
Effect of Real-Time Online High-Intensity Interval Training on Physiological and Physical Parameters for Abdominally Obese Women: A Randomized Pilot Study


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Subject
2.3. Intervention
- (1)
- HIIT
- (2)
- MICT
2.4. Study Measures and Methods
- (1)
- Body composition test
- (2)
- Abdominal obesity
- (3)
- Blood test
- (4)
- Muscle strength test
- (5)
- Stress Index test
2.5. Data Processing
3. Results
3.1. Changes of Body Composition According to Exercise Intensity
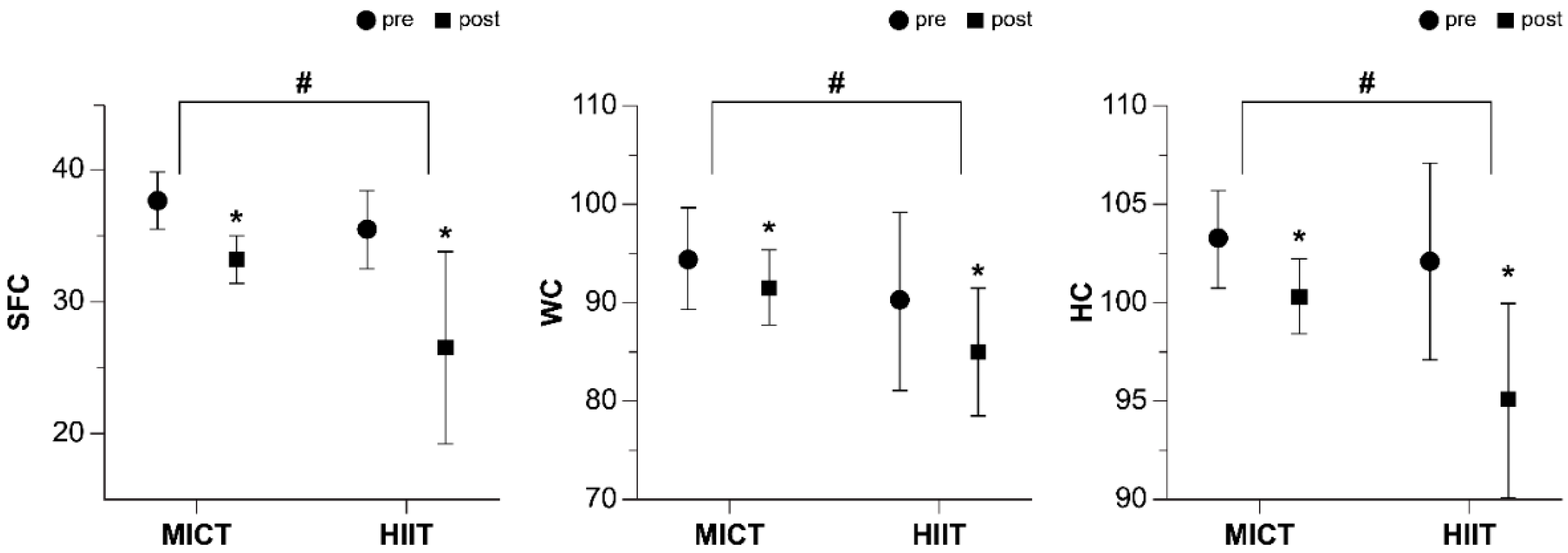
3.2. Changes of Abdominal Fat According to Exercise Intensity
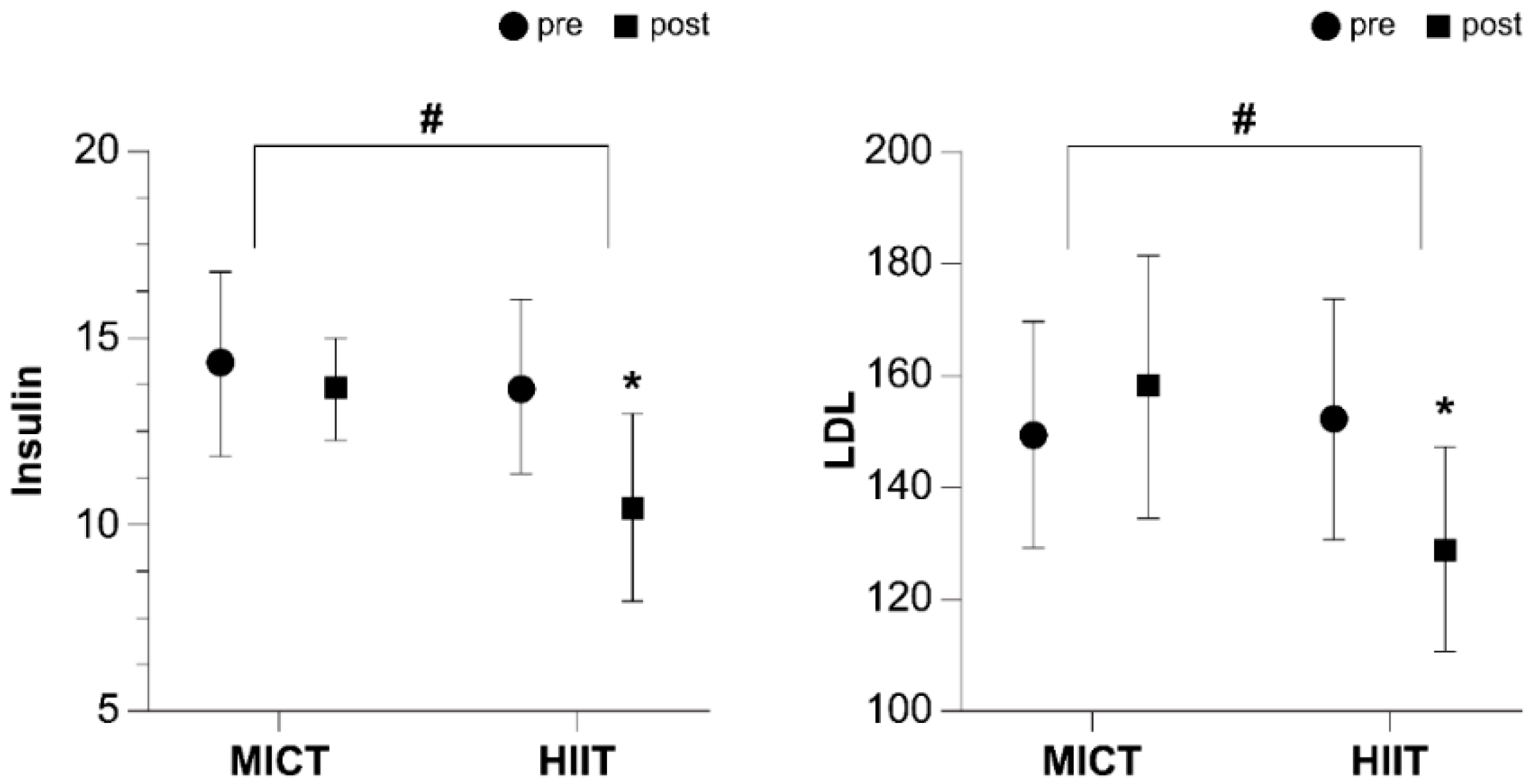
3.3. Changes of Blood Glucose and Lipid Profile According to Exercise Intensity
