
Cartilage Repair Activity during Joint-Preserving Treatment May Be Accompanied by Osteophyte Formation

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Knee Joint Distraction Patients
2.2. Follow-Up
2.3. High Tibial Osteotomy Patients
2.4. Control Group of Untreated OA Patients
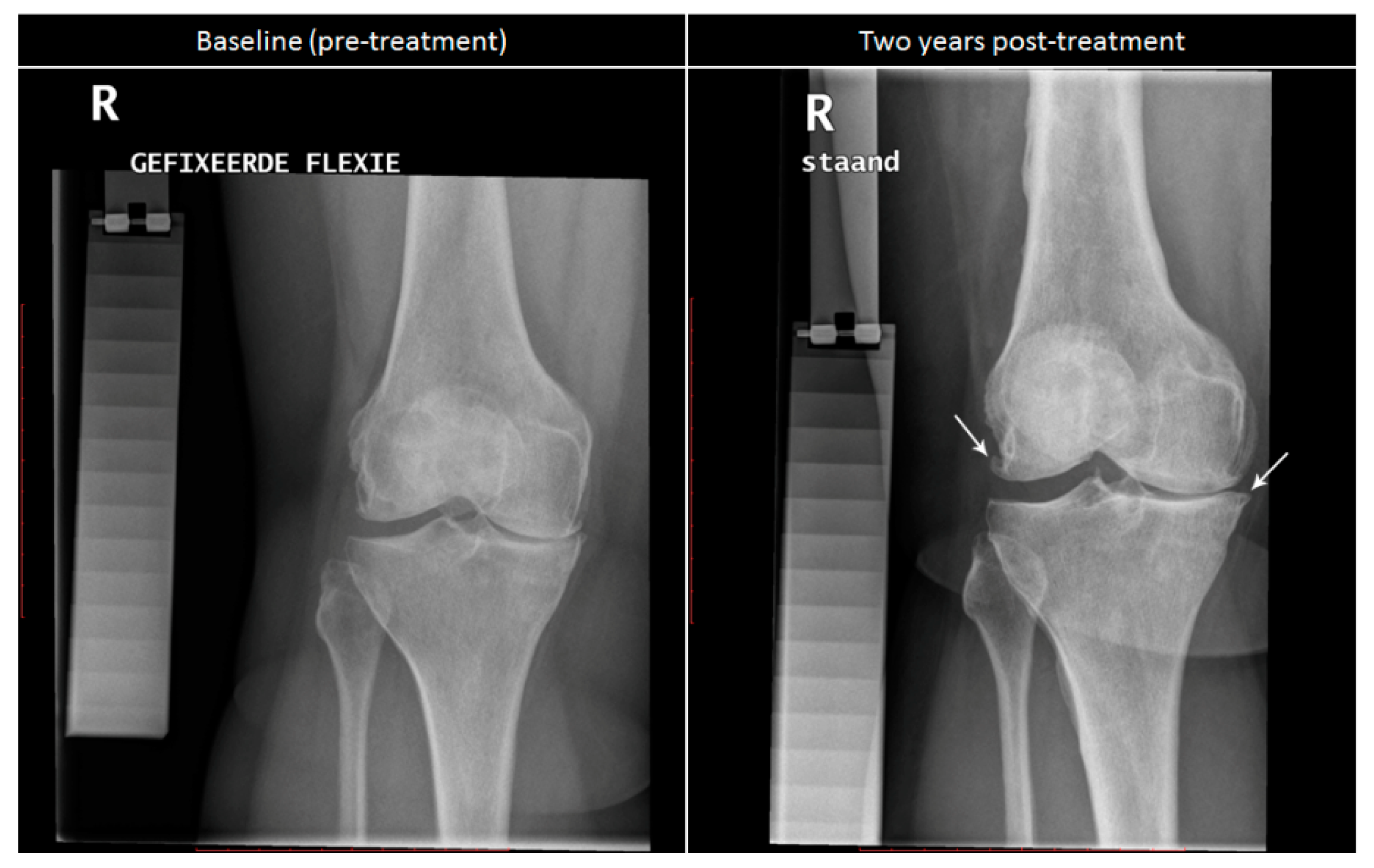
2.5. Radiographic Analysis
2.6. Synovial Fluid Aspirations
2.7. Statistical Analysis
3. Results
3.1. Patients
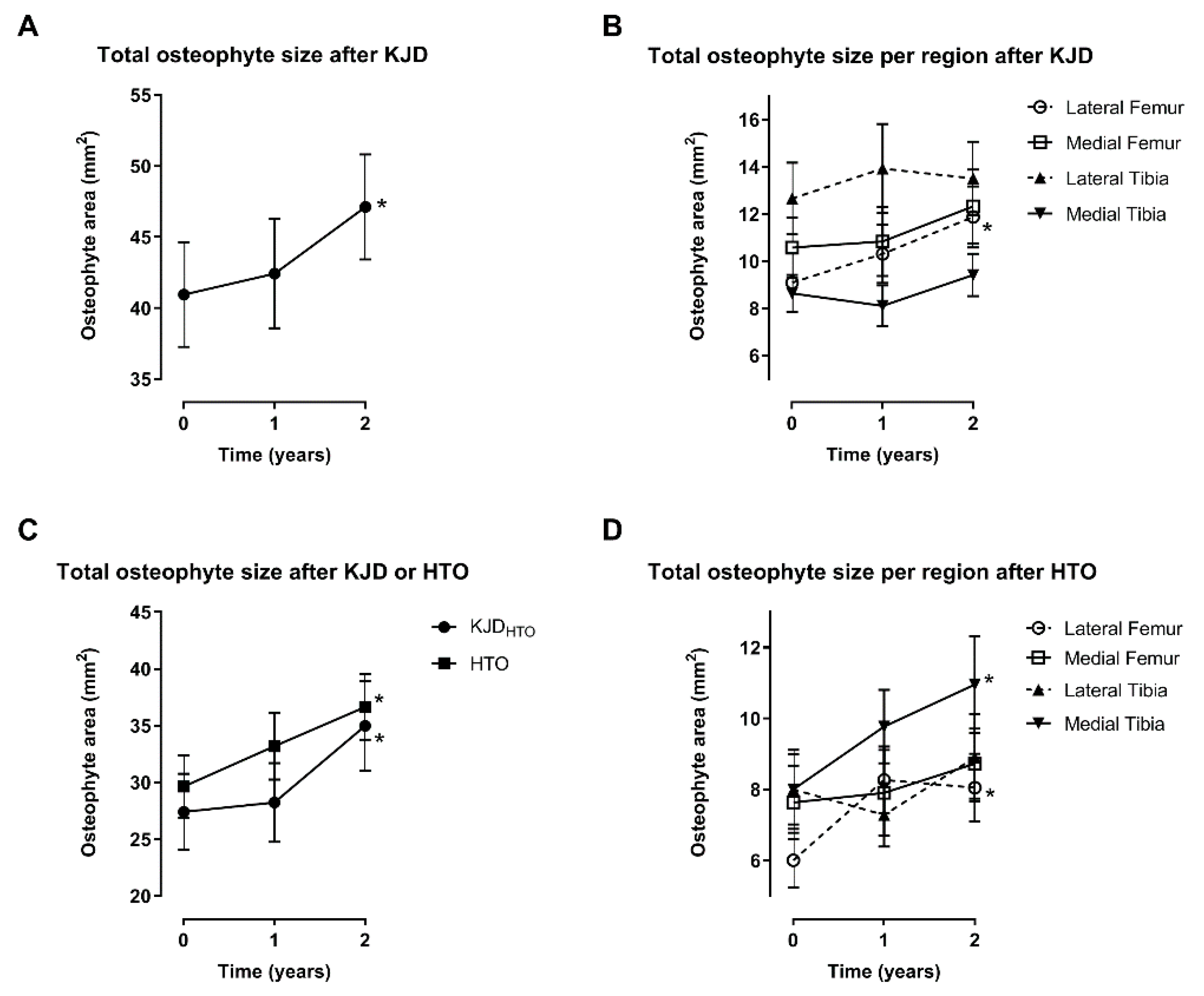
3.2. Changes after Knee Joint Distraction
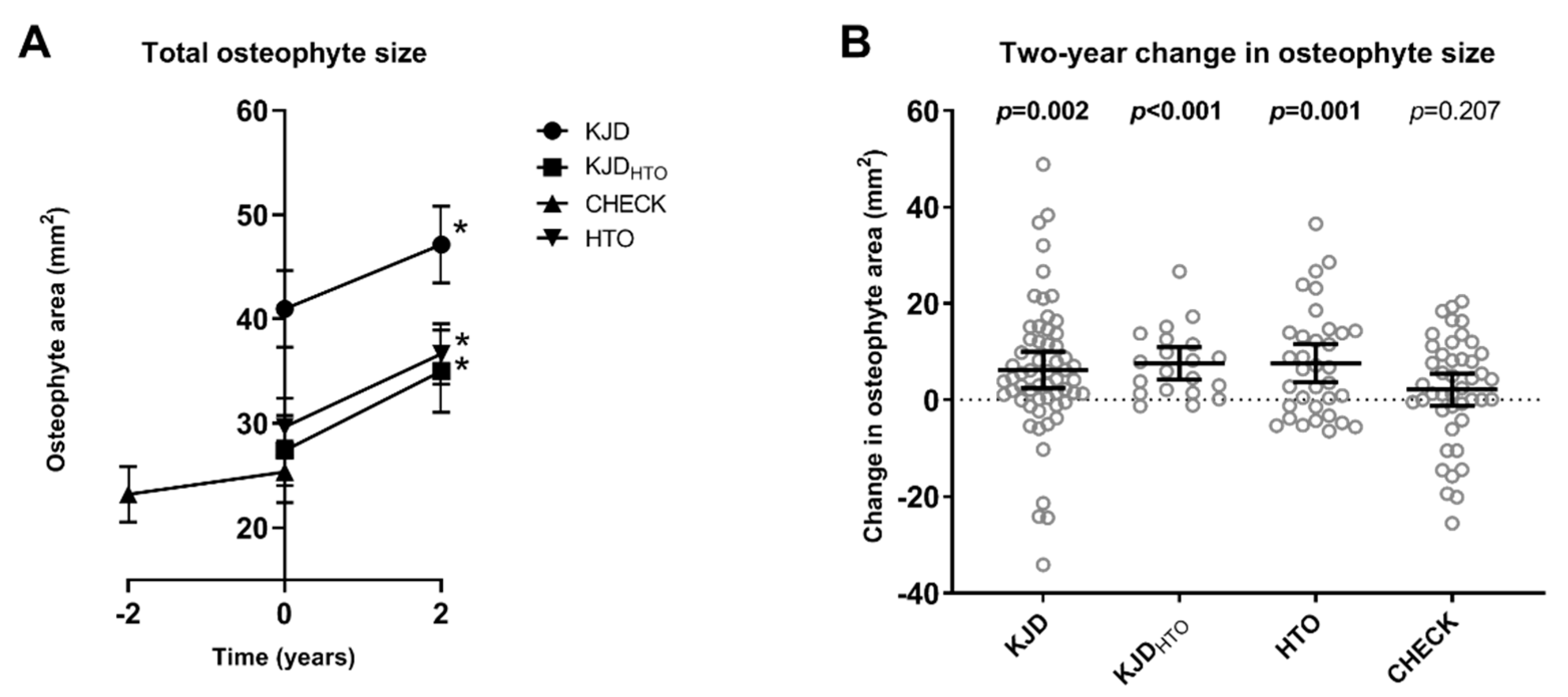
3.3. Comparison with High Tibial Osteotomy
3.4. Comparison with Untreated OA Patients
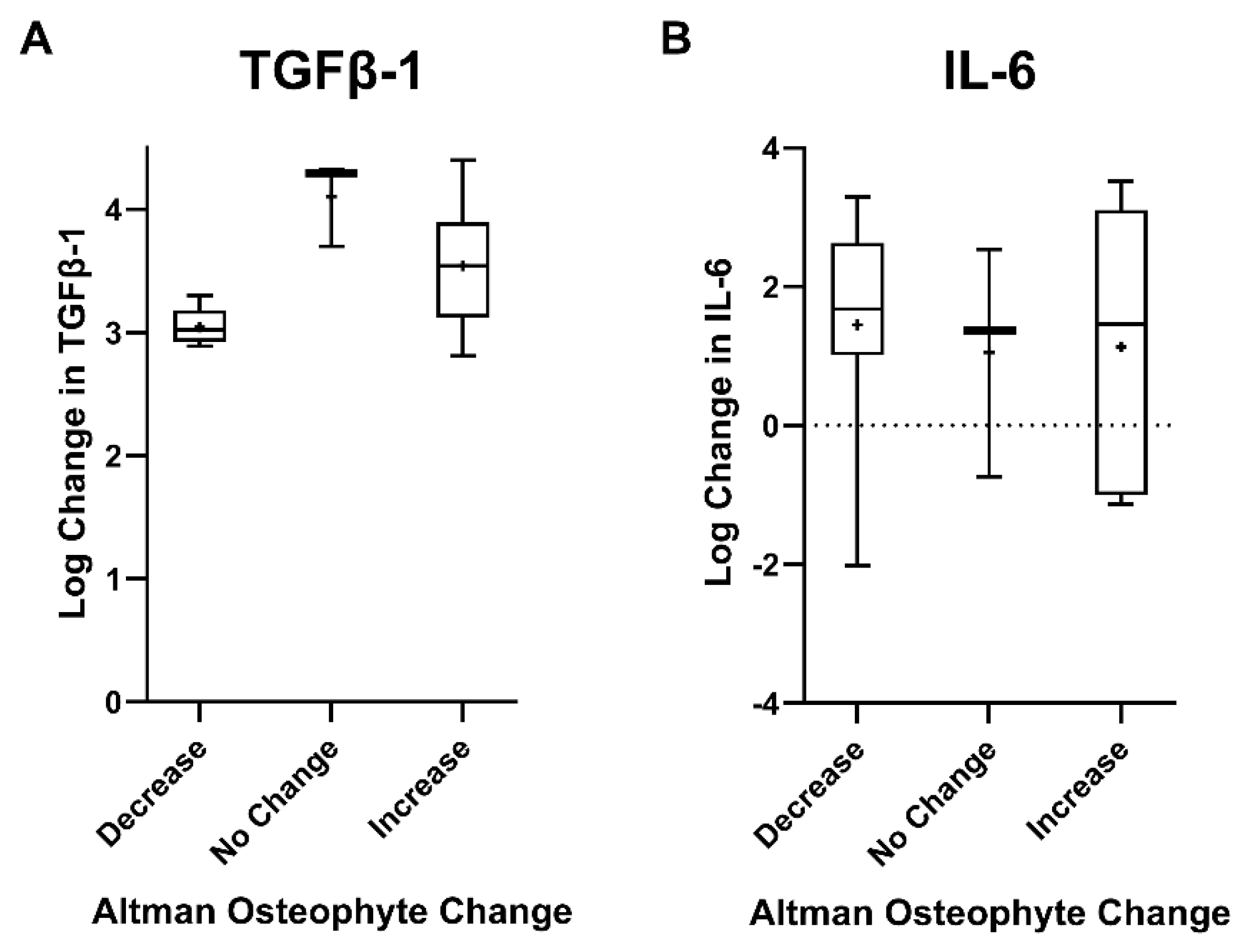
3.5. Relation with Synovial Fluid Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Woolf, A.; Pfleger, B. Burden of major musculoskeletal conditions. Bull. World Health Organ. 2003, 81, 646–656. [Google Scholar]
- Van der Kraan, P.M.; van den Berg, W.B. Osteophytes: Relevance and biology. Osteoarthr. Cartil. 2007, 15, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Felson, D.T.; Gale, D.R.; Gale, M.E.; Niu, J.; Hunter, D.J.; Goggins, J.; LaValley, M. Osteophytes and progression of knee osteoarthritis. Rheumatology 2005, 44, 100–104. [Google Scholar] [CrossRef] [Green Version]
- Dieppe, P.A.; Cushnaghan, J.; Shepstone, L. The Bristol ‘OA500′ Study: Progression of osteoarthritis (OA) over 3 years and the relationship between clinical and radiographic changes at the knee joint. Osteoarthr. Cartil. 1997, 5, 87–97. [Google Scholar] [CrossRef] [Green Version]
- Braun, H.J.; Gold, G.E. Diagnosis of osteoarthritis: Imaging. Bone 2012, 51, 278–288. [Google Scholar] [CrossRef] [Green Version]
