Evaluation of Cross-Sectional Root Canal Shape and Presentation of New Classification of Its Changes Using Cone-Beam Computed Tomography Scanning

Abstract
:1. Introduction
2. Materials and Methods
- Type I: Incomplete isthmus between two canals.
- Type II: A complete isthmus between two canals.
- Type III: A short, complete isthmus between two canals.
- Type IV: A complete or incomplete isthmus between three or more canals.
- Type V: two or three canals without obvious connection between them.
3. Results
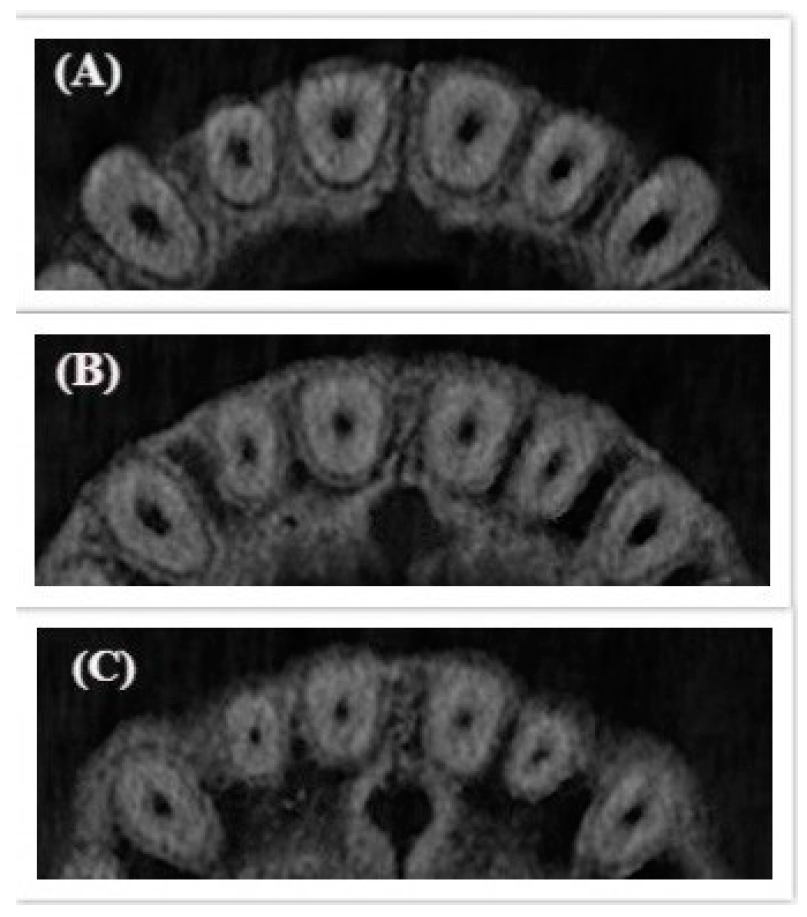
3.1. Anterior Teeth
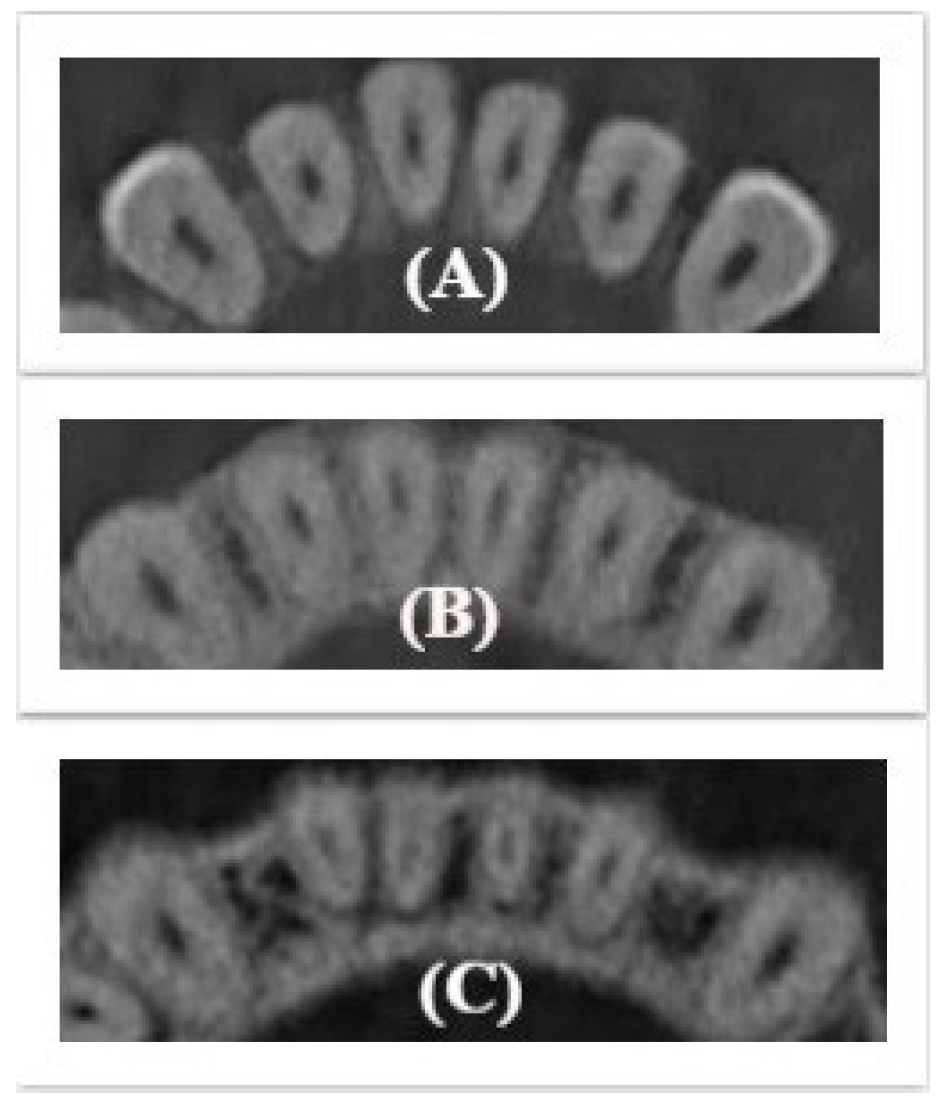
3.2. Premolars Teeth
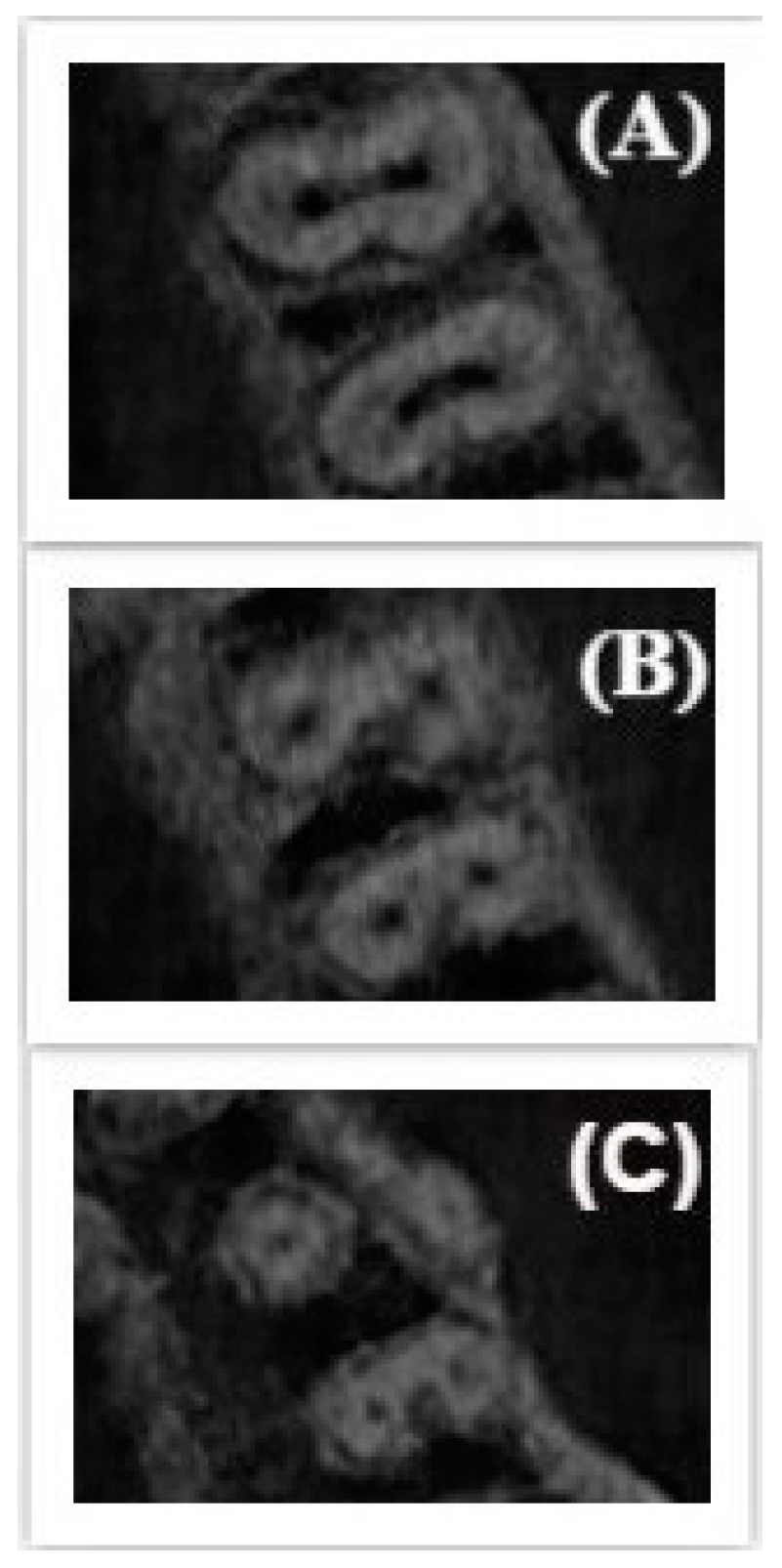
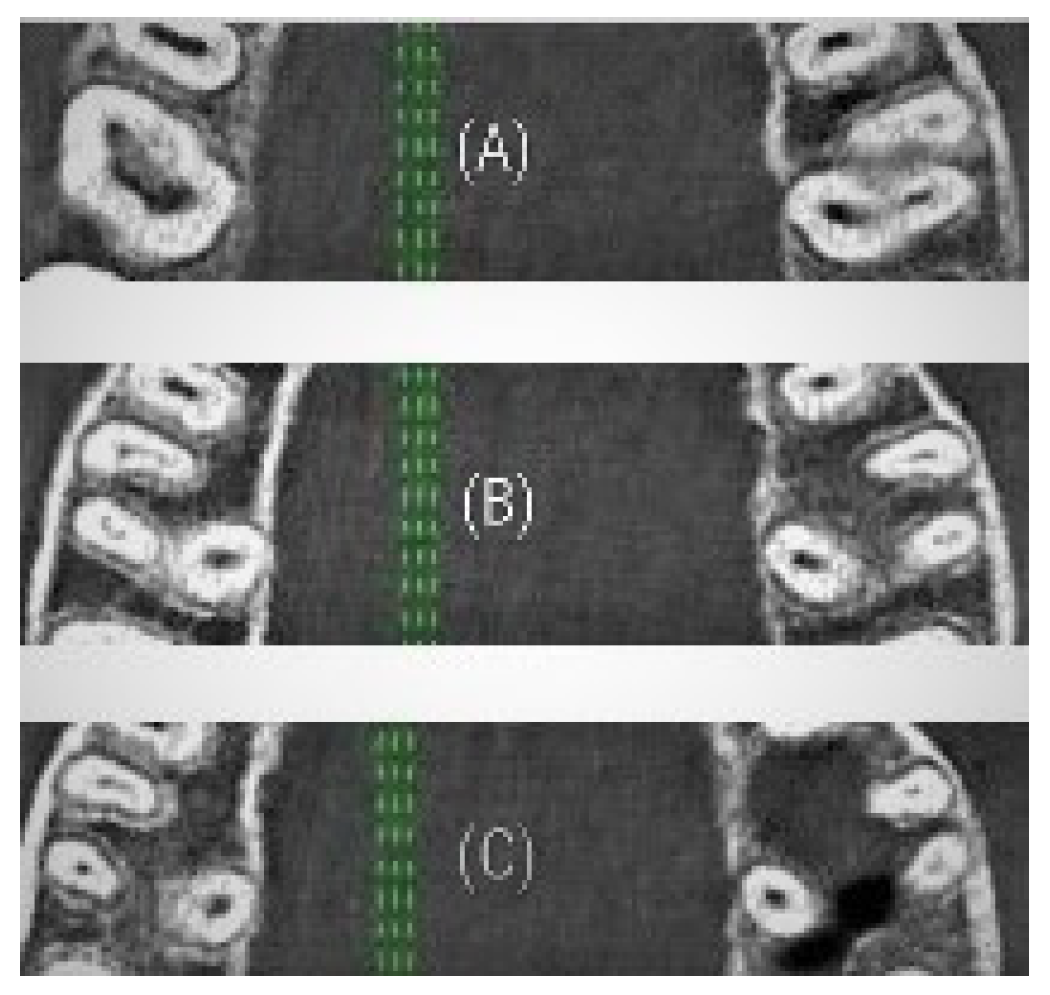
3.3. Molars Teeth
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Razumova, S.; Brago, A.; Khaskhanova, L.; Howijieh, A.; Barakat, H.; Manvelyan, A. A Cone-Beam Computed Tomography Scanning of the Root Canal System of Permanent Teeth among the Moscow Population. Int. J. Dent. 2018, 2018, 2615746. [Google Scholar] [CrossRef] [PubMed]
- Valenti-Obino, F.; Di Nardo, D.; Quero, L.; Miccoli, G.; Gambarini, G.; Testarelli, L.; Galli, M. Symmetry of root and root canal morphology of mandibular incisors: A cone-beam computed tomography study in vivo. J. Clin. Exp. Dent. 2019, 11, 527. [Google Scholar] [CrossRef] [PubMed]