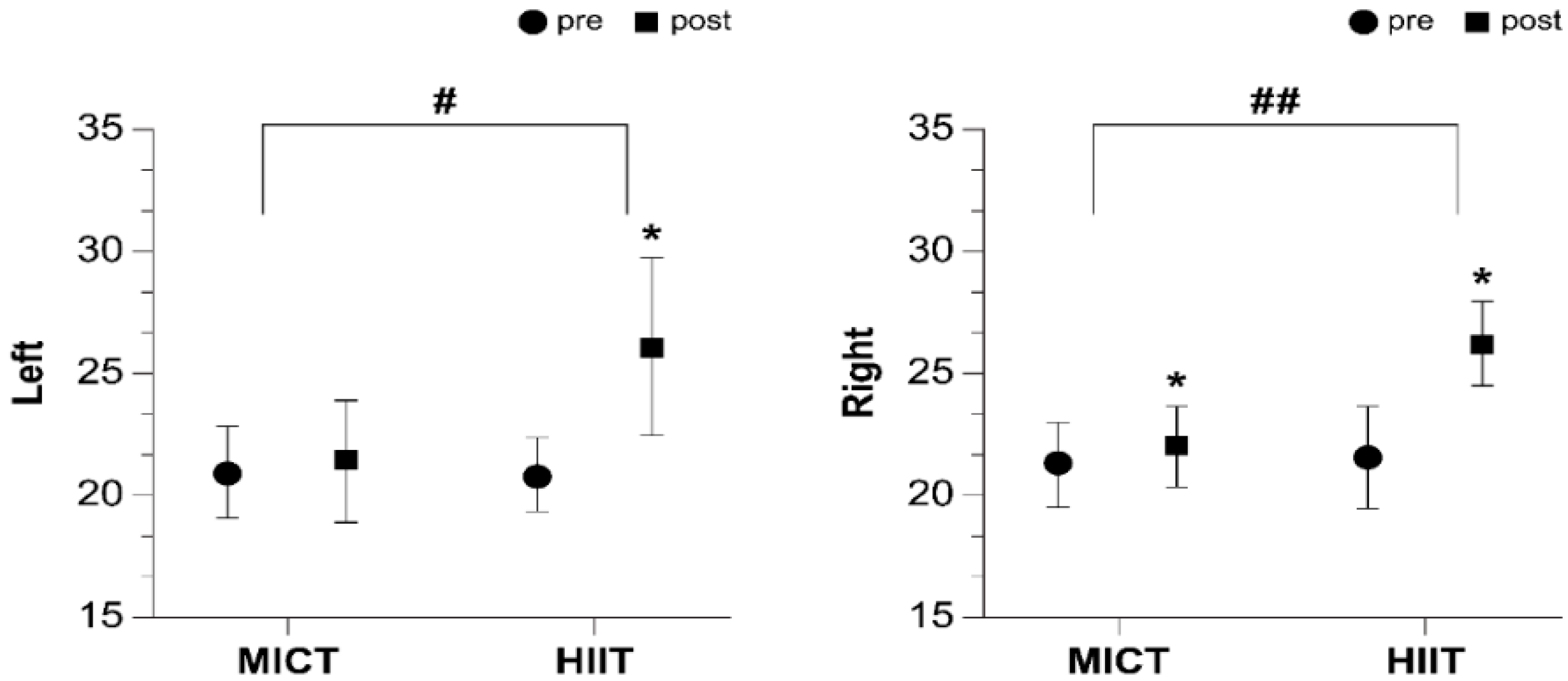
3.4. Changes of Muscle Strength According to Exercise Intensity
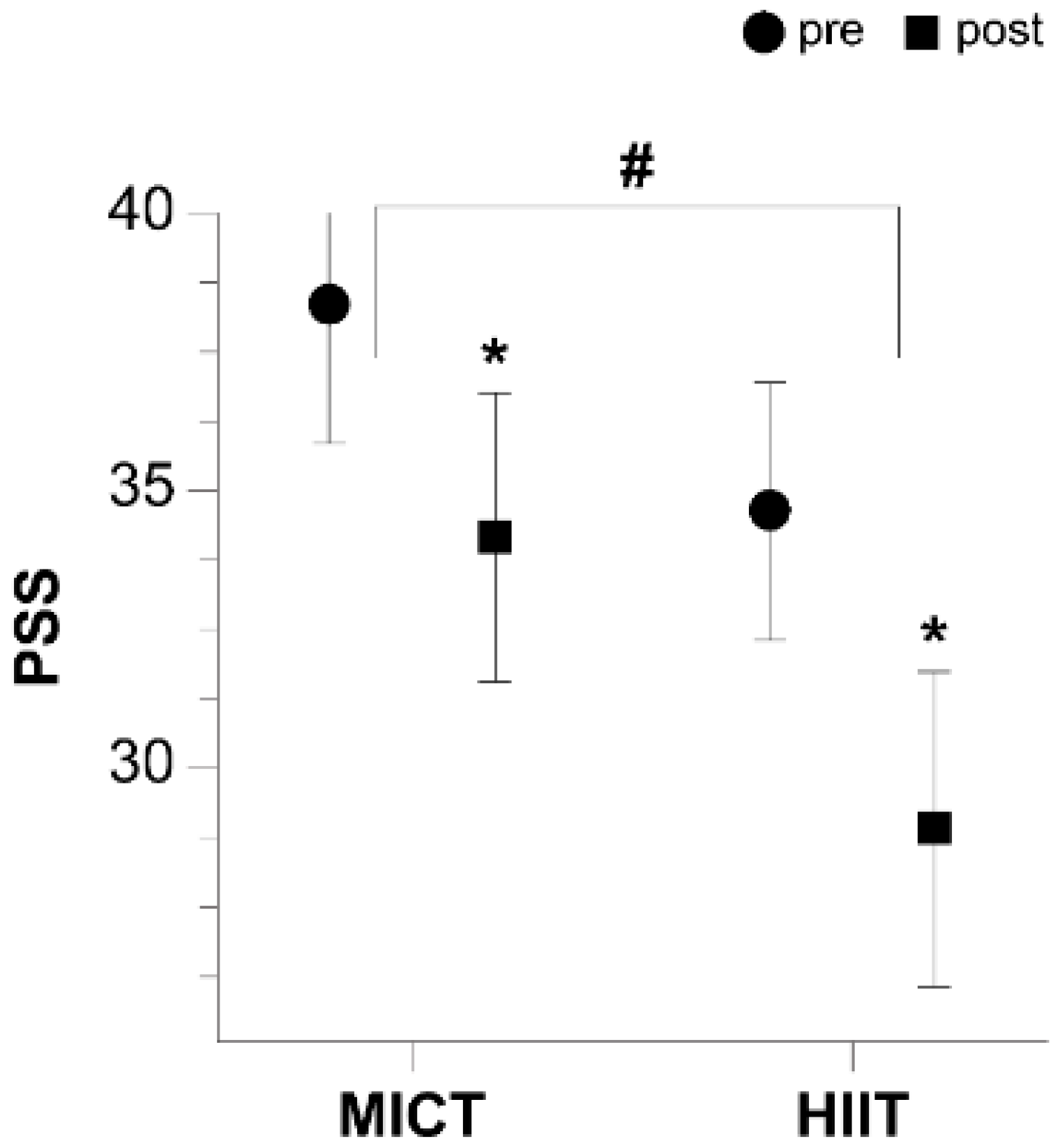
3.5. Changes of Stress According to Exercise Intensity
4. Discussion
4.1. Effects of Online HIIT on Body Composition and Abdominal Obesity
4.2. Effects of Online HIIT on Blood Glucose and Lipid Profile
4.3. Effects of Online HIIT on Muscle Strength
4.4. Effects of Online HIIT on Stress
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Mead, B.R.; Noonan, R.; Hardman, C.A. Obesity, eating behavior and physical activity during COVID-19 lockdown: A study of UK adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Ghram, A.; Briki, W.; Mansoor, H.; Al-Mohannadi, A.S.; Lavie, C.J.; Chamari, K. Home-based