
Effect of the Passive Ultrasonic Irrigation and the Apical Diameter Size on the Debridement Efficacy of Infected Root Canals: A Multivariate Statistical Assessment of Histological Data

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Study Groups
2.3. Instrumentation Procedures
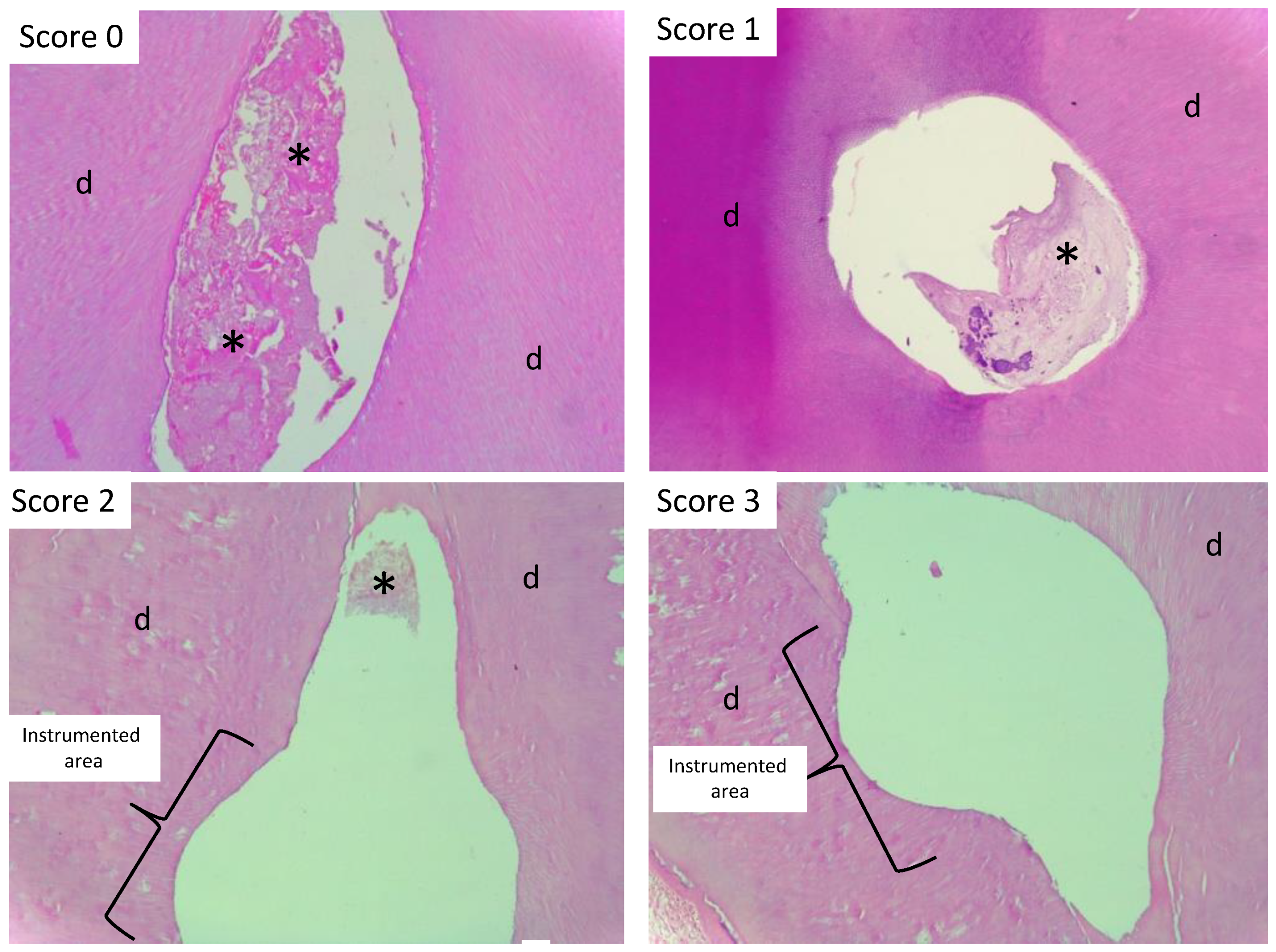
2.4. Histological Procedures and Organic Remnant Analysis
2.5. Statistical Analyses
3. Results
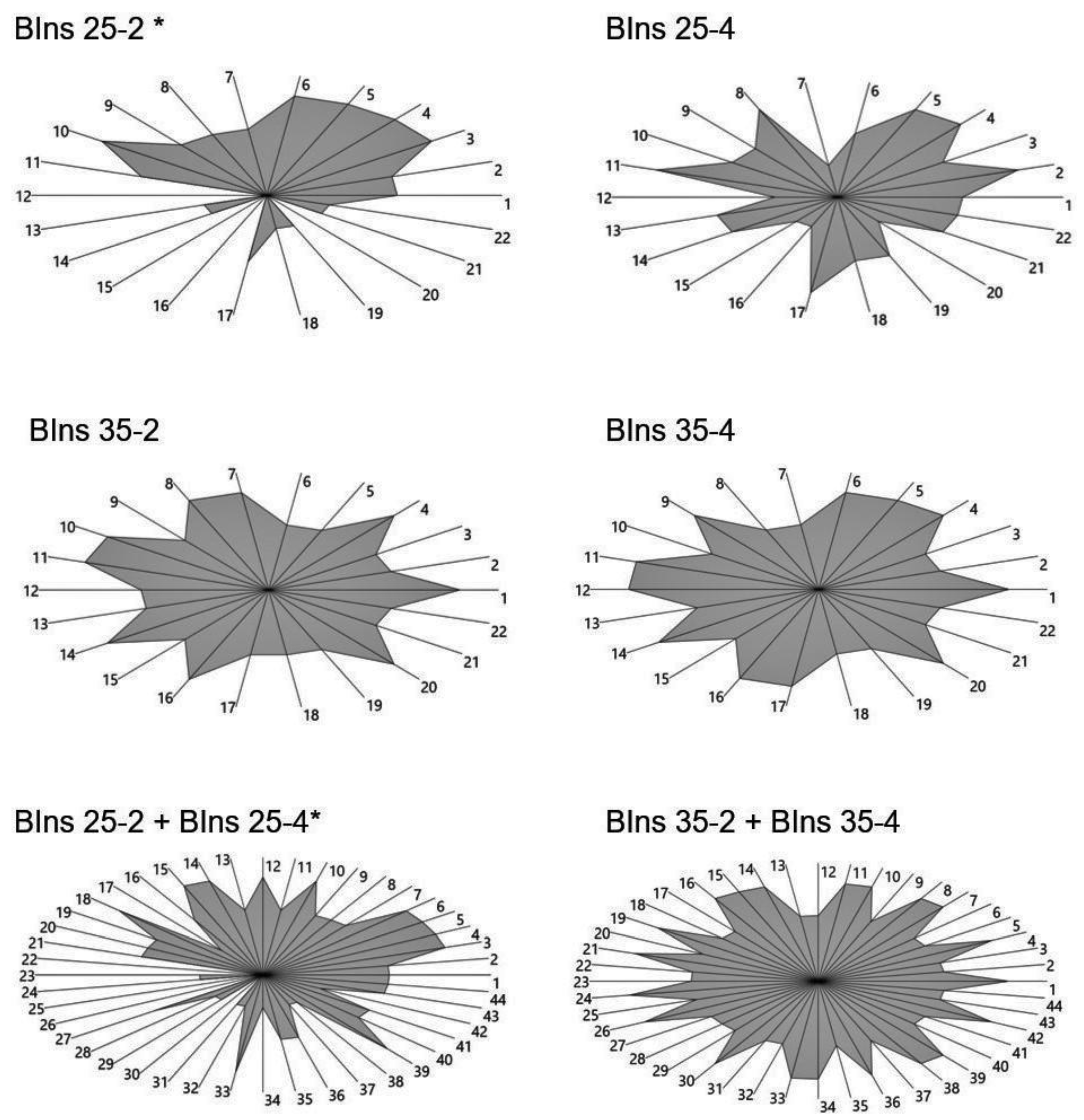
3.1. Effect of PUI on the Organic Remnant Removal Regarding the Instrumentation with Different Diameters
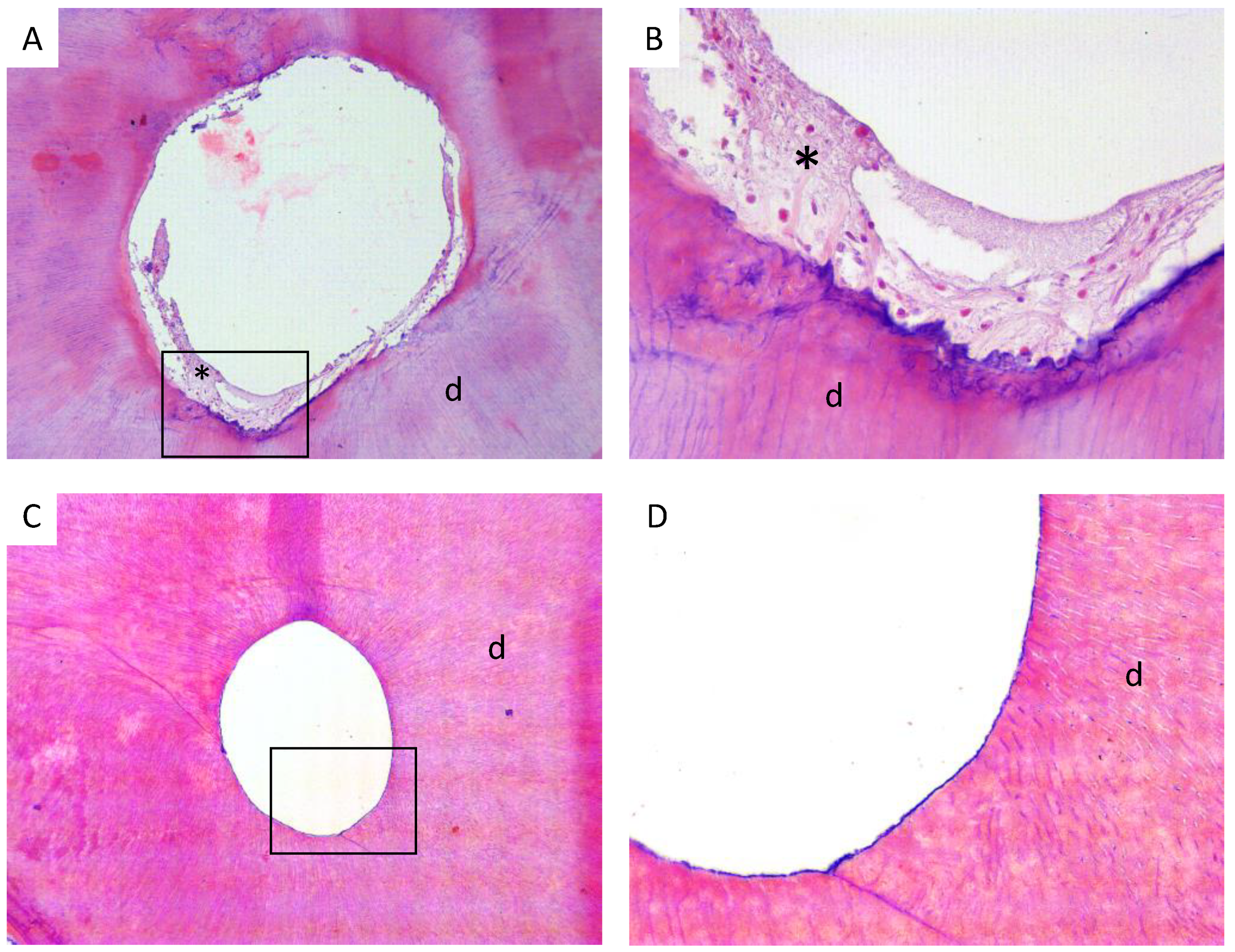
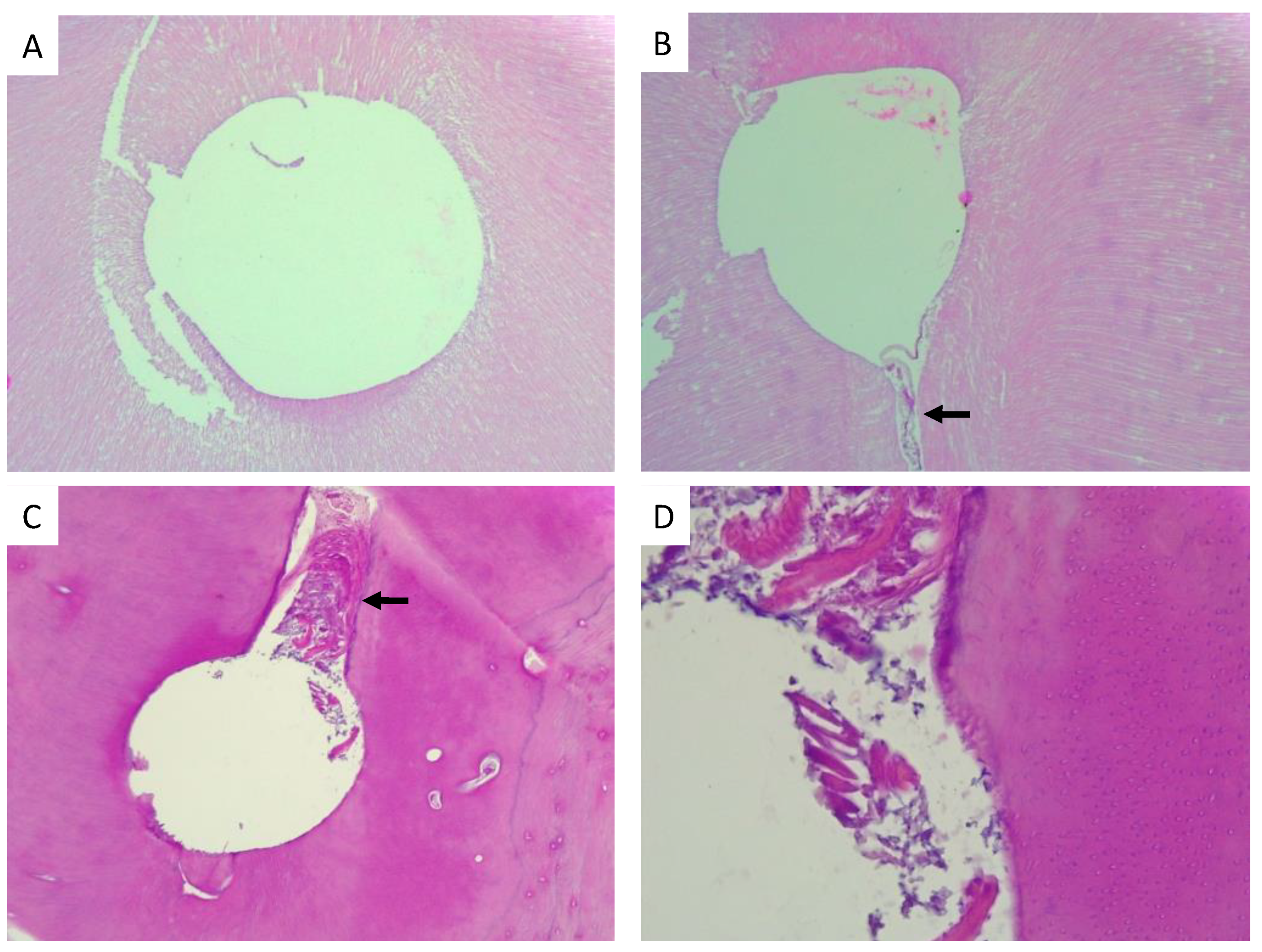
3.2. Effect of PUI and the Diameter of Endodontic Instruments for Biomechanical Removal on Teeth Cleanness
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cesario, F.; Hungaro Duarte, M.A.; Duque, J.A.; Alcalde, M.P.; de Andrade, F.B.; Reis So, M.V.; De Vasconcelos, B.C.; Vivan, R.R. Comparisons by microcomputed tomography of the efficiency of different irrigation techniques for removing dentinal debris from artificial grooves. J. Conserv. Dent. 2018, 21, 383–387. [Google Scholar] [CrossRef]
- Dioguardi, M.; Di Gioia, G.; Illuzzi, G.; Laneve, E.; Cocco, A.; Troiano, G. Endodontic irrigants: Different methods to improve efficacy and related problems. Eur. J. Dent. 2018, 12, 459–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozo, S.; Llena, C.; Forner, L. Review of ultrasonic irrigation in endodontics: Increasing action of irrigating solutions. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e512–e516. [Google Scholar] [CrossRef] [Green Version]