- Altman, R.; Gold, G. Atlas of individual radiographic features in osteoarthritis, revised. Osteoarthr. Cartil. 2007, 15, A1–A56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellgren, J.H.; Lawrence, J.S. Radiological Assessment of Osteo-Arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nevalainen, M.T.; Kauppinen, K.; Pylväläinen, J.; Pamilo, K.; Pesola, M.; Haapea, M.; Koski, J.; Saarakkala, S. Ultrasonography of the late-stage knee osteoarthritis prior to total knee arthroplasty: Comparison of the ultrasonographic, radiographic and in-tra-operative findings. Sci. Rep. 2018, 8, 17742. [Google Scholar] [CrossRef] [PubMed]
- Lützner, J.; Kasten, P.; Günther, K.-P.; Kirschner, S. Surgical options for patients with osteoarthritis of the knee. Nat. Rev. Rheumatol. 2009, 5, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Bayliss, L.E.; Culliford, D.; Monk, A.P.; Glyn-Jones, S.; Prieto-Alhambra, D.; Judge, A.; Cooper, C.; Carr, A.J.; Arden, N.K.; Beard, D.J.; et al. The effect of patient age at interven-tion on risk of implant revision after total replacement of the hip or knee: A population-based cohort study. Lancet 2017, 389, 1424–1430. [Google Scholar] [CrossRef] [Green Version]
- Dean, C.S.; Liechti, D.J.; Chahla, J.; Moatshe, G.; LaPrade, R.F. Clinical Outcomes of High Tibial Osteotomy for Knee Instabil-ity: A Systematic Review. Orthop. J. Sport. Med. 2016, 4, 2325967116633419. [Google Scholar]
- Kim, C.-W.; Seo, S.-S.; Lee, C.-R.; Gwak, H.-C.; Kim, J.-H.; Jung, S.-G. Factors affecting articular cartilage repair after open-wedge high tibial osteotomy. Knee 2017, 24, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Kim, H.-J.; Lee, D.-H. Survival of opening versus closing wedge high tibial osteotomy: A meta-analysis. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Lafeber, F.P.J.G.; Intema, F.; Van Roermund, P.M.; Marijnissen, A.C. Unloading joints to treat osteoarthritis, including joint distraction. Curr. Opin. Rheumatol. 2006, 18, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Jansen, M.P.; van der Weiden, G.S.; Van Roermund, P.M.; Custers, R.J.; Mastbergen, S.C.; Lafeber, F.P. Initial tissue repair predicts long-term clinical success of knee joint distraction as treatment for knee osteoarthritis. Osteoarthr. Cartil. 2018, 26, 1604–1608. [Google Scholar] [CrossRef] [Green Version]
