
Analysis of Clinical Profiles, Deformities, and Plantar Pressure Patterns in Diabetic Foot Syndrome

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Protocol 1: Data Collection and Analysis
2.3. Experimental Protocol 2: Data Collection and Analysis
2.4. Data Analysis and Statistics
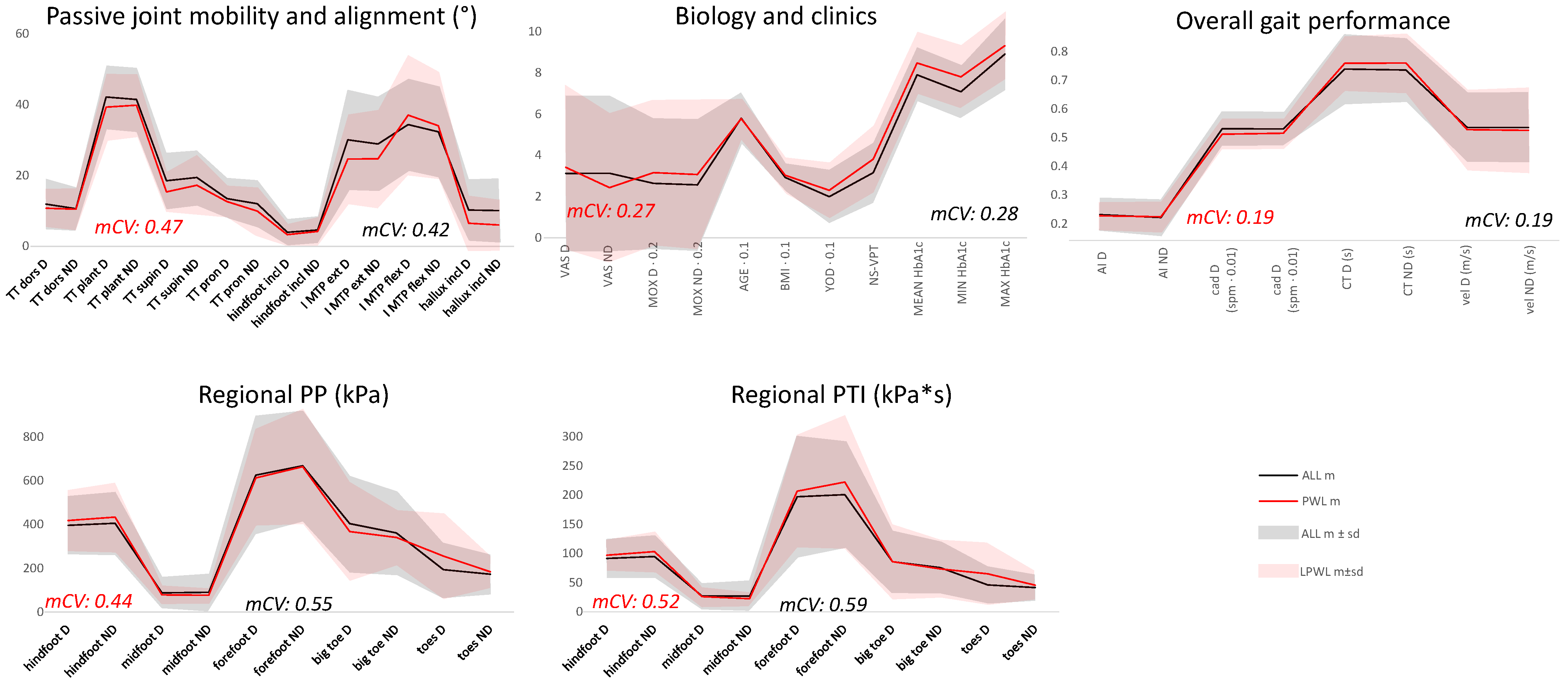
- Passive joint mobility and alignment (all measured in degrees) [15]: maximum passive ankle dorsiflexion (TT dors); maximum passive ankle plantar flexion (TT plant); maximum passive ankle inversion (TT supin); maximum passive ankle eversion (TT pron); maximum passive first metatarsophalangeal joint extension (I MTP ext); maximum passive first metatarsophalangeal joint flexion (I MTP flex); hindfoot inclination in the frontal plane (hindfoot incl); hallux inclination in the transverse plane (hallux incl);
- Biology and clinics: age (years); body mass index (BMI, kg/m2); years of disease (YOD, years); combined neuropathy score (NS-VPT, relative unit), which combines scores from the MNSI with the vibration perception threshold (VPT, volts) at both limbs [11]; mean glycated hemoglobin (Mean HbA1c, %) averaged over the 48-month follow-up; minimum HbA1c (MIN HbA1c, %) and maximum HbA1c (MAX HbA1c, %) recorded over the 48-month follow-up; pain visual analogue scale questionnaire (VAS, 10-points score) for each limb; Manchester Oxford Foot Questionnaire (MoX, 16 items, max score 64) [16];
- Overall gait performance: dynamic arch index (AI, relative unit), cadence (cad, steps/min), foot contact time (CT, ms), velocity (vel, m/s);
- Plantar peak pressure distribution: peak pressure during gait (PP, kPa) at the hindfoot, midfoot, forefoot, big toe, and toes; dominant (D) and not-dominant (ND) limbs were analyzed separately; and
- Plantar pressure-time integral distribution: pressure-time integral during gait (PTI, kPa·s) at the hindfoot, midfoot, forefoot, big toe, and toes; dominant (D) and not-dominant (ND) limbs were analyzed separately.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bus, S.A.; Lavery, L.A.; Monteiro-Soares, M.; Rasmussen, A.; Raspovic, A.; Sacco, I.C.N.; van Netten, J.J.; International Working Group on the Diabetic Foot. IWGDF Guideline on the Prevention of Foot Ulcers in Persons with Diabetes. 2019. Available online: www.iwgdfguidelines.org (accessed on 29 November 2021).
- Armstrong, D.G.; Boulton, A.J.; Bus, S.A. Diabetic foot ulcers and their recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef]
