
The Risk-Taking and Self-Harm Inventory for Adolescents: Validation of the Italian Version (RTSHIA-I)
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Measures
2.2.1. Risk Taking and Self-Harm Inventory for Adolescents—Italian Version
2.2.2. Difficulties in Emotion Regulation Scale
2.2.3. The Assessment of Psychopathology in Adolescence Questionnaire
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Exploratory Factor Analysis
3.2. Descriptive Analysis of RTSHIA Items
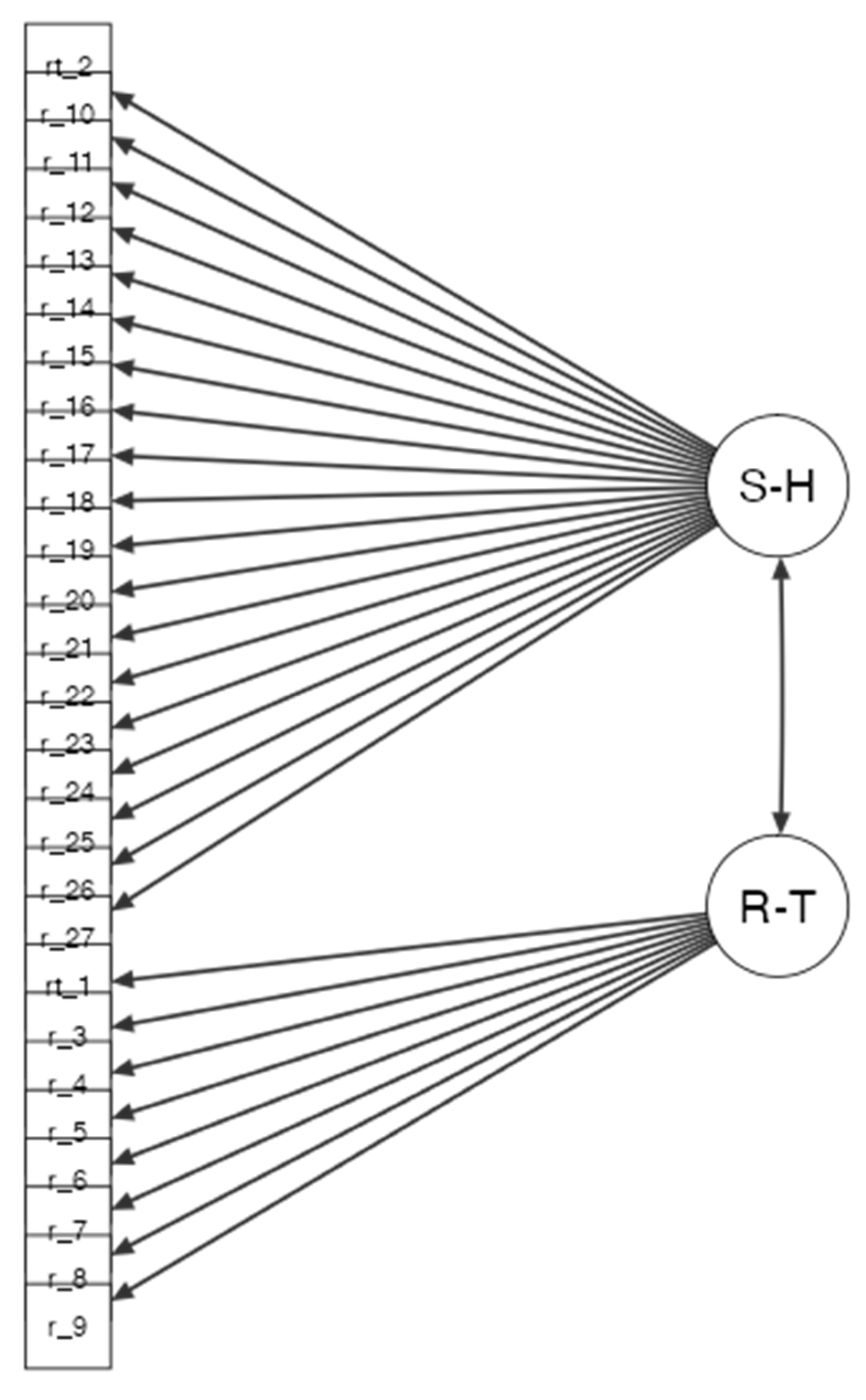
3.3. Confirmatory Factor Analysis
3.4. Reliability and Validity Analyses
4. Discussion
4.1. Limitations
4.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Risk-Taking and Self-Harm Inventory for Adolescents
Appendix A.1. Instructions
- Please complete this questionnaire on your own.