- Van Der Woude, J.A.D.; Wiegant, K.; Van Heerwaarden, R.J.; Spruijt, S.; Emans, P.J.; Mastbergen, S.C.; Lafeber, F.P.J.G. Knee joint distraction compared with total knee arthroplasty a randomised controlled trial. Bone Jt. J. 2017, 99, 51–58. [Google Scholar] [CrossRef]
- Van der Woude, J.A.D.; Wiegant, K.; Van Heerwaarden, R.J.; Spruijt, S.; Van Roermund, P.M.; Custers, R.J.H.; Mastbergen, S.C.; Lafeber, F.P.J.G. Knee joint dis-traction compared with high tibial osteotomy: A randomized controlled trial. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 876–886. [Google Scholar] [CrossRef] [Green Version]
- Jansen, M.P.; Besselink, N.J.; van Heerwaarden, R.J.; Custers, R.J.H.; Emans, P.J.; Spruijt, S.; Mastbergen, S.C.; Lafeber, F.P.J.G. Knee Joint Distraction Compared with High Tibial Osteotomy and Total Knee Arthroplasty: Two-Year Clinical, Radiographic, and Biochemical Marker Outcomes of Two Randomized Controlled Trials. Cartilage 2019, 12, 181–191. [Google Scholar] [CrossRef] [Green Version]
- Jansen, M.P.; Boymans, T.A.; Custers, R.J.; Van Geenen, R.C.; Van Heerwaarden, R.J.; Huizinga, M.R.; Nellensteijn, J.M.; Sollie, R.; Spruijt, S.; Mastbergen, S.C. Knee Joint Distraction as Treatment for Osteoarthritis Results in Clinical and Structural Benefit: A Systematic Review and Meta-Analysis of the Limited Number of Studies and Patients Available. Cartilage 2020. submitted. [Google Scholar] [CrossRef]
- Hoorntje, A.; Kuijer, P.P.F.M.; Koenraadt, K.L.M.; Waterval-Witjes, S.; Kerkhoffs, G.M.M.J.; Mastbergen, S.C.; Marijnissen, A.C.A.; Jansen, M.; Van Geenen, R.C.I. Return to Sport and Work after Randomization for Knee Distraction versus High Tibial Osteotomy: Is There a Difference? J. Knee Surg. 2020. [Google Scholar] [CrossRef]
