
Low Radiation Dose Implications in Obese Abdominal Computed Tomography Imaging

 , , , ,
, , , ,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
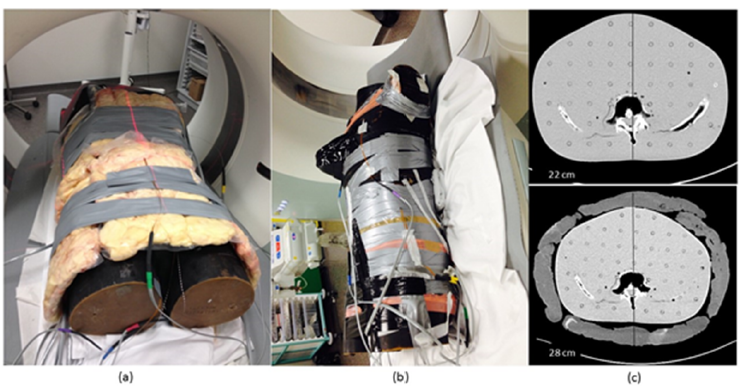
2.1. Phantom Preparation
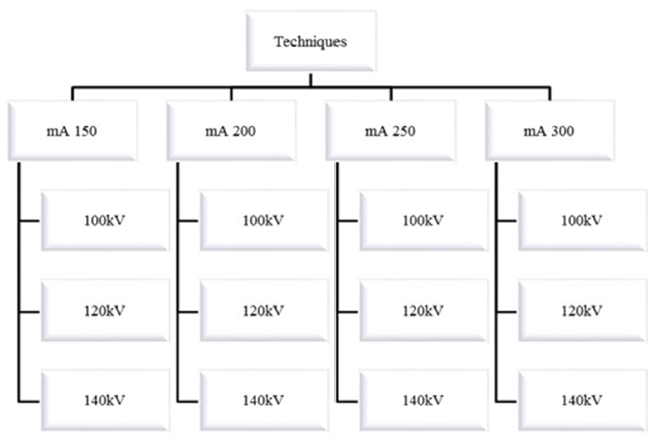
2.2. Scanning Protocol
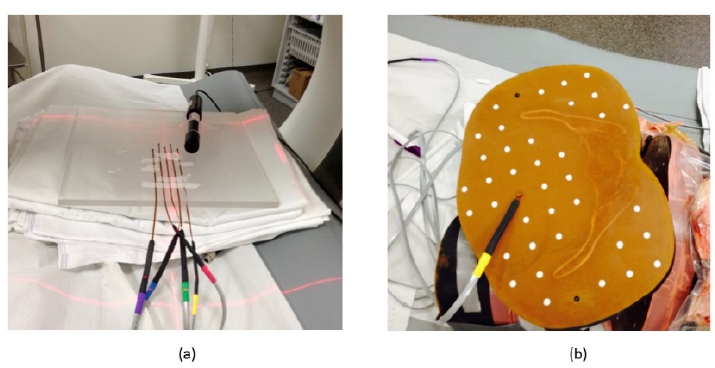
2.3. Dosimetry
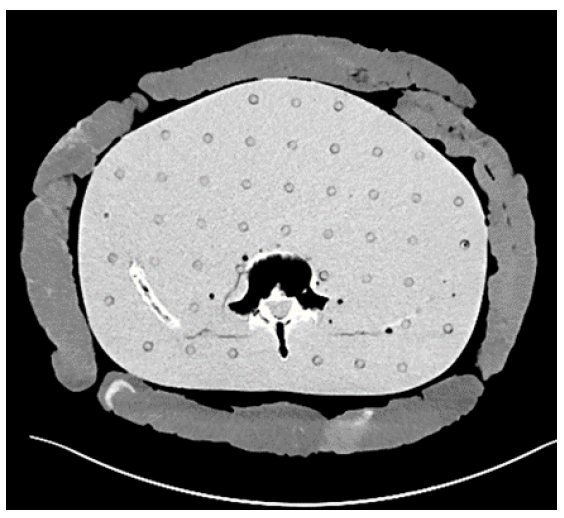
2.4. Objective Analysis of CT Image Quality
2.5. Statistical Analysis
3. Results
3.1. Radiation Dose
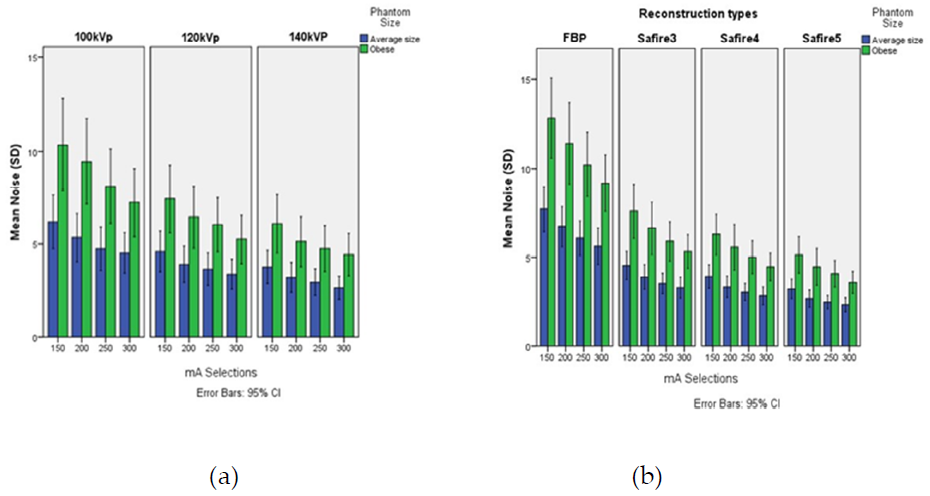
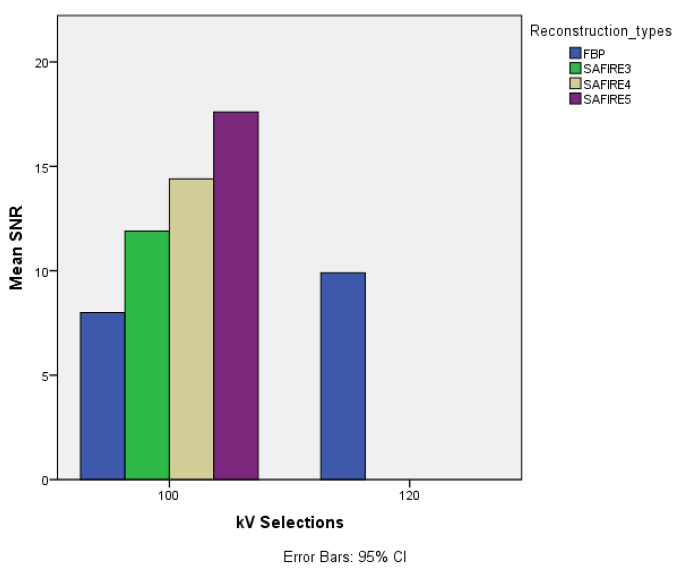
3.2. CT Objective Image Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sulieman, A.; Adam, H.; Elnour, A.; Tamam, N.; Alhaili, A.; Alkhorayef, M.; Alghamdi, S.; Khandaker, M.U.; Bradley, D.A. Patient radiation dose reduction using a commercial iterative reconstruction technique package. Radiat. Phys. Chem. 2021, 178, 108996. [Google Scholar] [CrossRef]
- Schindera, S.T.; Nelson, R.C.; Lee, E.R.; Delong, D.M.; Ngyen, G.; Toncheva, G.; Yoshizumi, T.T. Abdominal Multislice CT for Obese Patients: Effect on Image Quality and Radiation Dose in a Phantom Study. Acad. Radiol. 2007, 14, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Konkol, M.; Sniatała, K.; Sniatała, P.; Wilk, S.; Baczynska, B.; Milecki, P. Computer Tools to Analyze Lung CT Changes after Radiotherapy. Appl. Sci. 2021, 11, 1582. [Google Scholar] [CrossRef]
- Manabe, K.; Asami, Y.; Yamada, T.; Sugimori, H. Improvement in the Convolutional Neural Network for Computed Tomography Images. Appl. Sci. 2021, 11, 1505. [Google Scholar] [CrossRef]
- Bamberg, F.; Marcus, R.; Petersilka, M.; Nikolaou, K.; Becker, C.; Reiser, M.; Johnson, T. Challenges for computed tomography of overweight patients. Der Radiol. 2011, 51, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Desai, G.S.; Uppot, R.N.; Elaine, W.Y.; Kambadakone, A.R.; Sahani, D.V. Impact of iterative reconstruction on image quality and radiation dose in multidetector CT of large body size adults. Eur. Radiol. 2012, 22, 1631–1640. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M. Radiation dose issues in multi-slice CT scanning. ImPACT Technol. Update 2005, 3, 1–4. [Google Scholar]
