A Measurement Software for Professional Training in Early Detection of Melanoma

 , ,
, ,
Abstract
:Featured Application
Abstract
1. Introduction
- Design and training of a new measurement system able to identify, in dermoscopic images, the seven parameters of the Seven-Point Checklist;
- Evaluation of the diagnostic reliability guaranteed by the developed system, compared to the reliability of the expert dermatologists (DE) and the non-expert (NED) groups;
- Evaluation of the capability by the automated system to improve the diagnostic confidence of NED, when used for the analysis of dermoscopic images (“semi-automatic“ diagnosis).
2. Materials and Methods
2.1. Color-Based Detection of Dermoscopic Criteria
2.2. Texture-Based Detection of Dermoscopic Criterion
2.3. Atypical Vascular Pattern(AVP)
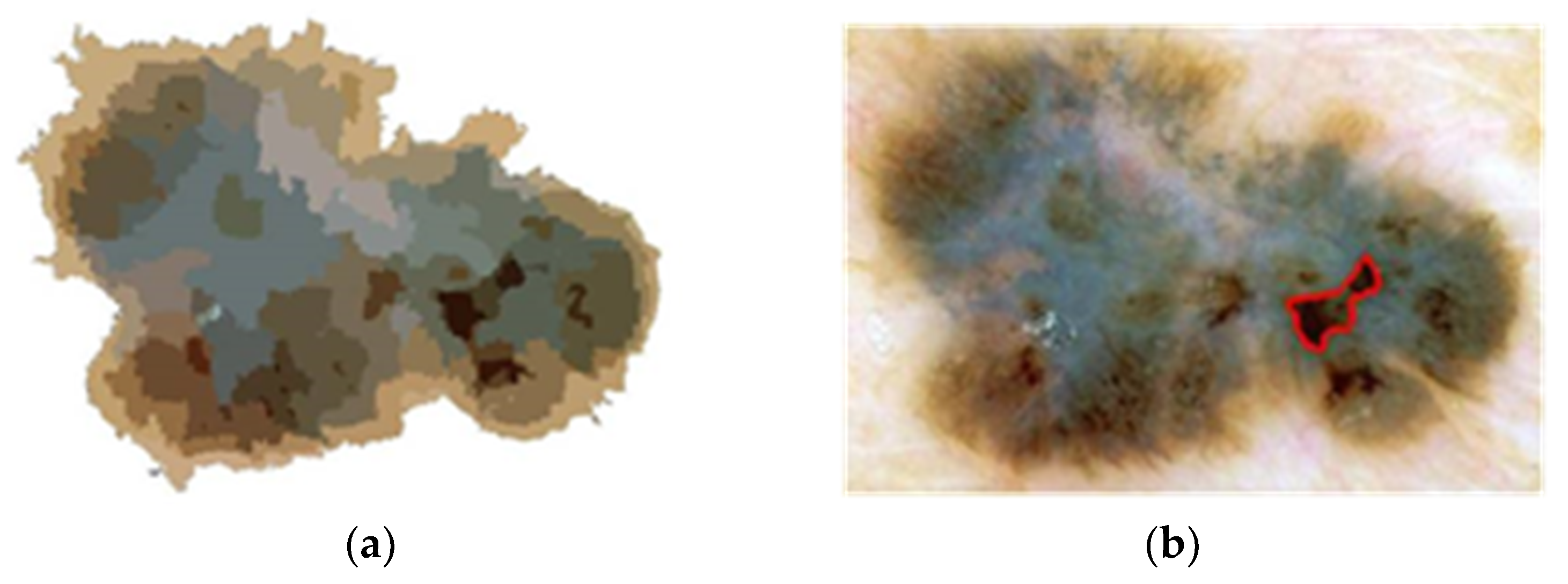
2.4. Irregular Dots and Globules
2.5. Irregular Streaks
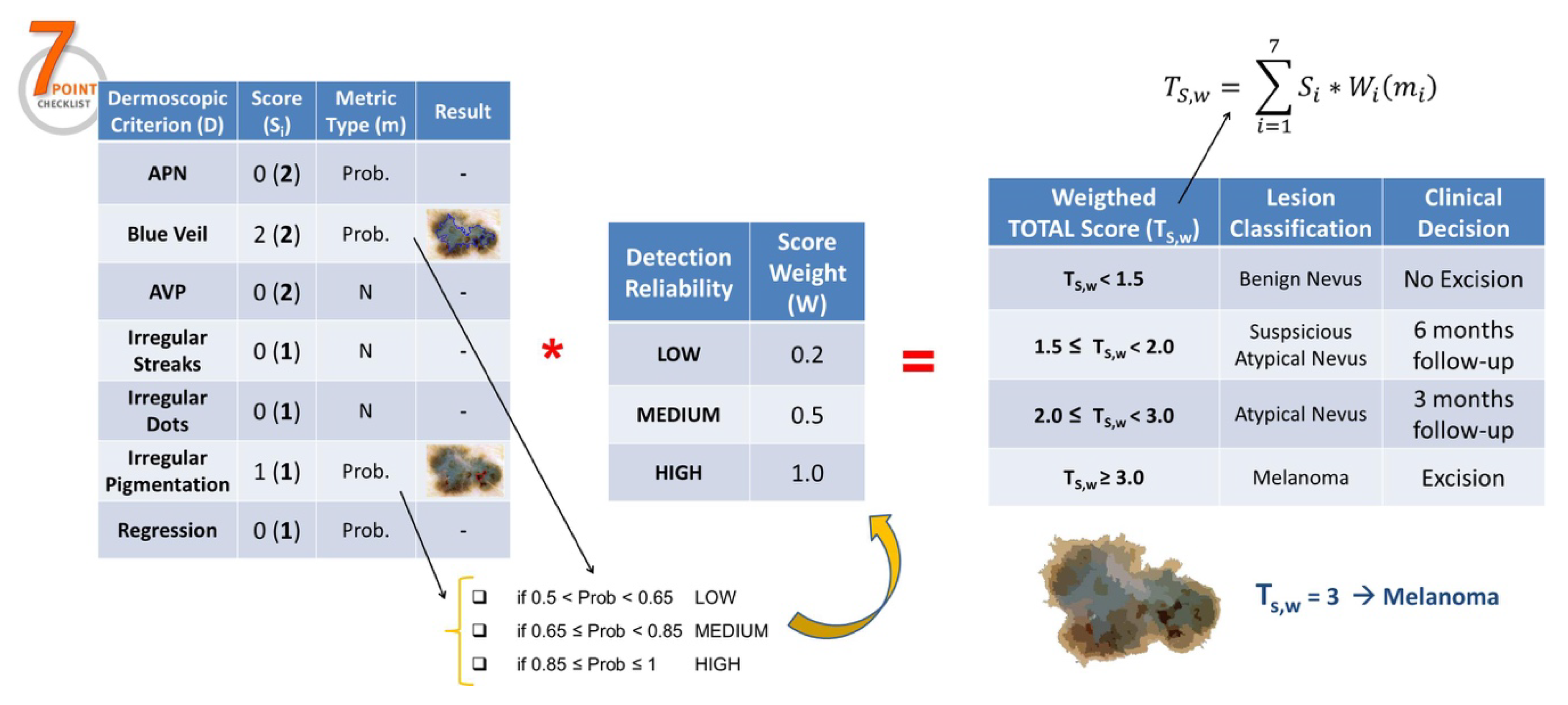
2.6. Lesion Classification
3. Results
- 107 benign nevi;
- 99 atypical nevi (73 suspicious nevi);
- 64 melanomas.
- The expert dermatologists (ED) group including 3 physicians (B.B., S.C., M.A.) with clinical activity <10 years;
- The non-expert dermatologists (NED) group including 3 physicians (C.C., A.M., F.C.) with less than 3 years’ experience in dermoscopy;
- The former performance represents the weighted mean of sensitivity (i.e., the ratio of the correct detection of melanoma and the corresponding class dimension, 64) and specificity (i.e., the ratio of the correct detection of the benign/atypical nevi and the number of lesions not classified as melanoma, 206);
- The latter performance takes into account the correct decision of both excisions (with respect to the group of lesions including melanomas and strongly atypical nevi) and of following-up/ignoring (with respect to the group of benign and suspicious nevi).
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Cancer Society. Cancer Facts & Figures. 2019. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2019/cancer-facts-and-figures-2019.pdf (accessed on 21 January 2019).
- Glocker-Reis, L.A.; Melber, D.; Krapcho, M. SEER Cancer Statistics Review 1975–2005. National Cancer Institute. 2008. Available online: https://seer.cancer.gov/csr/1975_2005/ (accessed on 23 January 2020).
