
Regenerative Healing of Chitosan Scaffold Impregnated with Simvastatin in Repairing Furcal Perforation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size Estimation
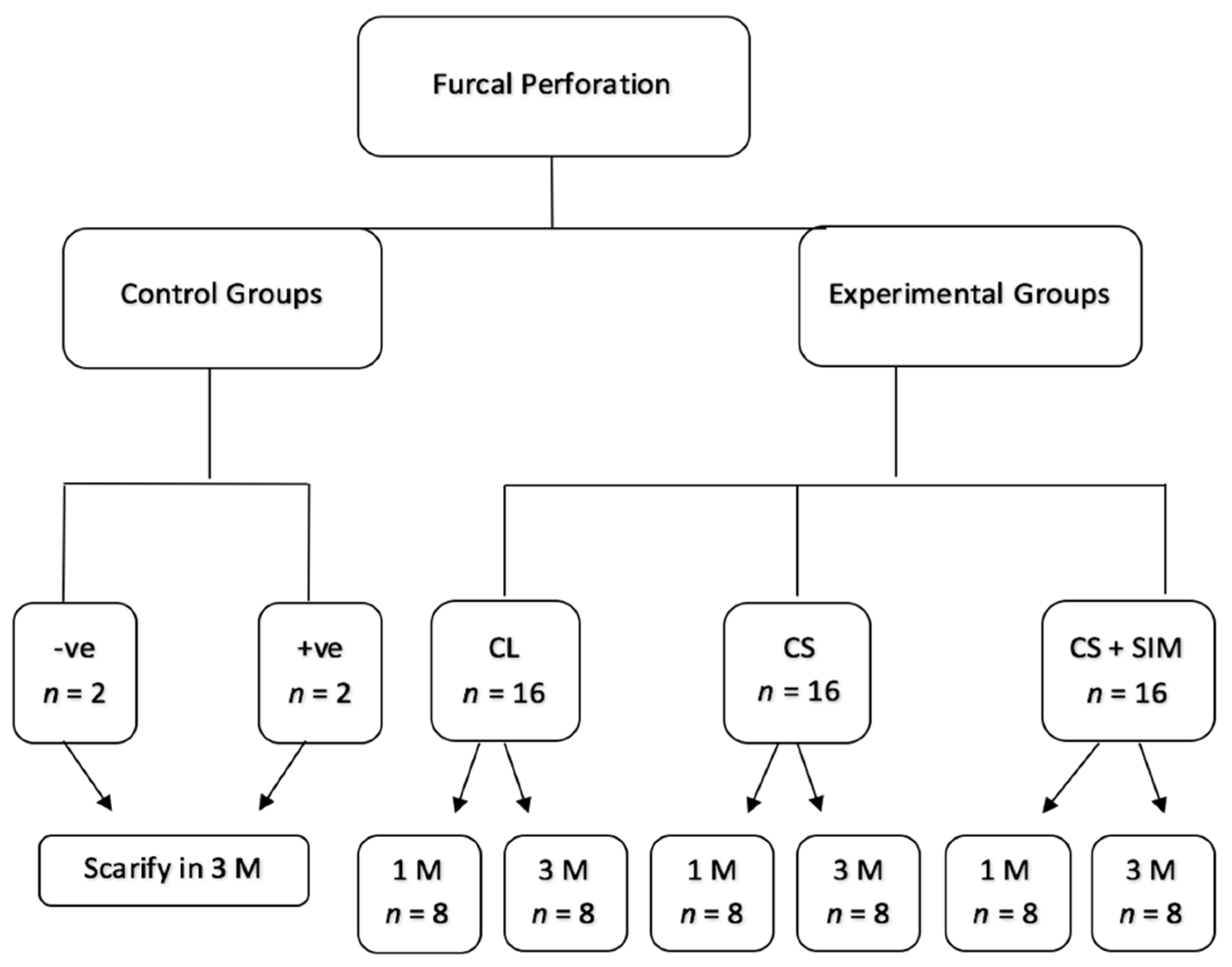
2.2. Sample Selection, Animal Preparation, Randomization, and Grouping
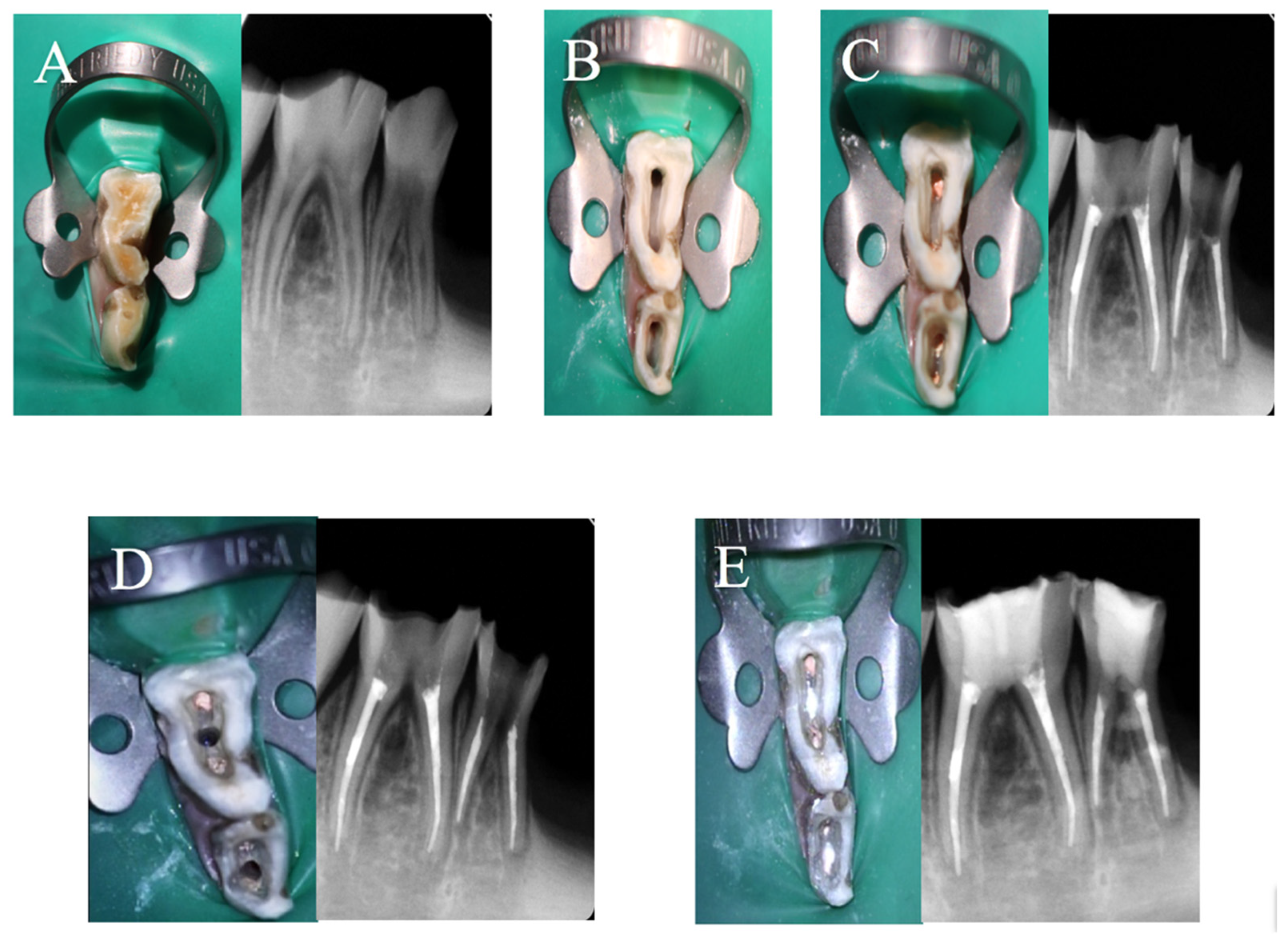
2.3. Operative Procedure
- Group 1: Negative control. No perforation was created in the pulp chamber after finishing the root canal filling. The access cavity was left open without coronal filling;
- Group 2: Positive control. The furcal perforation and access cavity were left open without coronal filling;
- Group 3: CollaCote (CollaCote®; Zimmer, Warsaw, IN, USA). CL was placed in the furcal perforation then white MTA (ProRoot MTA; Dentsply Tulsa Dental Specialties, Johnson City, TN, USA) mixed with sterile saline (3 parts powder to 1 part liquid) was carried into the furcal site with amalgam carrier and compacted with a size 1 Buchanan hand plugger with light pressure, followed by a 2–3 mm resin-modified glass ionomer (GC Fuji II LC Capsule; GC Corporation, Tokyo, Japan);
- Group 4: Chitosan. CS scaffold with no SIM was placed in the furcal perforation site then the same procedure was repeated as in group 3;
- Group 5: Chitosan scaffold impregnated with SIM was placed in the furcal site, then the same procedure was repeated as in group 3. Group distribution is illustrated in Figure 1.
