
Minimally Invasive Dentistry for Pre-Eruptive Enamel Lesions—A Case Series

 , ,
, ,  , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
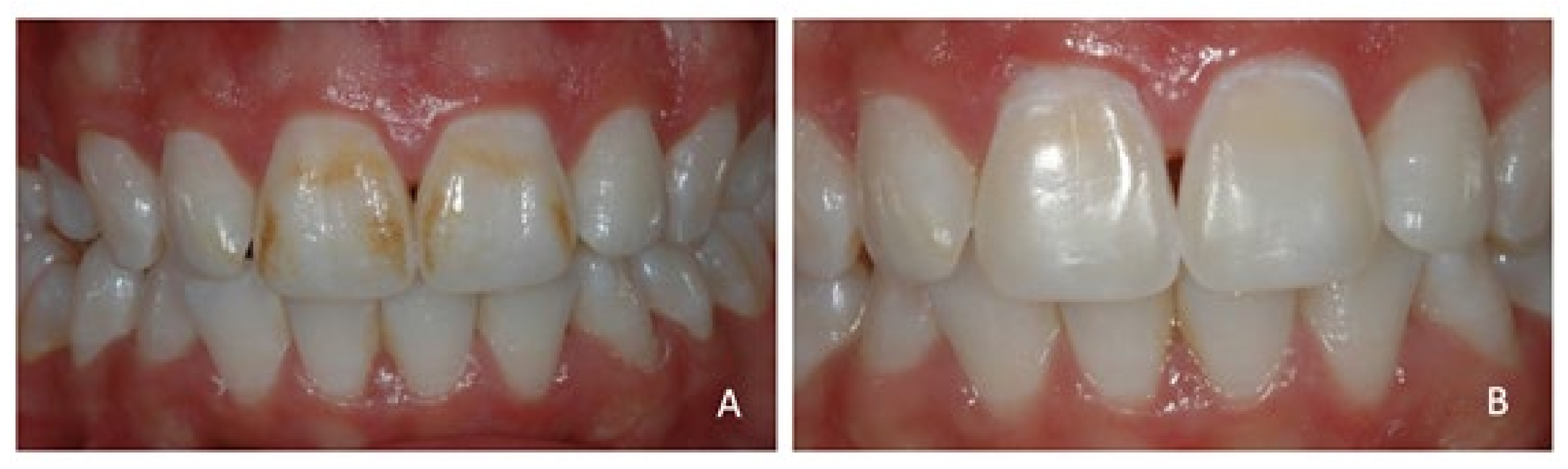
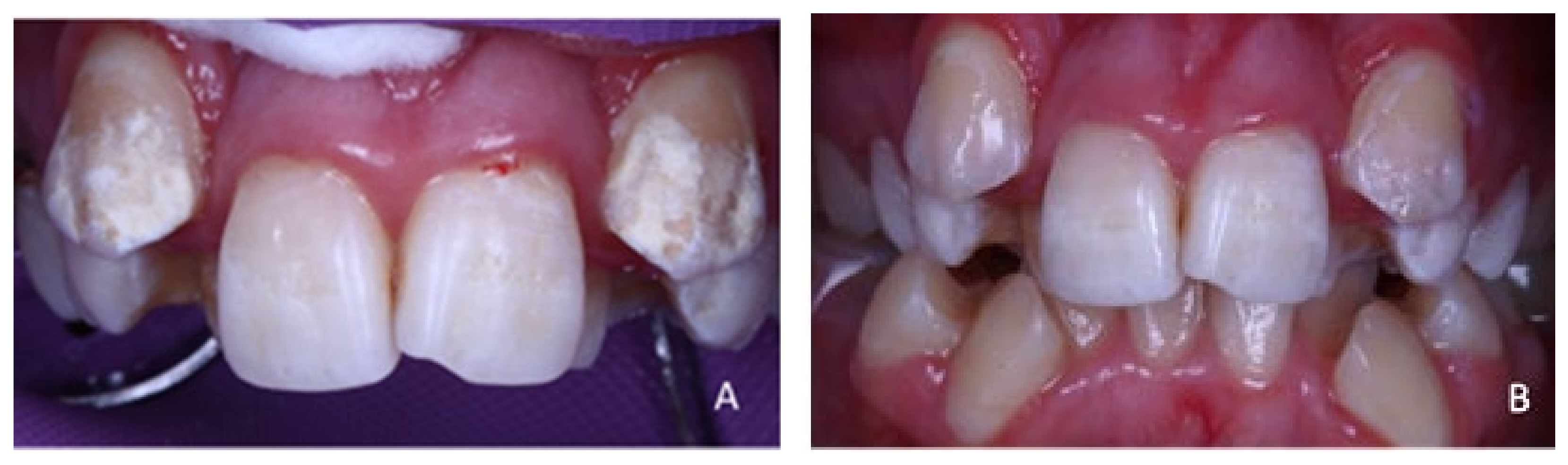
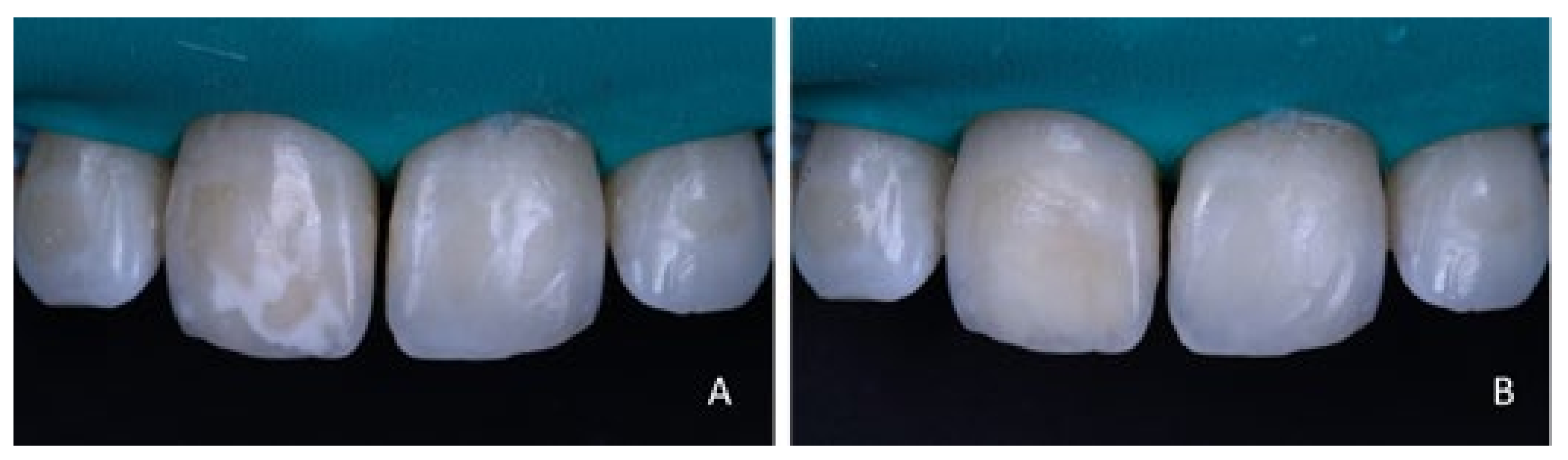
2.1. Cases’ Selection and Description
2.2. Microabrasion Procedure
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Denis, M.; Atlan, A.; Vennat, E.; Tirlet, G.; Attal, J.P. White defects on enamel: Diagnosis and anatomopathology: Two essential factors for proper treatment (part 1). Int. Orthod. 2013, 11, 139–165. [Google Scholar] [CrossRef] [Green Version]
- Krämer, N.; Bui Khac, N.N.; Lücker, S.; Stachniss, V.; Frankenberger, R. Bonding strategies for MIH-affected enamel and dentin. Dent. Mater. 2018, 34, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Bronckers, A.L.; Lyaruu, D.M.; DenBesten, P.K. The impact of fluoride on ameloblasts and the mechanisms of enamel fluorosis. J. Dent Res. 2009, 88, 877–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.; Li, J.Z.; Zuo, Q.L.; Liu, C.; Jiang, H.; Du, M.Q. Accelerated aging effects on color, microhardness and microstructure of ICON resin infiltration. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 7722–7731. [Google Scholar] [PubMed]
- Horowitz, H.S.; Driscoll, W.S.; Meyers, R.J.; Heifetz, S.B.; Kingman, A. A new method for assessing the prevalence of dental fluorosis--the Tooth Surface Index of Fluorosis. J. Am. Dent. Assoc. 1984, 109, 37–41. [Google Scholar] [CrossRef]
- Sundfeld, D.; Pavani, C.C.; Pini, N.I.P.; Machado, L.S.; Schott, T.C.; Sundfeld, R.H. Enamel microabrasion and dental bleaching on teeth presenting severe-pitted enamel fluorosis: A case report. Oper. Dent. 2019, 44, 566–573. [Google Scholar] [CrossRef]
- Pini, N.I.P.; Lima, D.A.N.L.; Ambrosano, G.M.B.; da Silva, W.J.; Aguiar, F.H.B.; Lovadino, J.R. Effects of acids used in the microabrasion technique: Microhardness and confocal microscopy analysis. J. Clin. Exp. Dent. 2015, 7, e506–e512. [Google Scholar] [CrossRef]