exercise can be beneficial for counteracting sedentary behavior and physical inactivity during the COVID-19 pandemic in older adults. Postgrad. Med. 2021, 133, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Halpern, B.; Louzada, M.L.D.C.; Aschner, P.; Gerchman, F.; Brajkovich, I.; Faria-Neto, J.R.; Polanco, F.E.; Montero, J.; Juliá, S.M.M.; Lotufo, P.A.; et al. Obesity and COVID-19 in Latin America: A tragedy of two pandemics—Official document of the Latin American Federation of Obesity Societies. Obes. Rev. 2021, 22, 13165. [Google Scholar] [CrossRef]
- Lockhart, S.M.; O’Rahilly, S. When Two Pandemics Meet: Why Is Obesity Associated with Increased COVID-19 Mortality? Med 2020, 1, 33–42. [Google Scholar] [CrossRef]
- Barranco-Ruiz, Y.; Villa-González, E. Health-Related Physical Fitness Benefits in Sedentary Women Employees after an Exercise Intervention with Zumba Fitness®. Int. J. Environ. Res. Public Health 2020, 17, 2632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delfino, L.D.; Tebar, W.; Gil Tebar, F.C.S.; De Souza, J.M.; Romanzini, M.; Fernandes, R.A.; Christofaro, D.G.D. Association between sedentary behavior, obesity and hypertension in public school teachers. Ind. Health 2020, 58, 345–353. [Google Scholar] [CrossRef] [Green Version]
- National Health Insurance Service. Korea National Health Insurance Announces. 2020. Available online: https://www.nhis.or.kr/static/html/wbd/g/a/wbdga0601.html (accessed on 1 September 2020).