- Boschetti, E.; Silva-Sousa, Y.T.C.; Mazzi-Chaves, J.F.; Leoni, G.B.; Versiani, M.A.; Pecora, J.D.; Saquy, P.C.; de Sousa-Neto, M.D. Micro-CT Evaluation of Root and Canal Morphology of Mandibular First Premolars with Radicular Grooves. Braz. Dent. J. 2017, 28, 597–603. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.K.; R’oris, A.; Barkis, D.; Wesselink, P.R. Prevalence and extent of long oval canals in the apical third. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 89, 739–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jou, Y.T.; Karabuchak, B.; Levin, J.; Liu, D. Endodontic working width: Current concepts and techniques. Dent. Clin. North. Am. 2004, 48, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Kacharaju, K.R.; Hari, P.; Yee, A.; Ngo, J.; Ismail, M.F. Analysis of Mandibular Premolars Root Canal Morphology Using Radiographic and Cross-Sectional Techniques in Malaysian Population. Dent. Hypotheses 2019, 10, 9–14. [Google Scholar] [CrossRef]
- Mehrvarzfar, P.; Akhlagi, N.M.; Khodaei, F.; Shojaee, G.; Shirazi, S. Evaluation of isthmus prevalence, location, and types in mesial roots of mandibular molars in the Iranian Population. Dent. Res. J. (Isfahan) 2014, 11, 251–256. [Google Scholar]
- Martins, J.N.; Mata, A.; Marques, D.; Anderson, C. Prevalence and Characteristics of the Maxillary C-shaped Molar. J. Endod. 2016, 42, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.; Kim, S. The resected root surface: The issue of canal isthmuses. Dent. Clin. N. Am. 1997, 3, 529–540. [Google Scholar]
- Kim, S.; Pecora, G.; Rubinstein, R. Color Atlas of Microsurgery in Endodontics; WB Saunders: Philadelphia, PA, USA, 2001; pp. 125–150. [Google Scholar]
