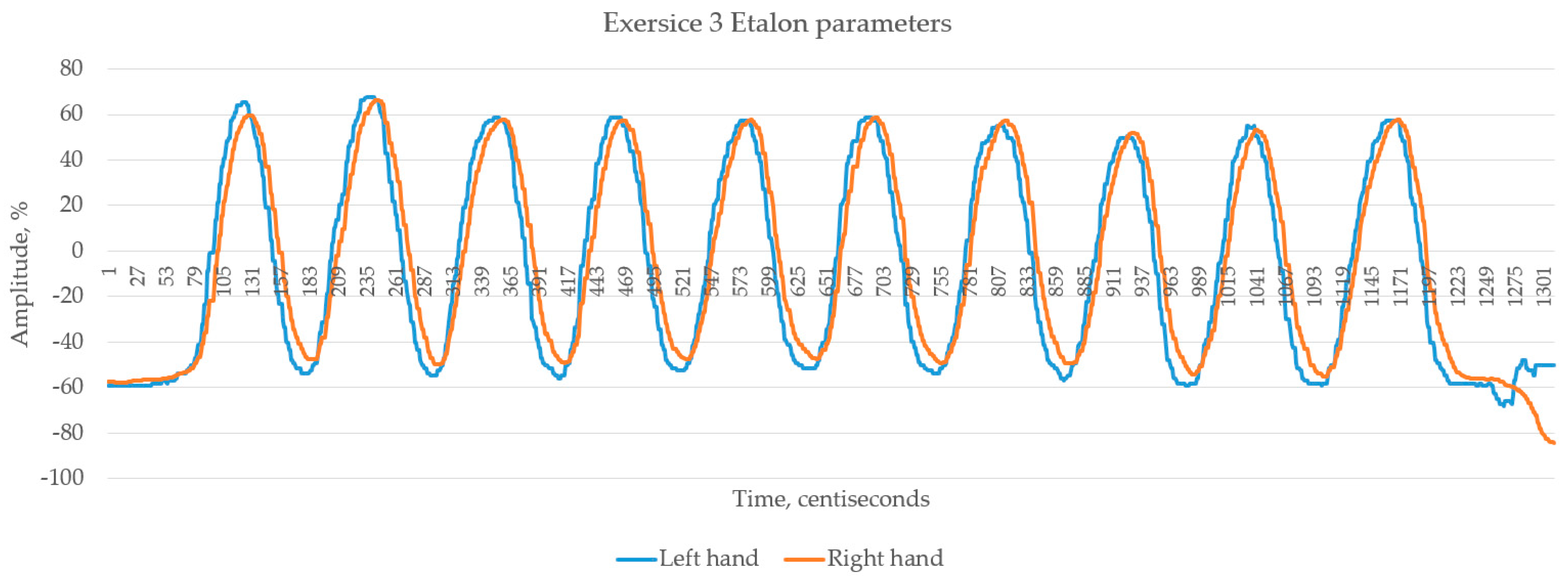
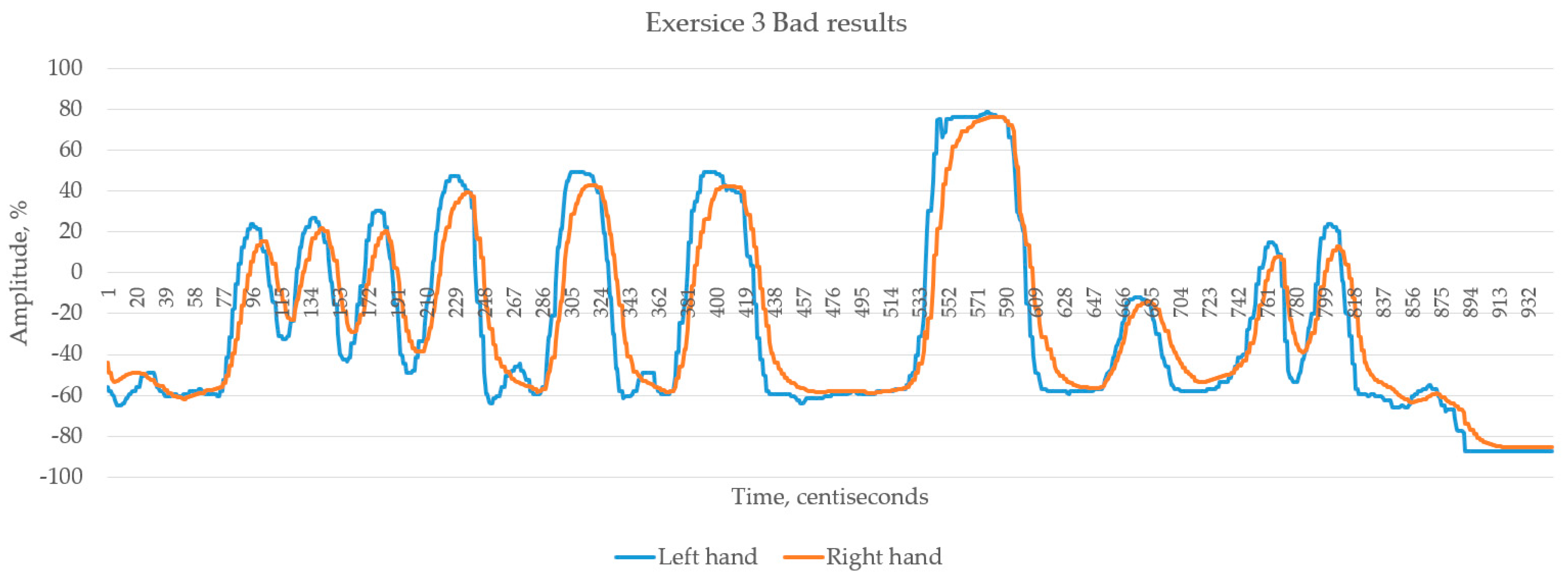
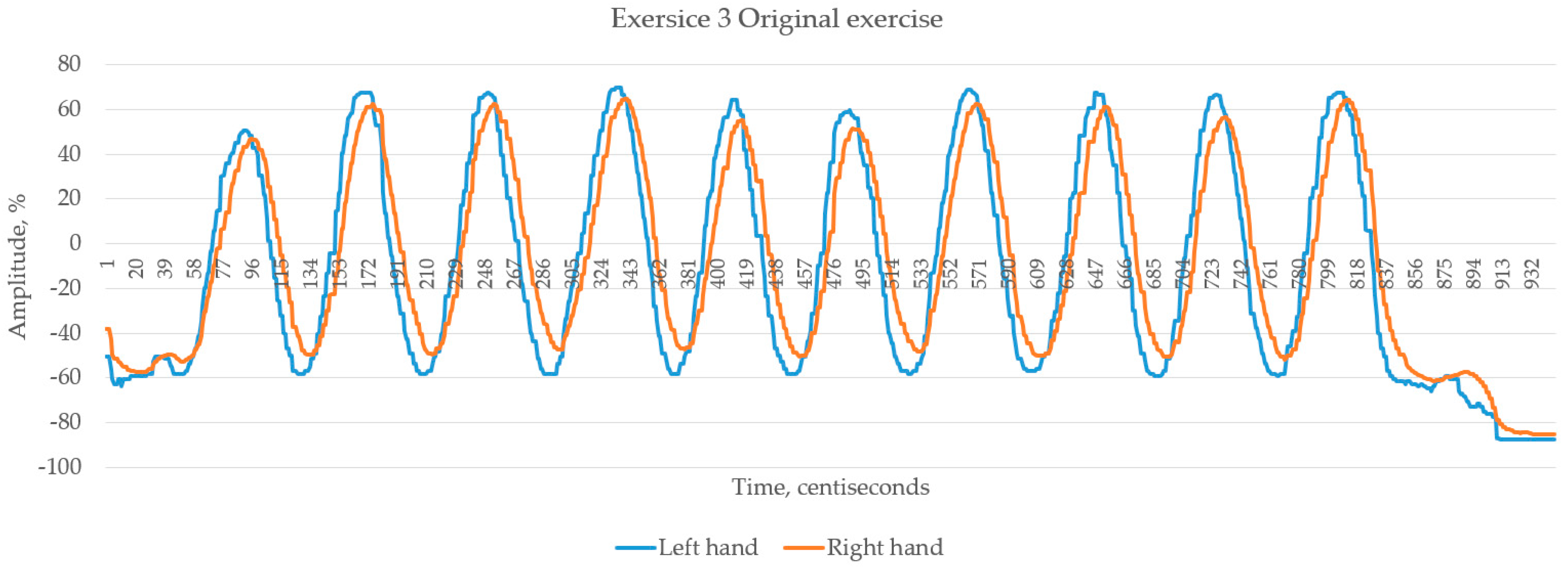
- Amplitude parameter:
- (c)
- Frequency of repetitions:
- (d)
- Shimmer and Jitter:
4. Results
4.1. Comparison of Results
4.2. Explanations of Results
5. Discussion
6. Conclusions and Future Plans
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tscheikner-Gratl, F.; Egger, P.; Rauch, W.; Kleidorfer, M. Comparison of multi-criteria decision support methods for integrated rehabilitation prioritization. Water 2017, 9, 68. [Google Scholar] [CrossRef] [Green Version]
- Bisio, I.; Delfino, A.; Lavagetto, F.; Sciarrone, A. Enabling IoT for in-home rehabilitation: Accelerometer signals classification methods for activity and movement recognition. IEEE Internet Things J. 2016, 4, 135–146. [Google Scholar]
- Faria, A.L.; Andrade, A.; Soares, L.; i Badia, S.B. Benefits of virtual reality based cognitive rehabilitation through simulated activities of daily living: A randomized controlled trial with stroke patients. J. Neuroeng. Rehabil. 2016, 13, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bush, M.L.; Dougherty, W. Assessment of vestibular rehabilitation therapy training and practice patterns. J. Community Health 2015, 40, 802–807. [Google Scholar] [CrossRef]
- Tsoupikova, D.; Stoykov, N.S.; Corrigan, M.; Thielbar, K.; Vick, R.; Li, Y.; Kamper, D. Virtual immersion for post-stroke hand rehabilitation therapy. Ann. Biomed. Eng. 2015, 43, 467–477. [Google Scholar] [CrossRef]
- Röijezon, U.; Clark, N.C.; Treleaven, J. Proprioception in musculoskeletal rehabilitation. Part 1: Basic science and principles of assessment and clinical interventions. Man. Ther. 2015, 20, 368–377. [Google Scholar] [CrossRef]
- Tannous, H.; Istrate, D.; Benlarbi-Delai, A.; Sarrazin, J.; Gamet, D.; Ho Ba Tho, M.C.; Dao, T.T. A new multi-sensor fusion scheme to improve the accuracy of knee flexion kinematics for functional rehabilitation movements. Sensors 2016, 16, 1914. [Google Scholar] [CrossRef] [Green Version]
- Grooms, D.; Appelbaum, G.; Onate, J. Neuroplasticity following anterior cruciate ligament injury: A framework for visual-motor training approaches in rehabilitation. J. Orthop. Sports Phys. Ther. 2015, 45, 381–393. [Google Scholar]
- Sánchez-Rodríguez, D.; Miralles, R.; Muniesa, J.M.; Mojal, S.; Abadía-Escartín, A.; Vázquez-Ibar, O. Three measures of physical rehabilitation effectiveness in elderly patients: A prospective, longitudinal, comparative analysis. BMC Geriatr. 2015, 15, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohse, K.; Shirzad, N.; Verster, A.; Hodges, N.; Van der Loos, H.M. Video games and rehabilitation: Using design principles to enhance engagement in physical therapy. J. Neurol. Phys. Ther. 2013, 37, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Mugueta-Aguinaga, I.; Garcia-Zapirain, B. Is technology present in frailty? Technology a back-up tool for dealing with frailty in the elderly: A systematic review. Aging Dis. 2017, 8, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaparro-Cárdenas, S.L.; Lozano-Guzmán, A.A.; Ramirez-Bautista, J.A.; Hernández-Zavala, A. A review in gait rehabilitation devices and applied control techniques. Disabil. Rehabil. Assist. Technol. 2018, 13, 819–834. [Google Scholar] [CrossRef] [PubMed]
