Bone Healing and Regeneration Potential in Rabbit Cortical Defects Using an Innovative Bioceramic Bone Graft Substitute

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Study Design
2.3. Implantation Procedure
2.4. Micro-Computed Tomographic (μ-CT) Evaluation
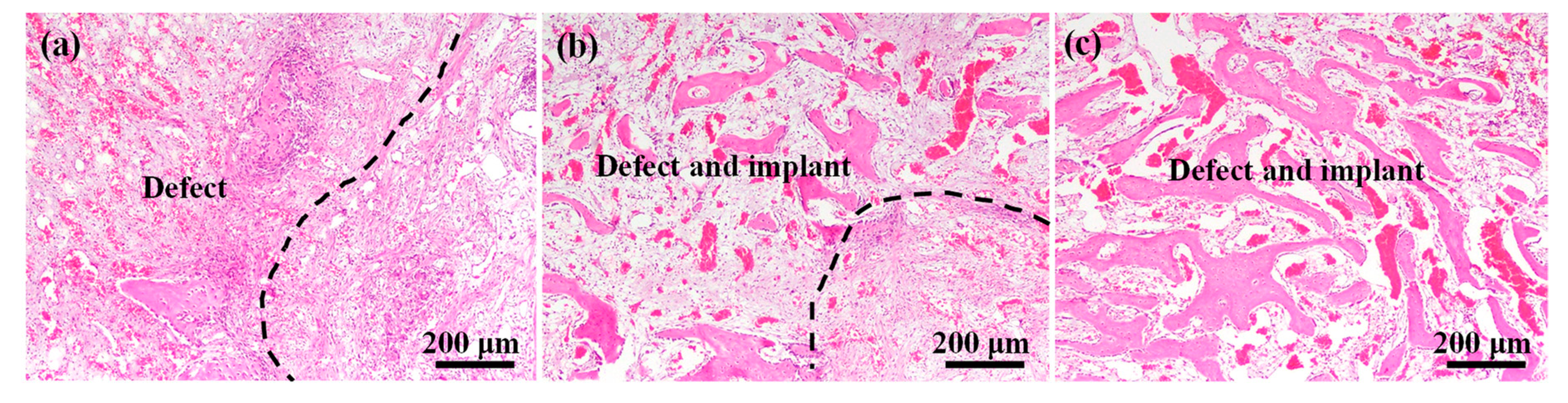
2.5. Histopathological Analysis
2.6. Statistical Analysis
3. Results and Discussion
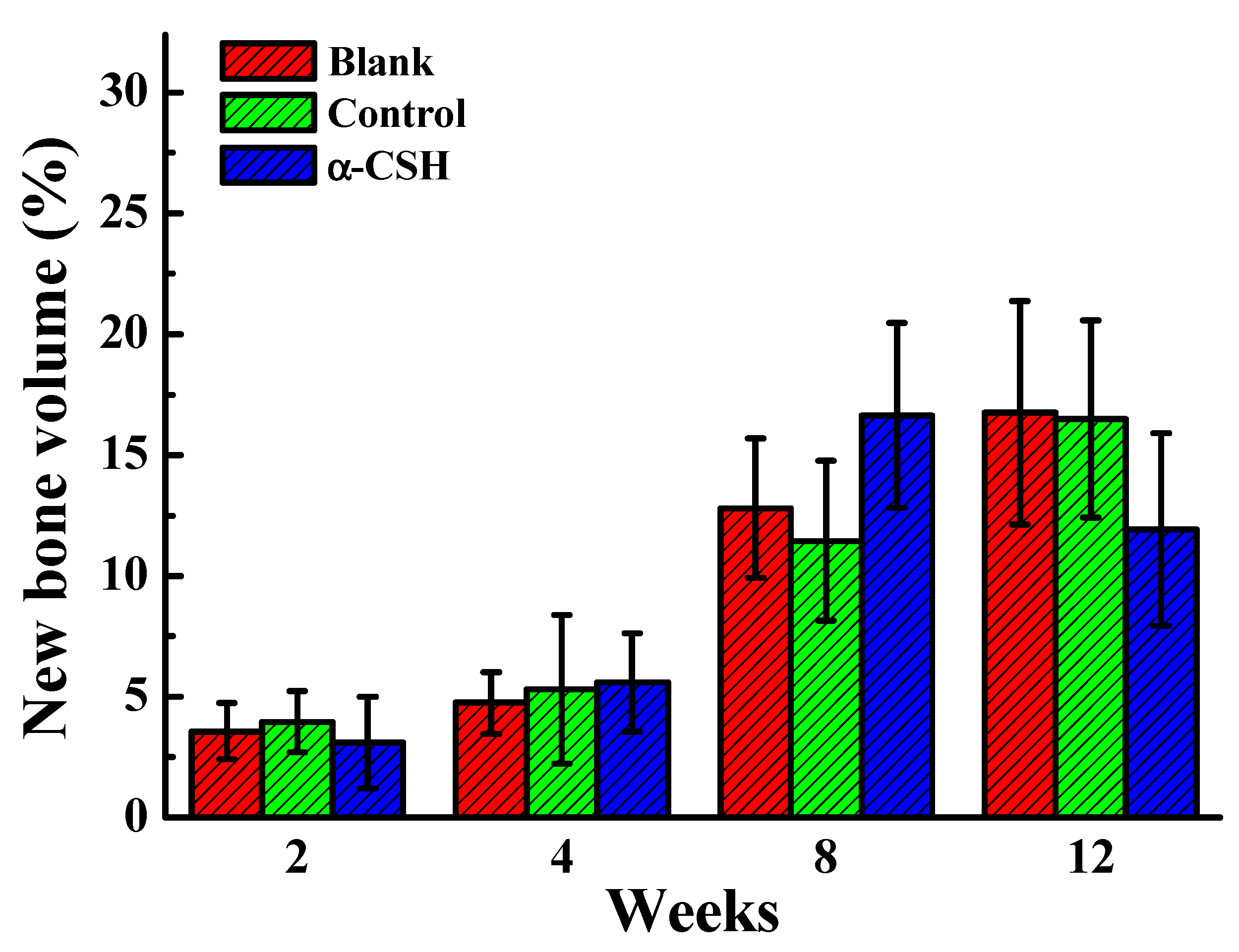
3.1. Bone Healing Features of the Implanted Materials
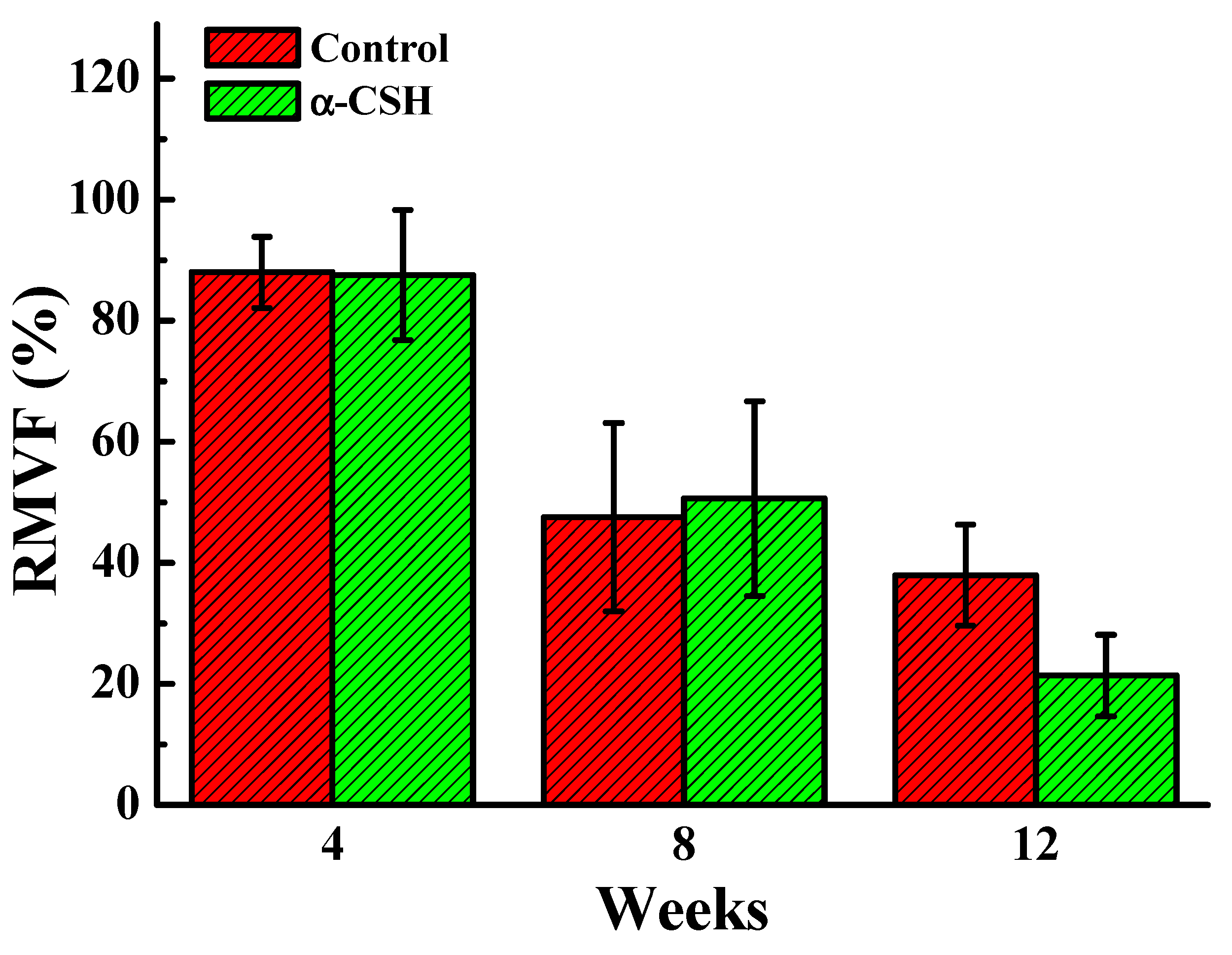
3.2. Degradation Properties of the Implanted Materials
3.3. Bone Regeneration Characteristics of the Implanted Materials
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Smrke, D.; Roman, P.; Veselko, M.; Gubi, B. Treatment of bone defects—allogenic platelet gel and autologous bone technique. In Regenerative Medicine and Tissue Engineering; IntechOpen: London, UK, 2013. [Google Scholar]
- Xiang, H.; Wang, Y.; Chang, H.; Yang, S.; Tu, M.; Zhang, X.; Yu, B. Cerium-containing α-calcium sulfate hemihydrate bone substitute promotes osteogenesis. J. Biomater. Appl. 2019, 34, 250–260. [Google Scholar] [CrossRef] [PubMed]
- De Grado, G.F.; Keller, L.; Idoux-Gillet, Y.; Wagner, Q.; Musset, A.-M.; Benkirane-Jessel, N.; Bornert, F.; Offner, D. Bone substitutes: A review of their characteristics, clinical use, and perspectives for large bone defects management. J. Tissue Eng. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Zhou, Y.; Yang, S.; Li, J.J.; Li, X.; Ma, Y.; Hou, Y.; Jiang, N.; Xu, C.; Zhang, S.; et al. Novel bone substitute composed of chitosan and strontium-doped α-calcium sulfate hemihydrate: Fabrication, characterisation and evaluation of biocompatibility. Mater. Sci. Eng. C 2016, 66, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Calori, G.M.; Mazza, E.; Colombo, M.; Ripamonti, C. The use of bone-graft substitutes in large bone defects: Any specific needs? Injury 2011, 42, S56–S63. