1. Introduction
In recent decades, surgical procedures have evolved significantly in order to reduce the operative risk for the patient. Open procedures have evolved to minimally invasive procedures in which smaller incisions are used to minimize muscle retraction and the infection risk and, subsequently, shorten the hospitalization period. However, the disadvantage of these minimal invasive procedures is the lack of anatomic orientation. This resulted in the technological evolution using medical imaging techniques to guide the surgical procedure [
1,
2,
3]. Nowadays, image guidance occurs in combination with navigation systems. Navigation systems are intraoperative imaging modalities based on X-rays that guide the surgeon in inserting the surgical instruments in the operation field. Navigation systems have evolved from uniplanar C-arm fluoroscopy generating two-dimensional (2D) images to more advanced multiplanar or three-dimensional (3D) navigation systems such as the mobile intraoperative computed tomography (iCT) [
1,
3]. Several studies have shown that navigation systems are associated with safer and more accurate surgery compared to freehand surgeries [
4,
5,
6,
7]. However, intraoperative imaging devices almost exclusively use ionizing radiation. As a result, the surgical staff and patients are exposed to the radiation source repetitively. While the patient is mainly exposed to the primary beam, the surgeon and the operating staff are exposed to scatter radiation. Exposure to ionizing radiation can potentially cause several pathologies. To minimize the occurrence of radiation associated pathologies, the ALARA (As Low As Reasonably Achievable) principle is used, which claims that the exposure to radiation must be kept as low as reasonably achievable [
8,
9,
10,
11]. It is especially important for surgeons and the operating nurses, who are repetitively exposed to ionizing radiation during surgical procedures, to have knowledge about the radiation dose [
8,
9,
10,
11].
One of the procedures in which navigation systems are used is the lumbar interbody fusion (LIF), an effective treatment for patients with lumbar spinal disorders where conservative management fails [
12,
13,
14,
15]. The spine can be approached in five main directions: posterior, transforaminal, oblique, anterior, and lateral [
12,
14]. The approach direction depends on the surgical indication, and all approaches can be performed in a minimally invasive way [
12,
14,
15]. A posterior approach of the lumbar interbody fusion (PLIF) is used to treat degenerative conditions requiring a fusion procedure. A minimally invasive PLIF procedure (MI-PLIF) allows excellent visualization of the nerve roots and adequate interbody height restoration in order to decompress the nerves. Furthermore, this approach allows a 360-degree fusion through a single incision.
As described above, navigation systems are used to increase the accuracy and safety of instrumentation during minimally invasive surgery. This study evaluates the use of a novel, 3D navigation system, iCT, during an MI-PLIF procedure with comparison to the golden standard technique, C-arm fluoroscopy, regarding radiation exposure to the patient and the operating staff. Furthermore, attention was focused on the length of both procedures because knowledge about clinical efficacy is important to outweigh the benefits for the patient with the potential harm of ionizing radiation.
2. Materials and Methods
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Ziekenhuis Oost-Limburg Genk, Belgium (eudract/B-nr B371201630400—approved 17 January 2017). All patients with a planned MI-PLIF surgery from January 2017 until May 2019 were asked to participate. Patients younger than eighteen years old and patients with fusion of more than two levels were excluded from the study. Informed consent was obtained from every participant. The MI-PLIF procedures were performed by three neurosurgeons with eleven (EB—surgeon 1), sixteen (TD—surgeon 2) and nineteen (DP—surgeon 3) years of experience respectively. The assistant imaging techniques during the surgery were either biplanar OEC Fluorostar 7900 series C-arm (GE Healthcare, Little Chalfont, UK) or AIRO
® iCT (Mobius Imaging, Shirley, MA, USA) in combination with a lateral OEC Fluorostar 7900 series C-arm (GE Healthcare); this will be referred to as C-arm fluoroscopy and iCT, respectively (
Figure 1) The operating surgeon chose which imaging techniques were used during the procedures.
