
Virtual Reality Training of Social Skills in Adults with Autism Spectrum Disorder: An Examination of Acceptability, Usability, User Experience, Social Skills, and Executive Functions

 ,
, 
 , ,
, ,
Abstract
:1. Introduction
1.1. Social Skills and Executive Functions in ASD
1.2. Assessment, Training, and Intervention in ASD
1.3. Ecological Validity, Virtual Reality Assessments, and Interventions
1.4. VRESS
1.5. Research Aims
- Usability: the capacity of a system to provide a condition for its users to perform the tasks safely, effectively, and efficiently while enjoying the experience.
- User experience: how a user interacts with and experiences a product, system, or service.
- Acceptability: the quality of being satisfactory and able to be agreed to or approved of being software for a specific purpose.
- (1)
- Evaluate the usability and user experience of an immersive VR training software for social skills (i.e., VRESS) in adults with ASD.
- (2)
- Examine the acceptability of the VR training software of social skills as a social service (i.e., from a service user’s point of view) that may be prescribed and/or offered by clinicians, educators, and social workers to adults with ASD for training and improving their everyday social skills.
- (3)
- Investigate the relationships between cognitive functioning (i.e., aspects of social cognition and EFs), the independence/functionality level of individuals with ASD, performance in VR social scenarios, and acceptability, usability, and user experience ratings.
2. Materials and Methods
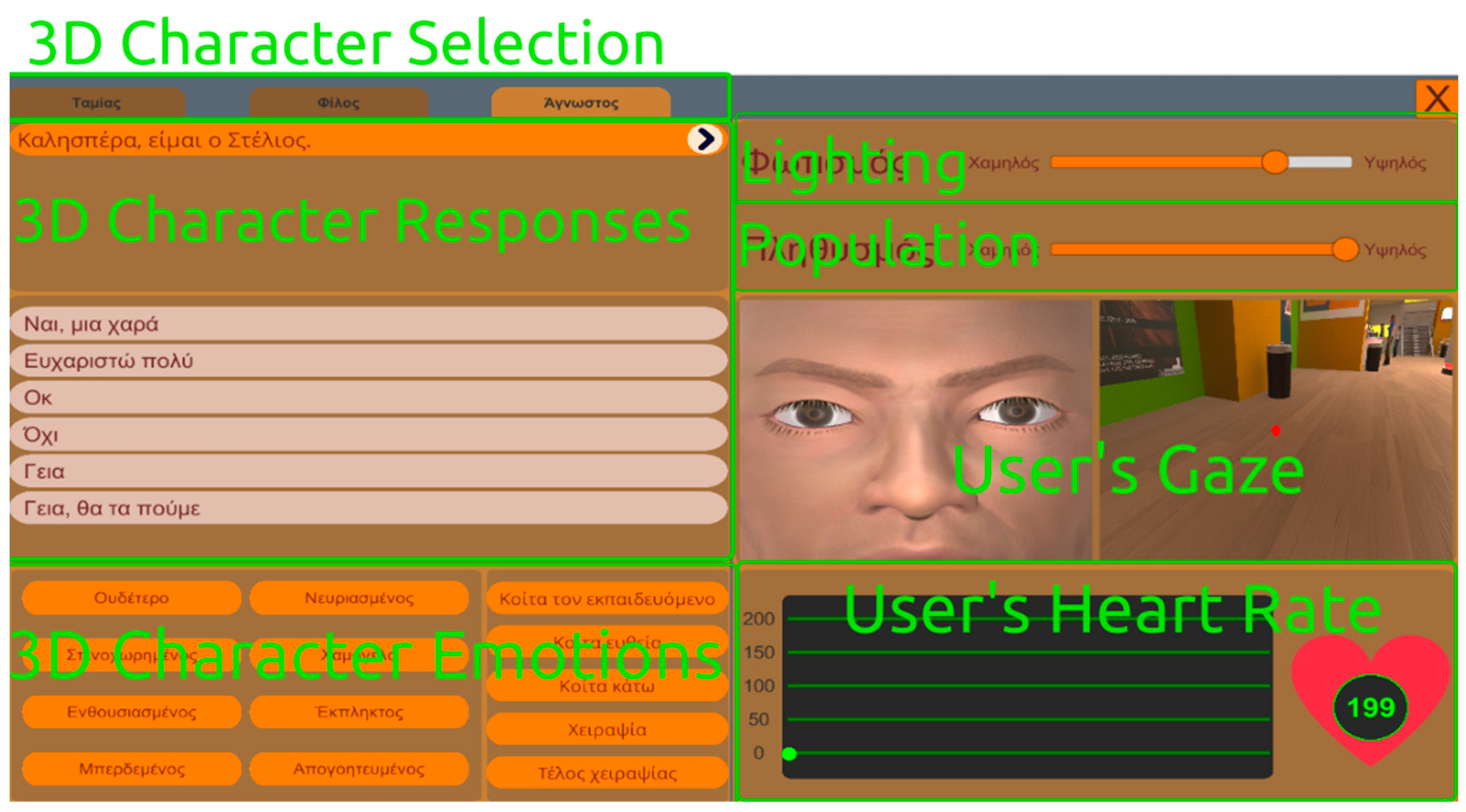
2.1. VRESS Scenarios and Interface
2.1.1. Gym
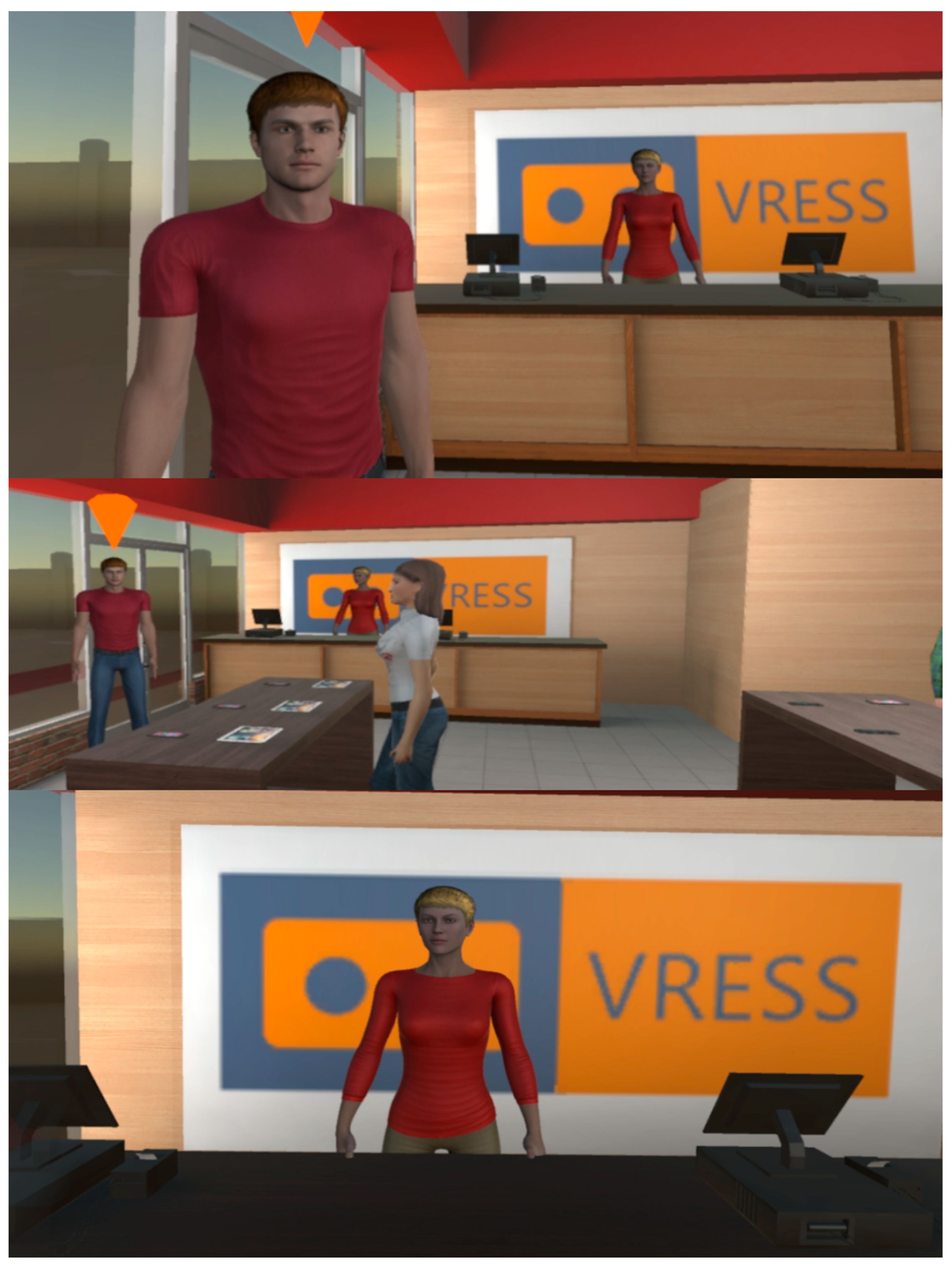
2.1.2. Phone Store
2.1.3. Cinema
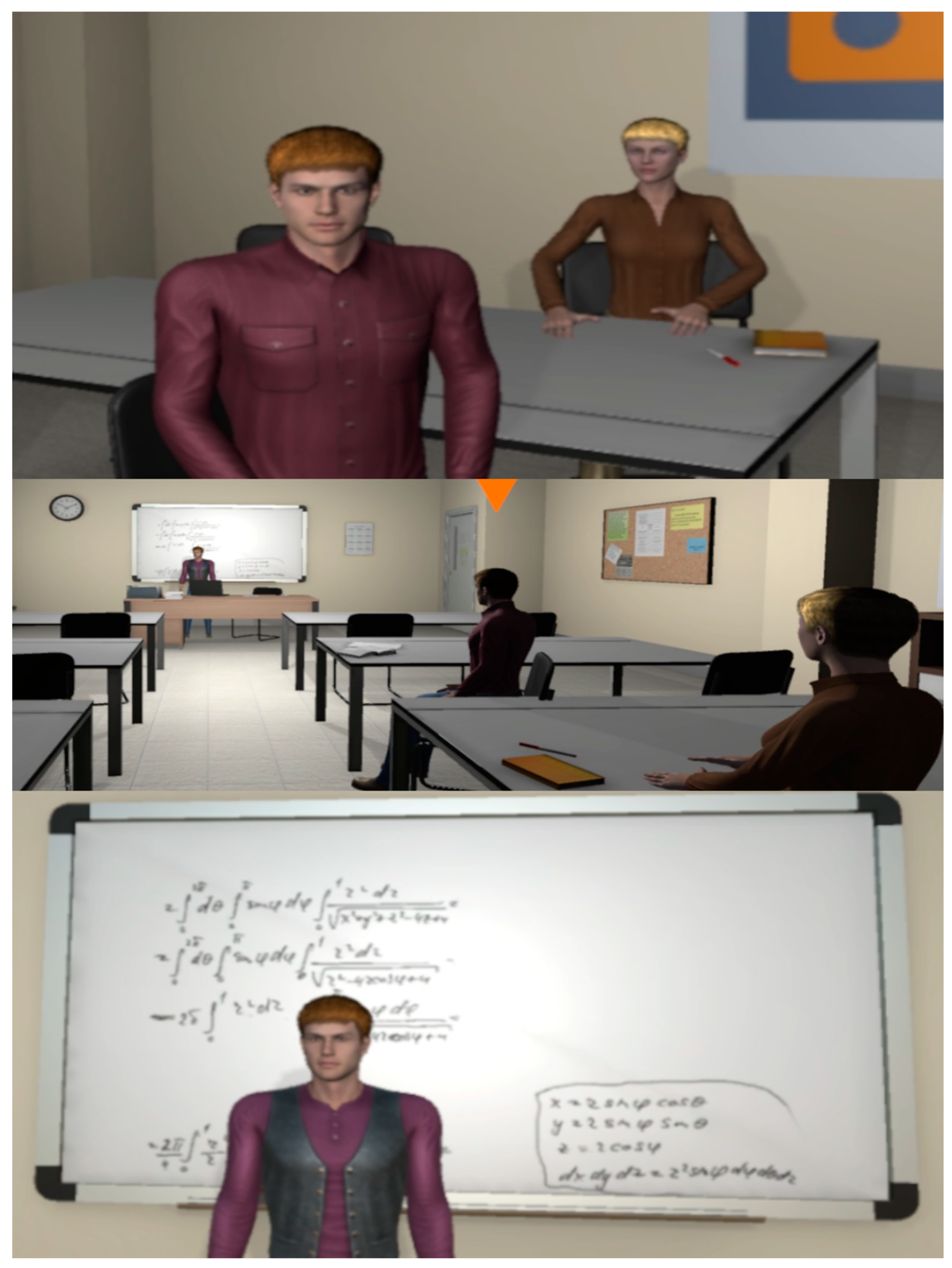
2.1.4. Classroom
2.1.5. Interview
2.2. Neuropsychological Assessment
2.2.1. Reading the Mind in the Eyes Test (Adult Version)—Mental State/Emotion Recognition
2.2.2. Tower of London—Planning
2.2.3. Digit Recall—Verbal Working Memory
2.2.4. Stroop Test—Inhibition
2.3. Questionnaires
2.3.1. Demographics and IT Skills
2.3.2. Service User Technology Acceptability Questionnaire
2.3.3. User Experience Questionnaire
2.3.4. System Usability Scale
2.3.5. Cybersickness in Virtual Reality Questionnaire
2.4. Participants
2.5. Procedures
2.5.1. Neuropsychological Session
2.5.2. VR Sessions
2.5.3. Performance Evaluation in the VR Social Scenarios
2.6. Statistical Analyses
3. Results
3.1. Descriptive Statistics
3.1.1. Demographic Information
3.1.2. Performance on Neuropsychological Tests and in Social Scenarios
3.1.3. Acceptability, User Experience, and Usability Ratings
3.2. Pearson’s and Kendall’s Tau Correlations
3.2.1. Demographics Correlations with Self-Reports and Performance
3.2.2. Self-Reports, Performance Metrics, and ASD Functionality Level
3.3. Linear Regression and Generalised Linear Models
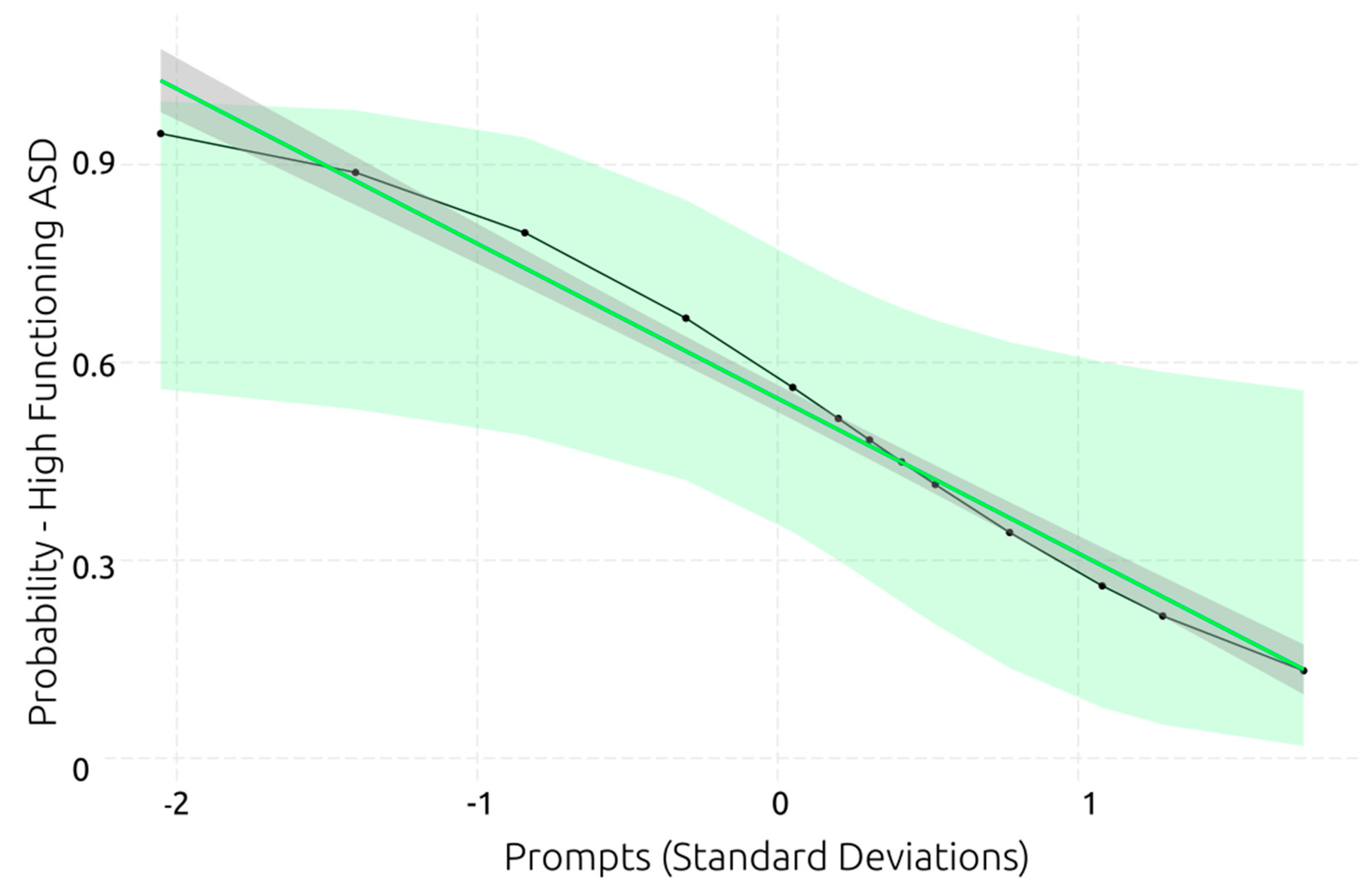
3.3.1. ASD Functionality Level
3.3.2. Performance in VR Social Scenarios
3.3.3. Service User’s Acceptability and User Experience Ratings
3.3.4. System’s Perceived Usability
4. Discussion
4.1. VR Training of Social Skills in Adults with ASD
4.2. Demographics’ Role in Cognition
4.2.1. Executive Functions
4.2.2. Mental State/Emotion Recognition
4.3. Executive Functions and Social Skills
4.4. Predictors of Functionality Level in ASD
4.5. Limitations and Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Zeidan, J.; Fombonne, E.; Scorah, J.; Ibrahim, A.; Durkin, M.S.; Saxena, S.; Yusuf, A.; Shih, A.; Elsabbagh, M. Global prevalence of autism: A systematic review update. Autism Res. 2022, 15, 778–790. [Google Scholar] [CrossRef] [PubMed]
- Loomes, R.; Hull, L.; Mandy, W.P.L. What Is the Male-to-Female Ratio in Autism Spectrum Disorder? A Systematic Review and Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Chaste, P.; Leboyer, M. Autism risk factors: Genes, environment, and gene-environment interactions. Dialogues Clin. Neurosci. 2012, 14, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Elsabbagh, M.; Baird, G.; Veenstra-Vanderweele, J. Autism spectrum disorder. Lancet 2018, 392, 508–520. [Google Scholar] [CrossRef] [PubMed]
- Keller, R.; Ardizzone, F.; Finardi, C.; Colella, R.; Genuario, C.; Lopez, M.; Salerno, L.; Nobile, E.; Cicinelli, G. Real-Life Social-Skills Training and Motor-Skills Training in Adults with Autism Spectrum Disorder: The Con-Tatto Project Walking Down the Francigena Route. Front. Psychiatry 2022, 13, 743. Available online: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.846619 (accessed on 14 March 2023). [CrossRef]
- McVey, A.J.; Dolan, B.K.; Willar, K.S.; Pleiss, S.; Karst, J.S.; Casnar, C.L.; Caiozzo, C.; Vogt, E.M.; Gordon, N.S.; Van Hecke, A.V. A Replication and Extension of the PEERS® for Young Adults Social Skills Intervention: Examining Effects on Social Skills and Social Anxiety in Young Adults with Autism Spectrum Disorder. J. Autism Dev. Disord. 2016, 46, 3739–3754. [Google Scholar] [CrossRef]
- Morrison, K.E.; Pinkham, A.E.; Penn, D.L.; Kelsven, S.; Ludwig, K.; Sasson, N.J. Distinct profiles of social skill in adults with autism spectrum disorder and schizophrenia. Autism Res. 2017, 10, 878–887. [Google Scholar] [CrossRef]
- Ratto, A.B.; Turner-Brown, L.; Rupp, B.M.; Mesibov, G.B.; Penn, D.L. Development of the Contextual Assessment of Social Skills (CASS): A Role Play Measure of Social Skill for Individuals with High-Functioning Autism. J. Autism Dev. Disord. 2011, 41, 1277–1286. [Google Scholar] [CrossRef]