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Yu, Z.; Chang, H.; Wang, Y.; Xiang, H.; Zhang, X.; Yu, B. Strontium-containing α-calcium sulfate hemihydrate promotes bone repair via the TGF-β/Smad signaling pathway. Mol. Med. Rep. 2019, 20, 3555–3564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pförringer, D.; Harrasser, N.; Mühlhofer, H.; Kiokekli, M.; Stemberger, A.; Van Griensven, M.; Lucke, M.; Burgkart, R.; Obermeier, A. Osteoinduction and -conduction through absorbable bone substitute materials based on calcium sulfate: In vivo biological behavior in a rabbit model. J. Mater. Sci. Mater. Electron. 2018, 29, 17. [Google Scholar] [CrossRef]
- Leventis, M.; Fairbairn, P.; Mangham, C.; Galanos, A.; Vasiliadis, O.; Papavasileiou, D.; Horowitz, R. Bone Healing in Rabbit Calvaria Defects Using a Synthetic Bone Substitute: A Histological and Micro-CT Comparative Study. Materials 2018, 11, 2004. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Garcés, M.Á.; Camps-Font, O.; Escoda-Francolí, J.; Muñoz-Guzón, F.; Toledano-Serrabona, J.; Gay-Escoda, C. Short time guided bone regeneration using beta-tricalcium phosphate with and without fibronectin–An experimental study in rats. Medicina Oral Patología Oral Cirugia Bucal 2020. [Google Scholar] [CrossRef]
- Yamada, M.; Egusa, H. Current bone substitutes for implant dentistry. J. Prosthodont. Res. 2018, 62, 152–161. [Google Scholar] [CrossRef]
- Sohn, H.-S.; Oh, J.-K. Review of bone graft and bone substitutes with an emphasis on fracture surgeries. Biomater. Res. 2019, 23, 9. [Google Scholar] [CrossRef] [Green Version]
- Auston, D.A.; Feibert, M.; Craig, T.; Damron, T. Unexpected radiographic lucency following grafting of bone defects with calcium sulfate/tricalcium phosphate bone substitute. Skelet. Radiol. 2015, 44, 1453–1459. [Google Scholar] [CrossRef]
- Lobb, D.C.; DeGeorge, B.R.; Chhabra, A.B. Bone Graft Substitutes: Current Concepts and Future Expectations. J. Hand Surg. 2019, 44, 497–505.e2. [Google Scholar] [CrossRef] [PubMed]