- Wiegant, K.; van Roermund, P.; Intema, F.; Cotofana, S.; Eckstein, F.; Mastbergen, S.; Lafeber, F. Sustained clinical and structural benefit after joint distraction in the treatment of severe knee osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1660–1667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Woude, J.T.A.; Wiegant, K.; Van Roermund, P.M.; Intema, F.; Custers, R.J.; Eckstein, F.; van Laar, J.M.; Mastbergen, S.C.; Lafeber, F.P. Five-Year Follow-up of Knee Joint Distraction: Clinical Benefit and Cartilaginous Tissue Repair in an Open Uncontrolled Prospective Study. Cartilage 2017, 8, 263–271. [Google Scholar] [CrossRef]
- Jansen, M.P.; Maschek, S.; van Heerwaarden, R.J.; Mastbergen, S.C.; Wirth, W.; Lafeber, F.P.J.G.; Eckstein, F. Changes in Cartilage Thickness and Denuded Bone Area after Knee Joint Distraction and High Tibial Osteotomy—Post-Hoc Analyses of Two Randomized Controlled Trials. J. Clin. Med. 2021, 10, 368. [Google Scholar] [CrossRef]
- Tuan, R.S.; Chen, A.F.; Klatt, B.A. Cartilage regeneration. J. Am. Acad. Orthop. Surg. 2013, 21, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Watt, F.; Hamid, B.; Garriga, C.; Judge, A.; Hrusecka, R.; Custers, R.; Jansen, M.; Lafeber, F.; Mastbergen, S.; Vincent, T. The molecular profile of synovial fluid changes upon joint distraction and is associated with clinical response in knee osteoarthritis. Osteoarthr. Cartil. 2020, 28, 324–333. [Google Scholar] [CrossRef] [Green Version]
- Blaney Davidson, E.N.; van der Kraan, P.M.; van den Berg, W.B. TGF-β and osteoarthritis. Osteoarthr. Cartil. 2007, 15, 597–604. [Google Scholar] [CrossRef] [Green Version]