- Shtayermman, O. Peer Victimization in Adolescents and Young Adults Diagnosed with Asperger’s Syndrome: A Link to Depressive Symptomatology, Anxiety Symptomatology and Suicidal Ideation. Issues Compr. Pediatr. Nurs. 2007, 30, 87–107. [Google Scholar] [CrossRef]
- Iarocci, G.; Gardiner, E. Executive Functions and the Developing Social Competence of Children With Autism Spectrum Disorder. In Executive Functions in Children’s Everyday Lives: A Handbook for Professionals in Applied Psychology; Hoskyn, M.J., Iarocci, G., Young, A.R., Eds.; Oxford University Press: New York, NY, USA, 2017; pp. 134–156. [Google Scholar] [CrossRef]
- Haigh, S.M.; Walsh, J.A.; Mazefsky, C.A.; Minshew, N.J.; Eack, S.M. Processing Speed is Impaired in Adults with Autism Spectrum Disorder, and Relates to Social Communication Abilities. J. Autism Dev. Disord. 2018, 48, 2653–2662. [Google Scholar] [CrossRef]
- Demetriou, E.A.; DeMayo, M.M.; Guastella, A.J. Executive Function in Autism Spectrum Disorder: History, Theoretical Models, Empirical Findings, and Potential as an Endophenotype. Front. Psychiatry 2019, 10, 753. Available online: https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00753 (accessed on 14 March 2023). [CrossRef] [PubMed]
- Lezak, M.D. Neuropsychological Assessment, 3rd ed.; Oxford University Press: New York, NY, USA, 1995; pp. 461–481, 1026. [Google Scholar]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex ‘Frontal Lobe’ Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed]
- Demetriou, E.A.; Lampit, A.; Quintana, D.S.; Naismith, S.L.; Song, Y.J.C.; E Pye, J.; Hickie, I.; Guastella, A.J. Autism spectrum disorders: A meta-analysis of executive function. Mol. Psychiatry 2018, 23, 1198–1204. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.L.E.; Lau, Z.; Lui, S.S.Y.; Lok, E.; Tam, V.; Chan, Q.; Cheng, K.M.; Lam, S.M.; Cheung, E.F.C. Meta-analysis of neuropsychological measures of executive functioning in children and adolescents with high-functioning autism spectrum disorder. Autism Res. 2017, 10, 911–939. [Google Scholar] [CrossRef]
- Fong, V.C.; Iarocci, G. The Role of Executive Functioning in Predicting Social Competence in Children with and without Autism Spectrum Disorder. Autism Res. 2020, 13, 1856–1866. [Google Scholar] [CrossRef]
- Riggs, N.R.; Jahromi, L.B.; Razza, R.P.; Dillworth-Bart, J.E.; Mueller, U. Executive function and the promotion of social–emotional competence. J. Appl. Dev. Psychol. 2006, 27, 300–309. [Google Scholar] [CrossRef]
- Nilsen, E.S.; Fecica, A.M. A model of communicative perspective-taking for typical and atypical populations of children. Dev. Rev. 2011, 31, 55–78. [Google Scholar] [CrossRef]
- Freeman, L.M.; Locke, J.; Rotheram-Fuller, E.; Mandell, D. Brief Report: Examining Executive and Social Functioning in Elementary-Aged Children with Autism. J. Autism Dev. Disord. 2017, 47, 1890–1895. [Google Scholar] [CrossRef] [PubMed]
- Kenworthy, L.; Black, D.O.; Harrison, B.; della Rosa, A.; Wallace, G.L. Are Executive Control Functions Related to Autism Symptoms in High-Functioning Children? Child Neuropsychol. 2009, 15, 425–440. [Google Scholar] [CrossRef]
- Pugliese, C.E.; Anthony, L.; Strang, J.F.; Dudley, K.; Wallace, G.L.; Kenworthy, L. Increasing Adaptive Behavior Skill Deficits From Childhood to Adolescence in Autism Spectrum Disorder: Role of Executive Function. J. Autism Dev. Disord. 2015, 45, 1579–1587. [Google Scholar] [CrossRef]
- Gilotty, L.; Kenworthy, L.; Sirian, L.; Black, D.O.; Wagner, A.E. Adaptive Skills and Executive Function in Autism Spectrum Disorders. Child Neuropsychol. 2002, 8, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Leslie, A.M.; Frith, U. Does the autistic child have a ‘theory of mind’? Cognition 1985, 21, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Alkire, D.; McNaughton, K.A.; Yarger, H.A.; Shariq, D.; Redcay, E. Theory of mind in naturalistic conversations between autistic and typically developing children and adolescents. Autism 2022, 27, 13623613221103700. [Google Scholar] [CrossRef] [PubMed]
- Kouklari, E.-C.; Thompson, T.; Monks, C.P.; Tsermentseli, S. Hot and Cool Executive Function and its Relation to Theory of Mind in Children with and without Autism Spectrum Disorder. J. Cogn. Dev. 2017, 18, 399–418. [Google Scholar] [CrossRef]
- Kouklari, E.-C.; Tsermentseli, S.; Monks, C.P. Developmental trends of hot and cool executive function in school-aged children with and without autism spectrum disorder: Links with theory of mind. Dev. Psychopathol. 2019, 31, 541–556. [Google Scholar] [CrossRef]
- Gentil-Gutiérrez, A.; Santamaría-Peláez, M.; Mínguez-Mínguez, L.A.; Fernández-Solana, J.; González-Bernal, J.J.; González-Santos, J.; Obregón-Cuesta, A.I. Executive Functions in Children and Adolescents with Autism Spectrum Disorder in Family and School Environment. Int. J. Environ. Res. Public Health 2022, 19, 7834. [Google Scholar] [CrossRef]
- Hughes, C.; Dunn, J.; White, A. Trick or Treat?: Uneven Understanding of Mind and Emotion and Executive Dysfunction in ‘Hard-to-manage’ Preschoolers. J. Child Psychol. Psychiatry Allied Discip. 1998, 39, 981–994. [Google Scholar] [CrossRef]
- Tager-Flusberg, H. Evaluating the Theory-of-Mind Hypothesis of Autism. Curr. Dir. Psychol. Sci. 2007, 16, 311–315. [Google Scholar] [CrossRef]
- Mazefsky, C.A.; Herrington, J.; Siegel, M.; Scarpa, A.; Maddox, B.B.; Scahill, L.; White, S.W. The Role of Emotion Regulation in Autism Spectrum Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 679–688. [Google Scholar] [CrossRef]