- Kumar, T.; Dhillon, J.S.; Gill, G.S.; Singla, R.; Rani, S.; Dhillon, M. An in vitro comparison of the antimicrobial efficacy of positive pressure and negative pressure irrigation techniques in root canals infected with Enterococcus faecalis. J. Conserv. Dent. 2018, 21, 438–442. [Google Scholar] [CrossRef]
- Baugh, D.; Wallace, J. The role of apical instrumentation in root canal treatment: A review of the literature. J. Endod. 2005, 31, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, B.T.; Messer, H.H. The effect of instrument type and preflaring on apical file size determination. Int. Endod. J. 2002, 35, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr.; Lima, K.C.; Magalhaes, F.A.; Lopes, H.P.; de Uzeda, M. Mechanical reduction of the bacterial population in the root canal by three instrumentation techniques. J. Endod. 1999, 25, 332–335. [Google Scholar] [CrossRef]
- Waltimo, T.M.; Orstavik, D.; Siren, E.K.; Haapasalo, M.P. In vitro yeast infection of human dentin. J. Endod. 2000, 26, 207–209. [Google Scholar] [CrossRef]
- Berkiten, M.; Okar, I.; Berkiten, R. In vitro study of the penetration of Streptococcus sanguis and Prevotella intermedia strains into human dentinal tubules. J. Endod. 2000, 26, 236–239. [Google Scholar] [CrossRef]
- Srikanth, P.; Krishna, A.G.; Srinivas, S.; Reddy, E.S.; Battu, S.; Aravelli, S. Minimal Apical Enlargement for Penetration of Irrigants to the Apical Third of Root Canal System: A Scanning Electron Microscope Study. J. Int. Oral Health 2015, 7, 92–96. [Google Scholar]