- Bakker, A.C.; Van De Loo, F.A.J.; Van Beuningen, H.M.; Sime, P.; Van Lent, P.L.E.M.; Van Der Kraan, P.M.; Richards, C.D.; Van Den Berg, W.B. Overexpression of ac-tive TGF-beta-1 in the murine knee joint: Evidence for synovial-layer-dependent chondro-osteophyte formation. Osteoarthr. Cartil. 2001, 9, 128–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scharstuhl, A.; Glansbeek, H.L.; van Beuningen, H.M.; Vitters, E.L.; van der Kraan, P.M.; van den Berg, W.B. Inhibition of En-dogenous TGF-β During Experimental Osteoarthritis Prevents Osteophyte Formation and Impairs Cartilage Repair. J. Immunol. 2002, 169, 507–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Beuningen, H.M.; van der Kraan, P.M.; Arntz, O.J.; van den Berg, W.B. Transforming growth factor-beta 1 stimulates ar-ticular chondrocyte proteoglycan synthesis and induces osteophyte formation in the murine knee joint. Lab. Investig. 1994, 71, 279–290. [Google Scholar]
- Dodds, R.A.; Merry, K.; Littlewood, A.; Gowen, M. Expression of mRNA for IL1 beta, IL6 and TGF beta 1 in developing hu-man bone and cartilage. J. Histochem. Cytochem. 1994, 42, 733–744. [Google Scholar] [CrossRef] [PubMed]
- Horner, A.; Kemp, P.; Summers, C.; Bord, S.; Bishop, N.; Kelsall, A.; Coleman, N.; Compston, J. Expression and distribution of transforming growth factor-β isoforms and their signaling receptors in growing human bone. Bone 1998, 23, 95–102. [Google Scholar] [CrossRef]
- Sakao, K.; Takahashi, K.A.; Arai, Y.; Saito, M.; Honjo, K.; Hiraoka, N.; Asada, H.; Shin-Ya, M.; Imanishi, J.; Mazda, O.; et al. Osteoblasts derived from osteophytes produce in-terleukin-6, interleukin-8, and matrix metalloproteinase-13 in osteoarthritis. J. Bone Miner. Metab. 2009, 27, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Intema, F.; Van Roermund, P.M.; Marijnissen, A.C.; Cotofana, S.; Eckstein, F.; Castelein, R.M.; Bijlsma, J.W.; Mastbergen, S.C.; Lafeber, F.P. Tissue structure modifica-tion in knee osteoarthritis by use of joint distraction: An open 1-year pilot study. Ann. Rheum. Dis. 2011, 70, 1441–1446. [Google Scholar] [CrossRef] [PubMed]