- Constantino, J.N. Social Responsiveness Scale. In Encyclopedia of Autism Spectrum Disorders; Volkmar, F.R., Ed.; Springer: New York, NY, USA, 2013; pp. 2919–2929. [Google Scholar] [CrossRef]
- Bruni, T.P. Test Review: Social Responsiveness Scale–Second Edition (SRS-2). J. Psychoeduc. Assess. 2014, 32, 365–369. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Wheelwright, S.; Hill, J.; Raste, Y.; Plumb, I. The ‘Reading the Mind in the Eyes’ Test Revised Version: A Study with Normal Adults, and Adults with Asperger Syndrome or High-functioning Autism. J. Child Psychol. Psychiatry 2001, 42, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, K.; Paliokosta, E.; Houliaras, G.; Vgenopoulou, S.; Giouroukou, E.; Pehlivanidis, A.; Tomaras, V.; Tsiantis, I. Using the Autism Diagnostic Interview-Revised and the Autism Diagnostic Observation Schedule-Generic for the Diagnosis of Autism Spectrum Disorders in a Greek Sample with a Wide Range of Intellectual Abilities. J. Autism Dev. Disord. 2009, 39, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H., Jr.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule—Generic: A Standard Measure of Social and Communication Deficits Associated with the Spectrum of Autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef] [PubMed]
- Dandil, Y.; Smith, K.; Kinnaird, E.; Toloza, C.; Tchanturia, K. Cognitive Remediation Interventions in Autism Spectrum Condition: A Systematic Review. Front. Psychiatry 2020, 11, 722. Available online: https://www.frontiersin.org/articles/10.3389/fpsyt.2020.00722 (accessed on 14 March 2023). [CrossRef] [PubMed]
- Eack, S.M.; Greenwald, D.P.; Hogarty, S.S.; Bahorik, A.L.; Litschge, M.Y.; Mazefsky, C.A.; Minshew, N.J. Cognitive Enhancement Therapy for Adults with Autism Spectrum Disorder: Results of an 18-month Feasibility Study. J. Autism Dev. Disord. 2013, 43, 2866–2877. [Google Scholar] [CrossRef] [PubMed]
- Miyajima, M.; Omiya, H.; Yamashita, K.; Miyata, T.; Yambe, K.; Matsui, M.; Denda, K. The effects of cognitive remediation therapy using the frontal/executive program for autism spectrum disorder. Int. J. Psychiatry Med. 2016, 51, 223–235. [Google Scholar] [CrossRef]
- Pasqualotto, A.; Mazzoni, N.; Bentenuto, A.; Mulè, A.; Benso, F.; Venuti, P. Effects of Cognitive Training Programs on Executive Function in Children and Adolescents with Autism Spectrum Disorder: A Systematic Review. Brain Sci. 2021, 11, 1280. [Google Scholar] [CrossRef]
- Au, J.; Sheehan, E.; Tsai, N.; Duncan, G.J.; Buschkuehl, M.; Jaeggi, S.M. Improving fluid intelligence with training on working memory: A meta-analysis. Psychon. Bull. Rev. 2015, 22, 366–377. [Google Scholar] [CrossRef]
- Karbach, J.; Verhaeghen, P. Making Working Memory Work: A Meta-Analysis of Executive-Control and Working Memory Training in Older Adults. Psychol. Sci. 2014, 25, 2027–2037. [Google Scholar] [CrossRef]
- Melby-Lervåg, M.; Redick, T.S.; Hulme, C. Working Memory Training Does Not Improve Performance on Measures of Intelligence or Other Measures of ‘Far Transfer’: Evidence from a Meta-Analytic Review. Perspect. Psychol. Sci. 2016, 11, 512–534. [Google Scholar] [CrossRef]
- Laugeson, E.A.; Ellingsen, R. Social Skills Training for Adolescents and Adults with Autism Spectrum Disorder. In Adolescents and Adults with Autism Spectrum Disorders; Volkmar, F.R., Reichow, B., McPartland, J.C., Eds.; Springer: New York, NY, USA, 2014; pp. 61–85. [Google Scholar] [CrossRef]
- Gantman, A.; Kapp, S.K.; Orenski, K.; Laugeson, E.A. Social Skills Training for Young Adults with High-Functioning Autism Spectrum Disorders: A Randomized Controlled Pilot Study. J. Autism Dev. Disord. 2012, 42, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Bishop-Fitzpatrick, L.; Minshew, N.J.; Eack, S.M. A Systematic Review of Psychosocial Interventions for Adults with Autism Spectrum Disorders. J. Autism Dev. Disord. 2013, 43, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Bottema-Beutel, K.; Park, H.; Kim, S.Y. Commentary on Social Skills Training Curricula for Individuals with ASD: Social Interaction, Authenticity, and Stigma. J. Autism Dev. Disord. 2018, 48, 953–964. [Google Scholar] [CrossRef] [PubMed]
- Gates, J.A.; Kang, E.; Lerner, M.D. Efficacy of group social skills interventions for youth with autism spectrum disorder: A systematic review and meta-analysis. Clin. Psychol. Rev. 2017, 52, 164–181. [Google Scholar] [CrossRef]
- Bolis, D.; Balsters, J.; Wenderoth, N.; Becchio, C.; Schilbach, L. Beyond Autism: Introducing the Dialectical Misattunement Hypothesis and a Bayesian Account of Intersubjectivity. Psychopathology 2017, 50, 355–372. [Google Scholar] [CrossRef] [PubMed]
- Beaumont, R.; Sofronoff, K. A multi-component social skills intervention for children with Asperger syndrome: The Junior Detective Training Program. J. Child Psychol. Psychiatry 2008, 49, 743–753. [Google Scholar] [CrossRef]
- Chaytor, N.; Schmitter-Edgecombe, M. The Ecological Validity of Neuropsychological Tests: A Review of the Literature on Everyday Cognitive Skills. Neuropsychol. Rev. 2003, 13, 181–197. [Google Scholar] [CrossRef]
- Kourtesis, P.; Collina, S.; Doumas, L.A.A.; MacPherson, S.E. Validation of the Virtual Reality Everyday Assessment Lab (VR-EAL): An Immersive Virtual Reality Neuropsychological Battery with Enhanced Ecological Validity. J. Int. Neuropsychol. Soc. 2021, 27, 181–196. [Google Scholar] [CrossRef]
