
Systematic Review and Meta-Analysis of the Use of Hyaluronic Acid Injections to Restore Interproximal Papillae

 ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Selection of Studies
2.4. Inclusion Criteria
2.5. Exclusion Criteria
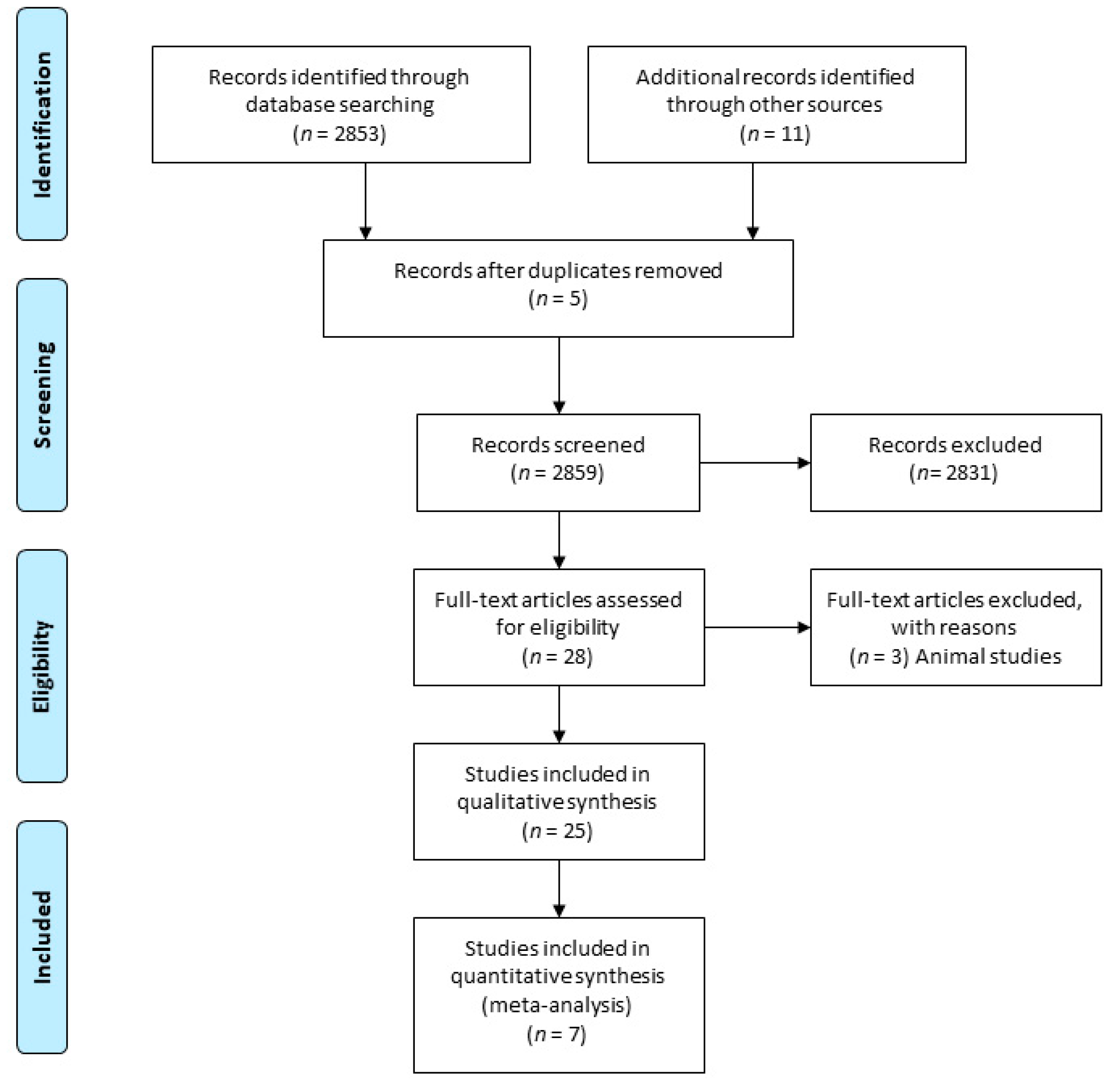
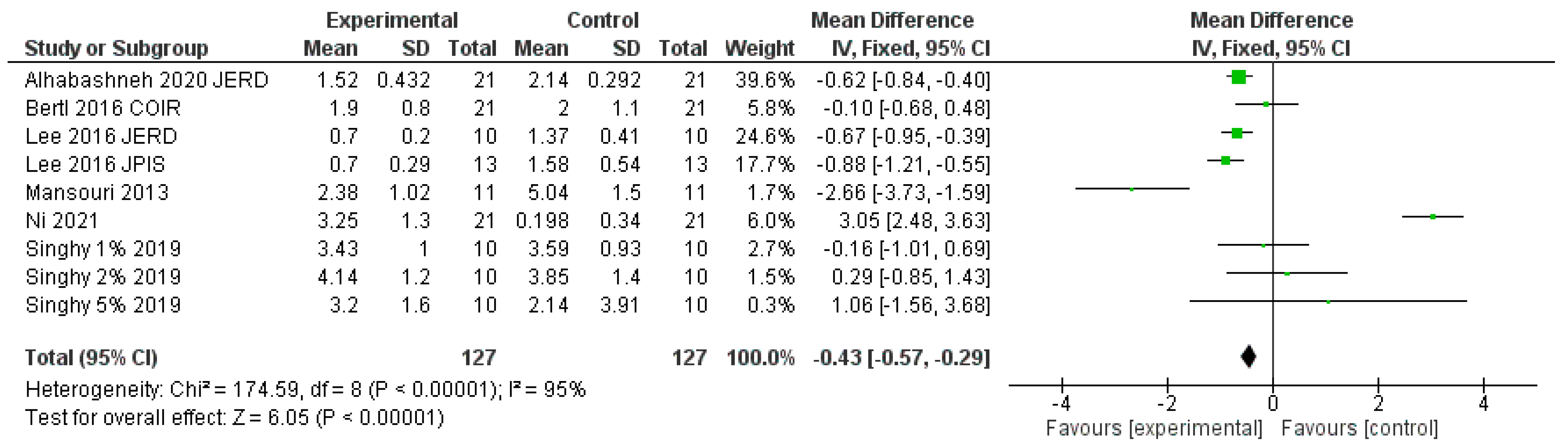