- Teixeira, F.B.; Sano, C.L.; Gomes, B.P.; Zaia, A.A. A preliminary in vitro study of the incidence and position of the root canal isthmus in maxillary and mandibular first molars. Int. Endod. J. 2003, 36, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Mohammadzadeh-Akhlaghi, N.; Mehrvarzfar, P.; Hossein, M.; Dds, Z. Incidence, location, and type of isthmus in mandibular second molars among individuals of an Iranian population. J. Oral. Health Oral Epidemiol. 2018, 7, 59–63. [Google Scholar]
- Shrestha, S.; Karki, S.; Agrawal, N.; Vikram, M. Prevalence of Different Types of Apical Root Canal Morphology and their Treatment Recommendations in an Institute. J. Nepal. Med. Assoc. 2018, 56, 616–620. [Google Scholar] [CrossRef]
- Pécora, J.D.; Estrela, C.; Bueno, M.R.; Porto, O.C.; Alencar, A.H.; Sousa-Neto, M.; de Araújo Estrela, C.R. Detection of Root Canal Isthmuses in Molars by Map-Reading Dynamic using CBCT images. Braz. Dent. J. 2013, 24, 569–574. [Google Scholar]
- Uma, C.H.; Ramachandran, S.; Indira, R.; Shankar, P. Canal and isthmus morphology in mandibular incisors – An in vitro study. J. Endod. 2004, 16, 7–11. [Google Scholar]
- Peters, O.A.; Peters, C.I.; Schönenberger, K.; Barbakow, F. ProTaper rotary root canal preparation: Effects of canal anatomy on final shape analysed by micro CT. Int. Endod. J. 2003, 36, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Lacerda, M.F.; Marceliano-Alves, M.F.; Pérez, A.R.; Provenzano, J.C. Cleaning and shaping oval canals with 3 instrumentation systems: A correlative micro-computed tomographic and histologic study. J. Endod. 2017, 43, 1878–1884. [Google Scholar] [CrossRef]