- If a statement is not applicable to you, please circle Never.
- You do not have to answer any questions that you prefer not to answer.
- Please try to answer as truthfully as possible.
- All your answers are kept strictly confidential.
| 1 | Have you ever put yourself in a risky situation (such as classroom cheating, traveling without a valid ticket, shoplifting, etc.) knowing that you may get caught? | Never | Once | More than once | Many times |
| 1 | Ti sei mai messo in una situazione pericolosa (ad esempio, saltare la scuola, viaggiare senza biglietto, rubare in un negozio), sapendo di poter essere scoperto? | Mai | Una volta | Più di una volta | Molto spesso |
| 2 | Have you ever been suspended (i.e., punished with exclusion) or dropped out of school? | Never | Once | More than once | Many times |
| 2 | Sei mai stato sospeso (punito con il divieto di entrare in classe) o espulso da scuola? | Mai | Una volta | Più di una volta | Molto spesso |
| 3 | Have you ever stayed out late at night, without your parents knowing where you are? | Never | Once | More than once | Many times |
| 3 | Sei mai stato fuori fino a tarda notte, senza che i tuoi genitori sapessero dov’eri? | Mai | Una volta | Più di una volta | Molto spesso |
| 4 | Have you ever participated in gang violence or physical fights or held a weapon? | Never | Once | More than once | Many times |
| 4 | Hai mai partecipato a una rissa, fatto a botte o tenuto in mano un’arma? | Mai | Una volta | Più di una volta | Molto spesso |
| 5 | Have you ever been promiscuous (i.e., had many sexual partners within a short period of time)? | Never | Once | More than once | Many times |
| 5 | Ti è mai capitato di fare sesso con più persone nel giro di poco tempo? | Mai | Una volta | Più di una volta | Molto spesso |
| - | |||||
| 6 | Hai mai fatto sesso senza proteggerti dal rischio di prendere qualche malattia o di una gravidanza? | Mai | Una volta | Più di una volta | Molto spesso |
| 7 | Have you ever had so much alcohol that you were really drunk? | Never | Once | More than once | Many times |
| 7 | Hai mai bevuto alcolici fino ad essere completamente ubriaco? | Mai | Una volta | Più di una volta | Molto spesso |
| 8 | Have you ever used drugs (such as marijuana, cocaine, LSD, etc.)? | Never | Once | More than once | Many times |
| 8 | Hai mai fatto uso di droghe (come marijuana, cocaina, LSD o altro)? | Mai | Una volta | Più di una volta | Molto spesso |
| 9 | Have you ever smoked tobacco? | Never | Once | More than once | Many times |
| 9 | Hai mai fumato tabacco? | Mai | Una volta | Più di una volta | Molto spesso |
| 10 | Have you ever intentionally cut your skin? | Never | Once | More than once | Many times |
| 10 | Ti sei mai procurato intenzionalmente dei tagli? | Mai | Una volta | Più di una volta | Molto spesso |
| 11 | Have you ever intentionally burned yourself with a hot object (such as a cigarette)? | Never | Once | More than once | Many times |
| 11 | Ti sei mai fatto volontariamente una bruciatura con qualcosa di rovente (come per esempio una sigaretta accesa)? | Mai | Una volta | Più di una volta | Molto spesso |
| 12 | Have you ever intentionally bitten yourself, to the extent that you broke the skin? | Never | Once | More than once | Many times |
| 12 | Ti sei mai morsicato da solo, fino al punto di lacerare la pelle? | Mai | Una volta | Più di una volta | Molto spesso |
| 13 | Have you ever intentionally banged your head against something or hit or punched yourself, to the extent that you caused a bruise to appear? | Never | Once | More than once | Many times |
| 13 | Ti sei mai fatto venire un livido o un bernoccolo sbattendo intenzionalmente la testa contro qualcosa oppure colpendoti da solo? | Mai | Una volta | Più di una volta | Molto spesso |