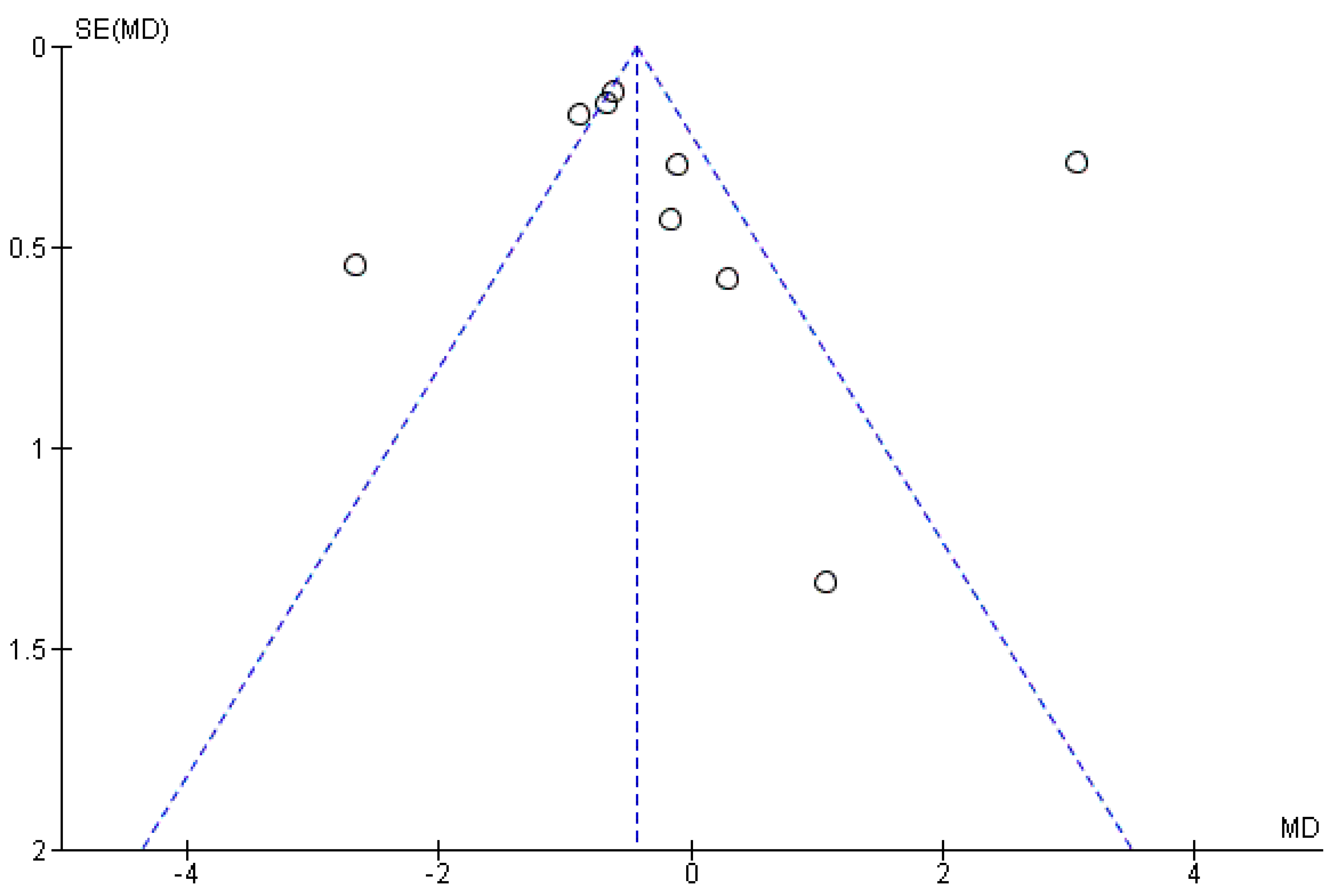
3. Results
“To assess the validity of the review, the Kappa coefficient was used. Kappa is a measure of agreement proposed by Cohen in 1960, which is based on comparing the agreement observed in a set of data, with respect to what could occur by mere chance. The agreement obtained in our study was 0.824.”