- Wiegant, K.; van Heerwaarden, R.; van der Woude, J.T.; Custers, R.R.; Emans, P.; Kuchuk, N.; Mastbergen, S.; Lafeber, F.F. Knee Joint Distraction as an Alternative Surgical Treatment for Osteoarthritis: Rationale and Design of two Randomized Controlled Trials (vs High Tibial Osteotomy and Total Knee Prosthesis). Int. J. Orthop. 2015, 2, 353–360. [Google Scholar] [CrossRef]
- Buckland-Wright, J.C.; Ward, R.J.; Peterfy, C.; Mojcik, C.F.; Leff, R.L. Reproducibility of the semiflexed (metatarsophalangeal) radiographic knee position and automated measurements of medial tibiofemoral joint space width in a multicenter clinical trial of knee osteoarthritis. J. Rheumatol. 2004, 31, 1588–1597. [Google Scholar]
- Buckland-Wright, J.C.; Wolfe, F.; Ward, R.J.; Flowers, N.; Hayne, C. Substantial superiority of semiflexed (MTP) views in knee osteoarthritis: A comparative radiographic study, without fluoroscopy, of standing extended, semiflexed (MTP), and schuss views. J. Rheumatol. 1999, 26, 2664–2674. [Google Scholar]
- Wesseling, J.; Boers, M.; Viergever, M.A.; Hilberdink, W.K.; Lafeber, F.P.; Dekker, J.; Bijlsma, J.W. Cohort profile: Cohort Hip and Co-hort Knee (CHECK) study. Int. J. Epidemiol. 2016, 45, 36–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marijnissen, A.; Vincken, K.; Vos, P.; Saris, D.; Viergever, M.; Bijlsma, J.; Bartels, L.; Lafeber, F. Knee Images Digital Analysis (KIDA): A novel method to quantify individual radiographic features of knee osteoarthritis in detail. Osteoarthr. Cartil. 2008, 16, 234–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, M.P.; Mastbergen, S.C.; van Heerwaarden, R.J.; Spruijt, S.; van Empelen, M.D.; Kester, E.C.; Lafeber, F.P.; Custers, R.J. Knee joint distraction in regular care for treatment of knee osteoarthritis: A comparison with clinical trial data. PLoS ONE 2020, 15, e0227975. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, S.C.; Muir, K.R.; Doherty, M.; O’reilly, S.C.; Muir, K.R. Screening for pain in knee osteoarthritis: Which question? Ann Rheum Dis. 1996, 55, 931–933. [Google Scholar] [CrossRef] [Green Version]
- Spector, T.D.; Hart, D.J.; Byrne, J.; Harris, P.A.; Dacre, J.E.; Doyle, D.V. Definition of osteoarthritis of the knee for epidemiologi-cal studies. Ann. Rheum. Dis. 1993, 52, 790–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanyon, P.; O’Reilly, S.; Jones, A.; Doherty, M. Radiographic assessment of symptomatic knee osteoarthritis in the commu-nity: Definitions and normal joint space. Ann. Rheum. Dis. 1998, 57, 595–601. [Google Scholar] [CrossRef]
- Hamilton, T.W.; Choudhary, R.; Jenkins, C.; Mellon, S.; Dodd, C.A.F.; Murray, D.W.; Pandit, H.G. Lateral osteophytes do not represent a contraindication to medial unicompartmental knee arthroplasty: A 15-year follow-up. Knee Surg. Sports Traumatol. Arthrosc. 2016, 25, 652–659. [Google Scholar] [CrossRef]
- Waldstein, W.; Kasparek, M.F.; Faschingbauer, M.; Windhager, R.; Boettner, F. Lateral-compartment Osteophytes are not As-sociated With Lateral-compartment Cartilage Degeneration in Arthritic Varus Knees. Clin. Orthop. Relat. Res. 2017, 475, 1386–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teitge, R.A. CORR Insights®: Lateral-compartment Osteophytes are not associated with Lateral-compartment Cartilage Degeneration in Arthritic Varus Knees. Clin. Orthop. Relat. Res. 2017, 475, 1393–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | KJD (n = 58) | KJDHTO (n = 20) | HTO (n = 36) | CHECK (n = 44) | SF (n = 17) |
|---|---|---|---|---|---|
| Age, mean (SD) | 51.4 (8.0) | 51.2 (5.8) | 49.1 (6.5) | 64.0 (4.3) | 53.8 (4.7) |
| Male gender, n (%) | 34 (59) | 15 (75) | 23 (64) | 5 (11) | 10 (59) |