- Fernando, M.E.; Crowther, R.G.; Lazzarini, P.A.; Sangla, K.S.; Wearing, S.; Buttner, P.; Golledge, J. Plantar pressures are higher in cases with diabetic foot ulcers compared to controls despite a longer stance phase duration. BMC Endocr. Disord. 2016, 16, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacomozzi, C.; Martelli, F. Peak pressure curve: An effective parameter for early detection of foot functional impairments in diabetic patients. Gait Posture 2006, 23, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Hazari, A.; Maiya, A.; Agouris, I.; Monteiro, A. Shivashankar Prediction of peak plantar pressure for diabetic foot: The regressional model. Foot 2019, 40, 87–91. [Google Scholar] [CrossRef]
- Barn, R.; Waaijman, R.; Nollet, F.; Woodburn, J.; Bus, S.A. Predictors of barefoot plantar pressure during walking in patients with diabetes, peripheral neuropathy and a history of ulceration. PLoS ONE 2015, 10, e0117443. [Google Scholar] [CrossRef] [PubMed]
- Fawzy, O.A.; Arafa, A.I.; Wakeel, M.A.; Kareem, S.H. Plantar pressure as a risk assessment tool for diabetic foot ulceration in Egyptian patients with diabetes. Clin. Med. Insights Endocrinol. Diabetes 2014, 7, CMED.S17088. [Google Scholar] [CrossRef] [Green Version]
- Al-Rubeaan, K.; Al Derwish, M.; Ouizi, S.; Youssef, A.M.; Subhani, S.N.; Ibrahim, H.M.; Alamri, B.N. Diabetic foot complications and their risk factors from a large retrospective cohort study. PLoS ONE 2015, 10, e0124446. [Google Scholar] [CrossRef]
- Wouter, B.; Abu-Hanna, A.; Bus, S.A. Development of a multivariable prediction model for plantar foot ulcer recurrence in high- risk people with diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001207. [Google Scholar]
- Guldemond, N.A.; Leffers, P.; Walenkamp, G.H.; Schaper, N.; Sanders, A.P.; Nieman, F.H.; Van Rhijn, L.W. Prediction of peak pressure from clinical and radiological measurements in patients with diabetes. BMC Endocr. Disord. 2008, 8, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belvedere, C.; Giacomozzi, C.; Carrara, C.; Lullini, G.; Caravaggi, P.; Berti, L.; Marchesini, G.; Baccolini, L.; Durante, S.; Leardini, A. Correlations between weight-bearing 3D bone architecture and dynamic plantar pressure measurements in the diabetic foot. J. Foot Ankle Res. 2020, 13, 64. [Google Scholar] [CrossRef]