- Parkin, D.M.; Bray, F.; Ferlay, J. Global cancer statistics, 2002. CA: Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef]
- Stolz, W.; Bilek, P.; Landthaler, M. Skin surface microscopy. Lancet 1989, 2, 864–865. [Google Scholar] [CrossRef]
- Clark, W.H.; From, L.; Bernardino, E.A. The histogenesis and biologic behaviour of primary human malignant melanomas of the skin. Cancer Res. 1969, 29, 705–727. [Google Scholar]
- Mihm, M.C.; Clark, W.H.; From, L. The clinical diagnosis, classification and histogenetic concepts of the early stages of cutaneous malignant melanomas. N. Engl. J. Med. 1971, 284, 1078–1082. [Google Scholar] [CrossRef] [PubMed]
- De Vries, E.; Bray, F.L.; Coebergh, J.W. Changing epidemiology of malignant cutaneous melanoma in Europe 1953–1997: Rising trends in incidence and mortality but recent stabilizations in western Europe and decreases in Scandinavia. Int. J. Cancer 2003, 107, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Tromme, I.; Sacré, L.; Hammouch, F. Availability of digital dermoscopy in daily practice dramatically reduces the number of excised melanocytic lesions: Results from an observational study. Br. J. Dermatol. 2012, 167, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Binder, M.; Schwarz, M.; Winkler, A. Epiluminescence microscopy. A useful tool for the diagnosis of pigmented skin lesions for formally trained dermatologists. Arch. Dermatol. 1995, 131, 286–291. [Google Scholar] [CrossRef]
- Kittler, H.; Pehamberger, H.; Wolff, K.; Binder, M. Diagnostic accuracy of dermoscopy. Lancet Oncol. 2002, 3, 159–165. [Google Scholar] [CrossRef]
- Piccolo, D.; Ferrari, A.; Peris, K. Dermoscopic diagnosis by a trained clinician vs. a clinician with minimal dermoscopy training vs. computer-aided diagnosis of 341 pigmented skin lesions: A comparative study. Br. J. Dermatol. 2002, 147, 481–486. [Google Scholar] [CrossRef]
- Blum, A.; Luedtke, H.; Ellwanger, U.; Schwabe, R. Digital image analysis for diagnosis of cutaneous melanoma. Development of a highly effective computer algorithm based on analysis of 837 melanocytic lesions. Br. J. Dermatol. 2004, 151, 1029–1038. [Google Scholar] [CrossRef]
- Betta, G.; Di Leo, G.; Fabbrocini, G.; Paolillo, A.; Sommella, P. Dermoscopic image-analysis system: Estimation of atypical pigment network and atypical vascular pattern. In Proceedings of the IEEE International Workshop on Medical Measurement and Applications, MeMeA 2006, Benevento, Italy, 20–21 April 2006. [Google Scholar]
- Di Leo, G.; Liguori, C.; Paolillo, A.; Sommella, P. An Improved procedure for the automatic detection of dermoscopic structures in digital ELM images of skin lesion. In Proceedings of the 2008 IEEE International Conference on Virtual Environments, Human-Computer Interfaces, and Measurement Systems, Istanbul, Turkey, 14–16 July 2008. [Google Scholar]
- Di Leo, G.; Fabbrocini, G.; Paolillo, A.; Rescigno, O.; Sommella, P. Towards an automatic diagnosis system for skin lesions: Estimation of blue-whitish veil and regression structures. In Proceedings of the 2009 6th International Multi-Conference on Systems, Signals and Devices, Djerba, Taiwan, 23–26 March 2009. [Google Scholar]
- Fabbrocini, G.; Betta, G.; Di Leo, G.; Liguori, C.; Paolillo, A.; Pietrosanto, A.; Sommella, P.; Rescigno, O.; Cacciapuoti, S.; Pastore, F.; et al. Epiluminescence image processing for melanocytic skin lesion diagnosis based on 7-Point Check-list: A preliminary discussion on three parameters. Open Dermatol. J. 2010, 4, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Di Leo, G.; Paolillo, A.; Sommella, P.; Fabbrocini, G.; Rescigno, O. A software tool for the diagnosis of melanomas automatic implementation of the 7-Point Check list method. In Proceedings of the 2010 IEEE International Instrumentation and Measurement Technology Conference, Austin, TX, USA, 3–6 May 2010. [Google Scholar]