- Babaiasl, M.; Mahdioun, S.H.; Jaryani, P.; Yazdani, M. A review of technological and clinical aspects of robot-aided rehabilitation of upper-extremity after stroke. Disabil. Rehabil. Assist. Technol. 2016, 11, 263–280. [Google Scholar] [CrossRef]
- Ward, T.; Heffernan, R. The role of values in forensic and correctional rehabilitation. Aggress. Violent Behav. 2017, 37, 42–51. [Google Scholar] [CrossRef]
- Wade, D. Rehabilitation—A new approach. Overview and part one: The problems. Sage J. 2015, 29, 1041–1050. [Google Scholar] [CrossRef] [Green Version]
- Frutos-Pascual, M.; Zapirain, B.G.; Zorrilla, A.M. Adaptive tele-therapies based on serious games for health for people with time-management and organisational problems: Preliminary results. Int. J. Environ. Res. Public Health 2014, 11, 749–772. [Google Scholar] [CrossRef] [Green Version]
- Khan, F.; Amatya, B. Refugee health and rehabilitation: Challenges and response. J. Rehabil. Med. 2017, 49, 378–384. [Google Scholar] [CrossRef] [Green Version]
- Christiansen, B.; Feiring, M. Challenges in the nurse’s role in rehabilitation contexts. J. Clin. Nurs. 2017, 26, 3239–3247. [Google Scholar] [CrossRef] [PubMed]
- Rikkers, W.; Lawrence, D.; Hafekost, J.; Zubrick, S.R. Internet use and electronic gaming by children and adolescents with emotional and behavioural problems in Australia–results from the second Child and Adolescent Survey of Mental Health and Wellbeing. BMC Public Health 2016, 16, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnechère, B. Serious Games in Physical Rehabilitation; Springer International Publishing: Berlin/Heidelberg, Germany, 2018; pp. 72–78. [Google Scholar]
- Ortiz-Vigon Uriarte, I.D.L.; Garcia-Zapirain, B.; Garcia-Chimeno, Y. Game design to measure reflexes and attention based on biofeedback multi-sensor interaction. Sensors 2015, 15, 6520–6548. [Google Scholar] [CrossRef] [Green Version]
- Ushaw, G.; Davison, R.; Eyre, J.; Morgan, G. Adopting best practices from the games industry in development of serious games for health. In Proceedings of the 5th International Conference on Digital Health, Florence, Italy, 18–20 May 2015; pp. 1–8. [Google Scholar]
- de Urturi Breton, Z.S.; Hernández, F.J.; Zorrilla, A.M.; Zapirain, B.G. Mobile communication for intellectually challenged people: A proposed set of requirements for interface design on touch screen devices. Commun. Mob. Comput. 2012, 1, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Ricotti, V.; Mandy, W.P.; Scoto, M.; Pane, M.; Deconinck, N.; Messina, S.; Muntoni, F. Neurodevelopmental, emotional, and behavioural problems in Duchenne muscular dystrophy in relation to underlying dystrophin gene mutations. Dev. Med. Child Neurol. 