| 14 | Have you ever intentionally prevented wounds from healing or picked at areas of your body to the point of drawing blood? | Never | Once | More than once | Many times |
| 14 | Hai mai fatto qualcosa per evitare che una ferita guarisse, o ti sei mai ferito da solo in una qualsiasi parte del corpo? | Mai | Una volta | Più di una volta | Molto spesso |
| 15 | Have you ever intentionally scraped, scrubbed, or scratched your skin to the point of breaking your skin or drawing blood? | Never | Once | More than once | Many times |
| 15 | Hai mai raschiato, rimosso o graffiato volontariamente la tua pelle fino al punto di farla sanguinare? | Mai | Una volta | Più di una volta | Molto spesso |
| 16 | Have you ever intentionally rubbed a sharp object (such as sandpaper) or dripped anything toxic (such as acid) onto your skin? | Never | Once | More than once | Many times |
| 16 | Hai mai strofinato volontariamente un oggetto tagliente (per esempio, carta vetrata) o versato qualcosa di tossico (come un acido) sulla tua pelle? | Mai | Una volta | Più di una volta | Molto spesso |
| 17 | Have you ever exercised an injured part of your body intending to hurt yourself? | Never | Once | More than once | Many times |
| 17 | Hai mai forzato una parte del tuo corpo che ti faceva male, con lo scopo di fartene ancora? | Mai | Una volta | Più di una volta | Molto spesso |
| 18 | Have you ever intentionally pulled your hair out? | Never | Once | More than once | Many times |
| 18 | Ti sei mai strappato i capelli di proposito? | Mai | Una volta | Più di una volta | Molto spesso |
| 19 | Have you ever starved yourself to hurt or punish yourself? | Never | Once | More than once | Many times |
| 19 | Hai mai rifiutato di mangiare allo scopo di punire te stesso? | Mai | Una volta | Più di una volta | Molto spesso |
| 20 | Have you ever forced yourself to eat too much to hurt or punish yourself? | Never | Once | More than once | Many times |
| 20 | Ti sei mai obbligato a mangiare così tanto da star male, con lo scopo di provocarti dolore o di punire te stesso? | Mai | Una volta | Più di una volta | Molto spesso |
| 21 | Have you ever stayed in a friendship or a relationship with somebody who repeatedly hurt your feelings on purpose? | Never | Once | More than once | Many times |
| 21 | Sei mai stato coinvolto in un’amicizia o in una relazione con qualcuno che feriva ripetutamente e di proposito i tuoi sentimenti? | Mai | Una volta | Più di una volta | Molto spesso |
| 22 | Have you ever tried to make yourself suffer by thinking horrible things about yourself? | Never | Once | More than once | Many times |
| 22 | Hai mai tentato di provocarti dolore pensando cose orribili di te stesso? | Mai | Una volta | Più di una volta | Molto spesso |
| 23 | Have you ever taken an overdose? (i.e., taken an excessive amount of medication without having been prescribed this dosage) | Never | Once | More than once | Many times |
| 23 | Hai mai preso un’overdose (per esempio, un quantitativo eccessivo di un farmaco, senza che quel dosaggio ti fosse prescritto)? | Mai | Una volta | Più di una volta | Molto spesso |
| 24 | Have you ever seriously thought about harming a part of your body? | Never | Once | More than once | Many times |
| 24 | Hai mai pensato sul serio di farti fisicamente del male? | Mai | Una volta | Più di una volta | Molto spesso |
| 25 | Have you ever seriously thought about killing yourself? | Never | Once | More than once | Many times |
| 25 | Hai mai pensato di toglierti la vita? | Mai | Una volta | Più di una volta | Molto spesso |