- Giacomozzi, C.; Sartor, C.D.; Telles, R.; Uccioli, L.; Sacco, I.C.N. Ulcer-risk classification and plantar pressure distribution in patients with diabetic polyneuropathy: Exploring the factors that can lead to foot ulceration. Ann. Ist. Super Sanita 2018, 54, 284–293. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation; WHO Technical Report Series 894; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Feldman, E.L.; Stevens, M.; Thomas, P.; Brown, M.; Canal, N.; Greene, D. A practical two-step quantitative clinical and electrophysiological assessment for the diagnosis and staging of diabetic neuropathy. Diabetes Care 1994, 17, 1281–1289. [Google Scholar] [CrossRef] [PubMed]
- Hazel, M. Clarkson Musculoskeletal Assessment: Joint Motion and Muscle Testing; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Marinozzi, A.; Martinelli, N.; Panascì, M.; Cancilleri, F.; Franceschetti, E.; Vincenzi, B.; Di Martino, A.; Denaro, V. Italian translation of the Manchester-Oxford Foot Questionnaire, with re-assessment of reliability and validity. Qual. Life Res. 2009, 18, 923–927. [Google Scholar] [CrossRef] [PubMed]
- Giacomozzi, C.; Leardini, A.; Caravaggi, P. Correlates between kinematics and baropodometric measurements for an integrated in-vivo assessment of the segmental foot function in gait. J. Biomech. 2014, 47, 2654–2659. [Google Scholar] [CrossRef]
- Giacomozzi, C.; Macellari, V.; Leardini, A.; Benedetti, M.G. Integrated pressure-force-kinematics measuring system for the characterisation of plantar foot loading during locomotion. Med. Biol. Eng. Comput. 2000, 38, 156–163. [Google Scholar] [CrossRef]
- Giacomozzi, C.; Stebbins, J.A. Anatomical masking of pressure footprints based on the Oxford Foot Model: Validation and clinical relevance. Gait Posture 2017, 53, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Leardini, A.; Benedetti, M.G.; Berti, L.; Bettinelli, D.; Nativo, R.; Giannini, S. Rear-foot, mid-foot and fore-foot motion during the stance phase of gait. Gait Posture 2007, 25, 453–462. [Google Scholar] [CrossRef]
- Lavery, L.A.; Oz, O.K.; Bhavan, K.; Wukich, D.K. Diabetic Foot Syndrome in the Twenty-First Century. Clin. Podiatr. Med. Surg. 2019, 36, 355–359. [Google Scholar] [CrossRef]
- Lukin, P.; Kuchumov, A.G.; Zarivchatskiy, M.F.; Kravtsova, T. Clinical Classification of the Diabetic Foot Syndrome Adapted to ICD-10 as a Solution to the Problem of Diagnostics, Statistics and Standardisation. Medicina 2021, 57, 817. [Google Scholar] [CrossRef]
- Edmonds, M.; Manu, C.; Vas, P. The current burden of diabetic foot disease. J. Clin. Orthop. Trauma 2021, 17, 88–93. [Google Scholar] [CrossRef]
- Krzemińska, S.; Kostka, A. Influence of Pain on the Quality of Life and Disease Acceptance in Patients with Complicated Diabetic Foot Syndrome. Diabetes Metab. Syndr. Obes. 2021, 14, 1295–1303. [Google Scholar] [CrossRef]