2016, 58, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Edgren, J.; Salpakoski, A.; Sihvonen, S.E.; Portegijs, E.; Kallinen, M.; Arkela, M.; Sipilä, S. Effects of a home-based physical rehabilitation program on physical disability after hip fracture: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2015, 16, 350-e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goršič, M.; Cikajlo, I.; Novak, D. Competitive and cooperative arm rehabilitation games played by a patient and unimpaired person: Effects on motivation and exercise intensity. J. Neuroeng. Rehabil. 2017, 14, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Bonnechère, B.; Jansen, B.; Omelina, L.; Van Sint Jan, S. The use of commercial video games in rehabilitation: A systematic review. Int. J. Rehabil. Res. 2016, 39, 277–290. [Google Scholar] [CrossRef]
- Hocine, N.; Gouaïch, A.; Cerri, S.A.; Mottet, D.; Froger, J.; Laffont, I. Adaptation in serious games for upper-limb rehabilitation: An approach to improve training outcomes. User Model. User Adapt. Interact. 2015, 25, 65–98. [Google Scholar] [CrossRef]
- Nguyen TT, H.; Ishmatova, D.; Tapanainen, T.; Liukkonen, T.N.; Katajapuu, N.; Makila, T.; Luimula, M. Impact of serious games on health and well-being of elderly: A systematic review. In Proceedings of the 50th Hawaii International Conference on System Sciences, Hilton Waikoloa Village, HI, USA, 4–7 January 2017. [Google Scholar]
- Howard, M.C. A meta-analysis and systematic literature review of virtual reality rehabilitation programs. Comput. Hum. Behav. 2017, 70, 317–327. [Google Scholar] [CrossRef]
- Kawagoshi, A.; Kiyokawa, N.; Sugawara, K.; Takahashi, H.; Sakata, S.; Satake, M.; Shioya, T. Effects of low-intensity exercise and home-based pulmonary rehabilitation with pedometer feedback on physical activity in elderly patients with chronic obstructive pulmonary disease. Respir. Med. 2015, 109, 364–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madani, K.; Pierce, T.W.; Mirchi, A. Serious games on environmental management. Sustain. Cities Soc. 2017, 29, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Rego, P.; Moreira, P.M.; Reis, L.P. Serious games for rehabilitation: A survey and a classification towards a taxonomy. In Proceedings of the 5th Iberian Conference on Information Systems and Technologies, Santiago de Compostela, Spain, 16–19 June 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 1–6. [Google Scholar]
- Loh, C.S.; Sheng, Y.; Ifenthaler, D. Serious games analytics: Theoretical framework. In Serious Games Analytics; Springer: Cham, Switzerland, 2015; pp. 3–29. [Google Scholar]
- Lun, R.; Zhao, W. A survey of applications and human motion recognition with Microsoft kinect. Int. J. Pattern Recognit. Artif. Intell. 2015, 29, 1555008. [Google Scholar] [CrossRef] [Green Version]
- Anthes, C.; García-Hernández, R.J.; Wiedemann, M.; Kranzlmüller, D. State of the art of virtual reality technology. In Proceedings of the 2016 IEEE Aerospace Conference, Big Sky, MT, USA, 5–12 March 2016; IEEE: Piscataway, NJ, USA; pp. 1–19. [Google Scholar]
- Cao, Z.; Hidalgo, G.; Simon, T.; Wei, S.E.; Sheikh, Y. OpenPose: Realtime multi-person 2D pose estimation using Part Affinity Fields. IEEE Trans. Pattern Anal. Mach. Intell. 2019, 43, 172–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kendall, A.; Grimes, M.; Cipolla, R. Posenet: A convolutional network for real-time 6-dof camera relocalization. In Proceedings of the IEEE International Conference on Computer Vision, Santiago, Chile, 7–13 December 2015; pp. 2938–2946. [Google Scholar]