Peak skin dose (PSD) and effective dose (ED) of the patient, surgeon, operating nurse, and anesthesiologist were measured during MI-PLIF procedures with iCT and C-arm fluoroscopy. The radiation exposure of the neurosurgeon, anesthesiologist, and operating nurse was quantified by the ED. This dosage was measured using personal dosimeters (DoseAware system, Phillips, 56,884 PC Best, The Netherlands). Personal dosimeters were allocated before the start of the surgery and were always positioned on top of the lead apron. The Hp(10) value (personal dose equivalent) was obtained using the Dose View software (DoseAware system, Phillips) by marking the start and end time of the operation. This value represents an estimate of the radiation dose at 10 mm depth in soft tissue and was used as the ED.
To evaluate the radiation exposure of the patient during the surgery, the PSD and the ED of the patient were quantified. The ED of the patient was calculated using the parameters of the imaging devices and a conversion factor. The parameters of iCT were collected after each scan and included kilovolt (kV), milliampere (mA), milliampere-second (mAs), computed tomography dose index (CTDI), and dose length product (DLP). Parameters of the lateral C-arm were collected at the end of the surgery. These consisted of kV, mA, dose area product (DAP), entrance dose, and fluoroscopy time. All collected parameters provide indirect information about the X-rays and the radiation dose produced by the devices. A conversion factor was calculated with a Monte Carlo simulation; this simulation computes a 3D dose distribution for a geometrical model of a fictive patient by tracking the trajectory and energy deposition of X-ray photons through the geometrical model (9). Thereafter, the ED derived from iCT was computed by multiplying the conversion factor with the sum of all collected DLPs during surgery. The ED produced by the lateral C-arm was calculated by multiplying the conversion factor with the entrance dose. Because the placement of the graft cages in the iCT group is assisted by a lateral C-arm, the total ED for these patients was obtained by a summation of the ED of the iCT and the ED of the lateral C-arm. In order to measure the localized radiation dose on the frontal and lateral skin, the PSD was quantified with GafchromicTM films (Ashland Advanced Materials, Bridgewater, NJ, USA).
To evaluate the time efficiency of the surgeries, the duration of pedicle screw placement and the total operation time was measured. The total operation time length includes the time between the first incision and the last suture. The duration of pedicle screw placement was measured from narcosis to decompression.
Normally distributed or not-normally distributed, continuous variables are expressed as mean ± SD or as median (interquartile range), respectively. Normality was assessed by the Shapiro–Wilk statistic. To define the difference in unpaired continuous variables between both groups, an independent T-test or Mann–Whitney U test was performed. Differences between unpaired categorical variables were assessed by a Chi-square or Fisher’s exact (n < 5) test. Furthermore, a Spearman’s correlation analysis was performed to evaluate the correlation between the BMI and the ED of the patient per group. All statistical analyses were performed using SPSS 25.0 (IBM®, Chicago, IL, USA) with a significance level α of 5%.
3. Results
There were 100 potential candidates for the study. Of these, 25 were excluded from the study because of the following reasons: incomplete informed consent (n = 9), no full MI-PLIF procedure (n = 9), other LIF procedure (n = 2), other C-arm fluoroscopy used (n = 4), or when more than two levels of vertebrae were fused (n = 1). A total of 75 patients participated in the study. Of these, 30 patients underwent a full MI-PLIF surgery with the assistance of the AIRO CT device, while 45 patients had surgery with the assistance of C-arm fluoroscopy devices.