- Zarb, F.; Mcentee, M.F.; Rainford, L. CT radiation dose and image quality optimization using a porcine model. Radiol. Technol. 2013, 85, 127–136. [Google Scholar] [PubMed]
- Higaki, T.; Nakamura, Y.; Fukumoto, W.; Honda, Y.; Tatsugami, F.; Awai, K. Clinical application of radiation dose reduction at abdominal CT. Eur. J. Radiol. 2019, 111, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Forbrig, R.; Ingrisch, M.; Stahl, R.; Winter, K.S.; Reiser, M.; Trumm, C.G. Radiation dose and image quality of high-pitch emergency abdominal CT in obese patients using third-generation dual-source CT (DSCT). Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Maurovich-Horvat, P.; Massaro, J.; Fox, C.S.; Moselewski, F.; O’Donnell, C.J.; Hoffmann, U. Comparison of anthropometric, area- and volume-based assessment of abdominal subcutaneous and visceral adipose tissue volumes using multi-detector computed tomography. Int. J. Obes. 2007, 31, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Mccollough, C.; Edyvean, S.; Cody, D.; Geise, R.; Gould, B. AAPM Report No. 96: The Measurement, Reporting, and Management of Radiation dose in CT—Report of AAPM Task Group 23 of the Diagnostic Imaging Council CT Committee. American Association of Physicists in Medicine Website. 2008. Available online: http://www.aapm.org/pubs/reports/RPT96.pdf (accessed on 25 January 2021).
- Qurashi, A.; Rainford, L.; Ajlan, A.; Khashoggi, K.; Ashkar, L.; AL-Raddadi, M.; AL-Ghamdi, M.; AL-Thobaiti, M.; Foley, S. Optimal abdominal CT protocol for obese patients. Radiography 2018, 24, e1–e12. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.S.; Singh, I.R.R.; Sharma, S.; Ravindran, B.P. Performance characteristics of mobile MOSFET dosimeter for kilovoltage X-rays used in image guided radiotherapy. J. Med. Phys. 2015, 40, 123–128. [Google Scholar]