- Sousa-Neto, M.D.; Silva-Sousa, Y.C.; Mazzi-Chaves, J.F.; Teodoro Carvalho, K.K. Root canal preparation using micro-computed tomography analysis: A literature review. Braz. Oral. Res. 2018, 32, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkaabi, W.; AlShwaimi, E.; Farooq, I.; Goodis, H.; Chogle, S. A Micro-Computed Tomography Study of the Root Canal Morphology of Mandibular First Premolars in an Emirati Population. Med. Princ. Pract. 2017, 26, 118–124. [Google Scholar] [CrossRef]
- Zhu, L.N.; Qian, W.H.; Hong, J. A cone-beam computed tomography study of changes in canal isthmus of maxillary first premolars before and after instrumentation. Shanghai Kou Qiang Yi Xue 2013, 22, 41–45. [Google Scholar]
- Hu, R.C.; Cao, L.L.; Xie, W.; Hu, Y.Q. Aging changes of the root canal morphology in maxillary first premolars observed by cone-beam computerized tomography. Zhonghua Kou Qiang Yi Xue Za Zhi 2016, 51, 224–229. [Google Scholar] [CrossRef]
- Hu, R.C.; Xie, W.; Hu, Y.Q.; Piao, Z.G. Root canal anatomy of maxillary second premolars at various ages observed by cone-beam CT. Zhonghua Kou Qiang Yi Xue Za Zhi 2019, 54, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Zuolo, M.L.; Zaia, A.A.; Belladonna, F.G.; Silva, E.J.; Souza, E.M.; Versiani, M.A.; Lopes, R.T.; De-Deus, G. Micro-CT assessment of the shaping ability of four root canal instrumentation