- De Vita, V.; Di Leo, G.; Fabbrocini, G.; Paolillo, A.; Sommella, P. Statistical image processing for the detection of dermoscopic criteria. In Proceedings of the 18th IMEKO TC4 Symposium on Measurement of Electrical Quantities 2011, Natal, Brazil, 27–30 September 2011. [Google Scholar]
- Di Leo, G.; Paolillo, A.; Pietrosanto, A.; Sommella, P.; Fabbrocini, G.; Cacciapuoti, S. A distributed measurement system for dermoscopic analysis of pigmented skin lesions. In Proceedings of the 2015 IEEE International Instrumentation and Measurement Technology Conference, Pisa, Italy, 11–14 May 2015. [Google Scholar]
- Argenziano, G.; Soyer, H.P.; De Giorgi, V. Interactive Atlas of Dermoscopy; EDRA Medical Publishing & New Media: Milan, Italy, 2002. [Google Scholar]
- Landwehr, N.; Hall, M.; Frank, E. Logistic Model Trees. Mach. Learn. 2003, 59, 161–205. [Google Scholar] [CrossRef] [Green Version]
- Nock, R.; Nielsen, F. Statistical Region Merging. IEEE Trans. Pattern Anal. Mach. Intell. 2004, 26, 1452–1458. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, M.; Razmara, M.; Wighton, P.; Lee, T.K.; Atkins, M.S. A Novel Method for Detection of Pigment Network in Dermoscopic Images Using Graphs. Comput. Medi-cal Imaging Graph. 2011, 35, 137–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirk, J. Count Loops in a Network. Available online: http://www.mathworks.com/matlabcentral/fx_files/10722/1/content/html/run_loops_html.html (accessed on 12 May 2009).
- Frangi, A.; Niessen, W.J.; Vincken, K.L.; Viergever, M.A. Multiscale vessel enhancement filtering. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention, Cambridge, MA, USA, 11–13 October 1998. [Google Scholar]
- Mirzaalian, H.; Lee, T.K.; Hamarneh, G. Learning Features for Streak Detection in Dermoscopic Color Images using Localized Radial Flux of Principal Intensity Curvature. In Proceedings of the IEEE Workshop on Mathematical Methods in Biomedical Image Analysis 2012, Breckenridge, CO, USA, 9–10 January 2012. [Google Scholar]
- Argenziano, G.; Soyer, H.P. Dermoscopy of pigmented skin lesions—A valuable tool for early diagnosis of melanoma. Lancet Oncol. 2001, 2, 443–449. [Google Scholar] [CrossRef]
- Mayer, J. Systematic review of the diagnostic accuracy of dermatoscopy in detecting malignant melanoma. Med J. Aust. 1997, 167, 206–210. [Google Scholar] [CrossRef]
- Burroni, M.; Corona, R.; Dell’Eva, G. Melanoma computer-aided diagnosis: Reliability and feasibility study. Clin. Cancer Res. 2004, 10, 1881–1886. [Google Scholar] [CrossRef] [Green Version]
- Rubegni, P.; Cevenini, G.; Burroni, M. Automated diagnosis of pigmented skin lesions. Int. J. Cancer 2002, 101, 576–580. [Google Scholar] [CrossRef] [Green Version]
- Umbaugh, S.E.; Moss, R.H.; Stoecker, W.V.; Hance, G.A. Automatic color segmentation algorithms with application to skin tumor feature identification. IEEE Eng. Med. Biol. Mag. 1993, 12, 75–82. [Google Scholar] [CrossRef]
- Schmid, P. Segmentation of digitized dermatoscopic images by two-dimensional color clustering. IEEE Trans. Med. Imaging 1999, 18, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Schmid-Saugeona, P.; Guillodb, J.; Thirana, J.P. Towards a computer-aided diagnosis system for pigmented skin lesions. Comput. Med. Imaging Graph. 2003, 27, 65–78. [Google Scholar] [CrossRef] [Green Version]
- Ganster, H.; Pinz, A.; Röhrer, R. Automated melanoma recognition. IEEE Trans. Med. Imaging 2001, 20, 233–239. [Google Scholar] [CrossRef]