- ICRP 2007. The 2007 Recommendations of the International Commission on Radiological Protection. Ann. ICRP 2007, 37, 1–332. [Google Scholar]
- ICRP 2012. ICRP Statement on Tissue Reactions/Early and Late Effects of Radiation in Normal Tissues and Organs—Threshold Doses for Tissue Reactions in a Radiation Protection Context. Ann. ICRP 2012, 41, 1–322. [Google Scholar] [CrossRef] [PubMed]
- Huda, W.; Ogden, K.M.; Khorasani, M.R. Converting Dose-Length Product to Effective Dose at CT. Radiology 2008, 248, 995–1003. [Google Scholar] [CrossRef]
- Wang, R.; Schoepf, U.J.; Wu, R.; Reddy, R.P.; Zhang, C.; Yu, W.; Liu, Y.; Zhang, Z. Image quality and radiation dose of low dose coronary CT angiography in obese patients: Sinogram affirmed iterative reconstruction versus filtered back projection. Eur. J. Radiol. 2012, 81, 3141–3145. [Google Scholar] [CrossRef]
- Sulieman, A.; Adam, H.; Mahmoud, M.Z.; Hamid, O.; Alkhorayef, M.; Bradley, D. Radiogenic risk assessment for abdominal vascular computed tomography angiography. Radiat. Phys. Chem. 2020, 168, 1–5. [Google Scholar] [CrossRef]
- Uppot, R.N.; Sahani, D.V.; Hahn, P.F.; Gervais, D.; Mueller, P.R. Impact of obesity on medical imaging and image-guided intervention. Am. J. Roentgenol. 2007, 188, 433–440. [Google Scholar] [CrossRef]
- Ding, A.; Mille, M.M.; Liu, T.; Caracappa, P.F.; Xu, X.G. Extension of RPI-adult male and female computational phantoms to obese patients and a Monte Carlo study of the effect on CT imaging dose. Phys. Med. Biol. 2012, 57, 2441–2459. [Google Scholar] [CrossRef] [Green Version]
- Marin, D.; Nelson, R.C.; Schindera, S.T.; Richard, S.; Youngblood, R.S.; Yoshizumi, T.T.; Samei, E. Low-tube-voltage, high-tube-current multidetector abdominal CT: Improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm--initial clinical experience. Radiology 2010, 254, 145–153. [Google Scholar] [CrossRef]