- Rolvien, T.; Barbeck, M.; Wenisch, S.; Amling, M.; Krause, M. Cellular Mechanisms Responsible for Success and Failure of Bone Substitute Materials. Int. J. Mol. Sci. 2018, 19, 2893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, M.-L.; Fu, Y.-C.; Wang, Y.-H.; Chen, C.-H.; Wang, C.-K.; Wang, G.-J. Combination of calcium sulfate and simvastatin-controlled release microspheres enhances bone repair in critical-sized rat calvarial bone defects. Int. J. Nanomed. 2015, 10, 7231–7240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, S.; Wang, L.; Feng, S.; Yang, Q.; Yu, B.; Tu, M. Enhanced bone formation by strontium modified calcium sulfate hemihydrate in ovariectomized rat critical-size calvarial defects. Biomed. Mater. 2017, 12, 035004. [Google Scholar] [CrossRef]
- Pei, F.; Li, Y.; Yang, J.; Yang, X.; Huang, Q.; Shen, B. Evaluation of a biodegradable graft substitute in rabbit bone defect model. Indian J. Orthop. 2012, 46, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Shih, T.C.; Chang, W.J.; Yang, J.C.; Feng, S.W.; Lin, C.T.; Teng, N.C. In vivo evaluation of resorbable bone graft substitutes in mandibular sockets of the beagle. J. Biomed. Mater. Res. Part A 2012, 100, 2726–2731. [Google Scholar] [CrossRef]
- Kuo, T.-F.; Lee, S.-Y.; Wu, H.-D.; Poma, M.; Wu, Y.-W.; Yang, J.-C. An in vivo swine study for xeno-grafts of calcium sulfate-based bone grafts with human dental pulp stem cells (hDPSCs). Mater. Sci. Eng. C 2015, 50, 19–23. [Google Scholar] [CrossRef]
- Yang, G.; Liu, J.; Li, F.; Pan, Z.; Ni, X.; Shen, Y.; Xu, H.; Huang, Q. Bioactive calcium sulfate/magnesium phosphate cement for bone substitute applications. Mater. Sci. Eng. C 2014, 35, 70–76. [Google Scholar] [CrossRef]
- Meng, Z.L.; Wu, Z.Q.; Shen, B.X.; Li, H.B.; Bian, Y.Y.; Zeng, D.L.; Fu, J.; Peng, L. Reconstruction of large segmental bone defects in rabbit using the Masquelet technique with α-calcium sulfate hemihydrate. J. Orthop. Surg. Res. 2019, 14, 1–12. [Google Scholar] [CrossRef]