- Volmer-Thole, M.; Lobmann, R. Neuropathy and Diabetic Foot Syndrome. Int. J. Mol. Sci. 2016, 17, 917. [Google Scholar] [CrossRef] [Green Version]
- Van Netten, J.J.; Bus, S.A.; Apelqvist, J.; Lipsky, B.A.; Hinchliffe, R.J.; Game, F.; Rayman, G.; Lazzarini, P.A.; Forsythe, R.O.; Peters, E.J.G.; et al. Definitions and criteria for diabetic foot disease. Diabetes Metab. Res. Rev. 2019, 36, e3268. [Google Scholar] [CrossRef] [Green Version]
- Rossboth, S.; Lechleitner, M.; Oberaigner, W. Risk factors for diabetic foot complications in type 2 diabetes-A systematic review. Endocrinol. Diabetes Metab. 2020, 17, e00175. [Google Scholar] [CrossRef] [PubMed]
- Azhar, A.; Basheer, M.; Abdelgawad, M.S.; Roshdi, H.; Kamel, M.F. Prevalence of Peripheral Arterial Disease in Diabetic Foot Ulcer Patients and its Impact in Limb Salvage. Int. J. Low. Extrem. Wounds 2021, 15347346211027063. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, M. Vascular disease in the lower limb in type 1 diabetes. Cardiovasc. Endocrinol. Metab. 2019, 8, 39–46. [Google Scholar] [CrossRef]
- Wolf, G.; Müller, N.; Busch, M.; Eidner, G.; Kloos, C.; Hunger-Battefeld, W.; Müller, U.A. Diabetic foot syndrome and renal function in type 1 and 2 diabetes mellitus show close association. Nephrol. Dial. Transplant. 2009, 24, 1896–1901. [Google Scholar] [CrossRef]
- Kulwas, A.; Lisewska, B.; Jundziłł, W.; Ruszkowska, B.; Drewniak, W.; Ruprecht, Z.; Gadomska, G.; Rość, D. Tissue plasminogen activator (t-PA) and plasminogen activator inhibitor type 1 (PAI-1) in diabetic foot syndrome. Adv. Med. Sci. 2017, 62, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Humpert, P.M.; Battista, M.J.; Lammert, A.; Reismann, P.; Djuric, Z.; Rudofsky, G., Jr.; Zorn, M.; Morcos, M.; Hammes, H.P.; Nawroth, P.P.; et al. Association of stromal cell-derived factor 1 genotype with diabetic foot syndrome and macrovascular disease in patients with type 2 diabetes. Clin. Chem. 2006, 52, 1206–1208. [Google Scholar] [CrossRef]
- Najafi, B.; Mishra, R. Harnessing Digital Health Technologies to Remotely Manage Diabetic Foot Syndrome: A Narrative Review. Medicina 2021, 57, 377. [Google Scholar] [CrossRef]
- Asghar, A.; Naaz, S. The transverse arch in the human feet: A narrative review of its evolution, anatomy, biomechanics and clinical implications. Morphologie 2021, S1286-0115(21)00191-0. [Google Scholar] [CrossRef] [PubMed]
- Reeves, N.D.; Orlando, G.; Brown, S.J. Sensory-Motor Mechanisms Increasing Falls Risk in Diabetic Peripheral Neuropathy. Medicina 2021, 57, 457. [Google Scholar] [CrossRef] [PubMed]