2.4. Sample Preparation
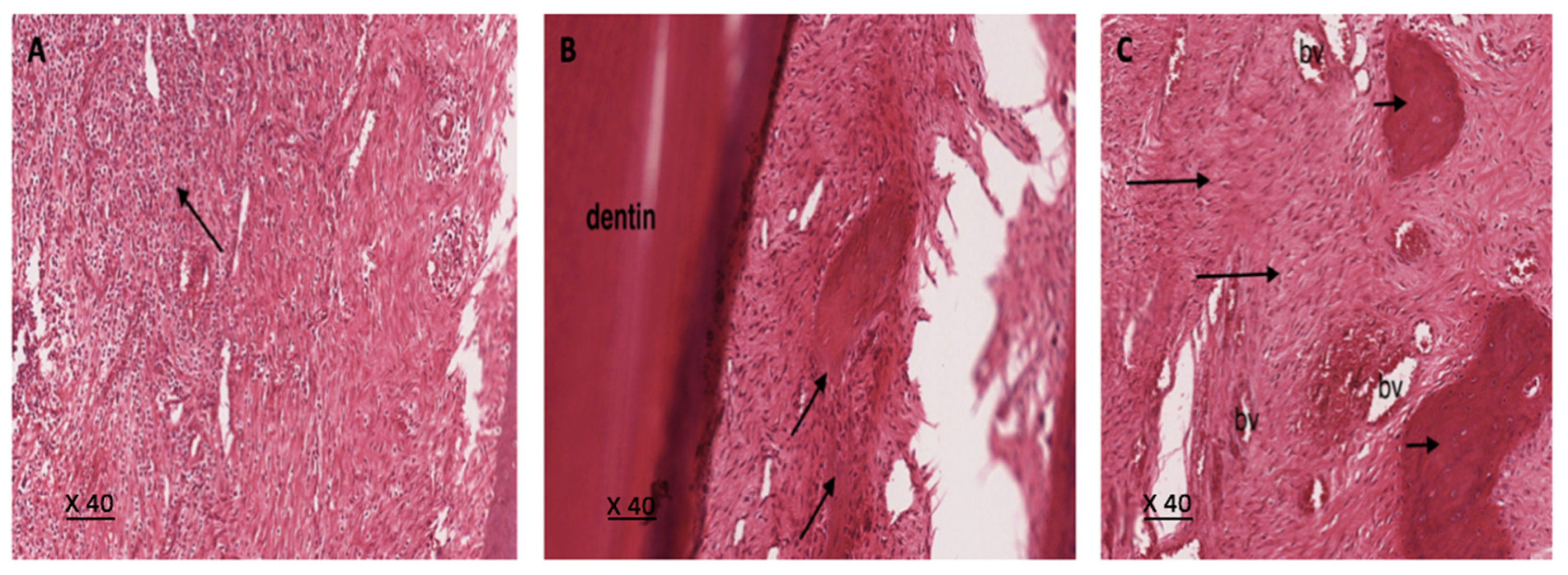
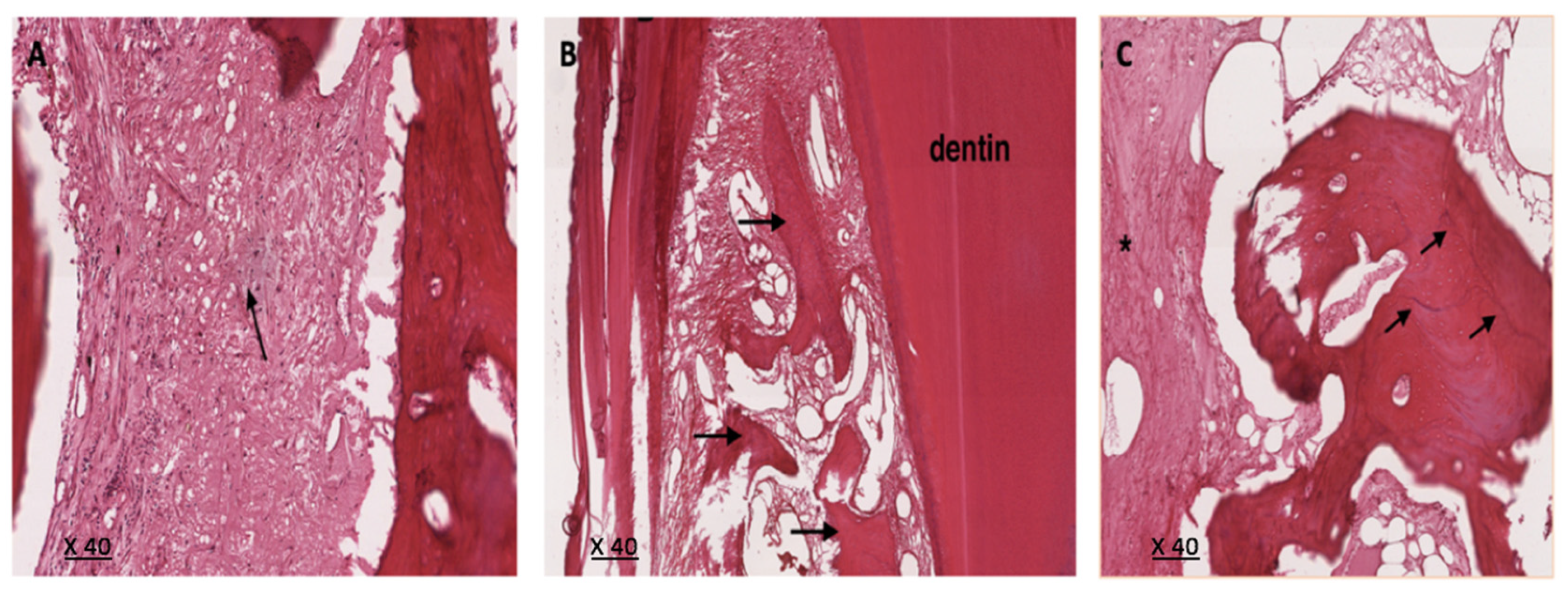
2.5. Histological Examination
- The inflammation quantification by counting the ratio of inflammatory cells in 100 cells under the high-power magnification (×400) and scored as follows [25]:
- Score 0: <10%;
- Score 1: 10–30%;
- Score 2: 30–50%;
- Score 3: >50%.
- Bone formation was marked with the presence or absence of osteoid cells;
- The osteoclastic activity was marked as absent or present;
- Foreign body reaction was marked with the presence or absence of macrophages or giant cells;
- Granulation tissue was marked as absent or present.