- Schabel, C.; Fenchel, M.; Schmidt, B.; Flohr, T.G.; Wuerslin, C.; Thomas, C.; Korn, A.; Tsiflikas, I.; Claussen, C.D.; Heuschmid, M. Clinical evaluation and potential radiation dose reduction of the novel sinogram-affirmed iterative reconstruction technique (SAFIRE) in abdominal computed tomography angiography. Acad. Radiol. 2013, 20, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Maldjian, P.D.; Goldman, A.R. Reducing radiation dose in body CT: A primer on dose metrics and key CT technical parameters. Am. J. Roentgenol. 2013, 200, 741–747. [Google Scholar] [CrossRef]
- Gariani, J.; Martin, S.P.; Botsikas, D.; Becker, C.D.; Montet, X. Evaluating the effect of increased pitch, iterative reconstruction and dual source CT on dose reduction and image quality. Br. J. Radiol. 2018, 91, 20170443. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Ma, Y.; Lyu, J.; Yang, Y.; Yuan, W.; Song, Z. Low kVp and low concentration contrast agent with iterative reconstruction of computed tomography (CT) coronary angiography: A preliminary study. Med. Sci. Monit. 2017, 23, 5005–5010. [Google Scholar] [CrossRef] [Green Version]
- Berlin, S.C.; Weinert, D.M.; Vasavada, P.S.; Martinez-rios, C.; Parikh, R.A.; Wien, M.A.; Jordan, D.W.; Novak, R.D. Successful dose reduction using reduced tube voltage with hybrid iterative reconstruction in pediatric abdominal CT. Am. J. Roentgenol. 2015, 205, 392–393. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, A.; Köhler, T.; Proksa, R. Noise and resolution in images reconstructed with FBP and OSC algorithms for CT. Med. Phys. 2007, 34, 585–598. [Google Scholar] [CrossRef] [PubMed]
- Mckenney, S.E.; Seibert, J.A.; Lamba, R.; Boone, J.M. Methods for CT automatic exposure control protocol translation between scanner platforms. J. Am. Coll. Radiol. 2014, 11, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Sulieman, A.; Tammam, N.; Alzimami, K.; Elnour, A.M.; Babikir, E.; Alfuraih, A. Dose reduction in chest CT examination. Radiat. Prot. Dosim. 2015, 165, 185–189. [Google Scholar] [CrossRef]
- Schindera, S.T.; Nelson, R.C.; Toth, T.L.; Nguyen, G.T.; Toncheva, G.I.; Delong, D.M.; Yoshizumi, T.T. Effect of patient size on radiation dose for abdominal MDCT with automatic tube current modulation: Phantom study. AJR Am. J. Roentgenol. 2008, 190, W100–W105. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Values |
