
Round Window Reinforcement-Induced Changes in Intracochlear Sound Pressure

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Temporal Bone Samples and Experimental Protocol
2.2. Surgical Preparation
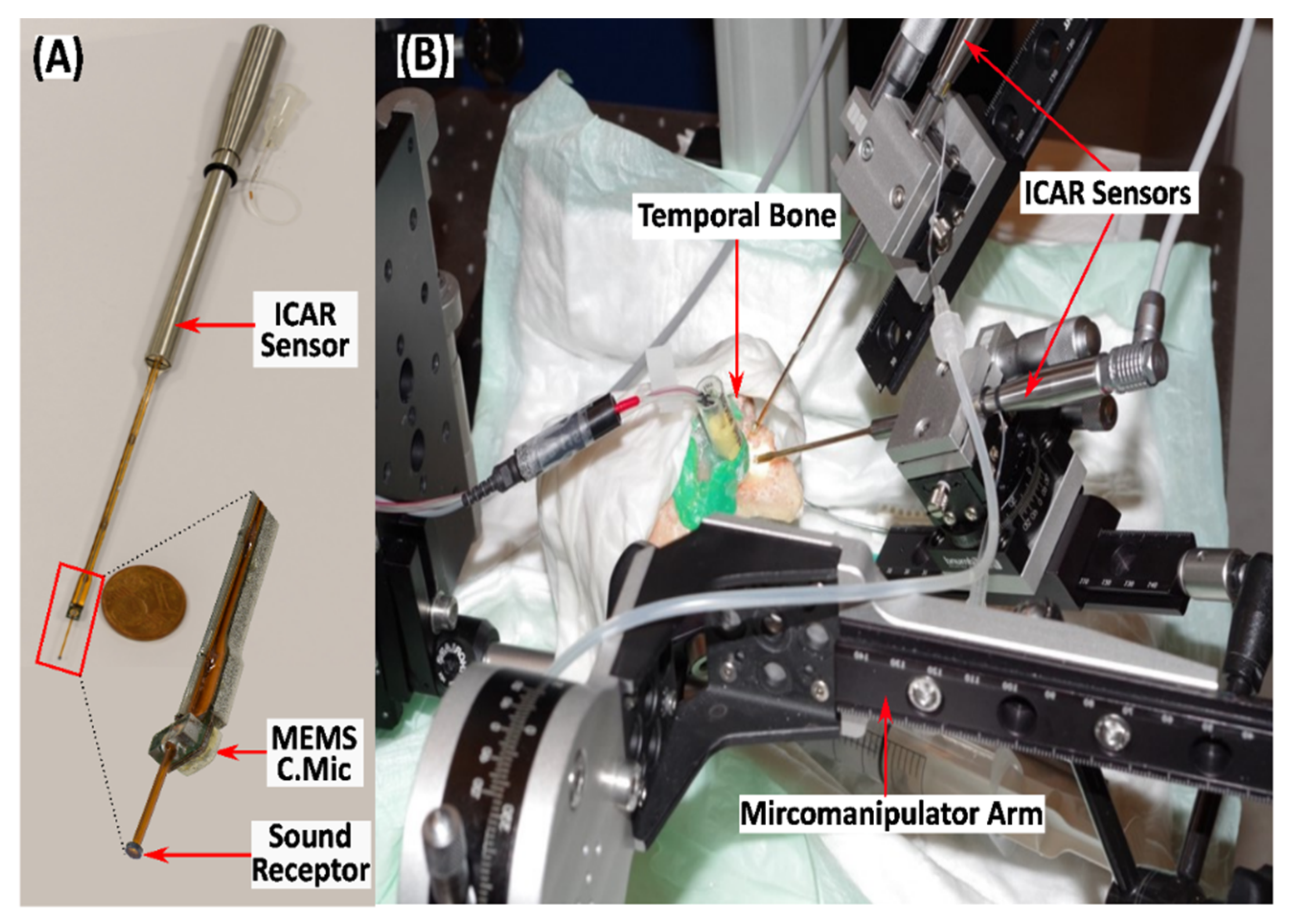
2.3. Measurement Setup
2.4. HTB Functionality and ICSP Measurements
2.5. Reinforcement of RWM
2.6. Numerical Approach to Assess the Effect of RWM Reinforcement on Cochlear Hydrodynamics
3. Results
3.1. Validation of the Experimental Method
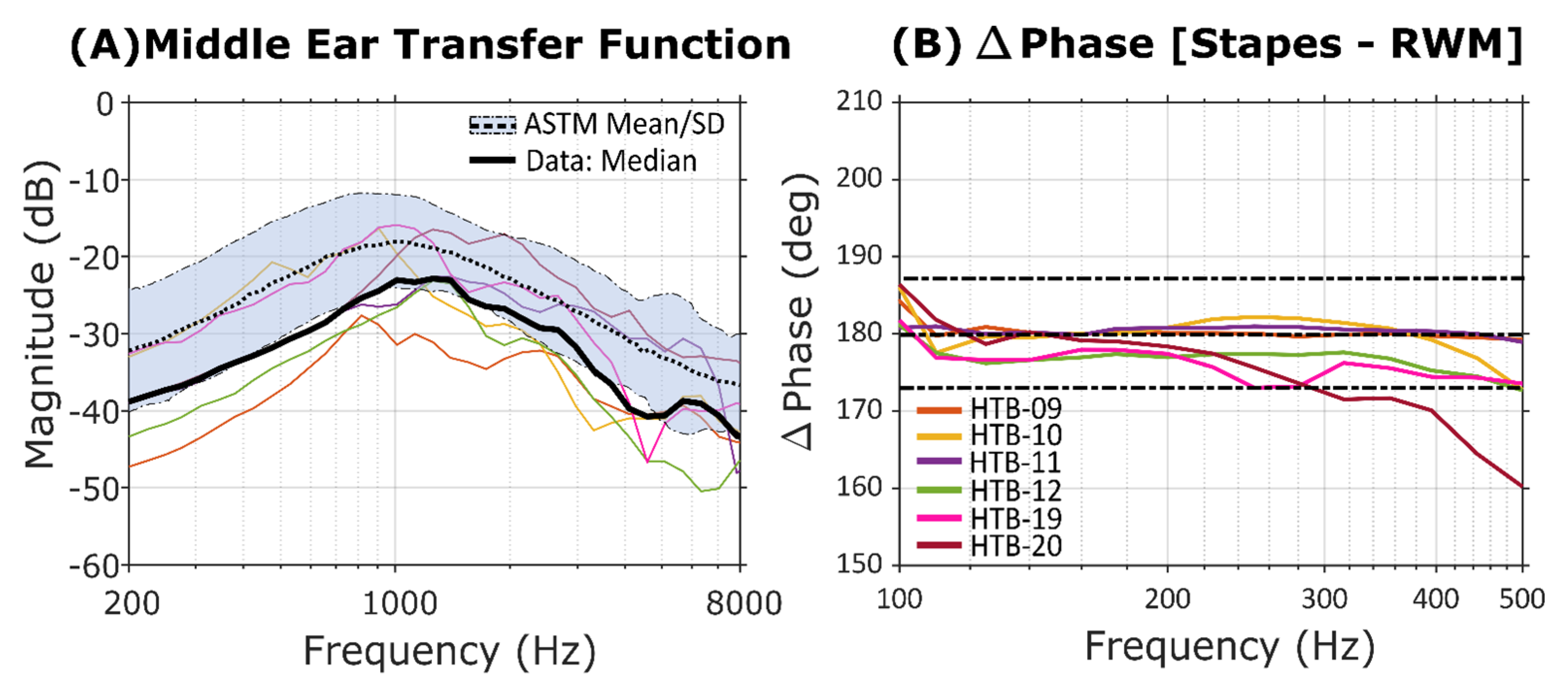
3.1.1. Assessment of the Middle Ear Function and the Hydrodynamic Condition of the Cochlea
3.1.2. Intracochlear Pressure Measurements in Scala Tympani and Scala Vestibuli
3.1.3. Effect of RWM Reinforcement on ICSP Measurement
4. Discussion
4.1. Validation of the HTB Functionality
4.2. Effect of RWM Reinforcement on the ICSP
4.3. Comparison with Numerical Calculations and RWM Impedance Estimation
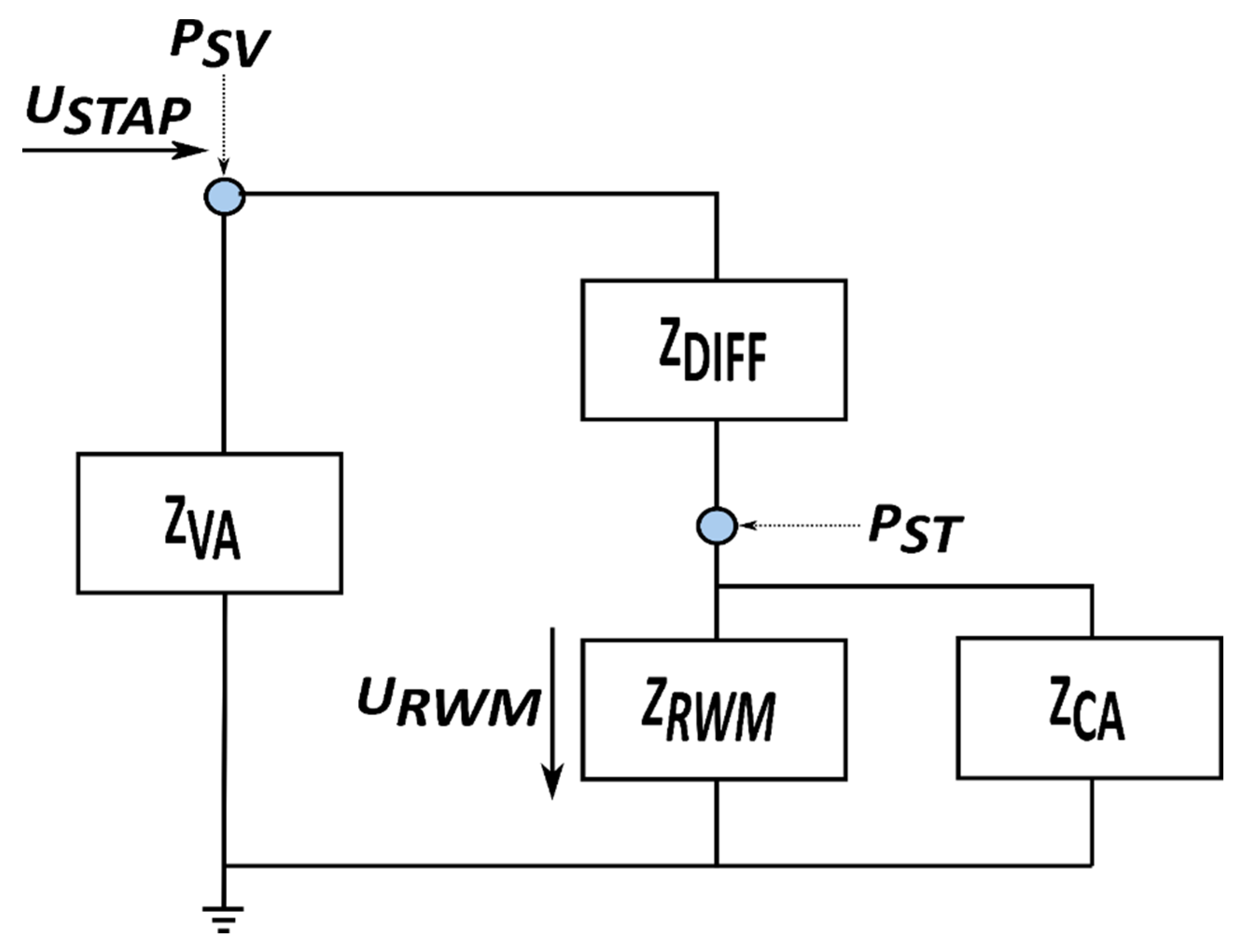
4.3.1. LEM of the Cochlea Proposed by Nakajima et al. (2009)
4.3.2. LEM of the Cochlea Proposed by Elliot et al. (2016)
4.3.3. Results
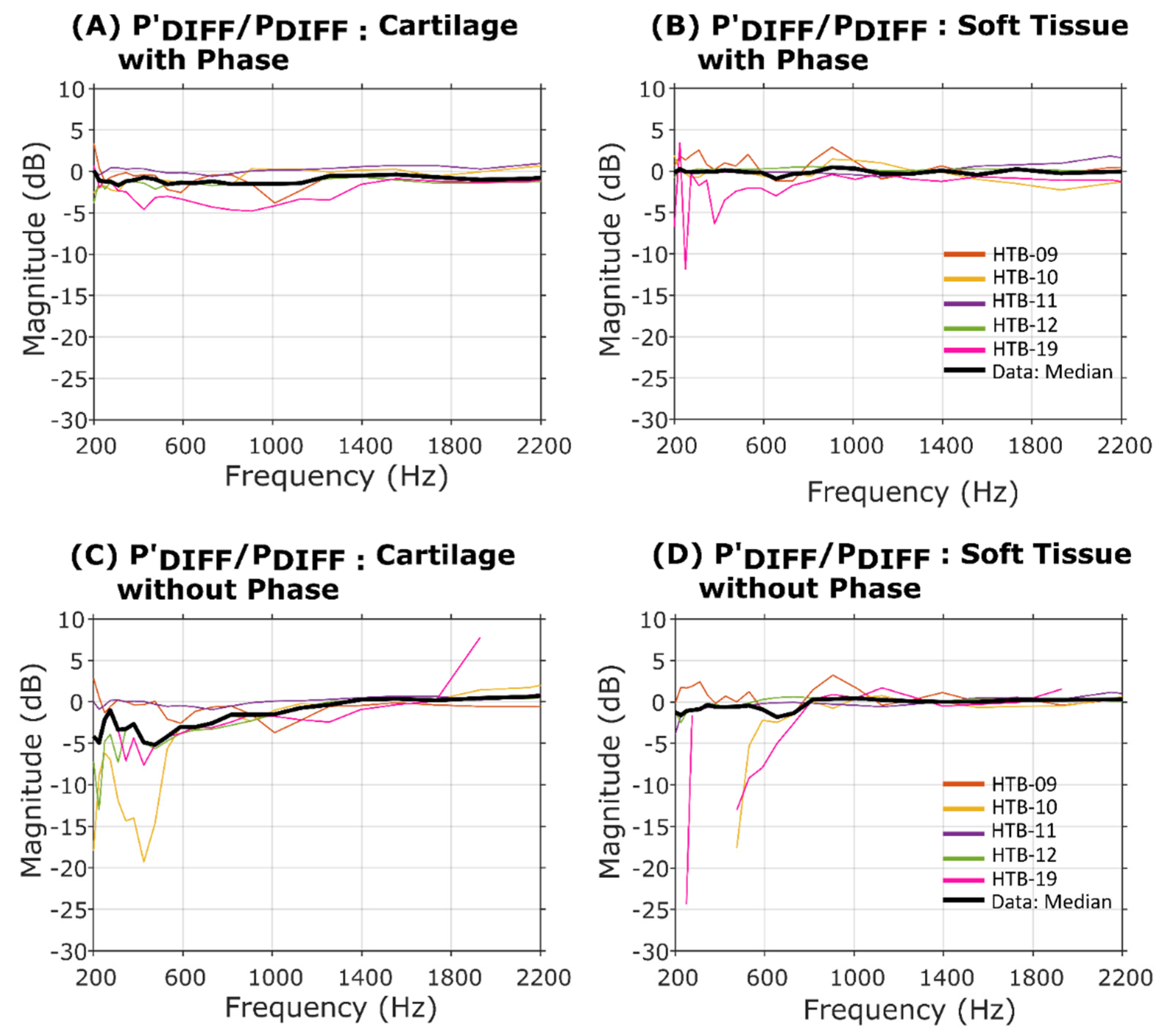
4.4. Effect of RWM Reinforcement on the Pressure Difference across the Partition
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A. Stapes Velocity Measurements with RWM Reinforcement

References
- Obrist, D. Flow phenomena in the inner ear. Annu. Rev. Fluid Mech. 2019, 51, 487–510. [Google Scholar] [CrossRef]