systems in oval-shaped canals. Int. Endod. J. 2018, 51, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Paqué, F.; Peters, O.A. Micro-computed tomography evaluation of the preparation of long oval root canals in mandibular molars with the selfadjusting file. J. Endod. 2011, 37, 517–521. [Google Scholar]
- Di Nardo, D.; Gambarini, G.; Miccoli, G.; Di Carlo, S.; Iannarilli, G.; Lauria, G.; Seracchiani, M.; Khrenova, T.; Bossù, M.; Testarelli, L. Sonic vs Ultrasonic activation of sodium hypoclorite for root canal treatments. In vitro assessment of debris removal from main and lateral canals. Giornale Italiano Di Endodonzia 2020, 34, 90–96. [Google Scholar]
- Fumes, A.C.; Sousa-Neto, M.D.; Leoni, G.B.; Versiani, M. Root canal morphology of primary molars: A micro-computed tomography study. Eur. Arch. Paediatr. Dent. 2014, 15, 317–326. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Change | Cross-Sectional Root Canal Shape | ||
|---|---|---|---|
| Change | |||
| In The Middle Third | In the Apical Third | In the Middle and Apical Thirds | |
| Anterior teeth | Mandibular incisors | Mandibular premolars and one-rooted maxillary premolars | Mandibular premolars and one-rooted maxillary premolars |
| Two-rooted maxillary premolars | One-rooted maxillary premolars | Mesio-buccal canals maxillary molars | Mesio-buccal canals maxillary molars |
| Distal and palatal canals maxillary molars | Mandibular premolars | Mesial and distal canals mandibular molars | Mesial and distal canals mandibular molars |