- Campana, V.; Milano, G.; Pagano, E.; Barba, M.; Cicione, C.; Salonna, G.; Lattanzi, W.; Logroscino, G. Bone substitutes in orthopaedic surgery: From basic science to clinical practice. J. Mater. Sci. Mater. Electron. 2014, 25, 2445–2461. [Google Scholar] [CrossRef]
- Orsini, G.; Ricci, J.; Scarano, A.; Pecora, G.; Petrone, G.; Iezzi, G.; Piattelli, A. Bone-defect healing with calcium-sulfate particles and cement: An experimental study in rabbit. J. Biomed. Mater. Res. 2004, 68, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Guarnieri, R.; Grassi, R.; Ripari, M.; Pecora, G. Maxillary sinus augmentation using granular calcium sulfate (surgiplaster sinus): Radiographic and histologic study at 2 years. Int. J. Periodontics Restor. Dent. 2006, 26, 79–85. [Google Scholar]
- Bagoff, R.; Mamidwar, S.; Chesnoiu-Matei, I.; Ricci, J.L.; Alexander, H.; Tovar, N. Socket Preservation and Sinus Augmentation Using a Medical Grade Calcium Sulfate Hemihydrate and Mineralized Irradiated Cancellous Bone Allograft Composite. J. Oral Implant. 2013, 39, 363–371. [Google Scholar] [CrossRef]
- Guarnieri, R.; Pecora, G.; Fini, M.; Aldini, N.N.; Giardino, R.; Orsini, G.; Piattelli, A. Medical Grade Calcium Sulfate Hemihydrate in Healing of Human Extraction Sockets: Clinical and Histological Observations at 3 Months. J. Periodontol. 2004, 75, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.-J.; Waris, R.A.; Ruslin, M.; Lin, Y.-H.; Chen, C.-S.; Ou, K.-L. An innovative α-calcium sulfate hemihydrate bioceramic as a potential bone graft substitute. J. Am. Ceram. Soc. 2017, 101, 419–427. [Google Scholar] [CrossRef]
- Zhang, S.; Yang, K.; Cui, F.; Jiang, Y.; E, L.; Xu, B.-H.; Liu, H. A Novel Injectable Magnesium/Calcium Sulfate Hemihydrate Composite Cement for Bone Regeneration. BioMed Res. Int. 2015, 2015, 297437. [Google Scholar] [CrossRef] [Green Version]
- Fu, L.; Xia, W.; Mellgren, T.; Moge, M.; Engqvist, H. Preparation of High Percentage? Calcium Sulfate Hemihydrate via a Hydrothermal Method. J. Biomater. Nanobiotechnol. 2017, 8, 36–49. [Google Scholar] [CrossRef] [Green Version]