- Duan, M.-L.; Zhi-Qiang, C.J. Permeability of round window membrane and its role for drug delivery: Our own findings and literature review. J. Otol. 2009, 4, 34–43. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, W.; Rajagopal, R.; Lloyd, G. Systematic review of round window operations for the treatment of superior semicircular canal dehiscence . J. Int. Adv. Otol. 2019, 15, 209. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, H.; Kartush, J.M.; Parnes, L.S.; Poe, D.S.; Babu, S.C.; Levenson, M.J.; Wazen, J.; Ridley, R.W. Round window reinforcement for superior semicircular canal dehiscence: A retrospective multi-center case series . Am. J. Otolaryngol. 2014, 35, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Wegner, I.; Eldaebes, M.M.; Landry, T.G.; Adamson, R.B.; Grolman, W.; Bance, M.L. Effect of round window reinforcement on hearing: A temporal bone study with clinical implications for surgical reinforcement of the round window . Otol. Neurotol. 2016, 37, 598–601. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, H.; Wu, Y.-H.E.; Hagan, S. Round and oval window reinforcement for the treatment of hyperacusis. Am. J. Otolaryngol. 2015, 36, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Causon, A.; Verschuur, C.; Newman, T.A. A retrospective analysis of the contribution of reported factors in cochlear implantation on hearing preservation outcomes . Otol. Neurotol. 2015, 36, 1137–1145. [Google Scholar] [CrossRef]
- Elliott, S.J.; Ni, G.; Verschuur, C.A. Modelling the effect of round window stiffness on residual hearing after cochlear implantation . Hear. Res. 2016, 341, 155–167. [Google Scholar] [CrossRef]