- Kourtesis, P.; Collina, S.; Doumas, L.A.A.; MacPherson, S.E. An ecologically valid examination of event-based and time-based prospective memory using immersive virtual reality: The effects of delay and task type on everyday prospective memory. Memory 2021, 29, 486–506. [Google Scholar] [CrossRef]
- Kourtesis, P.; MacPherson, S.E. An ecologically valid examination of event-based and time-based prospective memory using immersive virtual reality: The influence of attention, memory, and executive function processes on real-world prospective memory. Neuropsychol. Rehabil. 2021, 33, 1–26. [Google Scholar] [CrossRef]
- Liao, Y.-Y.; Chen, I.-H.; Lin, Y.-J.; Chen, Y.; Hsu, W.-C. Effects of Virtual Reality-Based Physical and Cognitive Training on Executive Function and Dual-Task Gait Performance in Older Adults with Mild Cognitive Impairment: A Randomized Control Trial. Front. Aging Neurosci. 2019, 11, 162. Available online: https://www.frontiersin.org/articles/10.3389/fnagi.2019.00162 (accessed on 14 March 2023). [CrossRef] [PubMed]
- Arlati, S.; Colombo, V.; Spoladore, D.; Greci, L.; Pedroli, E.; Serino, S.; Cipresso, P.; Goulene, K.; Stramba-Badiale, M.; Riva, G.; et al. A Social Virtual Reality-Based Application for the Physical and Cognitive Training of the Elderly at Home. Sensors 2019, 19, 261. [Google Scholar] [CrossRef] [PubMed]
- Zając-Lamparska, L.; Wiłkość-Dębczyńska, M.; Wojciechowski, A.; Podhorecka, M.; Polak-Szabela, A.; Warchoł, Ł.; Kędziora-Kornatowska, K.; Araszkiewicz, A.; Izdebski, P. Effects of virtual reality-based cognitive training in older adults living without and with mild dementia: A pretest–posttest design pilot study. BMC Res. Notes 2019, 12, 776. [Google Scholar] [CrossRef] [PubMed]
- Bradley, R.; Newbutt, N. Autism and virtual reality head-mounted displays: A state of the art systematic review. J. Enabling Technol. 2018, 12, 101–113. [Google Scholar] [CrossRef]
- Mesa-Gresa, P.; Gil-Gómez, H.; Lozano-Quilis, J.-A.; Gil-Gómez, J.-A. Effectiveness of Virtual Reality for Children and Adolescents with Autism Spectrum Disorder: An Evidence-Based Systematic Review. Sensors 2018, 18, 2486. [Google Scholar] [CrossRef]
- Rosenfield, N.S.; Lamkin, K.; Re, J.; Day, K.; Boyd, L.; Linstead, E. A Virtual Reality System for Practicing Conversation Skills for Children with Autism. Multimodal Technol. Interact. 2019, 3, 28. [Google Scholar] [CrossRef]
- Glaser, N.; Schmidt, M. Systematic Literature Review of Virtual Reality Intervention Design Patterns for Individuals with Autism Spectrum Disorders. Int. J. Hum.–Comput. Interact. 2022, 38, 753–788. [Google Scholar] [CrossRef]
- Kourtesis, P.; Collina, S.; Doumas, L.A.A.; MacPherson, S.E. Technological Competence Is a Pre-condition for Effective Implementation of Virtual Reality Head Mounted Displays in Human Neuroscience: A Technological Review and Meta-Analysis. Front. Hum. Neurosci. 2019, 13, 342. [Google Scholar] [CrossRef]
- Nolin, P.; Stipanicic, A.; Henry, M.; Lachapelle, Y.; Lussier-Desrochers, D.; Rizzo, A.; Allain, P. ClinicaVR: Classroom-CPT: A virtual reality tool for assessing attention and inhibition in children and adolescents. Comput. Hum. Behav. 2016, 59, 327–333. [Google Scholar] [CrossRef]
- Newbutt, N.; Sung, C.; Kuo, H.-J.; Leahy, M.J.; Lin, C.-C.; Tong, B. Brief Report: A Pilot Study of the Use of a Virtual Reality Headset in Autism Populations. J. Autism Dev. Disord. 2016, 46, 3166–3176. [Google Scholar] [CrossRef]
- Ghanouni, P.; Jarus, T.; Zwicker, J.G.; Lucyshyn, J.; Mow, K.; Ledingham, A. Social Stories for Children with Autism Spectrum Disorder: Validating the Content of a Virtual Reality Program. J. Autism Dev. Disord. 2019, 49, 660–668. [Google Scholar] [CrossRef] [PubMed]
- Herrero, J.F.; Lorenzo, G. An immersive virtual reality educational intervention on people with autism spectrum disorders (ASD) for the development of communication skills and problem solving. Educ. Inf. Technol. 2020, 25, 1689–1722. [Google Scholar] [CrossRef]
- Ip, H.H.S.; Wong, S.W.; Chan, D.F.; Byrne, J.; Li, C.; Yuan, V.S.; Lau, K.S.; Wong, J.Y. Enhance emotional and social adaptation skills for children with autism spectrum disorder: A virtual reality enabled approach. Comput. Educ. 2018, 117, 1–15. [Google Scholar] [CrossRef]
- Ke, F.; Moon, J.; Sokolikj, Z. Virtual Reality–Based Social Skills Training for Children With Autism Spectrum Disorder. J. Spec. Educ. Technol. 2022, 37, 49–62. [Google Scholar] [CrossRef]
- Yuan, S.N.V.; Ip, H.H.S. Using virtual reality to train emotional and social skills in children with autism spectrum disorder. Lond. J. Prim. Care 2018, 10, 110–112. [Google Scholar] [CrossRef]
- Kourtesis, P.; Korre, D.; Collina, S.; Doumas, L.A.A.; MacPherson, S.E. Guidelines for the Development of Immersive Virtual Reality Software for Cognitive Neuroscience and Neuropsychology: The Development of Virtual Reality Everyday Assessment Lab (VR-EAL), a Neuropsychological Test Battery in Immersive Virtual Reality. Front. Comput. Sci. 2020, 1, 12. [Google Scholar] [CrossRef]
- Kourtesis, P.; MacPherson, S.E. How immersive virtual reality methods may meet the criteria of the National Academy of Neuropsychology and American Academy of Clinical Neuropsychology: A software review of the Virtual Reality Everyday Assessment Lab (VR-EAL). Comput. Hum. Behav. Rep. 2021, 4, 100151. [Google Scholar] [CrossRef]
- Gray, C.A.; Garand, J.D. Social Stories: Improving Responses of Students with Autism with Accurate Social Information. Focus Autistic Behav. 1993, 8, 1–10. [Google Scholar] [CrossRef]