- Reddy, J.M.; Latha, P.; Gowda, B.; Manvikar, V.; Vijayalaxmi, D.B.; Ponangi, K.C. Smear layer and debris removal using manual Ni-Ti files compared with rotary Protaper Ni-Ti files—An In-Vitro SEM study. J. Int. Oral Health 2014, 6, 89–94. [Google Scholar] [PubMed]
- Brunson, M.; Heilborn, C.; Johnson, D.J.; Cohenca, N. Effect of apical preparation size and preparation taper on irrigant volume delivered by using negative pressure irrigation system. J. Endod. 2010, 36, 721–724. [Google Scholar] [CrossRef] [PubMed]
- van der Sluis, L.W.; Versluis, M.; Wu, M.K.; Wesselink, P.R. Passive ultrasonic irrigation of the root canal: A review of the literature. Int. Endod. J. 2007, 40, 415–426. [Google Scholar] [CrossRef] [PubMed]
- van der Sluis, L.W.; Shemesh, H.; Wu, M.K.; Wesselink, P.R. An evaluation of the influence of passive ultrasonic irrigation on the seal of root canal fillings. Int. Endod. J. 2007, 40, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.J.; Chivatxaranukul, P.; Parashos, P.; Messer, H.H. The effect of ultrasonically activated irrigation on reduction of Enterococcus faecalis in experimentally infected root canals. Int. Endod. J. 2010, 43, 968–977. [Google Scholar] [CrossRef] [PubMed]
- Freire, L.G.; Iglecias, E.F.; Cunha, R.S.; Dos Santos, M.; Gavini, G. Micro-Computed Tomographic Evaluation of Hard Tissue Debris Removal after Different Irrigation Methods and Its Influence on the Filling of Curved Canals. J. Endod. 2015, 41, 1660–1666. [Google Scholar] [CrossRef] [PubMed]