- Friedmann, D.R.; Peng, R.; Fang, Y.; McMenomey, S.O.; Roland, J.T.; Waltzman, S.B. Effects of loss of residual hearing on speech performance with the CI422 and the Hybrid-L electrode . Cochlear Implant. Int. 2015, 16, 277–284. [Google Scholar] [CrossRef]
- Verschuur, C.; Hellier, W.; Teo, C. Hearing impairment as a determinant of function in the elderly . Cochlear Implant. Int. 2016, 17 (Suppl. 1), S62–S65. [Google Scholar] [CrossRef]
- Nakajima, H.H.; Dong, W.; Olson, E.S.; Merchant, S.N.; Ravicz, M.E.; Rosowski, J.J. Differential intracochlear sound pressure measurements in normal human temporal bones . Assoc. Res. Otolaryngol. 2009, 10, 23. [Google Scholar] [CrossRef] [Green Version]
- Puria, S.; Allen, J.B.J. A parametric study of cochlear input impedance . Acoust. Soc. Am. 1991, 89, 287–309. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.; Cheng, Y.S.; Galaiya, D.; Nakajima, H.H. The Effect of Round Window Reinforcement on Human Hearing. In AIP Conference Proceedings; AIP Publishing LLC: Melville, NY, USA, 2018; p. 150004. [Google Scholar]
- Sim, J.H.; Chatzimichalis, M.; Röösli, C.; Laske, R.D.; Huber, A.M.J.E. Objective Assessment of Stapedotomy Surgery from Round Window Motion Measurement. Ear Hear. 2012, 33, e24–e31. [Google Scholar] [CrossRef]
- Zhang, X.; Gan, R.Z. Dynamic properties of human round window membrane in auditory frequencies running head: Dynamic properties of round window membrane . Med. Eng. Phys. 2013, 35, 310–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Péus, D.; Dobrev, I.; Prochazka, L.; Thoele, K.; Dalbert, A.; Boss, A.; Newcomb, N.; Probst, R.; Röösli, C.; Sim, J.H. Sheep