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alhadainy, H.A.; Himel, V.T. An In Vitro Evaluation of Plaster of Paris Barriers Used Under Amalgam and Glass Ionomer to Repair Furcation Perforations. J. Endod. 1994, 20, 449–452. [Google Scholar] [CrossRef]
- Seltzer, S.; Sinai, I.; August, D. Periodontal Effects of Root Perforations Before and During Endodontic Procedures. J. Dent. Res. 1970, 49, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.W.; Toth, J.M.; Berzins, D.W.; Charlton, D.G. Mineral Trioxide Aggregate Material Use in Endodontic Treatment: A Review of The Literature. Dent. Mater. 2008, 24, 149–164. [Google Scholar] [CrossRef] [Green Version]
- Baek, S.H.; Plenk, H., Jr.; Kim, S. Periapical Tissue Responses and Cementum Regeneration with Amalgam, SuperEBA, and MTA as Root-End Filling Materials. J. Endod. 2005, 31, 444–449. [Google Scholar] [CrossRef] [Green Version]
- Maltezos, C.; Glickman, G.N.; Ezzo, P.; He, J. Comparison of The Sealing of Resilon, Pro Root MTA, and Super-EBA as Root-End Filling Materials: A Bacterial Leakage Study. J. Endod. 2006, 32, 324–327. [Google Scholar] [CrossRef]
- Cohen, S.; Burns, R.C. Pathways of The Pulp, 2nd ed.; Mosby: St. Louis, MO, USA, 1980; pp. 106–108. [Google Scholar]
- Tsesis, I.; Fuss, Z. Diagnosis and Treatment of Accidental Root Perforations. Endod. Top. 2006, 13, 95–107. [Google Scholar] [CrossRef]
- Al-Daafas, A.; Al-Nazhan, S. Histological Evaluation of Contaminated Furcal Perforation in Dogs’ Teeth Repaired by MTA With or Without Internal Matrix. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, 92–99. [Google Scholar] [CrossRef]
- Lemon, R.R. Nonsurgical Repair of Perforation Defects. Internal Matrix Concept. Dent. Clin. N. Am. 1992, 36, 439–457. [Google Scholar] [PubMed]
- Rafter, M.; Baker, M.; Alves, M.; Daniel, J.; Remeikis, N. Evaluation of Healing with Use of an Internal Matrix to Repair Furcation Perforations. Int. Endod. J. 2002, 35, 775–783. [Google Scholar] [CrossRef]
- Li, Q.; Dunn, E.T.; Grandmaison, E.W.; Goosen, M.F.A. Applications and Properties of Chitosan. J. Bioact Compat Polym. 1992, 7, 370–397. [Google Scholar] [CrossRef]
- Kim, I.Y.; Seo, S.J.; Moon, H.S.; Yoo, M.K.; Park, I.Y.; Kim, B.C.; Cho, C.S. Chitosan and its Derivatives for Tissue Engineering Applications. Biotechnol. Adv. 2008, 26, 1–21. [Google Scholar] [CrossRef]
- Soares, D.; Anovazzi, G.; Bordini, E.A.F.; Zuta, U.O.; Leite, M.L.A.S.; Basso, F.G.; Hebling, J.; Costa, C.A.D.S. Biological Analysis of Simvastatin-releasing Chitosan Scaffold as a Cell-free System for Pulp-dentin Regeneration. J. Endod. 2018, 44, 971–976.e1. [Google Scholar] [CrossRef] [Green Version]
- Suresh, N.; Subbarao, H.J.; Natanasabapathy, V.; Kishen, A. Maxillary Anterior Teeth with Extensive Root Resorption Treated with Low-level Light-activated Engineered Chitosan Nanoparticles. J. Endod. 2021, 47, 1182–1190. [Google Scholar] [CrossRef]
- Schachter, M. Chemical, Pharmacokinetic and Pharmacodynamic Properties of Statins: An Update. Fundam. Clin. Pharmacol. 2004, 19, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Mundy, G.; Garrett, R.; Harris, S.; Chan, J.; Chen, D.; Rossini, G.; Boyce, B.; Zhao, M.; Gutierrez, G. Stimulation of Bone Formation in Vitro and in Rodents by Statins. Science 1999, 286, 1946–1949. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Lu, Z.; Zhang, X.; Yu, H.; Kirkwood, K.L.; Lopes-Virella, M.F.; Huang, Y. Metabolic syndrome exacerbates inflammation and bone loss in periodontitis. J. Dent. Res. 2015, 94, 362–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loesche, W.J.; Grossman, N.S. Periodontal disease as a specific, albeit chronic, infection: Diagnosis and treatment. Clin. Microbiol. Rev. 2001, 14, 727–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patini, R.; Gallenzi, P.; Spagnuolo, G.; Cordaro, M.; Cantiani, M.; Amalfitano, A.; Arcovito, A.; Callà, C.; Mingrone, G.; Nocca, G. Correlation Between Metabolic Syndrome, Periodontitis and Reactive Oxygen Species Production. A Pilot Study. Open Dent. J. 2017, 11, 621–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, I.S.; Jeong, B.C.; Kim, O.S.; Kim, Y.J.; Lee, S.E.; Lee, K.N.; Koh, J.T.; Chung, H.J. Lactone Form 3-hydroxy-3-methylglutaryl-coenzyme A Reductase Inhibitors (Statins) Stimulate the Osteoblastic Differentiation of Mouse Periodontal Ligament Cells Via the ERK Pathway. J. Periodontal Res. 2011, 46, 204–213. [Google Scholar] [CrossRef]
- Muniz, F.W.M.G.; Taminski, K.; Cavagni, J.; Celeste, R.K.; Weidlich, P.; Rösing, C.K. The Effect of Statins on Periodontal Treatment- A Systematic Review with Meta-Analyses and Meta-Regression. Clin. Oral Investig. 2018, 22, 671–687. [Google Scholar] [CrossRef]
- Implant Support Services. Available online: https://www.implant.co.za/our-products/membranes-and-bone-products/zimmer-colla-plug/ (accessed on 1 September 2021).