- Leoni, G.B.; Versiani, M.A.; Silva-Sousa, Y.T.; Bruniera, J.F.; Pecora, J.D.; Sousa-Neto, M.D. Ex vivo evaluation of four final irrigation protocols on the removal of hard-tissue debris from the mesial root canal system of mandibular first molars. Int. Endod. J. 2017, 50, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Lee, O.Y.S.; Khan, K.; Li, K.Y.; Shetty, H.; Abiad, R.S.; Cheung, G.S.P.; Neelakantan, P. Influence of apical preparation size and irrigation technique on root canal debridement: A histological analysis of round and oval root canals. Int. Endod. J. 2019, 52, 1366–1376. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef]
- Langeland, K.; Liao, K.; Pascon, E.A. Work-saving devices in endodontics: Efficacy of sonic and ultrasonic techniques. J. Endod. 1985, 11, 499–510. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Araujo, M.C.; Garcia, P.F.; Fraga, R.C.; Dantas, C.J. Histological evaluation of the effectiveness of five instrumentation techniques for cleaning the apical third of root canals. J. Endod. 1997, 23, 499–502. [Google Scholar] [CrossRef]
- Goerg, S.J.; Kaiser, J. Nonparametric Testing of Distributions—The Epps—Singleton Two-Sample Test using the Empirical Characteristic Function. Stata. J. 2009, 3, 454–465. [Google Scholar] [CrossRef] [Green Version]
- Clarke, K.R. Nonparametric Multivariate Analyses of Changes in Community Structure. Austral Ecol. 1993, 18, 117–143. [Google Scholar] [CrossRef]
- Hammer, O.; Harper, D.A.T.; Ryan, P.D. PAST: Paleontological Statistics Software Package for Education and Data Analysis. Palaeontol. Electron. 2001, 4, e9. [Google Scholar]
- Rodrigues, R.C.V.; Zandi, H.; Kristoffersen, A.K.; Enersen, M.; Mdala, I.; Orstavik, D.; Rocas, I.N.; Siqueira, J.F., Jr. Influence of the Apical Preparation Size and the Irrigant Type on Bacterial Reduction in Root Canal-treated Teeth with Apical Periodontitis. J. Endod. 2017, 43, 1058–1063. [Google Scholar] [CrossRef]