|---|---|
| Scan range | Lung bases to symphysis pubis |
| Detector Collimation (mm) | 128 × 0.6 |
| Slice thickness (mm) | 5 |
| Rotation Time (s) | 0.5 |
| Pitch | 0.6 |
| Kernel | Medium smooth |
| Window | Window width: 350, window center: 50 |
| Organs | Level of MOSFET Insertion |
|---|---|
| Red bone marrow (spine) | (T12) slice 22 |
| Lungs | (T8–T9) slice 17 |
| Breasts | (T7–T8) slice 16 |
| Transverse colon | (L3–L4) slice 28 |
| Stomach | (T12) slice 22 |
| Ovaries | (S2–S3) |
| Spleen | (T12) slice 22 |
| Kidneys | (L1–L2) slice 23 |
| Liver | (T11–T12) slice 22 |
| Bladder | (S2–S3) |
| Gonads | (S2–S3) |
| Skin | Umbilicus |
| mA | 150 | 200 | 250 | 300 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Phantom Size | Normal-Weighted | Obese | Normal-Weighted | Obese | Normal-Weighted | Obese | Normal-Weighted | Obese | |
| Organ | kVp | ||||||||
| Mid-lung | 100 120 140 | 0.67 ± 0.22 | 0.57 ± 0.12 | 0.67 ± 0.14 | 0.61 ± 0.13 | 0.98 ± 0.30 | 0.95 ± 0.23 | 0.76 ± 0.15 | 0.84 ± 0.05 |
| 0.81 ± 0.07 | 0.93 ± 0.07 | 1.01 ± 0.23 | 1.23 ± 0.42 | 1.56 ± 0.05 | 1.11 ± 0.11 | 1.48 ± 0.45 | 1.72 ± 0.04 | ||
| 1.57 ± 0.24 | 1.37 ± 0.43 | 1.55 ± 0.13 | 1.78 ± 0.13 | 2.05 ± 0.48 | 2.67 ± 0.33 | 2.29 ± 0.20 | 2.62 ± 1.02 | ||
| Spine | 100 120 140 | 9.70 ± 0.78 | 6.71 ± 0.57 | 13.13 ± 1.53 | 7.90 ± 0.44 | 16 ± 0.79 | 9.03 ± 0.92 | 20.76 ± 0.40 | 11.43 ± 0.40 |
| 17.40 ± 0.17 | 9.86 ± 0.31 | 21.70 ± 0.50 | 14.50 ± 0.43 | 26.86 ± 0.05 | 17.10 ± 0.45 | 31.73 ± 0.40 | 20.23 ± 0.40 | ||
| 23.76 ± 0.80 | 14.80 ± 0.87 | 30.63 ± 0.55 | 19.66 ± 1.06 | 37.16 ± 1.47 | 24.50 ± 0.88 | 46.20 ± 0.87 | 29.23 ± 0.85 | ||
| Stomach | 100 120 140 | 8.87 ± 1.24 | 8.15 ± 0.66 | 13.20 ± 1.11 | 9.88 ± 1.07 | 16.56 ± 1.04 | 12.40 ± 1.24 | 20.20 ± 0.79 | 14.36 ± 0.35 |
| 16.86 ± 0.55 | 12.60 ± 0.43 | 20.76 ± 1.27 | 16.43 ± 1.34 | 26.63 ± 0.45 | 20.56 ± 0.73 | 30.83 ± 1.80 | 24.43 ± 0.65 | ||