- Alsawah, G.M.; Al-Obaida, M.I.; Al-Madi, E.M. Effect of a Simvastatin-Impregnated Chitosan Scaffold on Cell Growth and Osteoblastic Differentiation. Appl. Sci. 2021, 11, 5346. [Google Scholar] [CrossRef]
- Hau, J.; Schapiro, S.J. Handbook of Laboratory Animal Science Volume I Essential Principles and Practices, 3rd ed.; CRC Press: Boca Raton, FL, USA, 2010. [Google Scholar]
- Salman, M.A.; Quinn, F.; Dermody, J.; Hussey, D.; Claffey, N. Histological Evaluation of Repair Using a Bioresorbable Membrane Beneath a Resin-Modified Glass Ionomer After Mechanical Furcation Perforation in Dogs’ Teeth. J. Endod. 1999, 25, 181–186. [Google Scholar] [CrossRef]
- Chen, L.; Deng, H.; Cui, H.; Fang, J.; Zuo, Z.; Deng, J.; Li, Y.; Wang, X.; Zhao, L. Inflammatory Responses and Inflammation-Associated Diseases in Organs. Oncotarget 2018, 9, 7204–7218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noetzel, J.; Ozer, K.; Reisshauer, B.H.; Anil, A.; Rössler, R.; Neumann, K.; Kielbassa, A.M. Tissue Responses to an Experimental Calcium Phosphate Cement and Mineral Trioxide Aggregate as Materials for Furcation Perforation Repair: A Histological Study in Dogs. Clin. Oral Investig. 2006, 10, 77–83. [Google Scholar] [CrossRef]
- Bakhtiar, H.; Mirzaei, H.; Bagheri, M.R.; Fani, N.; Mashhadiabbas, F.; Eslaminejad, M.B.; Sharifi, D.; Nekoofar, M.H.; Dummer, P. Histologic Tissue Response to Furcation Perforation Repair Using Mineral Trioxide Aggregate or Dental Pulp Stem Cells Loaded onto Treated Dentin Matrix or Tricalcium Phosphate. Clin. Oral Investig. 2017, 21, 1579–1588. [Google Scholar] [CrossRef] [Green Version]
- Tatullo, M.; Spagnuolo, G.; Codispoti, B.; Zamparini, F.; Zhang, A.; Espoti, M.D.; Aparicio, C.; Rengo, C.; Nuzzolese, M.; Manzoli, L.; et al. PLA-Based Mineral-Doped Scaffolds Seeded with Human Periapical Cyst-Derived MSCs: A Promising Tool for Regenerative Healing in Dentistry. Materials 2019, 12, 597. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Tian, X.; Fan, J.; Tong, H.; Ao, Q.; Wang, X. Chitosans for Tissue Repair and Organ Three-Dimensional (3D) Bioprinting. Micromachines 2019, 10, 765. [Google Scholar] [CrossRef] [Green Version]
- Palma, P.J.; Ramos, J.C.; Martins, J.B.; Diogenes, A.; Figueiredo, M.H.; Ferreira, P.; Viegas, C.; Santos, J.M. Histologic Evaluation of Regenerative Endodontic Procedures with the Use of Chitosan Scaffolds in Immature Dog Teeth with Apical Periodontitis. J. Endod. 2017, 43, 1279–1287. [Google Scholar] [CrossRef]
- Jayash, S.N.; Hashim, N.M.; Misran, M.; Ibrahim, N.; Al-Namnam, N.M.; Baharuddin, N.A. Analysis on Efficacy of Chitosan-Based Gel on Bone Quality and Quantity. Front. Mater. 2021, 8, 640950. [Google Scholar] [CrossRef]