as a large animal ear model: Middle-ear ossicular velocities and intracochlear sound pressure . Hear. Res. 2017, 351, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Pfiffner, F.; Prochazka, L.; Péus, D.; Dobrev, I.; Dalbert, A.; Sim, J.H.; Kesterke, R.; Walraevens, J.; Harris, F.; Röösli, C. A MEMS condenser microphone-based intracochlear acoustic receiver . IEEE Trans. Biomed. Eng. 2017, 64, 2431–2438. [Google Scholar] [CrossRef] [Green Version]
- Rosowski, J.J.; Chien, W.; Ravicz, M.E.; Merchant, S.N. Testing a method for quantifying the output of implantable middle ear hearing devices . Audiol. Neurootol. 2007, 12, 265–276. [Google Scholar] [CrossRef] [Green Version]
- Frear, D.L.; Guan, X.; Stieger, C.; Rosowski, J.J.; Nakajima, H.H. Impedances of the inner and middle ear estimated from intracochlear sound pressures in normal human temporal bones . Hear. Res. 2018, 367, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Stenfelt, S.; Hato, N.; Goode, R.L.J. Fluid volume displacement at the oval and round windows with air and bone conduction stimulation . Acoust. Soc. Am. 2004, 115, 797–812. [Google Scholar] [CrossRef] [PubMed]
- Stenfelt, S.; Hato, N.; Goode, R.L. Round window membrane motion with air conduction and bone conduction stimulation . Hear. Res. 2004, 198, 10–24. [Google Scholar] [CrossRef] [PubMed]
- Prochazka, L.; Huber, A.; Dobrev, I.; Harris, F.; Dalbert, A.; Röösli, C.; Obrist, D.; Pfiffner, F. Packaging Technology for an Implantable Inner Ear MEMS Microphone . Sensors 2019, 19, 4487. [Google Scholar] [CrossRef] [Green Version]