- Samuels, R.; Stansfield, J. The effectiveness of social storiesTM to develop social interactions with adults with characteristics of autism spectrum disorder. Br. J. Learn. Disabil. 2012, 40, 272–285. [Google Scholar] [CrossRef]
- Bakroon, A.; Lakshminarayanan, V. Visual function in autism spectrum disorders: A critical review. Clin. Exp. Optom. 2016, 99, 297–308. [Google Scholar] [CrossRef]
- Joshi, G.; Wozniak, J.; Petty, C.; Martelon, M.K.; Fried, R.; Bolfek, A.; Kotte, A.; Stevens, J.; Furtak, S.L.; Bourgeois, M.; et al. Psychiatric Comorbidity and Functioning in a Clinically Referred Population of Adults with Autism Spectrum Disorders: A Comparative Study. J. Autism Dev. Disord. 2013, 43, 1314–1325. [Google Scholar] [CrossRef]
- Rösler, L.; Göhring, S.; Strunz, M.; Gamer, M. Social anxiety is associated with heart rate but not gaze behavior in a real social interaction. J. Behav. Ther. Exp. Psychiatry 2021, 70, 101600. [Google Scholar] [CrossRef] [PubMed]
- Senju, A.; Johnson, M.H. Atypical eye contact in autism: Models, mechanisms and development. Neurosci. Biobehav. Rev. 2009, 33, 1204–1214. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Abascal, E.G.; Cabello, R.; Fernández-Berrocal, P.; Baron-Cohen, S. Test-retest reliability of the ‘Reading the Mind in the Eyes’ test: A one-year follow-up study. Mol. Autism 2013, 4, 33. [Google Scholar] [CrossRef] [PubMed]
- Vellante, M.; Baron-Cohen, S.; Melis, M.; Marrone, M.; Petretto, D.R.; Masala, C.; Preti, A. The ‘Reading the Mind in the Eyes’ test: Systematic review of psychometric properties and a validation study in Italy. Cogn. Neuropsychiatry 2013, 18, 326–354. [Google Scholar] [CrossRef]
- Shallice, T.; Broadbent, D.E.; Weiskrantz, L. Specific impairments of planning. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1997, 298, 199–209. [Google Scholar] [CrossRef]
- Chang, Y.-K.; Tsai, C.-L.; Hung, T.-M.; So, E.C.; Chen, F.-T.; Etnier, J.L. Effects of Acute Exercise on Executive Function: A Study with a Tower of London Task. J. Sport Exerc. Psychol. 2011, 33, 847–865. [Google Scholar] [CrossRef]
- Köstering, L.; Nitschke, K.; Schumacher, F.K.; Weiller, C.; Kaller, C.P. Test–retest reliability of the Tower of London Planning Task (TOL-F). Psychol. Assess. 2015, 27, 925–931. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Adult Intelligence Scale-Third Edition Manual; The Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- Siegel, D.J.; Minshew, N.J.; Goldstein, G. Wechsler IQ profiles in diagnosis of high-functioning autism. J. Autism Dev. Disord. 1996, 26, 389–406. [Google Scholar] [CrossRef]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643. [Google Scholar] [CrossRef]
- Strauss, G.P.; Allen, D.N.; Jorgensen, M.L.; Cramer, S.L. Test-Retest Reliability of Standard and Emotional Stroop Tasks: An Investigation of Color-Word and Picture-Word Versions. Assessment 2005, 12, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.P.; Du’Mont, S. Measuring the effect of gaming experience on virtual environment navigation tasks. In Proceedings of the 2009 IEEE Symposium on 3D User Interfaces, Lafayette, LA, USA, 14–15 March 2009; IEEE: Washington, DC, USA, 2009; pp. 3–10. [Google Scholar] [CrossRef]
- Hirani, S.P.; Rixon, L.; Beynon, M.; Cartwright, M.; Cleanthous, S.; Selva, A.; Sanders, C.; Newman, S.P. Quantifying beliefs regarding telehealth: Development of the Whole Systems Demonstrator Service User Technology Acceptability Questionnaire. J. Telemed. Telecare 2017, 23, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Schrepp, M.; Hinderks, A.; Thomaschewski, J. Design and evaluation of a short version of the user experience questionnaire (UEQ-S). Int. J. Interact. Multimed. Artif. Intell. 2017, 4, 103–108. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A Retrospective. J. Usability Stud. 2013, 8, 29–40. [Google Scholar]
- Bangor, A.; Kortum, P.; Miller, J. Determining What Individual SUS Scores Mean: Adding an Adjective Rating Scale. J. Usability Stud. 2009, 4, 114–123. [Google Scholar]
- Kourtesis, P.; Collina, S.; Doumas, L.A.A.; MacPherson, S.E. Validation of the Virtual Reality Neuroscience Questionnaire: Maximum Duration of Immersive Virtual Reality Sessions without the Presence of Pertinent Adverse Symptomatology. Front. Hum. Neurosci. 2019, 13, 417. [Google Scholar] [CrossRef]
- Kourtesis, P.; Linnell, J.; Amir, R.; Argelaguet, F.; MacPherson, S.E. Cybersickness in Virtual Reality Questionnaire (CSQ-VR): A Validation and Comparison against SSQ and VRSQ. Virtual Worlds 2023, 2, 16–35. [Google Scholar] [CrossRef]
- Pehlivanidis, A.; Papanikolaou, K.; Mantas, V.; Kalantzi, E.; Korobili, K.; Xenaki, L.-A.; Vassiliou, G.; Papageorgiou, C. Lifetime co-occurring psychiatric disorders in newly diagnosed adults with attention deficit hyperactivity disorder (ADHD) or/and autism spectrum disorder (ASD). BMC Psychiatry 2020, 20, 423. [Google Scholar] [CrossRef]
- Papaioannou, A.; Kalantzi, E.; Papageorgiou, C.C.; Korombili, K.; Bokou, A.; Pehlivanidis, A.; Papageorgiou, C.C.; Papaioannou, G. Differences in Performance of ASD and ADHD Subjects Facing Cognitive Loads in an Innovative Reasoning Experiment. Brain Sci. 2021, 11, 1531. [Google Scholar] [CrossRef]
- Mantas, V.; Pehlivanidis, A.; Papanikolaou, K.; Kotoula, V.; Papageorgiou, C. Strategic decision making and prediction differences in autism. PeerJ 2022, 10, e13328. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 14 March 2023).