- Combe, E.C.; Smith, D.C. Studies on the preparation of calcium sulphate hemihydrate by an autoclave process. J. Appl. Chem. 2007, 18, 307–312. [Google Scholar] [CrossRef]
- Mu, X.; Zhu, G.; Li, X.; Li, S.; Gong, X.; Li, H.; Sun, G. Effects of impurities on CaSO(4) crystallization in the Ca(H(2)PO(4))(2)-H(2)SO(4)-H(3)PO(4)-H(2)O system. ACS Omega 2019, 4, 12702–12710. [Google Scholar] [CrossRef] [Green Version]
- Ye, Q.; Guan, B.; Lou, W.; Yang, L.; Kong, B. Effect of particle size distribution on the hydration and compressive strength development of α-calcium sulfate hemihydrate paste. Powder Technol. 2011, 207, 208–214. [Google Scholar] [CrossRef]
- Teoreanu, I.; Preda, M.; Melinescu, A. Synthesis and characterization of hydroxyapatite by microwave heating using CaSO4· 2H2O and Ca(OH)2 as calcium source. J. Mater. Sci. Mater. Med. 2008, 19, 517–523. [Google Scholar] [CrossRef]
- Chen, Z.; Liu, H.; Liu, X.; Lian, X.; Guo, Z.; Jiang, H.-J.; Cui, F.-Z. Improved workability of injectable calcium sulfate bone cement by regulation of self-setting properties. Mater. Sci. Eng. C 2013, 33, 1048–1053. [Google Scholar] [CrossRef] [PubMed]
- Guan, B.; Ye, Q.; Zhang, J.; Lou, W.; Wu, Z. Interaction between α-calcium sulfate hemihydrate and superplasticizer from the point of adsorption characteristics, hydration and hardening process. Cem. Concr. Res. 2010, 40, 253–259. [Google Scholar] [CrossRef]
- Saghiri, M.A.; Asatourian, A.; Garcia-Godoy, F.; Sheibani, N. The role of angiogenesis in implant dentistry part II: The effect of bone-grafting and barrier membrane materials on angiogenesis. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e526–e537. [Google Scholar] [CrossRef] [PubMed]
- Schindeler, A.; McDonald, M.M.; Bokko, P.; Little, D.G. Bone remodeling during fracture repair: The cellular picture. Semin. Cell Dev. Biol. 2008, 19, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Rentsch, C.; Schneiders, W.; Manthey, S.; Rentsch, B.; Rammelt, S. Comprehensive histological evaluation of bone implants. Biomatter 2014, 4, e27993. [Google Scholar] [CrossRef]