- Ayala, A.M.C.; Salmon, J.; Dunstan, D.W.; Arundell, L.; Timperio, A. Does light-intensity physical activity moderate the relationship between sitting time and adiposity markers in adolescents? J. Sport Health Sci. 2020. [Google Scholar] [CrossRef]
- Reljic, D.; Frenk, F.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Effects of very low volume high intensity versus moderate intensity interval training in obese metabolic syndrome patients: A randomized controlled study. Sci. Rep. 2021, 11, 2836. [Google Scholar] [CrossRef] [PubMed]
- Mauvais-Jarvis, F. Aging, Male Sex, Obesity, and Metabolic Inflammation Create the Perfect Storm for COVID-19. Diabetes 2020, 69, 1857–1863. [Google Scholar] [CrossRef]
- Jesus, I.; Vanhee, V.; Deramaudt, T.B.; Bonay, M. Promising effects of exercise on the cardiovascular, metabolic and immune system during COVID-19 period. J. Hum. Hypertens. 2021, 35, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Nunes, P.R.; Martins, F.M.; Souza, A.P.; Carneiro, M.; Orsatti, C.; Michelin, M.A.; Murta, E.F.; de Oliveira, E.; Orsatti, F. Effect of high-intensity interval training on body composition and inflammatory markers in obese postmenopausal women: A randomized controlled trial. Menopause 2019, 26, 256–264. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 Public Health Emergency of International Concern (PHEIC) Global Research and Innovation Forum: Towards a Research Roadmap. 2020. Available online: https://covid19-evidence.paho.org/handle/20.500.12663/714 (accessed on 1 December 2021).
- Hyun, A.-H.; Cho, J.-Y. Effects of 12-weeks pilates mat exercise on body composition, delivery confidence, and neck disability index in pregnant women. Sports Sci. 2019, 36, 43–55. [Google Scholar] [CrossRef]
- Oh, S.; So, R.; Shida, T.; Matsuo, T.; Kim, B.; Akiyama, K.; Isobe, T.; Okamoto, Y.; Tanaka, K.; Shoda, J. High-Intensity Aerobic Exercise Improves Both Hepatic Fat Content and Stiffness in Sedentary Obese Men with Nonalcoholic Fatty Liver Disease. Sci. Rep. 2017, 7, 43029. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.X.; Gao, F.Q.; Wang, Y.T.; Li, Z.R.; Koji, O.; Sun, W. Relationship between body weight and spinopelvic alignment in Chinese adult people: A preliminary study. Eur. PMC 2020, 9, 149027. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Baker, J.S.; Quan, W.; Shen, S.; Fekete, G.; Gu, Y. A Preventive Role of Exercise Across the Coronavirus 2 (SARS-CoV-2) Pandemic. Front. Physiol. 2020, 11, 572718. [Google Scholar] [CrossRef]
- Thompson, W.R. Worldwide survey of fitness trends for 2020. ACSM’s Health Fit. J. 2019, 36, 10–18. [Google Scholar] [CrossRef]
- Franklin, B.A.; Thompson, P.D.; Al-Zaiti, S.S.; Albert, C.M.; Hivert, M.-F.; Levine, B.D.; Lobelo, F.; Madan, K.; Sharrief, A.Z.; Eijsvogels, T.M.; et al. Exercise-Related Acute Cardiovascular Events and Potential Deleterious Adaptations Following Long-Term Exercise Training: Placing the Risks into Perspective–An Update: A Scientific Statement from the American Heart Association. Circulation 2020, 141, e705–e736. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Frenk, F.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Low-volume high-intensity interval training improves cardiometabolic health, work ability and well-being in severely obese individuals: A randomized-controlled trial sub-study. J. Transl. Med. 2020, 18, 419. [Google Scholar] [CrossRef]