The iCT group consisted of 11 males and 19 females with a median BMI of 27 and a median age of 60 years. The fluoroscopy group included 21 males and 24 females with a median BMI of 26.5 and a median age of 60 years. The indications for MI-PLIF surgery in the iCT group consisted mainly of listhesis (n = 16) or a combination of multiple lumbar disorders (n = 7). However, some patients in the iCT group were offered MI-PLIF surgery because of discopathy (n = 3), hernia (n = 2), and severe osteoarthritis of discs (n = 2). Indications for MI-PLIF in the C-arm fluoroscopy group were listhesis (n = 16), multiple spinal disorders (n = 18), discopathy (n = 4), stenosis (n = 3), hernia (n = 1), facet arthrosis (n = 1), or another lumbar spine disorder (n = 1). A total of 29 (96.7%) patients in the iCT group had a single-level lumbar spinal fusion. Only one individual had two levels of vertebrae fused (3.3%). A total of 38 (84.4%) patients of the fluoroscopy group had a single-level fusion, while 7 (15.6%) patients had a multi-level fusion. There is no significant difference between both groups in terms of age, BMI, gender, indications, and number of levels to be fused.
Surgeon 1 performed 21 surgeries (iCT:
n = 19; C-arm fluoroscopy;
n = 2), surgeon 2 performed 18 surgeries (iCT:
n = 10; C-arm fluoroscopy;
n = 9), and surgeon 3 performed 36 surgeries (iCT:
n = 1; C-arm fluoroscopy;
n = 35). A summary of the basic characteristics of the study population in both groups is given in
Table 1.
3.1. Radiation Dose of the Operating Staff
The radiation doses of the neurosurgeon, operating nurse, and anesthesiologist were evaluated by assessing the ED via personal dosimeters that were always worn on top of the lead apron during surgery. The median ED of the surgeon was 11.00 (5.00–42.00) µSv during surgeries with iCT and 151.00 (77.00–329.00) µSv with C-arm fluoroscopy. Statistical analysis confirmed a significant difference in the surgeon’s radiation dose between surgeries with iCT and C-arm fluoroscopy (
Figure 2). In summary, the surgeon was exposed to a thirteenfold lower radiation dose on average when iCT was used instead of C-arm fluoroscopy.
Similar to the ED of the surgeon, the ED of the operating nurse was significantly reduced during surgeries with iCT, compared to C-arm fluoroscopy (
Figure 3). The median ED was 2.00 (1.00–6.75) µSv during surgeries with iCT and 8.00 (3.00–15.25) µSv during surgeries with C-arm fluoroscopy.
Furthermore, the ED of the anesthesiologist was also significantly lower during surgeries with iCT, compared to C-arm fluoroscopy (
Figure 4). The median ED of the anesthesiologist was 0.00 (0.00–1.00) µSv with iCT and 1.00 (0.00–3.00) µSv with C-arm fluoroscopy.
3.2. Radiation Dose of the Patient
3.2.1. Effective Dose of the Patient
The ED of the patient was calculated using the parameters of the used imaging devices and a conversion factor. Statistical analysis showed a significant difference in the ED of patients operated with iCT and C-arm fluoroscopy (
Figure 5). The median ED during surgeries with iCT was 8.869 (5.929–10.639) mSv, while during surgeries with C-arm fluoroscopy the ED of the patient was 2.274 (1.453–3.472) mSv. Therefore, the median ED of the patient was four times higher during surgery with iCT, compared to C-arm fluoroscopy.
A Spearman’s correlation analysis showed a moderate correlation (r = 0.438) between the patient’s BMI and the ED of patients who had an MI-PLIF surgery performed with iCT. However, for patients who had an MI-PLIF with C-arm fluoroscopy, the correlation was only very weak (r = 0.071) (
Figure 6).