- Marsell, R.; Einhorn, T. The biology of fracture healing. Injury 2011, 42, 551–555. [Google Scholar] [CrossRef] [Green Version]
- Yoo, Y.-M.; Lee, M.-H.; Park, J.H.; Seo, D.-H.; Lee, S.; Jung, B.; Kim, H.-S.; Bae, K. Decreased Bone Volume and Bone Mineral Density in the Tibial Trabecular Bone Is Associated with Per2 Gene by 405 nm Laser Stimulation. Int. J. Mol. Sci. 2015, 16, 27401–27410. [Google Scholar] [CrossRef]
- Dimitriou, R.; Jones, E.; McGonagle, D.; Giannoudis, P.V. Bone regeneration: Current concepts and future directions. BMC Med. 2011, 9, 66. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Tresguerres-Hernández-Gil, I.; Alobera-Gracia, M.A.; Del-Canto-Pingarrón, M.; Blanco-Jerez, L. Physiological bases of bone regeneration II. The remodeling process. Med. Oral Patol. Oral Cir. Bucal 2006, 11, E151–E157. [Google Scholar] [PubMed]
- Kim, J.H.; Oh, J.H.; Han, I.; Kim, H.-S.; Chung, S.W. Grafting Using Injectable Calcium Sulfate in Bone Tumor Surgery: Comparison with Demineralized Bone Matrix-based Grafting. Clin. Orthop. Surg. 2011, 3, 191–201. [Google Scholar] [CrossRef]
- Strocchi, R.; Orsini, G.; Iezzi, G.; Scarano, A.; Rubini, C.; Pecora, G.; Piattelli, A. Bone regeneration with calcium sulfate: Evidence for increased angiogenesis in rabbits. J. Oral Implantol. 2002, 28, 273–278. [Google Scholar] [CrossRef] [Green Version]
- Kumar, Y.; Nalini, K.; Menon, J.; Patro, D.K.; Banerji, B. Calcium Sulfate as Bone Graft Substitute in the Treatment of Osseous Bone Defects, A Prospective Study. J. Clin. Diagn. Res. 2013, 7, 2926–2928. [Google Scholar] [CrossRef] [PubMed]