- Carvalho, M.B.; Bellotti, F.; Berta, R.; De Gloria, A.; Sedano, C.I.; Hauge, J.B.; Rauterberg, M. An activity theory-based model for serious games analysis and conceptual design. Comput. Educ. 2015, 87, 166–181. [Google Scholar] [CrossRef]
- Lopez-Basterretxea, A.; Mendez-Zorrilla, A.; Garcia-Zapirain, B. A telemonitoring tool based on serious games addressing money management skills for people with intellectual disability. Int. J. Environ. Res. Public Health 2014, 11, 2361–2380. [Google Scholar] [CrossRef] [Green Version]
- Sáenz-de-Urturi, Z.; García Zapirain, B.; Méndez Zorrilla, A. Elderly user experience to improve a Kinect-based game playability. Behav. Inf. Technol. 2015, 34, 1040–1051. [Google Scholar] [CrossRef]
- Avola, D.; Cinque, L.; Foresti, G.L.; Marini, M.R. An interactive and low-cost full body rehabilitation framework based on 3D immersive serious games. J. Biomed. Inform. 2019, 89, 81–100. [Google Scholar] [CrossRef] [PubMed]
- González-González, C.S.; Toledo-Delgado, P.A.; Muñoz-Cruz, V.; Torres-Carrion, P.V. Serious games for rehabilitation: Gestural interaction in personalized gamified exercises through a recommender system. J. Biomed. Inform. 2019, 97, 103266. [Google Scholar] [CrossRef]
- Amengual Alcover, E.; Jaume-i-Capó, A.; Moyà-Alcover, B. PROGame: A process framework for serious game development for motor rehabilitation therapy. PLoS ONE 2018, 13, e0197383. [Google Scholar] [CrossRef] [Green Version]
- Meijer, H.A.; Graafland, M.; Goslings, J.C.; Schijven, M.P. Systematic review on the effects of serious games and wearable technology used in rehabilitation of patients with traumatic bone and soft tissue injuries. Arch. Phys. Med. Rehabil. 2018, 99, 1890–1899. [Google Scholar] [CrossRef]
- Morando, M.; Ponte, S.; Ferrara, E.; Dellepiane, S. Definition of motion and biophysical indicators for home-based rehabilitation through serious games. Information 2018, 9, 105. [Google Scholar] [CrossRef] [Green Version]
- Tăut, D.; Pintea, S.; Roovers, J.P.W.; Mañanas, M.A.; Băban, A. Play seriously: Effectiveness of serious games and their features in motor rehabilitation. A meta-analysis. NeuroRehabilitation 2017, 41, 105–118. [Google Scholar] [CrossRef]
- Sánchez-Herrera-Baeza, P.; Cano-de-la-Cuerda, R.; Oña-Simbaña, E.D.; Palacios-Ceña, D.; Pérez-Corrales, J.; Cuenca-Zaldivar, J.N.; Cuesta-Gomez, A. The Impact of a Novel Immersive Virtual Reality Technology Associated with Serious Games in Parkinson’s Disease Patients on Upper Limb Rehabilitation: A Mixed Methods Intervention Study. Sensors 2020, 20, 2168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Postolache, G.; Carry, F.; Lourenço, F.; Ferreira, D.; Oliveira, R.; Girão, P.S.; Postolache, O. Serious Games Based on Kinect and Leap Motion Controller for Upper Limbs Physical Rehabilitation. In Modern Sensing Technologies; Springer: Cham, Switzerland, 2019; pp. 147–177. [Google Scholar]