3.2.2. Lateral and Abdominal Peak Skin Dose
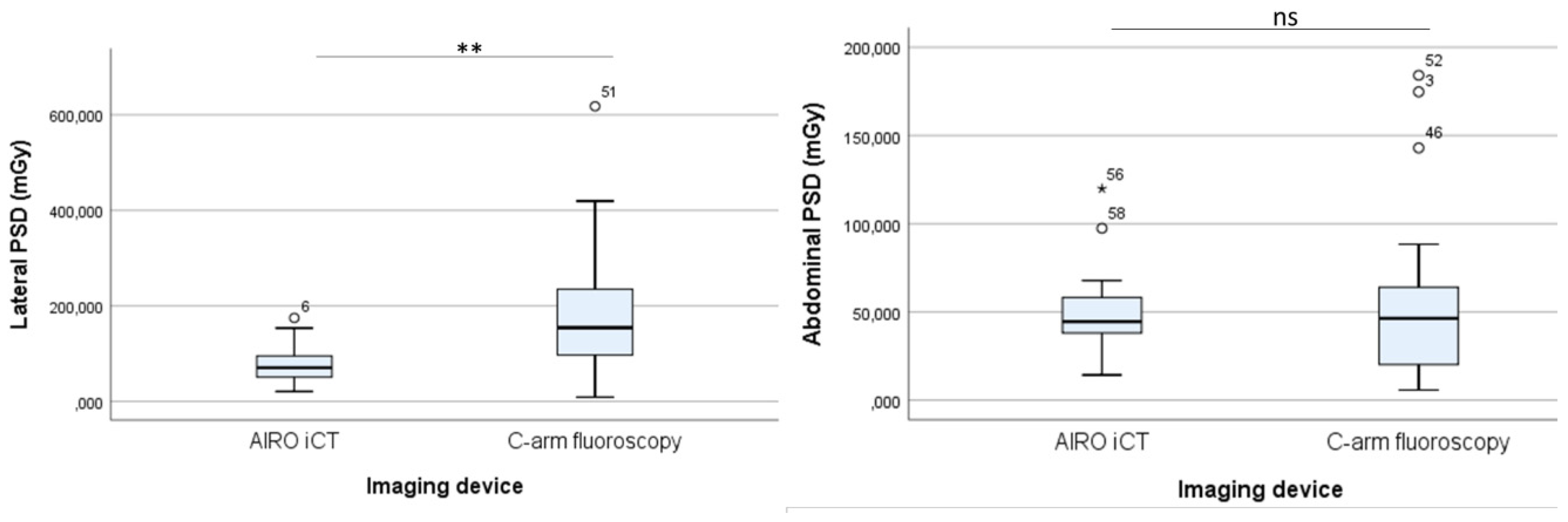
In contrast to the ED of the patient, the localized radiation dose at the lateral abdomen of the patient was significantly higher during surgeries with C-arm fluoroscopy, compared to iCT (
Figure 7 (left)). The median lateral PSD of the patient was 70.35 (49.06–96.49) mGy with iCT and 154.15 (96.60–235.14) mGy with C-arm fluoroscopy. Thus, the lateral PSD of the patients decreased approximately two times when iCT was used instead of C-arm fluoroscopy. However, the abdominal PSD was lower with both imaging devices and did not differ significantly between surgeries with iCT and C-arm fluoroscopy (
Figure 7 (right)). The median abdominal PSD of the patient ranged between 44.524 (37.973–59.103) mGy with iCT and 46.347 (19.972–65.721) mGy with C-arm fluoroscopy.
3.3. Time-Efficiency
In order to evaluate the time efficiency of MI-PLIF surgeries performed by the assistance of C-arm fluoroscopy or iCT, the total operation length and the duration of pedicle screw insertion was assessed. The median time length for pedicle screw placement and the total operation (in hours:minutes:seconds) was 02:01:41 (1:47:59–2:41:03) and 03:46:31 (3:22:35–04:29:20) with iCT, and 1:20:10 (01:02:45–01:45:52) and 2:16:00 (1:52:02–03:01:06). With C-arm fluoroscopy, respectively. In general, pedicle screw insertion last approximately 42 min longer on average during surgeries performed with the assistance of iCT, compared to C-arm fluoroscopy, and the total operation lasted circa 90 min longer on average with iCT. Statistical analysis confirmed a significant difference in time efficiency between MI-PLIF surgeries assisted by iCT and C-arm fluoroscopy (
Figure 8).