- Primadhi, R.A.; Herman, H. Diabetic foot: Which one comes first, the ulcer or the contracture? World J. Orthop. 2021, 12, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Hulshof, C.M.; van Netten, J.J.; Pijnappels, M.; Bus, S.A. The Role of Foot-Loading Factors and Their Associations with Ulcer Development and Ulcer Healing in People with Diabetes: A Systematic Review. J. Clin. Med. 2020, 9, 3591. [Google Scholar] [CrossRef] [PubMed]
- Hasan, R.; Firwana, B.; Elraiyah, T.; Domecq, J.P.; Prutsky, G.; Nabhan, M.; Prokop, L.J.; Henke, P.; Tsapas, A.; Montori, V.M.; et al. A systematic review and meta-analysis of glycemic control for the prevention of diabetic foot syndrome. J. Vasc. Surg. 2016, 63 (Suppl. 2), 22S–28S.e2. [Google Scholar] [CrossRef] [Green Version]
- Song, K.; Chambers, A.R. Diabetic Foot Care. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK553110/ (accessed on 29 November 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ALL | DNT1 | DNT2-No ob | DNT2-ob | DNNT1 | DNNT2-No ob | DNNT2-ob | |
|---|---|---|---|---|---|---|---|
| n (M/F) | 79 (39M/40F) | 12 (9M/3F) | 11 (6M/5F) | 20 (11M/9F) | 15 (1M/14F) | 7 (3M/4F) | 13 (8M/5F) |
| AGE (years) | 58.1 ± 12.0 | 53.1 ± 14.1 | 67.1 ± 8.8 | 61.6 ± 6.8 | 48.3 ± 14.6 | 65.4 ± 3.9 | 58.3 ± 8.2 |
| BMI (kg/m2) | 29.4 ± 6.8 | 24.8 ± 2.5 | 25.1 ± 3.1 | 35.7 ± 5.4 | 23.6 ± 3.2 | 25.6 ± 3.3 | 36.3 ± 3.8 |
| YOD (years) | 20.0 ± 12.8 | 34.2 ± 12.6 | 18.4 ± 8.6 | 13.9 ± 7.8 | 23.6 ± 3.2 | 12.4 ± 9.0 | 12.1 ± 6.7 |
| NS-VPT | 3.2 ± 1.4 | 3.8 ± 0.9 | 4.3 ± 1.0 | 4.2 ± 1.2 | 1.7 ± 0.7 | 2.5 ± 1.3 | 2.3 ± 0.9 |
| Mean HbA1c (%) * | 7.9 ± 1.3 | 8.4 ± 1.6 | 7.0 ± 0.8 | 8.0 ± 1.4 | 8.3 ± 1.0 | 7.1 ± 0.3 | 8.2 ± 1.5 |
| MIN HbA1c (%) * | 7.1 ± 1.2 | 7.7 ± 1.3 | 6.4 ± 0.5 | 7.1 ± 1.6 | 7.8 ± 1.1 | 6.2 ± 0.3 | 6.9 ± 1.1 |
| MAX HbA1c (%) * | 8.9 ± 1.7 | 9.4 ± 1.8 | 8.0 ± 1.7 | 9.0 ± 1.6 | 8.8 ± 1.0 | 8.2 ± 1.0 | 9.8 ± 2.3 |
| patients with lesions * | 12 (8M/4F) %: 15 (21/10) | 2 (2M) %: 17 (22) | 2 (2M) %: 18 (33) | 3 (3M) %: 15 (27) | 3 (3F) %: 20 (21) | - | 2 (1M/1F) %: 15 (20) |
| number of lesions * | 22 (1 midfoot; 5 forefoot; 6 big toe; 10 toes) r: 0.28 | 3 (1 forefoot; 2 10 toes) r: 0.25 | 5 (2 big toe; 3 toes) r: 0.45 | 9 (3 forefoot; 3 big toe; 3 toes) r: 0.45 | 3 (1 forefoot; 1 big toe; 1 toes) r: 0.20 | 2 (1 midfoot; 1 toes) r: 0.15 |
| Group | Cases | Patients with Lesions | Description of Lesions |
|---|---|---|---|
| DNT1 | 12 (9M/3F) | 2 (2M/0F) |  L1 (M): D (toes, m24) and ND (forefoot, m36) L1 (M): D (toes, m24) and ND (forefoot, m36)  L2 (M): D (toes, m36) L2 (M): D (toes, m36) |