- Leal, J.M.; Galliano, L.M.; Del Vecchio, F.B. Effectiveness of High-Intensity Interval Training Versus Moderate-Intensity Continuous Training in Hypertensive Patients: A Systematic Review and Meta-Analysis. Curr. Hypertens. Rep. 2020, 22, 26. [Google Scholar] [CrossRef]
- Way, K.L.; Sabag, A.; Sultana, R.N.; Baker, M.K.; Keating, S.E.; Lanting, S.; Gerofi, J.; Chuter, V.H.; Caterson, I.D.; Twigg, S.M.; et al. The effect of low-volume high-intensity interval training on cardiovascular health outcomes in type 2 diabetes: A randomised controlled trial. Int. J. Cardiol. 2020, 320, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Miroshnikov, A.B.; Smolensky, A.V.; Formenov, A.D. High-Intensity Interval Aerobic Work for Strength Athletes with Arterial Hypertension: A Randomized Controlled Trial. Hum. Physiol. 2021, 47, 33–41. [Google Scholar] [CrossRef]
- Saghaei, M. An overview of randomization and minimization programs for randomized clinical trials. J. Med. Signals Sens. 2011, 1, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Gholizadeh, M.; BabazaKordideh, M.; Akbarnejad, A. Comparison of Two High-Intensity Interval Training (HIIT) For Two Weeks on Fat Oxidation, Body Fat Percentage and VO2max in Overweight Young Males. J. Educ. Community Health 2017, 3, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Hortmann, K.; Boutouyrie, P.; Locatelli, J.C.; de Oliveira, G.H.; Simões, C.F.; Mendes, V.H.D.S.; Reck, H.B.; Okawa, R.T.; Lopes, W.A. Acute effects of high-intensity interval training and moderate-intensity continuous training on arterial stiffness in young obese women. Eur. J. Prev. Cardiol. 2020, 28, e7–e10. [Google Scholar] [CrossRef]
- Lee, J.; Shin, C.; Ko, Y.H.; Lim, J.; Joe, S.H.; Kim, S.; Han, C. The reliability and validity studies of the Korean version of the Perceived Stress Scale. Korean J. Psychosom. Med. 2017, 20, 127–134. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- Borrega-Mouquinho, Y.; Sánchez-Gómez, J.; Fuentes-García, J.P.; Collado-Mateo, D.; Villafaina, S. Effects of High-Intensity Interval Training and Moderate-Intensity Training on Stress, Depression, Anxiety, and Resilience in Healthy Adults During Coronavirus Disease 2019 Confinement: A Randomized Controlled Trial. Front. Psychol. 2021, 12, 643069. [Google Scholar] [CrossRef]
- McDaniel, B.B.; Naquin, M.R.; Sirikul, B.; Kraemer, R.R. Five Weeks of Aquatic-Calisthenic High Intensity Interval Training Improves Cardiorespiratory Fitness and Body Composition in Sedentary Young Adults. J. Sports Sci. Med. 2020, 19, 187–194. [Google Scholar]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Physical Activity Recommendations for Different Age Groups. 2021. Available online: https://www.cdc.gov/physicalactivity/basics/age-chart.html (accessed on 1 December 2021).
- Blüher, S.; Käpplinger, J.; Herget, S.; Reichardt, S.; Böttcher, Y.; Grimm, A.; Kratzsch, J.; Petroff, D. Cardiometabolic risk markers, adipocyte fatty acid binding protein (aFABP) and the impact of high-intensity interval training (HIIT) in obese adolescents. Metabolism 2017, 68, 77–87. [Google Scholar] [CrossRef]
- Motiani, K.K.; Savolainen, A.M.; Toivanen, J.; Eskelinen, J.-J.; Yli-Karjanmaa, M.; Virtanen, K.A.; Saunavaara, V.; Heiskanen, M.; Parkkola, R.; Haaparanta-Solin, M.; et al. Effects of short-term sprint interval and moderate-intensity continuous training on liver fat content, lipoprotein profile, and substrate uptake: A randomized trial. J. Appl. Physiol. 2019, 126, 1756–1768. [Google Scholar] [CrossRef] [PubMed]