| 21.76 ± 0.15 | 17.40 ± 0.65 | 30.43 ± 1.23 | 23.96 ± 0.85 | 35.30 ± 0.78 | 30.50 ± 0.95 | 45.16 ± 1.60 | 35.90 ± 1.67 | ||
| Liver | 100 120 140 | 11.50 ± 1.3 | 8.99 ± 0.60 | 14.06 ± 0.49 | 10.63 ± 0.40 | 17.56 ± 0.96 | 15 ± 0.34 | 21.43 ± 0.40 | 16.56 ± 0.66 |
| 18.23 ± 0.98 | 13.23 ± 0.49 | 22.43 ± 0.05 | 18.53 ± 0.58 | 27.20 ± 0.60 | 24.10 ± 1.85 | 33.76 ± 2 | 26.33 ± 1.84 | ||
| 24.43 ± 2.43 | 20.30 ± 0.50 | 30.76 ± 1.02 | 27.43 ± 1.38 | 40.73 ± 0.58 | 35.36 ± 0.37 | 47.40 ± 1.63 | 41.43 ± 3.10 | ||
| Spleen | 100 120 140 | 13.50 ± 1.67 | 8.99 ± 0.10 | 16.83 ± 1.45 | 13.10 ± 0.88 | 20.76 ± 1.85 | 14.50 ± 0.50 | 24.23 ± 0.77 | 18.70 ± 1.03 |
| 21.13 ± 0.87 | 15 ± 0.40 | 26.46 ± 1.16 | 19.26 ± 0.58 | 33 ± 3.45 | 24.40 ± 0.81 | 37.73 ± 2.31 | 29.56 ± 0.37 | ||
| 28.53 ± 1.81 | 21.96 ± 2.10 | 37.53 ± 3.09 | 28.26 ± 0.57 | 43.33 ± 1.91 | 36.73 ± 1.05 | 56.20 ± 4.34 | 41 ± 0.87 | ||
| Kidney | 100 120 140 | 9.28 ± 0.58 | 7.83 ± 0.13 | 13.26 ± 0.97 | 11 ± 0.26 | 16.13 ± 0.37 | 13.10 ± 0.36 | 19.96 ± 1.41 | 16.26 ± 0.37 |
| 16.26 ± 0.41 | 13.43 ± 0.20 | 23.10 ± 1.30 | 17.46 ± 0.55 | 25.96 ± 1 | 22.50 ± 0.60 | 31.10 ± 0.55 | 26.16 ± 1.76 | ||
| 23.20 ± 1.03 | 19.53 ± 1.10 | 31.90 ± 1.31 | 26.06 ± 0.85 | 38.76 ± 2.04 | 32.53 ± 0.61 | 46.43 ± 1.55 | 37.70 ± 1.20 | ||
| Colon | 100 120 140 | 10.83 ± 0.23 | 9.37 ± 0.89 | 14.50 ± 0.34 | 11.83 ± 0.25 | 17.96 ± 0.95 | 14.70 ± 0.55 | 20.53 ± 1.28 | 16.76 ± 0.75 |
| 19.43 ± 0.56 | 13.86 ± 0.05 | 23.23 ± 0.70 | 19.56 ± 0.92 | 29.06 ± 1.10 | 24.46 ± 0.37 | 35.76 ± 1.55 | 28.60 ± 1.99 | ||
| 24.63 ± 1.15 | 21.60 ± 0.62 | 33.23 ± 0.98 | 27.56 ± 0.58 | 41.90 ± 1.55 | 34.93 ± 1.45 | 47.83 ± 2.53 | 42.26 ± 1.02 | ||
| Ovary | 100 120 140 | 6.17 ± 0.18 | 4.71 ± 0.42 | 7.75 ± 0.10 | 6.47 ± 0.10 | 10.06 ± 0.76 | 8.42 ± 0.73 | 12.23 ± 0.55 | 9.58 ± 0.40 |
| 10.49 ± 0.60 | 8.25 ± 0.18 | 12.73 ± 0.75 | 10.90 ± 0.88 | 17.93 ± 1.06 | 13.66 ± 0.95 | 21.96 ± 1.13 | 15.13 ± 0.60 | ||
| 15.53 ± 1.30 | 12.43 ± 0.56 | 19.66 ± 0.32 | 15.80 ± 1.32 | 24.93 ± 0.15 | 20.23 ± 0.66 | 29 ± 1.99 | 23.10 ± 1.31 | ||