- Wong, R.W.K.; Rabie, A.B.M. Statin Collagen Grafts Used to Repair Defects in The Parietal Bone of Rabbits. Br. J. Oral. Maxillofac. Surg. 2003, 41, 244–248. [Google Scholar] [CrossRef]
- Ilker, Ö.; Erdem, K.; Cesur, G.; Fahrettin, G. Effect of Local Simvastatin Application on Mandibular Defects. J. Craniofac. Surg. 2007, 18, 546–550. [Google Scholar]
- Ayukawa, Y.; Okamura, A.; Koyano, K. Simvastatin Promotes Osteogenesis Around Titanium Implants. Clin. Oral Implants Res. 2004, 15, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Schmid, M.J.; Marx, D.B.; Beatty, M.W.; Diane, M.C.; Collins, M.E.; Reinhardt, R.A. The Effect of Local Simvastatin Delivery Strategies on Mandibular Bone Formation in Vivo. Biomaterials 2008, 29, 1940–1949. [Google Scholar] [CrossRef] [Green Version]
- Khosla, S.; Westendorf, J.J.; Oursler, M.J. Building Bone to Reverse Osteoporosis and Repair Fractures. J. Clin. Invest. 2008, 118, 421–428. [Google Scholar] [CrossRef] [Green Version]
- Wong, R.W.K.; Rabie, A.B.M. Histologic and Ultrastructural Study on Statin Graft in Rabbit Skulls. J. Oral Maxillofac. Surg. 2005, 63, 1515–1521. [Google Scholar] [CrossRef]
- Huang, X.; Huang, Z.; Li, W. Highly Efficient Release of Simvastatin from Simvastatin-Loaded Calcium Sulphate Scaffolds Enhances Segmental Bone Regeneration in Rabbits. Mol. Med. Rep. 2014, 9, 2152–2158. [Google Scholar] [CrossRef] [Green Version]
- Murali, V.P.; Guerra, F.D.; Ghardi, N.; Christian, J.M.; Stein, S.H.; Jennings, J.A.; Smith, R.A.; Bumgardner, J.D. Simvastatin loaded chitosan guided bone regeneration membranes stimulate bone healing. J. Periodontal Res. 2021, 56, 877–884. [Google Scholar] [CrossRef]
- Weis, M.; Heeschen, C.; Glassford, A.J.; Cooke, J.P. Statins Have Biphasic Effects on Angiogenesis. Circulation 2002, 105, 739–745. [Google Scholar] [CrossRef] [Green Version]
- Wong, R.W.K.; Rabie, A.B.M. Early healing pattern of statin-induced osteogenesis. Br. J. Oral. Maxillofac. Surg. 2005, 43, 46–50. [Google Scholar] [CrossRef]
- Thylin, M.R.; McConnell, J.C.; Schmid, M.J.; Reckling, R.R.; Ojha, J.; Bhattacharyya, I.; Marx, D.B.; Reinhardt, R.A. Effects of Simvastatin Gels on Murine Calvarial Bone. J. Periodontol. 2002, 73, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.; Lee, Y.; Schmid, M.J.; Killpack, B.; Genrich, M.A.; Narayana, N.; Marx, D.B.; Cullen, D.M.; Reinhardt, R.A. Local Simvastatin Effects on Mandibular Bone Growth and Inflammation. J. Periodontol. 2005, 76, 1861–1870. [Google Scholar] [CrossRef] [Green Version]
- Pullisaar, H.; Reseland, J.E.; Haugen, H.J.; Brinchmann, J.E.; Ostrup, E. Simvastatin Coating of TiO₂ Scaffold Induces Osteogenic Differentiation of Human Adipose Tissue-Derived Mesenchymal Stem Cells. Biochem. Biophys. Res. Commun. 2014, 447, 139–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.S.; Ou, M.E.; Liu, H.; Gu, M.; Lv, L.W.; Fan, C.; Chen, T.; Zhao, X.H.; Jin, C.Y.; Zhang, X.; et al. The Effect of Simvastatin on Chemotactic Capability of SDF-1α and The Promotion of Bone Regeneration. Biomaterials 2014, 35, 4489–4498. [Google Scholar] [CrossRef]