| BMI, mean (SD) | 28.0 (3.4) | 27.4 (3.3) | 27.0 (3.5) | 29.4 (4.6) | 29.0 (3.3) |
| Kellgren-Lawrence grade, n (%) | |||||
| Grade 0 | 0 (0) | 0 (0) | 1 (3) | 2 (5) | 0 (0) |
| Grade 1 | 8 (14) | 5 (25) | 4 (11) | 18 (41) | 0 (0) |
| Grade 2 | 9 (16) | 4 (20) | 10 (28) | 16 (36) | 2 (12) |
| Grade 3 | 28 (48) | 10 (50) | 18 (50) | 8 (18) | 7 (41) |
| Grade 4 | 13 (22) | 1 (5) | 3 (8) | 0 (0) | 8 (47) |
| KJD | HTO | CHECK | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | 2 Years | p-Value | Baseline | 2 Years | p-Value | Baseline | 2 Years | p-Value | |
| Total WOMAC, mean (SD) | 50.6 (15.7) | 78.8 (19.3) | <0.001 | 50.7 (14.6) | 81.5 (14.5) | <0.001 | 58.6 (15.9) | 51.8 (20.3) | 0.035 |
| JSW, mean (SD) | 2.36 (1.73) | 3.03 (1.57) | <0.001 | 2.24 (1.28) | 2.56 (1.37) | 0.034 | 3.18 (1.76) | 2.52 (1.72) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jansen, M.P.; Mastbergen, S.C.; Watt, F.E.; Willemse, E.J.; Vincent, T.L.; Spruijt, S.; Emans, P.J.; Custers, R.J.H.; van Heerwaarden, R.J.; Lafeber, F.P.J.G. Cartilage Repair Activity during Joint-Preserving Treatment May Be Accompanied by Osteophyte Formation. Appl. Sci. 2021, 11, 7156. https://doi.org/10.3390/app11157156
Jansen MP, Mastbergen SC, Watt FE, Willemse EJ, Vincent TL, Spruijt S, Emans PJ, Custers RJH, van Heerwaarden RJ, Lafeber FPJG. Cartilage Repair Activity during Joint-Preserving Treatment May Be Accompanied by Osteophyte Formation. Applied Sciences. 2021; 11(15):7156. https://doi.org/10.3390/app11157156
Chicago/Turabian StyleJansen, Mylène P., Simon C. Mastbergen, Fiona E. Watt, Elske J. Willemse, Tonia L. Vincent, Sander Spruijt, Pieter J. Emans, Roel J. H. Custers, Ronald J. van Heerwaarden, and Floris P. J. G. Lafeber. 2021. "Cartilage Repair Activity during Joint-Preserving Treatment May Be Accompanied by Osteophyte Formation" Applied Sciences 11, no. 15: 7156. https://doi.org/10.3390/app11157156