| DNT2 no ob | 11 (6M/5F) | 2 (2M/0F) |  L1 (M): D (big toe, m48; toes, m48) L1 (M): D (big toe, m48; toes, m48) L2 (M): D (big toe, m36; toes, m9 and m36) L2 (M): D (big toe, m36; toes, m9 and m36) |
| DNT2 ob | 20 (11M/9F) | 3 (3M/0F) |  L1 (M): D (toes, m9 and m48) L1 (M): D (toes, m9 and m48) L2 (M): ND (forefoot, m9 and m24 and m48) L2 (M): ND (forefoot, m9 and m24 and m48) L3 (M): D (big toe, m6 and m24 and m48) and ND (toes, m24) L3 (M): D (big toe, m6 and m24 and m48) and ND (toes, m24) |
| DNNT1 | 15 (1M/14F) | 3 (0M/3F) |  L1 (F): D (toes, m24) L1 (F): D (toes, m24) L2 (F): D (big toe, m36) L2 (F): D (big toe, m36) L3 (F): ND (forefoot, m36) L3 (F): ND (forefoot, m36) |
| DNNT2 no ob | 7 (3M/4F) | - | |
| DNNT2 ob | 13 (8M/5F) | 2 (1M/1F) |  L1 (M): ND (toes, m48) L1 (M): ND (toes, m48) L2 (F): D (midfoot, m24) L2 (F): D (midfoot, m24) |
| Total | 12 (8M/4F) | 22 (1 midfoot; 5 forefoot; 6 big toe; 10 toes) |
| DNT1 | DNT2-no ob | DNT2-ob | DNNT1 | DNNT2-no ob | DNNT2-ob | |
|---|---|---|---|---|---|---|
| DNT1 | AGE; YOD | TT dors ND; hindfoot incl ND; BMI; YOD; CT ND; vel ND; PTI midfoot D and ND | NS-VPT | YOD | YOD; NS-VPT; PTI midfoot D and ND | |
| DNT2-no ob | BMI; PTI hindfoot D; PTI midfoot D | AGE; NS-VPT; PTI forefoot D | NS-VPT; PTI forefoot D | NS-VPT; PTI forefoot D | ||
| DNT2-ob | MOX D and ND; AGE; YOD; NS-VPT; cad D and ND; CT D and ND; vel D and ND; PP midfoot D; PP forefoot D; PTI hindfoot D and ND; PTI midfoot D and ND; PTI forefoot D and ND | NS-VPT; PTI midfoot D | NS-VPT | |||
| DNNT1 | AGE; YOD; MIN HbA1c | BMI; YOD; vel D; PTI midfoot D and ND | ||||
| DNNT2-no ob | BMI; PTI midfoot D and ND | |||||
| DNNT2-ob |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giacomozzi, C.; Lullini, G.; Leardini, A.; Caravaggi, P.; Ortolani, M.; Marchesini, G.; Baccolini, L.; Berti, L. Analysis of Clinical Profiles, Deformities, and Plantar Pressure Patterns in Diabetic Foot Syndrome. Appl. Sci. 2021, 11, 11464. https://doi.org/10.3390/app112311464
Giacomozzi C, Lullini G, Leardini A, Caravaggi P, Ortolani M, Marchesini G, Baccolini L, Berti L. Analysis of Clinical Profiles, Deformities, and Plantar Pressure Patterns in Diabetic Foot Syndrome. Applied Sciences. 2021; 11(23):11464. https://doi.org/10.3390/app112311464
Chicago/Turabian StyleGiacomozzi, Claudia, Giada Lullini, Alberto Leardini, Paolo Caravaggi, Maurizio Ortolani, Giulio Marchesini, Luca Baccolini, and Lisa Berti. 2021. "Analysis of Clinical Profiles, Deformities, and Plantar Pressure Patterns in Diabetic Foot Syndrome" Applied Sciences 11, no. 23: 11464. https://doi.org/10.3390/app112311464