4. Discussion
Over the past decades, intraoperative navigation systems have evolved from 2D conventional C-arm fluoroscopy to 3D imaging, using the CT technique. Knowledge about radiation exposure to the operating staff is of great importance since the long-term effects of chronic low-dose exposure are still unclear [
16,
17,
18,
19]. Our study results show a significant lower radiation exposure to the operating staff in procedures performed with iCT, compared to C-arm fluoroscopy. The surgeon’s and the operating nurse’s radiation dose respectively decreased thirteen and four times on average (
Figure 2 and
Figure 3), while the radiation dose of the anesthesiologist (
Figure 4) was almost eliminated with iCT. This can be explained by the ability to insert the pedicle screws using a single iCT scan and spinal navigation [
8,
9,
20,
21]. During a procedure with iCT, prior to pedicle screw insertion, a scan is taken via a compact system pendant which can be held by an unsterile nurse behind a lead wall in the OR. The sterile surgeon and operating nurse also stand behind this lead wall. The generated image is then, together with navigation software, used to insert the screws in an accurate manner. Afterwards, a second iCT scan is obtained to evaluate the placement of the pedicle screws. If misplaced, the inaccurate screw(s) are relocated. In contrast, fluoroscopy-guided surgeries require real-time imaging of the surgical instruments in the region of interest [
22]. Herewith, the surgeon and operating nurse stand at the contralateral side of the X-ray source when radiographic images are made, resulting in a higher radiation dose. During MI-PLIF surgeries assisted by iCT, an additional lateral C-arm fluoroscopy device was used to guide the insertion of a graft cage in the intervertebral space. Therefore, we believe that the ED of the staff members is mainly due to radiation exposure derived from the lateral C-arm fluoroscope. This thought is supported by Lian et al. who could demonstrate that the radiation dose of the operating room staff could be completely eliminated during minimally invasive transforaminal LIF procedures guided by only an AIRO iCT device and 3D navigation [
23]. In addition, Navarro-Ramirez et al. demonstrated that various spinal procedures can be performed with only iCT navigation, eliminating the use of a C-arm fluoroscope in 75% of the cases [
24]. The greater interquartile range of surgeries performed with C-arm fluoroscopy, compared to iCT, suggest that the exposure of the operating room staff is dependent on the surgeon’s experience and the complexity of the surgery, while the radiation output of the iCT is more standardized. Thus, AIRO iCT-based spinal instrumentation increases the safety of the OR personnel by decreasing or even eliminating radiation exposure. Consequently, surgeons can perform more image-guided surgeries per year when they use iCT before they reach the annual dose limit of 20 mSv. In addition, it is not necessary to wear a lead skirt during iCT-navigated surgery, since the operating room staff can leave the room while scanning [
24,
25]. Therefore, it can increase ergonomics by avoiding back pain or muscular fatigue caused by the weight of the lead apron after long-lasting procedures [
26].