- Croll, T.P.; Cavanaugh, R.R. Enamel color modification by controlled hydrochloric acid-pumice abrasion. I. technique and examples. Quintessence Int. 1986, 17, 81–87. [Google Scholar]
- Croll, T.P.; Cavanaugh, R.R. Enamel color modification by controlled hydrochloric acid-pumice abrasion. II. Further examples. Quintessence Int. 1986, 17, 157–164. [Google Scholar]
- Sundfeld, R.H.; Franco, L.M.; Gonçalves, R.S.; de Alexandre, R.S.; Machado, L.S.; Neto, D.S. Accomplishing esthetics using enamel microabrasion and bleaching—A case report. Oper. Dent. 2014, 39, 223–227. [Google Scholar] [CrossRef] [Green Version]
- Yetkiner, E.; Wegehaupt, F.; Wiegand, A.; Attin, R.; Attin, T. Colour improvement and stability of white spot lesions following infiltration, micro-abrasion, or fluoride treatments in vitro. Eur. J. Orthod. 2014, 36, 595–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdullah, Z.; John, J. Minimally Invasive Treatment of White Spot Lesions -A Systematic Review. Oral. Health Prev. Dent. 2016, 14, 197–205. [Google Scholar]
- Pliska, B.T.; Warner, G.A.; Tantbirojn, D.; Larson, B.E. Treatment of white spot lesions with ACP paste and microabrasion. Angle. Orthod. 2012, 82, 765–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paula, A.B.P.; Fernandes, A.R.; Coelho, A.S.; Marto, C.M.; Ferreira, M.M.; Caramelo, F.; do Vale, F.; Carrilho, E. Therapies for White Spot Lesions—A Systematic Review. J. Evid. Based Dent. Pract. 2017, 17, 23–38. [Google Scholar] [CrossRef] [PubMed]
- Ashfaq, N.M.; Grindrod, M.; Barry, S. A discoloured anterior tooth: Enamel microabrasion. Br. Dent. J. 2019, 226, 486–489. [Google Scholar] [CrossRef]
- Hallgren, K.; Akyalcin, S.; English, J.; Tufekci, E.; Paravina, R.D. Color Properties of Demineralized Enamel Surfaces Treated with a Resin Infiltration System. J. Esthet. Restor. Dent. 2016, 28, 339–346. [Google Scholar] [CrossRef]