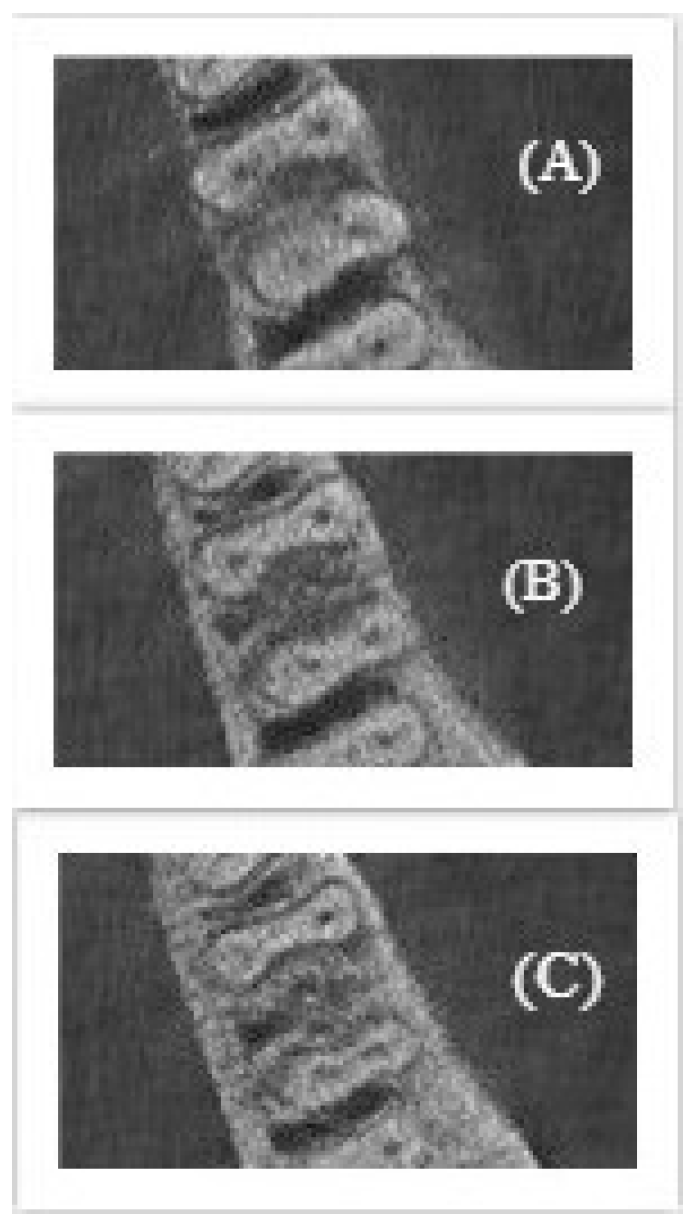
| Types | Description |
|---|---|
| Type I | Un-changed cross-sectional root canal shape from coronal to apical third |
| Type II | Changed cross-sectional root canal shape in the middle third |
| Type III | Changed cross-sectional root canal shape in the middle and apical thirds |
| Type IV | Changed cross-sectional root canal shape in the apical third |
| Young Group | Root | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|---|
| Maxillary anterior teeth | One-rooted | 100% | 0 | 0 | 0 |
| Maxillary premolars | Two-rooted | 100% | 0 | 0 | 0 |
| One-rooted | 60% | 13% | 17% | 10% | |
| Maxillary molars | MB | 5% | 6% | 49% | 40% |
| DB | 75% | 0 | 15% | 10% | |
| P | 88% | 0 | 4% | 8% | |
| Mandibular anterior teeth | One-rooted | 95% | 5% | 0 | 0 |
| Mandibular premolars | One-rooted | 36% | 8% | 40% | 16% |
| Mandibular molars | M | 68% | 0 | 12% | 20% |
| D | 46% | 0 | 28% | 26% |
| Middle Group | Root | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|---|
| Maxillary anterior teeth | One-rooted | 100% | 0 | 0 | 0 |
| Maxillary premolars | Two-rooted | 100% | 0 | 0 | 0 |
| One-rooted | 49% | 4% | 34% | 13% | |
| Maxillary molars | MB | 3% | 10% | 46% | 41% |
| DB | 71% | 0 | 11% | 18% | |
| P | 77% | 0 | 13% | 10% | |
| Mandibular anterior teeth | One-rooted | 96% | 3% | 1% | 0 |
| Mandibular premolars | One-rooted | 53% | 2% | 31% | 14% |
| Mandibular molars | M | 58% | 0 | 24% | 18% |
| D | 60% | 0 | 12% | 28% |