- Hassanien, E.; A-Seida, A.; Hashem, A.; Khanbash, S. Histologic Evaluation of Furcation Perforation Treated with Mineral Trioxide Aggregate and Bioaggregate. Asian J. Anim. Sci. 2015, 9, 148–156. [Google Scholar] [CrossRef] [Green Version]
- Holland, R.; Bisco Ferreira, L.; de Souza, V.; Otoboni Filho, J.A.; Murata, S.S.; Dezan, E., Jr. Reaction of the lateral periodontium of dogs’ teeth to contaminated and noncontaminated perforations filled with mineral trioxide aggregate. J. Endod. 2007, 33, 1192–1197. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | Group | No. of Specimen | Inflammation Quantification (%) | Presence of Bone Formation (%) | Presence of Osteoclastic Activity (%) | Presence of Foreign Body Reaction (%) | Presence of Granulation Tissue (%) | |||
|---|---|---|---|---|---|---|---|---|---|---|
| <10% | 10–30% | 30–50% | >50% | |||||||
| +ve control | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| CL | 8 | 88 | 0 | 0 | 12 | 0 | 12 | 0 | 12 | |
| 1 Month | CS | 8 | 75 | 25 | 0 | 0 | 50 | 25 | 0 | 0 |
| CS/SIM | 4 | 50 | 50 | 0 | 0 | 50 | 100 | 0 | 0 | |
| +ve control | 2 | 50 | 50 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 3 Months | CL | 8 | 50 | 0 | 0 | 50 | 50 | 0 | 25 | 50 |
| CS | 8 | 88 | 0 | 12 | 0 | 12 | 25 | 0 | 12 | |
| CS/SIM | 8 | 72 | 0 | 14 | 14 | 14 | 0 | 0 | 0 | |
| Index | CL (n = 8) | CS (n = 8) | CS with SIM (n = 4) | Kruskal-Wallis Test Results |
|---|---|---|---|---|
| Median (IQR) Range | 0 (0–0.75) 0–5 | 1 (0–2.75) 0–3 | 2.5 (1–4) 1–4 | p = 0.242 |
| Index | CL (n = 8) | CS (n = 8) | CS with SIM (n = 8) | Kruskal-Wallis Test Results |
|---|---|---|---|---|
| Median (IQR) Range | 3 (1–5.75) 1–6 | 0 (0–0) 0–6 | 0 (0–3) 0–4 | p = 0.040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsawah, G.M.; Alsheddi, M.; Al-Madi, E.M.; Al-Obaida, M.I. Regenerative Healing of Chitosan Scaffold Impregnated with Simvastatin in Repairing Furcal Perforation. Appl. Sci. 2021, 11, 8992. https://doi.org/10.3390/app11198992
Alsawah GM, Alsheddi M, Al-Madi EM, Al-Obaida MI. Regenerative Healing of Chitosan Scaffold Impregnated with Simvastatin in Repairing Furcal Perforation. Applied Sciences. 2021; 11(19):8992. https://doi.org/10.3390/app11198992
Chicago/Turabian StyleAlsawah, Ghaliah M., Manal Alsheddi, Ebtissam M. Al-Madi, and Mohammad I. Al-Obaida. 2021. "Regenerative Healing of Chitosan Scaffold Impregnated with Simvastatin in Repairing Furcal Perforation" Applied Sciences 11, no. 19: 8992. https://doi.org/10.3390/app11198992