- Ling, Y.; Ter Meer, L.P.; Yumak, Z.; Veltkamp, R.C. Usability test of exercise games designed for rehabilitation of elderly patients after hip replacement surgery: Pilot study. JMIR Serious Games 2017, 5, e19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palestra, G.; Rebiai, M.; Courtial, E.; Koutsouris, D. Evaluation of a rehabilitation system for the elderly in a day care center. Information 2019, 10, 3. [Google Scholar] [CrossRef] [Green Version]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Aim of the Article | Hardware Used | Algorithm | Measurements | Results |
|---|---|---|---|---|---|
| [42] | Present low-cost full body rehabilitation framework for the generation of 3D immersive serious games | Camera system: ToF camera IR camera HDM device (Virtual Reality helmet) | GRU-RNN Virtual Reality algorithms | Track position of the body in space. | Increase in rehabilitation rates by an average 15% |
| [43] | Introduce a smart rehabilitation system for the elderly, without requiring physical contact with traditional control systems. | Webcam | TANGO:H 2d representation system | The method used in the study is based on the evaluation of a vision-based gesture interface by measuring effectiveness, efficiency, and satisfaction. | Gestural exercises yielded higher percentages of task completion (>83%) and task effectiveness (>63%). Eye fatigue(x = 3.15; SD = 0.37). Accurate point is above average (x = 2.57; SD = 0.60) |
| [44] | Improvement in the balance and postural control of adults. | Webcam + markers Vision-based interaction sensor Wii mote | Modified algorithm based on Kinect body tracking technology | Body position Balance indicators | Usage of interaction objects related to patient interests; patients performed the rehabilitation activity 13.5% faster than when the objects did not represent such interests |
| [45] | Assess the effects on functional outcomes and treatment adherence of wearable technology and serious games currently used in physical rehabilitation of patients following traumatic bone and soft tissue injuries. | - | Comparison methods of serious games with standard therapy | The search yielded 2704 eligible articles, which were screened by 2 independent reviewers. | Serious games seem a safe alternative or addition to conventional physiotherapy following traumatic bone and soft tissue injuries. |
| [46] | Describe of newly-developed platform of Remote Monitoring Validation Engineering System for motion rehabilitation. | Microsoft Kinect V2 Microsoft Band 2 | Leap Motion Cloud back-end | Different aspects of upper and lower limbs movement, balance, heart rate and electrodermal activity, balance shift. | Most games within this system are nearly useless for supervised analysis. |
| [47] | Research into the effectiveness of SGs in motor rehabilitation for upper limb and movement/balance | - | Rehabilitation games and systems data systematizing and comparison | Meta-analysis including 61 studies reporting randomized controlled trials in which at least one intervention for motor rehabilitation is included. | Overall moderate effect of SGs on motor indexes, d = 0.59, [95% CI, 0.48, 0.71], p < 0.001 |