4. Discussion
4.1. Study Limitations
4.2. Future Research Suggestions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lang, N.P.; Lindhe, J. Clinical Periodontology and Implant Dentistry; John Wiley & Sons: Chichester, UK, 2015. [Google Scholar]
- Kokich, V.O.; Kokich, V.G.; Kiyak, H.A. Perceptions of dental professionals and laypersons to altered dental esthetics: Asymmetric and symmetric situations. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.; Reddy, B.; Reddy, R. Perception differences of altered dental esthetics by dental professionals and laypersons. Indian J. Dent. Res. 2011, 22, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Ko-Kimura, N.; Kimura-Hayashi, M.; Yamaguchi, M.; Ikeda, T.; Meguro, D.; Kanekawa, M.; Kasai, K. Some factors associated with open gingival embrasures following orthodontic treatment. Aust. Orthod. J. 2003, 19, 19–24. [Google Scholar] [PubMed]
- Seibert, J.; Lindhe, J. Esthetics and periodontal therapy. Textb. Clin. Periodontol. 1989, 2, 477–514. [Google Scholar]
- Wu, Y.J.; Tu, Y.K.; Huang, S.M.; Chan, C.P. The influence of the distance from the contact point to the crest of bone on the presence of the interproximal dental papilla. Chang Gung Med. J. 2003, 26, 822–828. [Google Scholar] [PubMed]
- Chow, Y.C.; Eber, R.M.; Tsao, Y.P.; Shotwell, J.L.; Wang, H.L. Factors associated with the appearance of gingival papillae. J. Clin. Periodontol. 2010, 37, 719–727. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.A.; Park, J.H. Esthetic considerations in interdental papilla: Remediation and regeneration. J. Esthet. Restor. Dent. 2010, 22, 18–28. [Google Scholar] [CrossRef]
- Rohrich, R.J.; Ghavami, A.; Crosby, M.A. The role of hyaluronic acid fillers (restylane) in facial cosmetic surgery: Review and technical considerations. Plast. Reconstr. Surg. 2007, 120, 41S–54S. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, B2700. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Vandana, K. Use of different concentrations of hyaluronic acid in interdental papillary deficiency treatment: A clinical study. J. Indian Soc. Periodontol. 2019, 23, 35–41. [Google Scholar] [CrossRef]
- Bertl, K.; Gotfredsen, K.; Jensen, S.S.; Bruckmann, C.; Stavropoulos, A. Can hyaluronan injections augment deficient papillae at implant-supported crowns in the anterior maxilla? A randomized controlled clinical trial with 6 months follow-up. Clin. Oral Implant. Res. 2017, 28, 1054–1061. [Google Scholar] [CrossRef]
- Lee, W.P.; Kim, H.J.; Yu, S.J.; Kim, B.O. Six month clinical evaluation of interdental papilla reconstruction with injectable hyaluronic acid gel using an image analysis system. J. Esthet. Restor. Dent. 2016, 28, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.P.; Seo, Y.S.; Kim, H.J.; Yu, S.J.; Kim, B.O. The association between radiographic embrasure morphology and interdental papilla reconstruction using injectable hyaluronic acid gel. J. Periodontal Implant Sci. 2016, 46, 277–287. [Google Scholar] [CrossRef] [Green Version]
- Mansouri, S.S.; Ghasemi, M.; Salmani, Z.; Shams, N. Clinical application of hyaluronic acid gel for reconstruction of interdental papilla at the esthetic zone. J. Islam. Dent. Assoc. Iran 2013, 28, 221–230. [Google Scholar]
- Alhabashneh, R.; Alomari, S.; Khaleel, B.; Qinawi, H.; Alzaubi, M. Interdental papilla reconstruction using injectable hyaluronic acid: A 6 month prospective longitudinal clinical study. J. Esthet. Restor. Dent. 2021, 33, 531–537. [Google Scholar] [CrossRef]