- Grana, C.; Pellacani, G.; Cucchiara, R.; Seidenari, S. A new algorithm for border description of polarized light surface microscopic images of pigmented skin lesions. IEEE Trans. Med. Imaging 2003, 22, 959–964. [Google Scholar] [CrossRef] [PubMed]
- Rajpara, S.M.; Botello, A.P.; Townend, J.; Ormerod, A.D. Systematic review of dermoscopy and digital dermoscopy/artificial intelligence for the diagnosis of melanoma. Br. J. Dermatol. 2009, 161, 591–604. [Google Scholar] [CrossRef] [PubMed]
- Korotkov, K.; Garcia, R. Computerized Analysis of Pigmented Skin Lesions: A Review. Artif. Intell. Med. 2012, 56, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Celebi, M.E.; Stoecker, W.V.; Moss, R.H. Advances in Skin Cancer Image Analysis. Comput. Med. Imaging Graph. 2011, 35, 83–84. [Google Scholar] [CrossRef] [PubMed]
- Argenziano, G.; Fabbrocini, G.; Carli, P. Epiluminescence microscopy for the diagnosis of doubtful melanocytic skin lesions. Comparison of the ABCD rule of dermatoscopy and a new 7-Point Checklist based on pattern analysis. Arch. Dermatol. 1998, 134, 1563–1570. [Google Scholar] [CrossRef] [Green Version]
- Kawahara, J.; Daneshvar, S.; Argenziano, G.; Hamarneh, G. Seven-point checklist and skin lesion classification using multitask multimodal neural nets. IEEE J. Biomed. Health Inform. 2019, 23, 538–546. [Google Scholar] [CrossRef]
- Alzahrani, S.; Al-Nuaimy, W.; Al-Bander, B. Seven-point checklist with convolutional neural networks for melanoma diagnosis. In Proceedings of the 2019 8th European Workshop on Visual Information Processing (EUVIP), Roma, Italy, 28–31 October 2019. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ELM Criterion | Atypical Pigment Network | Blue-Whitish Veil | Atypical Vascular Pattern |
|---|---|---|---|
| Score | 2 | ||
| Definition | Prominent (hyperpigmented and broad) and irregular network | Irregular, confluent, gray-blue to whitish-blue pigmentation not associated with red-blue lacunes or maple leaf pigmentation | Linear, dotted, or globular red structures irregularly distributed outside areas of regression |
| Histological correlates | Hyperpigmented or broadened ridges with irregular shape or distribution | Pigmented melanophages or melanocytes of mid-reticular dermis location | Neovascularization or vascularized nets of amelanotic cells |
| Main features | Texture | Color | Structures/color |
| Feature extraction | Structural analysis | Principal component analysis 2D thresholding | SRM structural analysis |
| Feature classification | Logistic model tree | Logistic model tree | Statistical analysis |
| ELM Criterion | Irregular Streaks | Regression Structures | Irregular Pigmentation | Irregular Dots/Globules |
|---|---|---|---|---|
| Score | 1 | |||
| Definition | Radially and asymmetrically arranged linear or extensions at the edge of the lesion | White and gray-blue areas, peppering, multiple blue-gray dots associated | Brown, gray, and black areas of diffuse pigmentation with irregular shape or disruption and abrupt end | Black, brown, or blue round structures irregularly distributed within the lesion |
| Histological correlates | Confluent radial junctional nests of melanocytes | Areas of loss of pigmentation and fibroplasias, with scattered melanophages | Hyperpigmentation throughout all levels of epidermis or upper dermis | Aggregates of pigment of stratum corneum, junctional, or dermis location |
| Main features | Structures | Color | Color | Structures |
| Feature extraction | Structural analysis SRM | SRM | SRM | SRM structural analysis |
| Feature classification | Statistical analysis | Logistic model tree | Logistic model tree | Statistical analysis |
| Weighted TOTAL Score | Lesion Classification | Clinical Decision |
|---|---|---|
| Benign nevus | No excision | |
| Suspicious atypical nevus | 6-month follow-up | |