| [48] | Evaluate the effects of novel immersive virtual reality technology used for serious games (Oculus Rift 2 plus leap motion controller—OR2-LMC) for upper limb outcomes. | Virtual Reality kit | Mixed methods intervention (MMI) | A mixed methods intervention study, with a qualitative design following technology intervention. | Good result in strength improvements, coordination and dexterity, and speed of participants. No side effects. |
| [49] | Implement and tests of a system for assessment and monitoring movements, which includes the sensors from Kinect and Leap Motion Controller devices | Microsoft Kinect Leap Motion Controller Kinect | Leap Motion | Using additional motion capture tools along with the virtual game environment. | A study of the feasibility and effectiveness of supplementary remedies on the results of rehabilitation of upper limb problems. Verification of further effectiveness. |
| [50] | The aim is to evaluate the Fietsgame (Dutch for cycling game), which translates existing rehabilitation exercises into fun exercise games | Control system based on Raspberry Pi Kinect v2 IoT platform | Kinect body tracking system | The study is conducted in a rehabilitation center with 9 participants, including 2 physiotherapists and 7 patients. 6 exercise games under the guidance of a physiotherapist. The mean age of the patients was 74.57 years; all the patients were in the recovery process following hip surgery. | The results showed that 75% to 100% of the patients experienced high levels of enjoyment in all the games except the squats game |
| [51] | Present a rehabilitation system based on a customizable exergame protocol to prevent falls in the elderly population | Web Camera | Self-developed body tracking platform KINOPTIM | System based on depth sensors and exergames. Measuring of physical abilities and emotional reaction | Performance of the postural response is improved by an average of 80% |
| Element | Characteristics |
|---|---|
| Desktop PC | |
| CPU | Ryzen 7 3700x, s-AM4 3.6 GHz/32 Mb |
| GPU | NVidia GeForce RTX 2070 Super, 8 Gb |
| RAM | DDR4 32 Gb 2888 GHz |
| HDD | Seagate Barracuda 1 Tb |
| Web Camera | InnJoo FHD1080p (1920 × 1080) 60 fps |
| Laptop Lenovo LEGION Y-540-IPS15i | |
| CPU | Intel(R) Core(TM) i7-9750H CPU@ 2.60 GHz |
| GPU | NVidia GeForce GTX 1660 Ti, 6 Gb |
| RAM | DDR4 16 Gb 2888 GHz |
| SSD | INTEL SSD PEKKW010T8L 1Tb |
| Web Camera | Integrated Web Camera 720p (1080 × 720) 30 fps |
| № | Gender | Age | Height | Weight | Spine or Limbs Problems | Country |
|---|---|---|---|---|---|---|
| 1 | Male | 26 | 182 | 72 | Left clavicle fracture | Ukraine |
| 2 | Female | 25 | 179 | 89 | - | Morocco |
| 3 | Male | 26 | 178 | 77 | Left arm fracture | Pakistan |
| 4 | Female | 42 | 167 | 55 | Right wrist injury | Spain |
| 5 | Male | 27 | 170 | 65 | - | Spain |
| 6 | Male | 25 | 178 | 72 | Left shoulder injury | Spain |
| 7 | Male | 31 | 173 | 78 | - | Pakistan |
| 8 | Male | 25 | 169 | 69 | - | Colombia |
| 9 | Female | 21 | 159 | 50 | Right hip fracture | Czech Republic |