- RStudio Team. RStudio: Integrated Development Environment for R; RStudio, PBC: Boston, MA, USA, 2022; Available online: http://www.rstudio.com/ (accessed on 14 March 2023).
- Peterson, R.A.; Cavanaugh, J.E. Ordered quantile normalization: A semiparametric transformation built for the cross-validation era. J. Appl. Stat. 2020, 47, 2312–2327. [Google Scholar] [CrossRef] [PubMed]
- Revelle, W. Psych: Procedures for Psychological, Psychometric, and Personality Research; Northwestern University: Evanston, IL, USA, 2022; Available online: https://CRAN.R-project.org/package=psych (accessed on 14 March 2023).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; Available online: https://ggplot2.tidyverse.org (accessed on 14 March 2023).
- Torbjørnsen, A.; Småstuen, M.C.; Jenum, A.K.; Årsand, E.; Ribu, L. The Service User Technology Acceptability Questionnaire: Psychometric Evaluation of the Norwegian Version. JMIR Hum. Factors 2018, 5, e10255. [Google Scholar] [CrossRef] [PubMed]
- Schrepp, M.; Hinderks, A.; Thomaschewski, J. Construction of a Benchmark for the User Experience Questionnaire (UEQ). Int. J. Interact. Multimed. Artif. Intell. 2017, 4, 40–44. [Google Scholar] [CrossRef]
- Lequerica, A.H.; Kortte, K. Therapeutic Engagement: A Proposed Model of Engagement in Medical Rehabilitation. Am. J. Phys. Med. Rehabil. 2010, 89, 415–422. Available online: https://journals.lww.com/ajpmr/Fulltext/2010/05000/Therapeutic_Engagement__A_Proposed_Model_of.10.aspx (accessed on 14 March 2023). [CrossRef] [PubMed]
- Leaf, J.B.; Cihon, J.H.; Ferguson, J.L.; Milne, C.M.; Leaf, R.; McEachin, J. Comparing Error Correction to Errorless Learning: A Randomized Clinical Trial. Anal. Verbal Behav. 2020, 36, 1–20. [Google Scholar] [CrossRef]
- Alloway, T.P.; Gathercole, S.E.; Adams, A.-M.; Willis, C.; Eaglen, R.; Lamont, E. Working memory and phonological awareness as predictors of progress towards early learning goals at school entry. Br. J. Dev. Psychol. 2005, 23, 417–426. [Google Scholar] [CrossRef]
- Gathercole, S.E.; Pickering, S.J.; Knight, C.; Stegmann, Z. Working memory skills and educational attainment: Evidence from national curriculum assessments at 7 and 14 years of age. Appl. Cogn. Psychol. 2004, 18, 1–16. [Google Scholar] [CrossRef]
- Unsworth, N.; Engle, R.W. On the division of short-term and working memory: An examination of simple and complex span and their relation to higher order abilities. Psychol. Bull. 2007, 133, 1038–1066. [Google Scholar] [CrossRef]
- Carretti, B.; Borella, E.; Cornoldi, C.; De Beni, R. Role of working memory in explaining the performance of individuals with specific reading comprehension difficulties: A meta-analysis. Learn. Individ. Differ. 2009, 19, 246–251. [Google Scholar] [CrossRef]
- Peng, P.; Namkung, J.; Barnes, M.; Sun, C. A meta-analysis of mathematics and working memory: Moderating effects of working memory domain, type of mathematics skill, and sample characteristics. J. Educ. Psychol. 2016, 108, 455–473. [Google Scholar] [CrossRef]
- Peng, P.; Barnes, M.; Wang, C.; Wang, W.; Li, S.; Swanson, H.L.; Dardick, W.; Tao, S. A meta-analysis on the relation between reading and working memory. Psychol. Bull. 2018, 144, 48–76. [Google Scholar] [CrossRef] [PubMed]
- Green, C.S.; Sugarman, M.A.; Medford, K.; Klobusicky, E.; Bavelier, D. The effect of action video game experience on task-switching. Comput. Hum. Behav. 2012, 28, 984–994. [Google Scholar] [CrossRef] [PubMed]
- Green, C.S.; Pouget, A.; Bavelier, D. Improved Probabilistic Inference as a General Learning Mechanism with Action Video Games. Curr. Biol. 2010, 20, 1573–1579. [Google Scholar] [CrossRef]
- Stockdale, L.; Morrison, R.G.; Palumbo, R.; Garbarino, J.; Silton, R.L. Cool, callous and in control: Superior inhibitory control in frequent players of video games with violent content. Soc. Cogn. Affect. Neurosci. 2017, 12, 1869–1880. [Google Scholar] [CrossRef]
- Golan, O.; Baron-Cohen, S. Systemizing empathy: Teaching adults with Asperger syndrome or high-functioning autism to recognize complex emotions using interactive multimedia. Dev. Psychopathol. 2006, 18, 591–617. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, M.V.; Barnes, J.L.; Wheelwright, S.J.; Baron-Cohen, S. Self-Referential Cognition and Empathy in Autism. PLoS ONE 2007, 2, e883. [Google Scholar] [CrossRef] [PubMed]
- Losh, M.; Adolphs, R.; Poe, M.D.; Couture, S.; Penn, D.; Baranek, G.; Piven, J. Neuropsychological Profile of Autism and the Broad Autism Phenotype. Arch. Gen. Psychiatry 2009, 66, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Gollwitzer, P. Implementation Intentions: Strong Effects of Simple Plans. Am. Psychol. 1999, 54, 493–503. [Google Scholar] [CrossRef]
- Morris, R.; Ward, G. The Cognitive Psychology of Planning; Psychology Press: London, UK, 2004. [Google Scholar] [CrossRef]