In contrary to the ED of the operating staff, the ED of the patient increased approximately four times on average during surgeries with iCT, compared to surgeries performed with C-arm fluoroscopy. (
Figure 5) The rotation and movement of the iCT causes a more widespread irradiated area, while the primary radiation bundle of the fluoroscopy device irradiates a more localized area. This also explains why the lateral PSD is higher during surgeries with biplanar C-arm fluoroscopy than with iCT. (
Figure 7 (left)) The abdominal Gafchromic
TM film was only exposed to radiation during pedicle screw fixation, while the lateral Gafchromic
TM film was exposed during pedicle screw and cage placement. Therefore, the abdominal PSD was relatively low and did not differ between surgeries with iCT or C-arm fluoroscopy. (
Figure 7 (right)) Bindal et al. reported a median anteroposterior skin dose of the patient of 59.5 (8.3–252) mGy and a lateral skin exposure of 78.8 mGy (6.3–269.5 mGy) during fluoroscopy-guided transforaminal LIF procedures [
27]. In comparison to our results, this is a slightly higher anteroposterior skin dose and a halved lateral skin dose. However, in their study, no graft cages were inserted with fluoroscopy guidance. Even though the ED of the patient was higher with iCT, a postoperative CT scan was not required anymore unless desired by the neurosurgeon. Moreover, it is stated that there is no need to consistently evaluate the placement of the pedicle screws with a second iCT scan since the accuracy is even higher with iCT navigation than with C-arm fluoroscopy [
25,
28]. Furthermore, there is a moderate positive correlation between the BMI and the ED of the patient during surgeries with iCT. (
Figure 6) This results from a personalized scan protocol in which the radiation dose is dependent on age, height, weight, and surgery level of the patient. Furthermore, the surgeon can choose to use the full proposed dose, to halve the proposed radiation dose, or to minimize the radiation output to 25% of the proposed radiation dose [
20]. This choice often depends on the body composition of the patient, since abdominal fat is negatively correlated with image quality [
29,
30]. In contrast, a C-arm fluoroscope only contains a low-, medium-, and high-dose mode which can be selected to adapt image quality. However, the radiation output of a C-arm fluoroscope is mainly dependent on the fluoroscopy time, which is controlled by the surgeon and might be biased by the surgeon’s experience or the complexity of the case [
22].
Surgeries performed with iCT lasted approximately 90 min longer on average than MI-PLIF procedures performed with C-arm fluoroscopy, including an average of 42 extra minutes for, patient positioning and the insertion of pedicle screws (
Figure 8). Similarly, Hecht et al. reported 30–50 min additional time for instrumentation with iCT set-up and navigation, including 18–34 min extra surgical time with iCT navigation [
25]. A meta-analysis, comparing computer-assisted and fluoroscopy-guided surgery confirmed a longer total operative time but reported a reduced thoracic pedicle screw insertion time, compared to fluoroscopy-guided surgeries [
31]. Several factors associated with iCT can increase the duration of the surgery. First, iCT is a newly developed technique and is associated with a steep learning curve [
25]. In contrast, surgeons are experienced in using C-arm fluoroscopy as the golden standard during image-guided surgeries. Although reports, investigating the learning curve of iCT are sparse, it has been hypothesized that surgeons with image-guidance skills merely need five cases to obtain sufficient experience with iCT. Furthermore, routine use of iCT and spinal navigation is required to overcome the learning curve [
23,
25]. During this research, iCT was not routinely used by the three neurosurgeons. The installment of the iCT during surgery is more difficult than the installment of the C-arm, due to the weight and positioning of iCT. Other possible influencing factors are disruption or interference with the navigation signal caused by bloodstains on the reflective markers or lightning of the surgery lamp. Retightening and recalibration after loosening of the navigation markers also occurred. A new iCT scan was needed to assure accurate navigation if the reference array for navigation loosened or moved [
24].
Our study has some limitations. Firstly, there was a significant difference between the iCT and the C-arm fluoroscopy group in terms of the surgeon who performed the MI-PLIF procedures. Patients were not randomized but were divided between the two groups, based on the surgeon’s preference. This was carried out because of the novelty of the iCT in our institution and the steep learning curve the surgeons experienced. Surgeon 1 mainly performed MI-PLIF procedures with iCT, while surgeon 3 only performed one surgery with iCT. Since the surgeons have unequal experience, it might have biased our group results and the time-efficiency results. On the other hand, the three surgeons are trained in radiation protection, and the final patient groups were balanced. Therefore, we believe our final results are valid. The AIRO iCT and spinal navigation present some limitations. Bugs in the software sometimes caused the need to restart the iCT device during surgery. Furthermore, operating room staff often had difficulties with calibration steps or scanning because of insufficient training. These events prolonged the surgery time and should be taken into account for the further clinical implementation of the iCT technique.
iCT promises a long-term benefit for the operating room staff by significantly decreasing radiation exposure. In order to implement this new technology, the cost/benefit ratio of iCT must be discussed and compared to other 3D navigation systems. Navigation systems are associated with higher costs.


 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}