| 10 | Male | 22 | 176 | 63 | - | Italy |
| Parameter | Title 2 |
|---|---|
| Left arm position | Object X. and Y.properties coordinate recording |
| Right arm position | Object X. and Y.properties coordinate recording |
| Head rotation angle | Function of coordinates transform + Vector angle calculation |
| Head position | Object X.properties coordinate recording |
| Shoulder position | Object X.properties coordinate recording |
| Hip position | Object X.properties coordinate recording |
| Body Parameter | Point 1 | Point 2 | Point 3 | Point 4 | Point 5 | Point 6 | Point 7 | Point 8 | Point 9 | Point 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| rightAngelData | −3.660 | −3.660 | −8.564 | −8.564 | −8.564 | −7.300 | −5.835 | −5.835 | −4.547 | −4.547 |
| leftAngelData | −82.022 | −82.042 | −82.006 | −81.974 | −81.974 | −82.679 | −82.825 | −82.789 | −83.523 | −83.467 |
| HeadAngelData | 179.786 | 179.780 | 179.791 | 179.784 | 179.805 | 179.794 | 179.795 | 179.789 | 179.792 | 179.785 |
| HipsData | 8.276 | 6.507 | 7.878 | 7.878 | 5.987 | 4.728 | 6.099 | 4.788 | 6.159 | 6.159 |
| HeadData | 179.788 | 179.786 | 179.780 | 179.791 | 179.784 | 179.805 | 179.794 | 179.795 | 179.789 | 179.792 |
| rangeData | 6.908 | 6.965 | 6.997 | 7.054 | 7.043 | 7.039 | 7.091 | 7.139 | 7.150 | 7.209 |
| shoulderData | −0.037 | 0.862 | −0.509 | −0.509 | 0.318 | 0.095 | −1.276 | −1.336 | −2.707 | −2.707 |
| leftMoveData | −58.095 | −58.103 | −58.103 | −58.103 | −58.128 | −58.115 | −58.115 | −58.138 | −58.138 | −58.138 |
| rightMoveData | −56.344 | −56.381 | −56.383 | −56.383 | −56.145 | −55.957 | −55.951 | −56.100 | −56.107 | −56.107 |
| averageArmLData | 60.127 | −57.823 | −58.518 | −50.405 | 6.438 | −19.626 | −49.406 | 48.971 | −53.573 | −41.703 |
| averageArmRData | 77.494 | −49.893 | −56.770 | 15.153 | −12.699 | −33.412 | 27.298 | −55.278 | 2.442 | −2.859 |
| averageHipsData | 95.968 | 4.780 | 7.458 | 8.700 | 8.086 | 8.137 | 8.336 | 6.683 | 8.547 | 8.080 |
| averageShouldersData | 47.749 | −3.716 | −0.577 | −0.610 | −0.642 | −0.603 | −1.873 | −0.038 | −2.035 | −1.135 |
| Result | Time, s | Min. Amplitude, % | Max. Amplitude, % | Frequency, Hz | Shimmer Absolute, dB | Shimmer Relative | Shimmer, % | Jitter Absolute | Jitter Relative | Jitter, % |
|---|---|---|---|---|---|---|---|---|---|---|
| LEFT HAND | ||||||||||
| Etalon | 13.01 | −68.15 | 67.52 | 0.859 | 11.78 | 0.029 | 2.886 | 0.076 | 0.064 | 5.344 |
| Bad | 9.46 | −87.34 | 77.69 | 1.025 | 25.14 | 0.318 | 31.827 | 0.414 | 0.512 | 63.168 |
| Exercise | 9.41 | −87.37 | 69.75 | 1.297 | 10.59 | 0.042 | 4.241 | 0.067 | 0.080 | 9.701 |
| InGame | 15.26 | −87.34 | 77.55 | 0.806 | 16.29 | 0.033 | 3.280 | 0.164 | 0.118 | 8.438 |
| RIGHT HAND | ||||||||||
| Etalon | 13.01 | −84.37 | 66.29 | 0.8591 | 8.69 | 0.029 | 2.940 | 0.091 | 0.076 | 6.380 |
| Bad | 9.46 | −85.22 | 76.35 | 1.025 | 25.04 | 0.373 | 37.262 | 0.389 | 0.477 | 58.548 |
| Exercise | 9.41 | −85.04 | 64.78 | 1.297 | 16.67 | 0.056 | 5.568 | 0.084 | 0.102 | 12.228 |
| InGame | 15.26 | −83.75 | 76.99 | 0.806 | 13.00 | 0.035 | 3.483 | 0.196 | 0.140 | 9.997 |