| Atypical nevus | Excision | |
| Melanoma | Excision |
| EXAMINER Dermoscopic Criterion | ED | NED | MS | Biopsy/ Reference | ||||
|---|---|---|---|---|---|---|---|---|
| S.C. | B.B. | M.A. | C.C. | A.M. | F.C. | MS | ||
| Atypical pigment network | 86 | 71 | 85 | 93 | 89 | 106 | 92 | 72 |
| Blue-whitish veil | 54 | 32 | 47 | 105 | 74 | 35 | 58 | 53 |
| Atypical vascular pattern | 15 | 28 | 12 | 19 | 37 | 18 | 28 | 18 |
| Irregular streaks | 24 | 11 | 16 | 18 | 19 | 23 | 32 | 23 |
| Regression structures | 74 | 15 | 76 | 66 | 35 | 91 | 87 | 68 |
| Irregular pigmentation | 74 | 53 | 56 | 122 | 114 | 103 | 46 | 65 |
| Irregular dots/globules | 60 | 51 | 55 | 70 | 71 | 63 | 80 | 53 |
| EXAMINER Performance Index | ED | NED | MS | Biopsy/ Reference | ||||
|---|---|---|---|---|---|---|---|---|
| S.C. | B.B. | M.A. | C.C. | A.M. | F.C. | MS | ||
| Correct (/classified) melanoma (MN) | 59/69 | 55/68 | 54/67 | 46/67 | 42/61 | 45/66 | 55/109 | 64 |
| Correct (/classified) atypical nevus (AN) | 64/67 | 65/70 | 63/68 | 53/63 | 55/64 | 53/61 | 46/52 | 73 |
| Correct (/classified) suspicious nevus (SN) | 25/26 | 21/25 | 23/27 | 25/30 | 26/35 | 25/33 | 22/24 | 26 |
| Correct (/classified) benign nevus (BN) | 107/108 | 107/107 | 107/108 | 107/110 | 106/110 | 107/110 | 84/85 | 107 |
| EXAMINER Performance Index | ED | NED | MS | Biopsy/ Reference | ||||
|---|---|---|---|---|---|---|---|---|
| S.C. | B.B. | M.A. | C.C. | A.M. | F.C. | MS | ||
| Sensitivity % [MNcorr_classif/MNReference] | 92 | 86 | 84 | 72 | 66 | 70 | 86 | - |
| Specificity % [(AN + SN + BN)corr_classif/(data − MNReference)] | 96 | 94 | 94 | 90 | 91 | 90 | 74 | - |
| Diagnostic Accuracy % | 95 | 92 | 92 | 86 | 85 | 85 | 77 | - |
| Clinical Accuracy % | 94 | 92 | 91 | 86 | 85 | 85 | 77 | - |
| EXAMINER Performance Index | NED | NED + MS | MS | Biopsy/ Reference | ||||
|---|---|---|---|---|---|---|---|---|
| C.C. | A.M. | F.C. | C.C. | A.M. | F.C. | MS | ||
| Correct (/classified) melanoma (MN) | 46/67 | 42/61 | 45/66 | 55/77 | 53/75 | 54/76 | 55/109 | 64 |
| Correct (/classified) atypical nevus (AN) | 53/63 | 55/64 | 53/61 | 52/58 | 55/58 | 53/57 | 46/52 | 73 |
| Correct (/classified) suspicious nevus (SN) | 25/30 | 26/35 | 25/33 | 24/27 | 26/31 | 24/30 | 22/24 | 26 |
| Correct (/classified) benign nevus (BN) | 107/110 | 106/110 | 107/110 | 107/108 | 106/106 | 106/107 | 84/85 | 107 |
| EXAMINER Performance Index | NED | NED + MS | MS | Biopsy/ Reference | ||||
|---|---|---|---|---|---|---|---|---|
| C.C. | A.M. | F.C. | C.C. | A.M. | F.C. | MS | ||
| Sensitivity % [MNcorr_classif/MNReference ] | 72 | 66 | 70 | 86 | 83 | 84 | 86 | - |
| Specificity % [(AN + SN + BN)corr_classif/(data − MNReference)] | 90 | 91 | 90 | 89 | 91 | 89 | 74 | - |
| Diagnostic Accuracy % | 86 | 85 | 85 | 88 | 89 | 88 | 77 | - |
| Clinical Accuracy % | 86 | 85 | 85 | 88 | 89 | 88 | 77 | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cacciapuoti, S.; Di Leo, G.; Ferro, M.; Liguori, C.; Masarà, A.; Scalvenzi, M.; Sommella, P.; Fabbrocini, G. A Measurement Software for Professional Training in Early Detection of Melanoma. Appl. Sci. 2020, 10, 4351. https://doi.org/10.3390/app10124351
Cacciapuoti S, Di Leo G, Ferro M, Liguori C, Masarà A, Scalvenzi M, Sommella P, Fabbrocini G. A Measurement Software for Professional Training in Early Detection of Melanoma. Applied Sciences. 2020; 10(12):4351. https://doi.org/10.3390/app10124351
Chicago/Turabian StyleCacciapuoti, Sara, Giuseppe Di Leo, Matteo Ferro, Consolatina Liguori, Anna Masarà, Massimiliano Scalvenzi, Paolo Sommella, and Gabriella Fabbrocini. 2020. "A Measurement Software for Professional Training in Early Detection of Melanoma" Applied Sciences 10, no. 12: 4351. https://doi.org/10.3390/app10124351