| Heart | 100 120 140 | 6.27 ± 0.30 | 4.71 ± 0.13 | 6.51 ± 0.51 | 6.59 ± 0.30 | 8.26 ± 0.73 | 7.97 ± 0.33 | 10.35 ± 1.16 | 10.76 ±0.25 |
| 10.76 ± 1.19 | 8.56 ± 0.62 | 10.51 ± 0.86 | 10.56 ± 0.49 | 13.23 ± 0.41 | 13.66 ± 1.45 | 15.66 ± 0.65 | 16.33 ± 1.30 | ||
| 10.83 ± 0.25 | 13.06 ± 0.80 | 15.06 ± 0.95 | 15.80 ± 0.60 | 19.56 ± 0.64 | 20.60 ± 1.76 | 23.16 ± 0.73 | 25.26 ± 1.50 | ||
| Female Breast | 100 120 140 | 0.21 ± 0.11 | 0.53 ± 0.05 | 0.59 ± 0.24 | 0.48 ± 0.24 | 0.67 ± 0.37 | 0.71 ± 0.20 | 0.70 ± 0.26 | 0.70 ± 0.15 |
| 0.37 ± 0.30 | 0.93 ± 0.16 | 0.92 ± 0.37 | 0.68 ± 0.18 | 0.98 ± 0.22 | 1.17 ± 0.27 | 0.95 ± 0.23 | 1.27 ± 0.20 | ||
| 1.35 ± 0.18 | 0.76 ± 0.33 | 1.08 ± 0.07 | 1.28 ± 0.33 | 1.59 ± 0.32 | 1.46 ± 0.36 | 1.78 ± 0.27 | 1.72 ± 0.44 | ||
| Skin Anterior | 100 120 140 | 8.91 ± 1.51 | 7.63 ± 1.18 | 10.53 ± 1.69 | 10.03 ± 1.33 | 15.20 ± 1.49 | 10.96 ± 0.25 | 17.56 ± 2.82 | 16.46 ± 0.77 |
| 15.36 ± 1.55 | 12.93 ± 0.75 | 17.43 ± 2.45 | 13.93 ± 1.04 | 23 ± 2.68 | 17.90 ± 2.55 | 27.66 ± 1.25 | 21.70 ± 2.69 | ||
| 18.93 ± 1.70 | 16.10 ± 2.88 | 26.73 ± 2.31 | 22.16 ± 1.68 | 33 ± 3.37 | 28.43 ± 4.31 | 36.10 ± 3.36 | 30.10 ± 3.98 | ||
| Skin Posterior | 100 120 140 | 7.21 ± 0.64 | 6.39 ± 1.01 | 10.03 ± 0.05 | 8.43 ± 0.49 | 11.80 ± 0.55 | 9.91 ± 0.79 | 15.36 ± 1.70 | 11.86 ± 0.64 |
| 12 ± 1.30 | 10.93 ± 0.15 | 16.26 ± 1.55 | 16.50 ± 0.79 | 18.76 ±1.41 | 17.16 ± 1.42 | 23.56 ± 2.54 | 22.40 ± 1 | ||
| 16.16 ± 1.43 | 15.86 ± 1.45 | 20.60 ± 1.44 | 19.66 ± 1.06 | 27.20 ± 0.60 | 25 ± 2.89 | 34.30 ± 1.60 | 31.40 ± 3.20 | ||
| Gonads (Male) | 100 120 140 | 0.80 ± 0.29 | 1.37 ± 0.24 | 1.18 ± 0.06 | 1.60 ± 0.50 | 1.32 ± 0.24 | 1.99 ± 0.11 | 1.75 ± 0.27 | 2.34 ± 0.22 |
| 1.65 ± 0.14 | 2.28 ± 0.37 | 1.99 ± 0.36 | 3.38 ± 0.57 | 2.59 ± 0.42 | 3.97 ± 0.17 | 2.89 ± 0.20 | 3.95 ± 1.66 | ||
| 2.20 ± 0.40 | 3.46 ± 0.44 | 2.87 ± 0.30 | 4.51 ± 0.24 | 3.99 ± 0.47 | 5.43 ± 0.46 | 4.82 ± 0.70 | 6.46 ± 0.34 | ||
| Protocol | Phantom Size | Effective Dose (mSv) | DLP (mGy·cm) | CTDIvol (mGy) |