- Roy, M.; Williams, S.M.; Brown, R.C.; Meredith-Jones, K.A.; Osborne, H.; Jospe, M.; Taylor, R.W. High-Intensity Interval Training in the Real World: Outcomes from a 12-Month Intervention in Overweight Adults. Med. Sci. Sports Exerc. 2018, 50, 1818–1826. [Google Scholar] [CrossRef]
- Maillard, F.; Pereira, B.; Boisseau, N. Effect of High-Intensity Interval Training on Total, Abdominal and Visceral Fat Mass: A Meta-Analysis. Sports Med. 2018, 48, 269–288. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, M.A.R.; Baptista, L.C.; Neves, R.; De França, E.; Loureiro, H.; Lira, F.S.; Caperuto, E.C.; Veríssimo, M.T.; Martins, R.A. The Effects of Concurrent Training Combining Both Resistance Exercise and High-Intensity Interval Training or Moderate-Intensity Continuous Training on Metabolic Syndrome. Front. Physiol. 2020, 11, 572. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Hu, J.; Zhu, C. Obesity aggravates COVID-19: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 257–261. [Google Scholar] [CrossRef]
- Rahmati-Ahmadabad, S.; Shirvani, H.; Ghanbari-Niaki, A.; Rostamkhani, F. The effects of high-intensity interval training on reverse cholesterol transport elements: A way of cardiovascular protection against atherosclerosis. Life Sci. 2018, 209, 377–382. [Google Scholar] [CrossRef]
- Wood, G.; Murrell, A.; Van Der Touw, T.; Smart, N. HIIT is not superior to MICT in altering blood lipids: A systematic review and meta-analysis. BMJ Open Sport Exerc. Med. 2019, 5, e000647. [Google Scholar] [CrossRef] [Green Version]
- García-Pinillos, F.; Laredo-Aguilera, J.A.; Muñoz, M.; Latorre-Román, P.A. Effects of 12-Week Concurrent High-Intensity Interval Strength and Endurance Training Program on Physical Performance in Healthy Older People. J. Strength Cond. Res. 2019, 33, 1445–1452. [Google Scholar] [CrossRef]
- Werneck, A.O.; Collings, P.J.; Barboza, L.L.; Stubbs, B.; Silva, D. Associations of sedentary behaviors and physical activity with social isolation in 100,839 school students: The Brazilian Scholar Health Survey. Gen. Hosp. Psychiatry 2019, 59, 7–13. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Castro-Astudillo, K.; Correa-Bautista, J.E.; González-Ruíz, K.; Izquierdo, M.; García-Hermoso, A.; Álvarez, C.; Ramírez-Campillo, R.; Correa-Rodríguez, M. The Effect of 12 Weeks of Different Exercise Training Modalities or Nutritional Guidance on Cardiometabolic Risk Factors, Vascular Parameters, and Physical Fitness in Overweight Adults: Cardiometabolic High-Intensity Interval Training-Resistance Training Randomized Controlled Study. J. Strength Cond. Res. 2020, 34, 2178–2188. [Google Scholar] [CrossRef]
- Schwendinger, F.; Pocecco, E. Counteracting Physical Inactivity during the COVID-19 Pandemic: Evidence-Based Recommendations for Home-Based Exercise. Int. J. Environ. Res. Public Health 2020, 17, 3909. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MICT (n = 8) | HIIT (n = 8) | F | p | |
|---|---|---|---|---|
| Age (years) | 37.75 ± 2.76 | 39.12 ± 2.35 | 0.930 | 0.351 |
| Height (cm) | 164.20 ± 4.44 | 163.75 ± 5.09 | 0.520 | 0.483 |
| Weight (kg) | 66.88 ± 4.57 | 65.51 ± 4.77 | 0.263 | 0.616 |
| BMI (kg/m2) | 25.36 ± 2.33 | 25.82 ± 1.98 | 0.001 | 0.971 |
| WC (cm) | 94.50 ± 5.18 | 90.06 ± 9.01 | 2.705 | 0.122 |
| Modes | Contents | Time (min) | Set and Rest | RPE |
|---|---|---|---|---|
| Warm-up | Breathing, Static Stretching | 5 | 12 | |