- Usman, N.; Baumgartner, J.C.; Marshall, J.G. Influence of instrument size on root canal debridement. J. Endod. 2004, 30, 110–112. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, L.J.; Baumgartner, J.C.; Marshall, J.G. Evaluation of apical debris removal using various sizes and tapers of ProFile GT files. J. Endod. 2004, 30, 425–428. [Google Scholar] [CrossRef] [PubMed]
- Dalton, B.C.; Orstavik, D.; Phillips, C.; Pettiette, M.; Trope, M. Bacterial reduction with nickel-titanium rotary instrumentation. J. Endod. 1998, 24, 763–767. [Google Scholar] [CrossRef]
- Plotino, G.; Grande, N.M.; Tocci, L.; Testarelli, L.; Gambarini, G. Influence of Different Apical Preparations on Root Canal Cleanliness in Human Molars: A SEM Study. J. Oral Maxillofac. Res. 2014, 5, e4. [Google Scholar] [CrossRef] [Green Version]
- Xu, K.; Wang, J.; Wang, K.; Gen, N.; Li, J. Micro-computed tomographic evaluation of the effect of the final apical size prepared by rotary nickel-titanium files on the removal efficacy of hard-tissue debris. J. Int. Med. Res. 2018, 46, 2219–2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paque, F.; Musch, U.; Hulsmann, M. Comparison of root canal preparation using RaCe and ProTaper rotary Ni-Ti instruments. Int. Endod. J. 2005, 38, 8–16. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Instrument Size (#-mm from Apex) | Epps-Singleton W2 | p Value (Same Distance) |
|---|---|---|
| 25-2 | 43.58 | 7.84 × 10−9 |
| 25-4 | 1.39 | 0.8460 |