- Ni, J.; Zhong, Z.; Wu, Y.; Shu, R.; Wu, Y.; Li, C. Hyaluronic acid vs. physiological saline for enlarging deficient gingival papillae: A randomized controlled clinical trial and an in vitro study. Ann. Transl. Med. 2021, 9, 759. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Ziahosseini, P.; Hussain, F.; Millar, B.J. Management of gingival black triangles. Br. Dent. J. 2014, 217, 559–563. [Google Scholar] [CrossRef]
- Kurth, J.R.; Kokich, V.G. Open gingival embrasures after orthodontic treatment in adults: Prevalence and etiology. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Choquet, V.; Hermans, M.; Adriaenssens, P.; Daelemans, P.; Tarnow, D.P.; Malevez, C. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. J. Periodontol. 2001, 72, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, X.; Vela, X.; Méndez, V.; Segalà, M.; Calvo-Guirado, J.L.; Tarnow, D.P. The effect of abutment dis/reconnections on peri-implant bone resorption: A radiologic study of platform-switched and non-platform-switched implants placed in animals. Clin. Oral Implant. Res. 2013, 24, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Salama, H.; Salama, M.A.; Garber, D.; Adar, P. The interproximal height of bone: A guidepost to predictable aesthetic strategies and soft tissue contours in anterior tooth replacement. Pract. Periodontics Aesthet. Dent. 1998, 10, 1131–1141. [Google Scholar] [PubMed]
- Roccuzzo, M.; Roccuzzo, A.; Ramanuskaite, A. Papilla height in relation to the distance between bone crest and interproximal contact point at single-tooth implants: A systematic review. Clin. Oral Implant. Res. 2018, 29, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Bertl, K.; Gotfredsen, K.; Jensen, S.S.; Bruckmann, C.; Stavropoulos, A. Adverse reaction after hyaluronan injection for minimally invasive papilla volume augmentation. A report on two cases. Clin. Oral Implant. Res. 2017, 28, 871–876. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PICO Process | |
|---|---|
| Population | Patients with interproximal papilla deficiency |
| Intervention | Hyaluronic acid injection |
| Comparison | Treatment with saline serum/placebo/or control prior to the treatment |
| Outcome | Height of the papilla in mm |
| Mansouri 2013 JIDAI | Bertl 2016 COIR | Lee 2016 JERD | Lee 2016 JPIS | Singh 1% 2019 JISP | Singh 2% 2019 JISP | Singh 5% 2019 JISP | Alhabashneh 2020 JERD | Ni 2021 ATM | |
|---|---|---|---|---|---|---|---|---|---|
| Confusion Bias | - | + | + | + | - | - | - | ? | ? |
| Selection Bias | + | + | + | + | - | - | - | - | ¿? |
| Classification Bias | - | + | - | ? | ? | ? | ? | ? | ? |
| Intervention? Intervention Bias | - | ? | ? | + | + | + | + | + | + |
| Lost Data Bias | + | ? | - | ? | - | - | - | - | - |
| Measurement Bias | ? | + | - | + | - | - | - | + | + |
| Results Bias | + | - | ? | + | ? | ? | ? | + | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanchez-Perez, A.; Vela-García, T.R.; Mateos-Moreno, B.; Jornet-García, A.; Navarro-Cuellar, C. Systematic Review and Meta-Analysis of the Use of Hyaluronic Acid Injections to Restore Interproximal Papillae. Appl. Sci. 2021, 11, 10572. https://doi.org/10.3390/app112210572
Sanchez-Perez A, Vela-García TR, Mateos-Moreno B, Jornet-García A, Navarro-Cuellar C. Systematic Review and Meta-Analysis of the Use of Hyaluronic Acid Injections to Restore Interproximal Papillae. Applied Sciences. 2021; 11(22):10572. https://doi.org/10.3390/app112210572
Chicago/Turabian StyleSanchez-Perez, Arturo, Tania Rosa Vela-García, Bibiana Mateos-Moreno, Alfonso Jornet-García, and Carlos Navarro-Cuellar. 2021. "Systematic Review and Meta-Analysis of the Use of Hyaluronic Acid Injections to Restore Interproximal Papillae" Applied Sciences 11, no. 22: 10572. https://doi.org/10.3390/app112210572