- Aibara, R.; Welsh, J.T.; Puria, S.; Goode, R.L. Human middle-ear sound transfer function and cochlear input impedance . Hear. Res. 2001, 152, 100–109. [Google Scholar] [CrossRef]
- Zhou, L.; Shen, N.; Feng, M.; Liu, H.; Duan, M.; Huang, X. Study of age-related changes in Middle ear transfer function. Comput. Methods Biomech. Biomed. Eng. 2019, 22, 1093–1102. [Google Scholar] [CrossRef] [PubMed]
- Gerig, R.; Ihrle, S.; Röösli, C.; Dalbert, A.; Dobrev, I.; Pfiffner, F.; Eiber, A.; Huber, A.M.; Sim, J.H. Contribution of the incudo-malleolar joint to middle-ear sound transmission . Hear. Res. 2015, 327, 218–226. [Google Scholar] [CrossRef] [Green Version]
- Merchant, S.N.; Ravicz, M.E.; Rosowski, J.J. Acoustic input impedance of the stapes and cochlea in human temporal bones . Hear. Res. 1996, 97, 30–45. [Google Scholar] [CrossRef]
- Wei, K.; Senturk, B.; Matter, M.T.; Wu, X.; Herrmann, I.K.; Rottmar, M.; Toncelli, C. Mussel-inspired injectable hydrogel adhesive formed under mild conditions features near-native tissue properties . ACS Appl. Mater. Interfaces 2019, 11, 47707–47719. [Google Scholar] [CrossRef] [PubMed]
- Peterson, L.; Bogert, B. A dynamical theory of the cochlea . J. Acoust. Soc. Am. 1950, 22, 369–381. [Google Scholar] [CrossRef]
- Wysocki, J. Dimensions of the human vestibular and tympanic scalae . Hear. Res. 1999, 135, 39–46. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lumped Element | Inclusive Elements | SI Unit | Value | Reference |