- Ruga, E.; Gallesio, C.; Chiusa, L.; Boffano, P. Clinical and Histologic Outcomes of Calcium Sulfate in the Treatment of Postextraction Sockets. J. Craniofacial Surg. 2011, 22, 494–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toloue, S.M.; Chesnoiu-Matei, I.; Blanchard, S.B. A Clinical and Histomorphometric Study of Calcium Sulfate Compared with Freeze-Dried Bone Allograft for Alveolar Ridge Preservation. J. Periodontol. 2012, 83, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Cortez, P.P.; Silva, M.A.; Santos, M.; Armada-da-Silva, P.; Afonso, A.; Lopes, M.A.; Santos, J.D.; Maurício, A.C. A glass-reinforced hydroxyapatite and surgical-grade calcium sulfate for bone regeneration: In vivo biological behavior in a sheep model. J. Biomater. Appl. 2012, 27, 201–217. [Google Scholar] [CrossRef]
- Von Rechenberg, B.; Génot, O.R.; Nuss, K.; Galuppo, L.; Fulmer, M.; Jacobson, E.; Kronen, P.; Zlinszky, K.; Auer, J.A. Evaluation of four biodegradable, injectable bone cements in an experimental drill hole model in sheep. Eur. J. Pharm. Biopharm. 2013, 85, 130–138. [Google Scholar] [CrossRef]
- Mao, K.; Zhou, F.; Cui, F.; Li, J.; Hou, X.; Li, P.; Du, M.; Liang, M.; Wang, Y. Preparation and properties of α-calcium sulphate hemihydrate and β-tricalcium phosphate bone substitute. Bio-Med. Mater. Eng. 2013, 23, 197–210. [Google Scholar] [CrossRef]









© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ou, K.-L.; Hou, P.-J.; Huang, B.-H.; Chou, H.-H.; Yang, T.-S.; Huang, C.-F.; Ueno, T. Bone Healing and Regeneration Potential in Rabbit Cortical Defects Using an Innovative Bioceramic Bone Graft Substitute. Appl. Sci. 2020, 10, 6239. https://doi.org/10.3390/app10186239
Ou K-L, Hou P-J, Huang B-H, Chou H-H, Yang T-S, Huang C-F, Ueno T. Bone Healing and Regeneration Potential in Rabbit Cortical Defects Using an Innovative Bioceramic Bone Graft Substitute. Applied Sciences. 2020; 10(18):6239. https://doi.org/10.3390/app10186239
Chicago/Turabian StyleOu, Keng-Liang, Ping-Jen Hou, Bai-Hung Huang, Hsin-Hua Chou, Tzu-Sen Yang, Chiung-Fang Huang, and Takaaki Ueno. 2020. "Bone Healing and Regeneration Potential in Rabbit Cortical Defects Using an Innovative Bioceramic Bone Graft Substitute" Applied Sciences 10, no. 18: 6239. https://doi.org/10.3390/app10186239