- Schonfeld, A.M.; Paley, B.; Frankel, F.; O’Connor, M.J. Executive Functioning Predicts Social Skills Following Prenatal Alcohol Exposure. Child Neuropsychol. 2006, 12, 439–452. [Google Scholar] [CrossRef]
- Kiley-Brabeck, K.; Sobin, C. Social Skills and Executive Function Deficits in Children with the 22q11 Deletion Syndrome. Appl. Neuropsychol. 2006, 13, 258–268. [Google Scholar] [CrossRef]
- Sinzig, J.; Morsch, D.; Bruning, N.; Schmidt, M.H.; Lehmkuhl, G. Inhibition, flexibility, working memory and planning in autism spectrum disorders with and without comorbid ADHD-symptoms. Child Adolesc. Psychiatry Ment. Health 2008, 2, 4. [Google Scholar] [CrossRef] [PubMed]
- Dubbelink, L.M.E.O.; Geurts, H.M. Planning Skills in Autism Spectrum Disorder Across the Lifespan: A Meta-analysis and Meta-regression. J. Autism Dev. Disord. 2017, 47, 1148–1165. [Google Scholar] [CrossRef] [PubMed]
- Kercood, S.; Grskovic, J.A.; Banda, D.; Begeske, J. Working memory and autism: A review of literature. Res. Autism Spectr. Disord. 2014, 8, 1316–1332. [Google Scholar] [CrossRef]
- Brüne, M. Theory of mind and the role of IQ in chronic disorganized schizophrenia. Schizophr. Res. 2003, 60, 57–64. [Google Scholar] [CrossRef]
- Baddeley, A.; Della Sala, S.; Papagno, C.; Spinnler, H. Dual-task performance in dysexecutive and nondysexecutive patients with a frontal lesion. Neuropsychology 1997, 11, 187–194. [Google Scholar] [CrossRef]
- Tang, Y.; Harris, P.L.; Zou, H.; Wang, J.; Zhang, Z. The relationship between emotion understanding and social skills in preschoolers: The mediating role of verbal ability and the moderating role of working memory. Eur. J. Dev. Psychol. 2021, 18, 593–609. [Google Scholar] [CrossRef]
- Kenny, L.; Cribb, S.J.; Pellicano, E. Childhood Executive Function Predicts Later Autistic Features and Adaptive Behavior in Young Autistic People: A 12-Year Prospective Study. J. Abnorm. Child Psychol. 2019, 47, 1089–1099. [Google Scholar] [CrossRef]
- Van Eylen, L.; Boets, B.; Steyaert, J.; Wagemans, J.; Noens, I. Executive functioning in autism spectrum disorders: Influence of task and sample characteristics and relation to symptom severity. Eur. Child Adolesc. Psychiatry 2015, 24, 1399–1417. [Google Scholar] [CrossRef]
- Kjellmer, L.; Hedvall, Å.; Fernell, E.; Gillberg, C.; Norrelgen, F. Language and communication skills in preschool children with autism spectrum disorders: Contribution of cognition, severity of autism symptoms, and adaptive functioning to the variability. Res. Dev. Disabil. 2012, 33, 172–180. [Google Scholar] [CrossRef]
- White, S.W.; Keonig, K.; Scahill, L. Social Skills Development in Children with Autism Spectrum Disorders: A Review of the Intervention Research. J. Autism Dev. Disord. 2007, 37, 1858–1868. [Google Scholar] [CrossRef]
- Carter, A.S.; Davis, N.O.; Klin, A.; Volkmar, F.R. Social Development in Autism. In Handbook of Autism and Pervasive Developmental Disorders: Diagnosis, Development, Neurobiology, and Behavior, 3rd ed.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2005; Volume 1, pp. 312–334. [Google Scholar]
- Hilton, C.; Graver, K.; LaVesser, P. Relationship between social competence and sensory processing in children with high functioning autism spectrum disorders. Res. Autism Spectr. Disord. 2007, 1, 164–173. [Google Scholar] [CrossRef]
- Luyster, R.; Lopez, K.; Lord, C. Characterizing communicative development in children referred for Autism Spectrum Disorders using the MacArthur-Bates Communicative Development Inventory (CDI). J. Child Lang. 2007, 34, 623–654. [Google Scholar] [CrossRef] [PubMed]
- Waizbard-Bartov, E.; Ferrer, E.; Young, G.S.; Heath, B.; Rogers, S.; Nordahl, C.W.; Solomon, M.; Amaral, D.G. Trajectories of Autism Symptom Severity Change During Early Childhood. J. Autism Dev. Disord. 2021, 51, 227–242. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean (SD) | Range | Maximum Score |
|---|---|---|---|
| Sex (Female/Male) | 6/19 | - | - |
| ASD Functionality Level (1/2) | 14/11 | - | - |
| Age | 29.96 (9.76) | 19–52 | - |
| Education | 15.88 (2.26) | 12–20 | - |
| Cybersickness | 7.52 (2.04) | 6–14 | 42 |
| VR Experience | 3.48 (1.38) | 2–6 | 12 |
| Computing Experience | 8.96 (2.38) | 3–12 | 12 |
| Gaming Experience | 6.68 (3.13) | 2–12 | 12 |
| Acceptability | 104.28 (21.07) | 49–127 | 132 |
| User Experience | 126.00 (26.33) | 78–180 | 180 |
| Usability | 77.12 (12.08) | 54–98 | 100 |
| Task Completion Score | 27.56 (1.82) | 24–30 | 30 |
| Prompts’ Score | 11.68 (4.38) | 6–20 | - |
| RTMIE | 25.72 (5.21) | 8–33 | 36 |
| Digit Span Forward | 9.88 (2.33) | 4–14 | 16 |
| Digit Span Backward | 7.52 (2.88) | 2–13 | 14 |
| Tower of London | 7.88 (2.06) | 3–11 | 12 |
| Stroop—Correct Responses | 48.24 (4.01) | 30–50 | 50 |
| Strop—Response Time * | 65.44 (24.99) | 36–159 | - |
| Age | Education | VR XP | Computing XP | Gaming XP | ||
|---|---|---|---|---|---|---|
| Acceptability | Pearson’s r | 0.345 | −0.044 | 0.071 | 0.213 | −0.141 |