|---|---|---|---|---|
| 150 mA, 100 kVp | Normal weight | 8.63 | 218.67 | 5.91 |
| Obese | 6.89 | |||
| 150 mA, 120 kVp | Normal weight | 14.90 | 376.66 | 10.18 |
| Obese | 11.11 | |||
| 150 mA, 140 kVp | Normal weight | 19.88 | 571.28 | 15.44 |
| Obese | 16.39 | |||
| 200 mA, 100 kVp | Normal weight | 11.37 | 291.93 | 7.89 |
| Obese | 9.03 | |||
| 200 mA, 120 kVp | Normal weight | 18.47 | 497.28 | 13.44 |
| Obese | 14.80 | |||
| 200 mA, 140 kVp | Normal weight | 26.39 | 761.83 | 20.59 |
| Obese | 21.43 | |||
| 250 mA, 100 kVp | Normal weight | 14.13 | 363.34 | 9.82 |
| Obese | 10.98 | |||
| 250 mA, 120 kVp | Normal-weighted | 23.02 | 621.97 | 16.81 |
| Obese | 18.55 | |||
| 250 mA, 140 kVp | Normal weight | 32.31 | 949.05 | 25.65 |
| Obese | 27.28 | |||
| 300 mA, 100 kVp | Normal weight | 17.09 | 436.60 | 11.80 |
| Obese | 13.25 | |||
| 300 mA, 120 kVp | Normal weight | 27.29 | 746.66 | 20.18 |
| Obese | 21.76 | |||
| 300 mA, 140 kVp | Normal weight | 39.25 | 1139.60 | 30.80 |
| Obese | 31.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qurashi, A.A.; Rainford, L.A.; Alhazmi, F.H.; Alshamrani, K.M.; Sulieman, A.; Alsharif, W.M.; Alshoabi, S.A.; Gameraddin, M.B.; Aloufi, K.M.; Aldahery, S.T.; et al. Low Radiation Dose Implications in Obese Abdominal Computed Tomography Imaging. Appl. Sci. 2021, 11, 2456. https://doi.org/10.3390/app11062456
Qurashi AA, Rainford LA, Alhazmi FH, Alshamrani KM, Sulieman A, Alsharif WM, Alshoabi SA, Gameraddin MB, Aloufi KM, Aldahery ST, et al. Low Radiation Dose Implications in Obese Abdominal Computed Tomography Imaging. Applied Sciences. 2021; 11(6):2456. https://doi.org/10.3390/app11062456
Chicago/Turabian StyleQurashi, Abdulaziz A., Louise A. Rainford, Fahad H. Alhazmi, Khalid M. Alshamrani, Abdelmoneim Sulieman, Walaa M. Alsharif, Sultan A. Alshoabi, Moawia B. Gameraddin, Khalid M. Aloufi, Shrooq T. Aldahery, and et al. 2021. "Low Radiation Dose Implications in Obese Abdominal Computed Tomography Imaging" Applied Sciences 11, no. 6: 2456. https://doi.org/10.3390/app11062456