| 35-2 | 0.40 | 0.9823 |
| 35-4 | 3.24 × 10−16 | 1 |
| 25 (2, 4) | 21.10 | 3 × 10−4 |
| 35 (2, 4) | 0.22 | 0.9944 |
| BIns 25-2 | BIns 25-4 | |
|---|---|---|
| BIns 25-4 | 0.9076 | |
| BIns 35-2 | 0.03814 | 0.5247 |
| BIns 35-4 | 0.01547 | 0.1988 |
 | Irrigation System | Diameter of the Instrument (RaCe 0.04 Taper) | ||
| PUI | CI | #25 | #35 | |
| + | – | – | + | |
| + | – | + | – | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alcota, M.; Osorio, J.; Díaz, C.; Ortega-Pinto, A.; Peñafiel, C.; Rivera, J.C.; Salazar, D.; Manríquez, G.; González, F.E. Effect of the Passive Ultrasonic Irrigation and the Apical Diameter Size on the Debridement Efficacy of Infected Root Canals: A Multivariate Statistical Assessment of Histological Data. Appl. Sci. 2021, 11, 7495. https://doi.org/10.3390/app11167495
Alcota M, Osorio J, Díaz C, Ortega-Pinto A, Peñafiel C, Rivera JC, Salazar D, Manríquez G, González FE. Effect of the Passive Ultrasonic Irrigation and the Apical Diameter Size on the Debridement Efficacy of Infected Root Canals: A Multivariate Statistical Assessment of Histological Data. Applied Sciences. 2021; 11(16):7495. https://doi.org/10.3390/app11167495
Chicago/Turabian StyleAlcota, Marcela, Jimena Osorio, Claudia Díaz, Ana Ortega-Pinto, Cristián Peñafiel, Juan C. Rivera, Daniela Salazar, Germán Manríquez, and Fermín E. González. 2021. "Effect of the Passive Ultrasonic Irrigation and the Apical Diameter Size on the Debridement Efficacy of Infected Root Canals: A Multivariate Statistical Assessment of Histological Data" Applied Sciences 11, no. 16: 7495. https://doi.org/10.3390/app11167495