| Main Exercise | HIIT exercise Level 1: 1~2 week Squat, Back lunge, Kneeing push-up tap, Side steps, Crunch, Spine twist, Burpee test Level 2: 3~4 week Lunge side kick, Down dog and push up, Squat Jump, Legs raise, Plank Level 3: 5~8 week Wall squat, Lunge-twist, Knee up runs, Push-up, 100 Breathing, Burpee jump | 20 | 85~90% HRmax 20 s, 70% HRmax 30 s X 10 Total 2 set | 15~17 |
| MICT exercise Cycle ergometer | 40 | 60~70% HRmax | 13 | |
| Cool-down | Deep breathing, Total body stretching | 5 | 12 |
| MICT (n = 8) | HIIT (n = 8) | Diff | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | z | p | Cohen’s d | |
| BW (kg) | 66.88 ± 4.57 | 65.01 ± 4.29 * | 65.51 ± 4.77 | 59.92 ± 4.68 * | −1.785 | 0.074 | 1.133 |
| BFM (kg) † | 24.92 ± 2.77 | 23.86 ± 2.50 * | 25.38 ± 4.60 | 19.86 ± 4.40 * | −2.102 | 0.036 | 1.117 |
| SMM (kg) | 22.66 ± 1.86 | 22.37 ± 1.67 | 21.58 ± 2.18 | 21.66 ± 2.07 | −1.261 | 0.210 | 0.213 |
| BMI (kg/m2) † | 25.36 ± 2.33 | 24.63 ± 2.01 * | 25.82 ± 1.98 | 22.41 ± 1.44 * | −2.312 | 0.021 | 1.269 |
| VFL † | 12.75 ± 1.83 | 11.87 ± 1.72 * | 12.12 ± 1.88 | 8.00 ± 1.85 * | −3.018 | 0.003 | 2.166 |
| PBF (%) | 37.51 ± 2.29 | 35.56 ± 2.57 * | 38.56 ± 5.00 | 34.50 ± 5.17 * | −0.579 | 0.563 | 0.259 |
| MICT (n = 8) | HIIT (n = 8) | Diff | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | z | p | Cohen’s d | |
| SFC (mm) * | 35.75 ± 2.18 | 33.25 ± 1.83 † | 35.50 ± 2.97 | 26.50 ± 7.32 † | −2.004 | 0.050 | 1.265 |
| WC (cm) * | 94.50 ± 5.18 | 91.50 ± 3.74 † | 90.06 ± 9.01 | 84.98 ± 6.51 † | −2.223 | 0.026 | 1.228 |
| HC (cm) * | 103.25 ± 2.49 | 100.25 ± 1.90 † | 102.12 ± 4.96 | 95.06 ± 4.91 † | −2.111 | 0.035 | 1.430 |
| MICT (n = 8) | HIIT (n = 8) | Diff | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | z | p | Cohen’s d | |
| Insulin * | 14.40 ± 2.44 | 13.66 ± 1.33 | 13.71 ± 2.36 | 10.48 ± 2.55 † | −2.310 | 0.021 | 1.563 |
| TC | 208.50 ± 22.36 | 203.37 ± 23.18 | 222.12 ± 25.85 | 187.75 ± 38.67 † | −1.314 | 0.189 | 0.489 |
| TG | 204.25 ± 37.91 | 195.75 ± 43.18 | 213.25 ± 42.00 | 193.25 ± 35.13 † | −0.053 | 0.958 | 0.063 |
| LDL * | 149.25 ± 20.45 | 158.00 ± 23.69 | 152.12 ± 21.77 | 128.37 ± 18.66 † | −2.260 | 0.024 | 1.389 |
| HDL | 62.12± 11.58 | 59.50 ± 10.78 * | 58.00 ± 9.25 | 66.62 ± 11.24 † | −0.790 | 0.430 | 0.646 |
| MICT (n = 8) | HIIT (n = 8) | Diff | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | z | p | Cohen’s d | |
| Left HGS * | 20.98 ± 1.90 | 21.45 ± 2.47 | 20.82 ± 1.58 | 26.10 ± 3.62 ‡ | −2.521 | 0.012 | 1.500 |
| Right HGS† | 21.22 ± 1.74 | 21.96 ± 1.65‡ | 21.48 ± 2.06 | 26.10 ± 1.77 ‡ | −3.046 | 0.002 | 2.419 |
| MICT (n = 8) | HIIT (n = 8) | Diff | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | z | p | Cohen’s d | |
| PSS * | 38.35 ± 2.44 | 34.12 ± 2.58 † | 34.62 ± 2.26 | 28.87 ± 2.85 † | −2.852 | 0.004 | 1.931 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hyun, A.-h. Effect of Real-Time Online High-Intensity Interval Training on Physiological and Physical Parameters for Abdominally Obese Women: A Randomized Pilot Study. Appl. Sci. 2021, 11, 12129. https://doi.org/10.3390/app112412129
Hyun A-h. Effect of Real-Time Online High-Intensity Interval Training on Physiological and Physical Parameters for Abdominally Obese Women: A Randomized Pilot Study. Applied Sciences. 2021; 11(24):12129. https://doi.org/10.3390/app112412129
Chicago/Turabian StyleHyun, Ah-hyun. 2021. "Effect of Real-Time Online High-Intensity Interval Training on Physiological and Physical Parameters for Abdominally Obese Women: A Randomized Pilot Study" Applied Sciences 11, no. 24: 12129. https://doi.org/10.3390/app112412129