| Elderly Group | Root | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|---|
| Maxillary anterior teeth | One-rooted | 100% | 0 | 0 | 0 |
| Maxillary premolars | Two-rooted | 100% | 0 | 0 | 0 |
| One-rooted | 56% | 9% | 24% | 11% | |
| Maxillary molars | MB | 6% | 7% | 39% | 48% |
| DB | 76% | 0 | 9% | 15% | |
| P | 84% | 0 | 9% | 7% | |
| Mandibular anterior teeth | One-rooted | 93% | 5% | 2% | 0 |
| Mandibular premolars | One-rooted | 43% | 5% | 24% | 28% |
| Mandibular molars | M | 64% | 0 | 21% | 15% |
| D | 56% | 0 | 31% | 13% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Razumova, S.; Brago, A.; Howijieh, A.; Barakat, H.; Kozlova, Y.; Baykulova, M. Evaluation of Cross-Sectional Root Canal Shape and Presentation of New Classification of Its Changes Using Cone-Beam Computed Tomography Scanning. Appl. Sci. 2020, 10, 4495. https://doi.org/10.3390/app10134495
Razumova S, Brago A, Howijieh A, Barakat H, Kozlova Y, Baykulova M. Evaluation of Cross-Sectional Root Canal Shape and Presentation of New Classification of Its Changes Using Cone-Beam Computed Tomography Scanning. Applied Sciences. 2020; 10(13):4495. https://doi.org/10.3390/app10134495
Chicago/Turabian StyleRazumova, Svetlana, Anzhela Brago, Ammar Howijieh, Haydar Barakat, Yuliya Kozlova, and Malina Baykulova. 2020. "Evaluation of Cross-Sectional Root Canal Shape and Presentation of New Classification of Its Changes Using Cone-Beam Computed Tomography Scanning" Applied Sciences 10, no. 13: 4495. https://doi.org/10.3390/app10134495