- Scholz, K.J.; Federlin, M.; Hiller, K.A.; Ebensberger, H.; Ferstl, G.; Buchalla, W. EDX-analysis of fluoride precipitation on human enamel. Sci. Rep. 2019, 9, 13442. [Google Scholar] [CrossRef] [Green Version]
- Romero, M.F.; Babb, C.S.; Delash, J.; Brackett, W.W. Minimally invasive esthetic improvement in a patient with dental fluorosis by using microabrasion and bleaching: A clinical report. J. Prosthet. Dent. 2018, 120, 323–326. [Google Scholar] [CrossRef]
- Sundfeld, R.H.; Croll, T.P.; Briso, A.L.; Alexandre, R.S.; Neto, D.S. Considerations about enamel microabrasion after 18 years. Am. J. Dent. 2007, 20, 67–72. [Google Scholar]
- Zenouz, G.A.; Ezoji, F.; Enderami, S.A.; Khafri, S. Effect of Fluoride, Casein Phosphopeptide-Amorphous Calcium Phosphate and Casein Phosphopeptide-Amorphous Calcium Phosphate Fluoride on Enamel Surface Microhardness After Microabrasion: An in Vitro Study. J. Dent. 2015, 12, 705–711. [Google Scholar]
- Vasconcelos, M.Q.S.B.; Vieira, K.A.; Salgueiro, M.C.C.; Alfaya, T.A.; Ferreira, C.S.; Bussadori, S.K. Microabrasion: A treatment option for white spots. J. Clin. Pediatr. Dent. 2014, 39, 27–29. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manaia, M.; Rocha, L.; Saraiva, J.; Coelho, A.; Amaro, I.; Marto, C.M.; Vale, F.; Ferreira, M.M.; Paula, A.; Carrilho, E. Minimally Invasive Dentistry for Pre-Eruptive Enamel Lesions—A Case Series. Appl. Sci. 2021, 11, 4732. https://doi.org/10.3390/app11114732
Manaia M, Rocha L, Saraiva J, Coelho A, Amaro I, Marto CM, Vale F, Ferreira MM, Paula A, Carrilho E. Minimally Invasive Dentistry for Pre-Eruptive Enamel Lesions—A Case Series. Applied Sciences. 2021; 11(11):4732. https://doi.org/10.3390/app11114732
Chicago/Turabian StyleManaia, Mariana, Larissa Rocha, José Saraiva, Ana Coelho, Inês Amaro, Carlos Miguel Marto, Francisco Vale, Manuel Marques Ferreira, Anabela Paula, and Eunice Carrilho. 2021. "Minimally Invasive Dentistry for Pre-Eruptive Enamel Lesions—A Case Series" Applied Sciences 11, no. 11: 4732. https://doi.org/10.3390/app11114732