| Result | Time, s | Min. Amplitude, % | Max. Amplitude, % | Frequency, Hz | Shimmer Absolute, dB | Shimmer Relative | Shimmer, % | Jitter Absolute | Jitter Relative | Jitter, % |
|---|---|---|---|---|---|---|---|---|---|---|
| Ordinary Exercise | ||||||||||
| Etalon | 25.39 | −19.4 | 19.7 | 28.55 | 0.44 | 7.91 | 0.044 | 4.398 | 0.590 | 0.241 |
| Bad | 12.41 | −11.92 | 28.67 | 31.01 | 0.82 | 13.54 | 0.198 | 19.77 | 0.229 | 0.201 |
| Try 1 | 11.24 | −19.04 | 11.15 | 24.75 | 0.91 | 10.76 | 0.120 | 12 | 0.158 | 0.140 |
| Try 2 | 10.94 | −9.46 | 22.86 | 29.12 | 0.93 | 7.91 | 0.057 | 5.731 | 0.142 | 0.130 |
| Try 3 | 10.61 | −15.16 | 18.98 | 27.66 | 0.96 | 10.38 | 0.112 | 11.241 | 0.108 | 0.096 |
| Try 4 | 10.54 | −12.28 | 17.88 | 26.72 | 1.06 | 4.94 | 0.055 | 5.498 | 0.100 | 0.095 |
| Try 5 | 10.44 | −10.96 | 20.92 | 28.09 | 0.98 | 11.04 | 0.090 | 8.955 | 0.082 | 0.083 |
| Try 6 | 9.18 | −13.81 | 17.58 | 26.824 | 1.12 | 7.82 | 0.092 | 9.233 | 0.128 | 0.139 |
| In-Game Exercise | ||||||||||
| Etalon | 19.27 | −37.20 | 41.82 | 70.35 | 0.31 | 15.41 | 0.084 | 8.422 | 0.508 | 0.155 |
| Bad | 29.79 | −38.53 | 38.27 | 63.08 | 0.28 | 17.85 | 0.178 | 17.770 | 2.758 | 0.484 |
| Try 1 | 28.00 | −45.05 | 58.12 | 80.16 | 0.21 | 19.83 | 0.136 | 13.585 | 0.330 | 0.077 |
| Try 2 | 25.69 | −45.06 | 46.28 | 76.19 | 0.23 | 13.40 | 0.092 | 9.168 | 0.223 | 0.050 |
| Try 3 | 25.72 | −39.05 | 49.01 | 83.95 | 0.19 | 18.02 | 0.182 | 18.24 | 0.545 | 0.127 |
| Try 4 | 23.17 | −42.46 | 44.82 | 70.47 | 0.3 | 21.70 | 0.196 | 19.573 | 0.368 | 0.105 |
| Try 5 | 22.88 | −43.91 | 46.9 | 74.81 | 0.26 | 21.39 | 0.162 | 16.153 | 0.952 | 0.254 |
| Try 6 | 22.09 | −22.68 | 26.4935 | 43.81 | 0.23 | 15.76 | 0.153 | 15.327 | 0.778 | 0.187 |
| Result | Time Standard, s | Time Standard Error, % | Time In-Game, s | Time In-Game Error, % | Percentage of Standard Accuracy, % | Percentage of In-Game Accuracy, % |
|---|---|---|---|---|---|---|
| Etalon | 25.39 | 0 | 19.27 | 0 | 100 | 100 |
| Try 1 | 11.24 | 55.73 | 29.79 | 45.30 | 44.27 | 54.70 |
| Try 2 | 10.94 | 56.91 | 28 | 33.32 | 43.09 | 66.68 |
| Try 3 | 10.61 | 58.21 | 25.69 | 33.47 | 41.79 | 66.53 |
| Try 4 | 10.54 | 58.49 | 25.72 | 20.24 | 41.51 | 79.76 |
| Try 5 | 10.44 | 58.88 | 23.17 | 18.73 | 41.12 | 81.27 |
| Try 6 | 9.18 | 63.84 | 22.88 | 14.63 | 36.16 | 85.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shapoval, S.; García Zapirain, B.; Mendez Zorrilla, A.; Mugueta-Aguinaga, I. Biofeedback Applied to Interactive Serious Games to Monitor Frailty in an Elderly Population. Appl. Sci. 2021, 11, 3502. https://doi.org/10.3390/app11083502
Shapoval S, García Zapirain B, Mendez Zorrilla A, Mugueta-Aguinaga I. Biofeedback Applied to Interactive Serious Games to Monitor Frailty in an Elderly Population. Applied Sciences. 2021; 11(8):3502. https://doi.org/10.3390/app11083502
Chicago/Turabian StyleShapoval, Serhii, Begoña García Zapirain, Amaia Mendez Zorrilla, and Iranzu Mugueta-Aguinaga. 2021. "Biofeedback Applied to Interactive Serious Games to Monitor Frailty in an Elderly Population" Applied Sciences 11, no. 8: 3502. https://doi.org/10.3390/app11083502