| p-value | 0.091 | 0.834 | 0.736 | 0.306 | 0.503 | |
| User Experience | Pearson’s r | 0.351 | −0.340 | −0.061 | 0.096 | −0.183 |
| p-value | 0.085 | 0.096 | 0.771 | 0.647 | 0.382 | |
| Usability | Pearson’s r | 0.119 | 0.031 | 0.269 | 0.310 | 0.169 |
| p-value | 0.572 | 0.884 | 0.193 | 0.131 | 0.420 |
| Age | Education | VR XP | Computing XP | Gaming XP | ||
|---|---|---|---|---|---|---|
| RTMIE | Pearson’s r | 0.059 | 0.372 | 0.276 | 0.427 * | 0.503 * |
| p-value | 0.780 | 0.067 | 0.181 | 0.033 | 0.010 | |
| DS Forward | Pearson’s r | −0.064 | 0.412 * | 0.281 | 0.331 | 0.348 |
| p-value | 0.760 | 0.040 | 0.173 | 0.106 | 0.088 | |
| DS Backward | Pearson’s r | 0.152 | 0.413 * | 0.108 | 0.195 | 0.237 |
| p-value | 0.469 | 0.040 | 0.607 | 0.349 | 0.255 | |
| ToL | Pearson’s r | 0.206 | 0.349 | 0.356 | 0.393 | 0.349 |
| p-value | 0.323 | 0.088 | 0.081 | 0.052 | 0.087 | |
| Stroop CR | Pearson’s r | 0.411 * | −0.049 | 0.100 | 0.267 | 0.193 |
| p-value | 0.041 | 0.815 | 0.635 | 0.197 | 0.354 | |
| Stroop RT | Pearson’s r | 0.037 | −0.227 | −0.340 | −0.380 | −0.483 * |
| p-value | 0.860 | 0.276 | 0.097 | 0.061 | 0.015 | |
| Prompts | Pearson’s r | −0.064 | −0.096 | 0.347 | −0.169 | −0.115 |
| p-value | 0.760 | 0.647 | 0.059 | 0.419 | 0.585 | |
| Task Completion | Pearson’s r | 0.177 | 0.206 | −0.392 | 0.468 * | 0.196 |
| p-value | 0.396 | 0.324 | 0.053 | 0.018 | 0.349 |
| Usability | Prompts | DS Forward | Stroop RT | ||
|---|---|---|---|---|---|
| ASD Functionality Level | Kendall’s Tau B | 0.488 ** | −0.406 * | 0.416 * | −0.365 * |
| p-value | 0.005 | 0.021 | 0.021 | 0.033 |
| Acceptability | User Experience | Usability | Prompts | Task Completion | ||
|---|---|---|---|---|---|---|
| Acceptability | Pearson’s r | - | - | - | - | - |
| p-value | - | - | - | - | - | |
| User Experience | Pearson’s r | 0.534 ** | - | - | - | - |
| p-value | 0.006 | - | - | - | - | |
| Usability | Pearson’s r | 0.693 *** | 0.486 * | - | - | - |
| p-value | <0.001 | 0.014 | - | - | - | |
| Prompts | Pearson’s r | −0.451 * | −0.200 | −0.757 *** | - | - |
| p-value | 0.024 | 0.339 | <0.001 | - | - | |
| Task Completion | Pearson’s r | 0.366 | 0.272 | 0.523 ** | −0.635 *** | - |
| p-value | 0.072 | 0.189 | 0.007 | <0.001 | - | |
| RTMIE | Pearson’s r | −0.076 | −0.158 | 0.004 | −0.014 | 0.107 |
| p-value | 0.716 | 0.452 | 0.987 | 0.947 | 0.611 | |
| DS Forward | Pearson’s r | 0.387 | 0.004 | 0.628 *** | −0.452 * | 0.285 |
| p-value | 0.056 | 0.986 | <0.001 | 0.023 | 0.167 | |
| DS Backward | Pearson’s r | 0.228 | 0.072 | 0.477 ** | −0.299 | 0.207 |
| p-value | 0.273 | 0.733 | 0.016 | 0.146 | 0.321 | |
| ToL | Pearson’s r | 0.354 | 0.001 | 0.685 *** | −0.499 * | 0.262 |
| p-value | 0.083 | 0.995 | <0.001 | 0.011 | 0.206 | |
| Stroop CR | Pearson’s r | 0.039 | 0.145 | 0.182 | −0.187 | 0.370 |
| p-value | 0.852 | 0.490 | 0.383 | 0.370 | 0.069 | |
| Stroop RT | Pearson’s r | −0.203 | 0.032 | −0.569 ** | 0.313 | 0.118 |
| p-value | 0.330 | 0.879 | 0.003 | 0.128 | 0.576 |
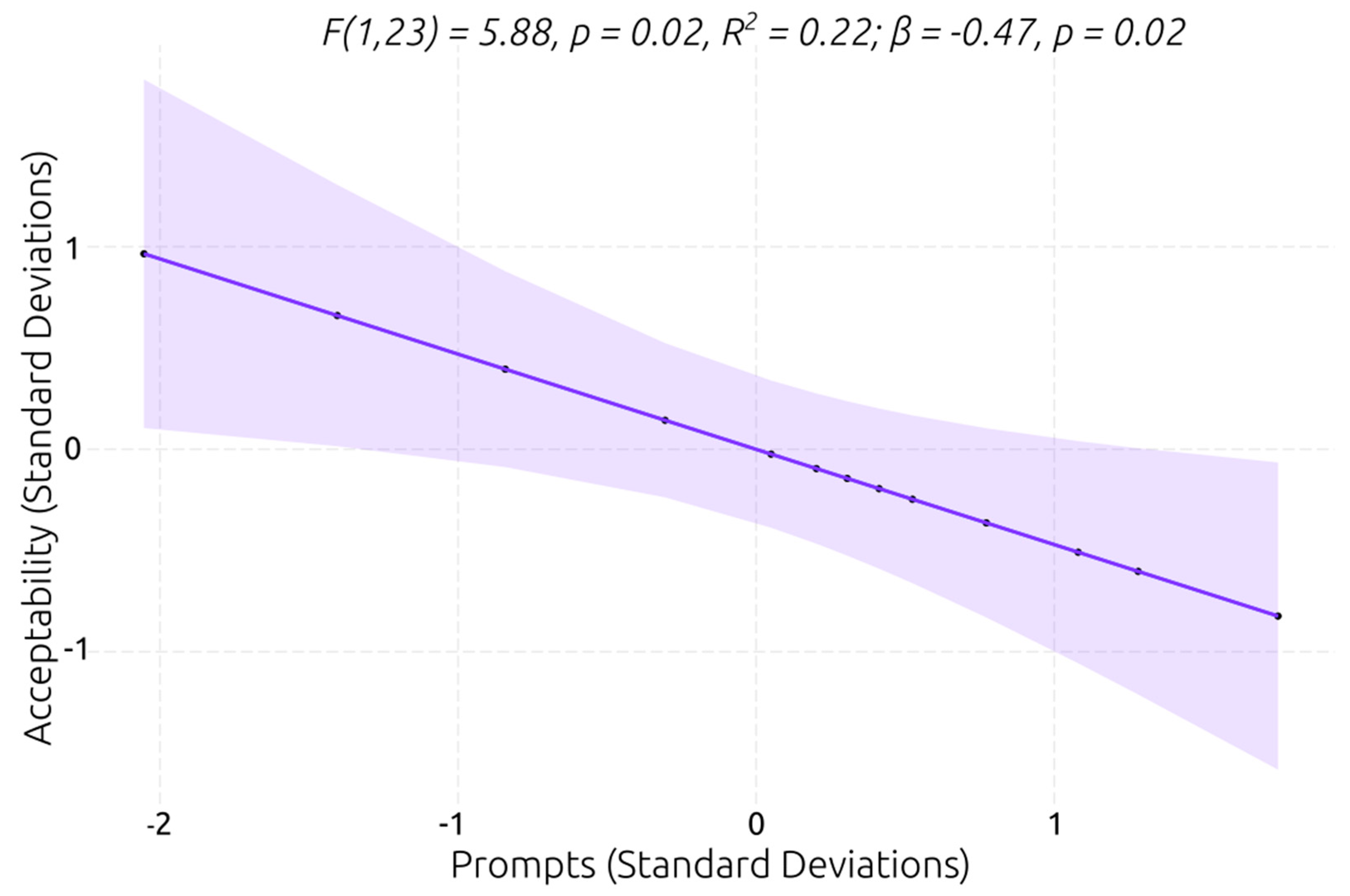
| Predictor | χ2 | p-Value (χ2) | β Coefficient | p-Value (β) | R2 |
|---|---|---|---|---|---|
| Prompts | 6.22 | 0.01 * | −1.25 | 0.03 * | 0.30 |
| DS Forward | 5.83 | 0.02 * | 1.22 | 0.04 * | 0.28 |
| Stroop RT | 5.30 | 0.02 * | −1.09 | 0.04 * | 0.26 |
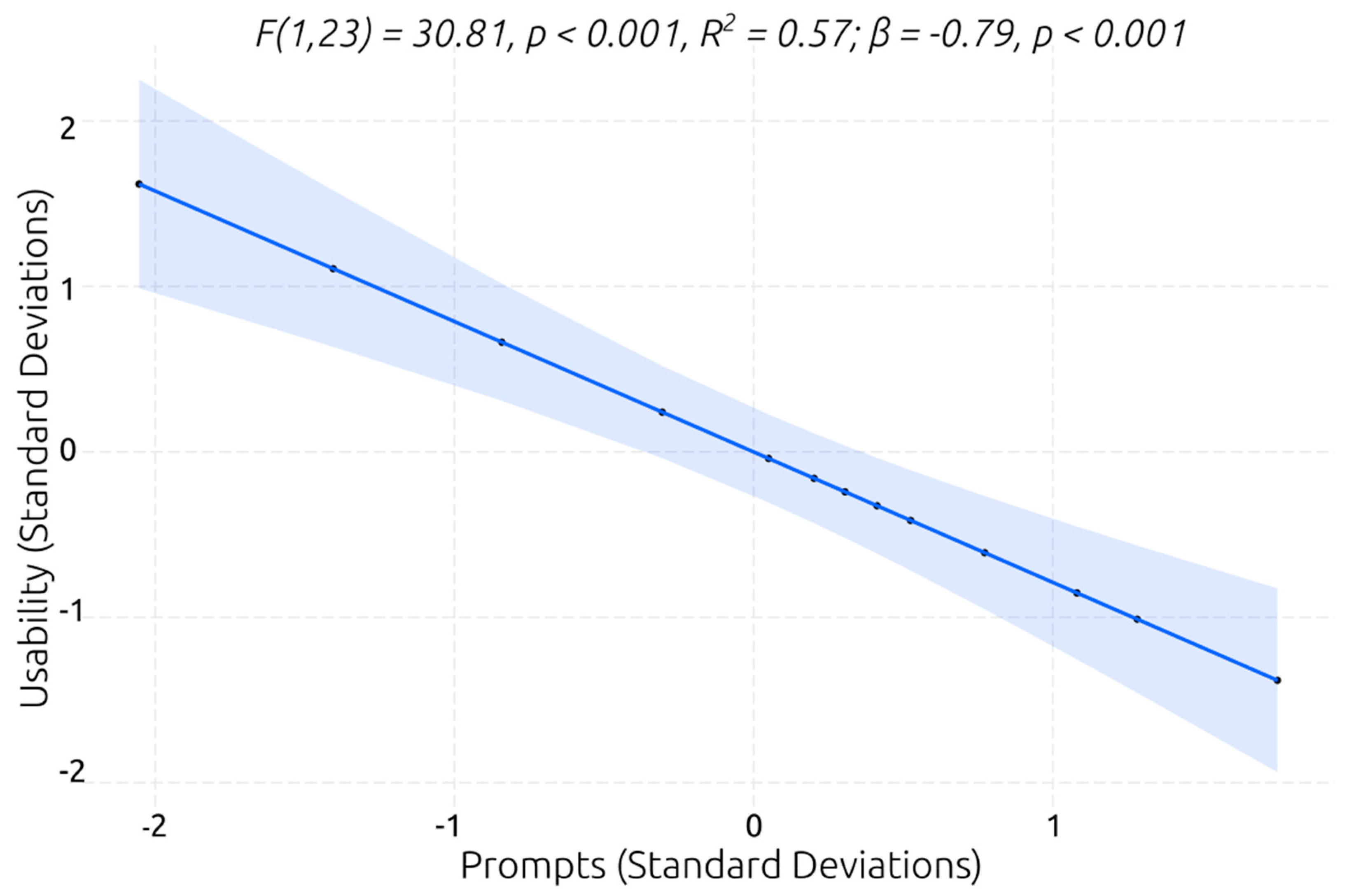
| Predictor | F | p-Value (F) | β Coefficient | p-Value (β) | R2 |
|---|---|---|---|---|---|
| Prompts | 30.81 | <0.001 *** | −0.79 | <0.001 *** | 0.57 |
| ToL | 20.37 | <0.001 *** | 0.69 | <0.001 *** | 0.47 |
| DS Forward | 14.98 | <0.001 *** | 0.67 | <0.001 *** | 0.39 |
| Task Completion | 8.64 | 0.01 ** | 0.52 | 0.01 ** | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kourtesis, P.; Kouklari, E.-C.; Roussos, P.; Mantas, V.; Papanikolaou, K.; Skaloumbakas, C.; Pehlivanidis, A. Virtual Reality Training of Social Skills in Adults with Autism Spectrum Disorder: An Examination of Acceptability, Usability, User Experience, Social Skills, and Executive Functions. Behav. Sci. 2023, 13, 336. https://doi.org/10.3390/bs13040336
Kourtesis P, Kouklari E-C, Roussos P, Mantas V, Papanikolaou K, Skaloumbakas C, Pehlivanidis A. Virtual Reality Training of Social Skills in Adults with Autism Spectrum Disorder: An Examination of Acceptability, Usability, User Experience, Social Skills, and Executive Functions. Behavioral Sciences. 2023; 13(4):336. https://doi.org/10.3390/bs13040336
Chicago/Turabian StyleKourtesis, Panagiotis, Evangelia-Chrysanthi Kouklari, Petros Roussos, Vasileios Mantas, Katerina Papanikolaou, Christos Skaloumbakas, and Artemios Pehlivanidis. 2023. "Virtual Reality Training of Social Skills in Adults with Autism Spectrum Disorder: An Examination of Acceptability, Usability, User Experience, Social Skills, and Executive Functions" Behavioral Sciences 13, no. 4: 336. https://doi.org/10.3390/bs13040336