|---|---|---|---|---|
| ZDIFF | RDIFF | Nsm−5 | 2.0 × 1010 | [23] |
ZRWM | C | N−1m5 | 9.0 × 10−14 | [11] |
| L | kgm−4 | 4.62 × 107 | ||
| R | Nsm−5 | 2.34 × 108 | ||
| X (spacing) | ||||
| N (number of branches) | 6 |
| Lumped Element | Inclusive Elements | SI Units | Value | Reference |
|---|---|---|---|---|
| ZDIFF | RDIFF | Nsm−5 | 2.0 × 1010 | [23] |
| ZRWM | LRWM | Ns2m−5 | 1.0 × 106 | [8] |
| RRWM | Nsm−5 | 2.5 × 109 | ||
| CRWM | N−1m5 | 1.0 × 10−13 | ||
| ZVA | LVA | Ns2m−5 | 5.1 × 107 | |
| RVA | Nsm−5 | 1.1 × 1010 × | ||
| ZCA | LCA | Ns2m−5 | 5.6 × 108 | |
| RCA | Nsm−5 | 3.5 × 1011 × |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liyanage, N.; Prochazka, L.; Grosse, J.; Dalbert, A.; Tabibi, S.; Chatzimichalis, M.; Dobrev, I.; Kleinjung, T.; Huber, A.; Pfiffner, F. Round Window Reinforcement-Induced Changes in Intracochlear Sound Pressure. Appl. Sci. 2021, 11, 5062. https://doi.org/10.3390/app11115062
Liyanage N, Prochazka L, Grosse J, Dalbert A, Tabibi S, Chatzimichalis M, Dobrev I, Kleinjung T, Huber A, Pfiffner F. Round Window Reinforcement-Induced Changes in Intracochlear Sound Pressure. Applied Sciences. 2021; 11(11):5062. https://doi.org/10.3390/app11115062
Chicago/Turabian StyleLiyanage, Nuwan, Lukas Prochazka, Julian Grosse, Adrian Dalbert, Sonia Tabibi, Michail Chatzimichalis, Ivo Dobrev, Tobias Kleinjung, Alexander Huber, and Flurin Pfiffner. 2021. "Round Window Reinforcement-Induced Changes in Intracochlear Sound Pressure" Applied Sciences 11, no. 11: 5062. https://doi.org/10.3390/app11115062