| 26 | Have you ever tried to kill yourself? | Never | Once | More than once | Many times |
| 26 | Hai mai tentato di ucciderti? | Mai | Una volta | Più di una volta | Molto spesso |
| 27 | Have you ever intentionally hurt yourself in any of the abovementioned ways so that it led to hospitalization or injury severe enough to require medical treatment? | Never | Once | More than once | Many times |
| 27 | Ti sei mai provocato delle lesioni in uno dei modi descritti sopra, fino al punto di dover andare in ospedale o di dover ricorrere a cure mediche? | Mai | Una volta | Più di una volta | Molto spesso |
References
- Van der Kolk, B.A.; Perry, J.C.; Herman, J.L. Childhood Origins of Self-Destructive Behavior. Am. J. Psychiatry 1991, 148, 1665–1671. [Google Scholar] [CrossRef] [PubMed]
- Boyer, T.W. The Development of Risk-Taking: A Multi-Perspective Review. Dev. Rev. 2006, 26, 291–345. [Google Scholar] [CrossRef]
- Dahlen, E.R.; Martin, R.C.; Ragan, K.; Kuhlman, M.M. Driving Anger, Sensation Seeking, Impulsiveness, and Boredom Proneness in the Prediction of Unsafe Driving. Accid. Anal. Prev. 2005, 37, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Hoyle, R.H.; Fejfar, M.C.; Miller, J.D. Personality and Sexual Risk Taking: A Quantitative Review. J. Pers. 2000, 68, 1203–1231. [Google Scholar] [CrossRef]
- Zuckerman, M.; Kuhlman, D.M. Personality and Risk-Taking: Common Biosocial Factors. J. Pers. 2000, 68, 999–1029. [Google Scholar] [CrossRef]
- Pérez, J.; Torrubia, R. Sensation Seeking and Antisocial Behaviour in a Student Sample. Personal. Individ. Differ. 1985, 6, 401–403. [Google Scholar] [CrossRef]
- Murtagh, A.M.; Todd, S.A. Self-Regulation: A Challenge to the Strength Model. J. Artic. Support Null Hypothesis 2004, 3, 32. [Google Scholar]
- Magar, E.; Phillips, L.; Hosie, J. Self-Regulation and Risk-Taking. Personal. Individ. Differ. 2008, 45, 153–159. [Google Scholar] [CrossRef]
- Do, S.; Coumans, J.M.J.; Börnhorst, C.; Pohlabeln, H.; Reisch, L.A.; Danner, U.N.; Russo, P.; Veidebaum, T.; Tornaritis, M.; Molnár, D.; et al. Associations Between Psychosocial Well-Being, Stressful Life Events and Emotion-Driven Impulsiveness in European Adolescents. J. Youth Adolesc. 2022, 51, 1106–1117. [Google Scholar] [CrossRef]
- Patterson, M.W.; Pivnick, L.; Mann, F.D.; Grotzinger, A.D.; Monahan, K.C.; Steinberg, L.D.; Oosterhoff, B.; Tackett, J.L.; Tucker-Drob, E.M.; Harden, K.P.; et al. A mixed-methods approach to refining and measuring the construct of positive risk-taking in adolescence. J. Res. Adolesc. 2022, 1–21. [Google Scholar] [CrossRef]
- Banfield, J.F.; Wyland, C.L.; Macrae, C.N.; Münte, T.F.; Heatherton, T.F. The Cognitive Neuroscience of Self-Regulation. In Handbook of Self-Regulation: Research, Theory, and Applications; The Guilford Press: New York, NY, USA, 2004; pp. 62–83. ISBN 978-1-57230-991-3. [Google Scholar]
- Lauriola, M.; Cerniglia, L.; Tambelli, R.; Cimino, S. Deliberative and Affective Risky Decisions in Teenagers: Different Associations with Maladaptive Psychological Functioning and Difficulties in Emotion Regulation? Children 2022, 9, 1915. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association, Ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-554-1. [Google Scholar]
- Simeon, D.; Favazza, A.R. Self-Injurious Behaviors: Phenomenology and Assessment. In Self-Injurious Behaviors: Assessment and Treatment; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2001; pp. 1–28. ISBN 978-0-88048-808-2. [Google Scholar]
- Nock, M.K.; Favazza, A.R. Nonsuicidal Self-Injury: Definition and Classification. In Understanding Nonsuicidal Self-Injury: Origins, Assessment, and Treatment; American Psychological Association: Washington, DC, USA, 2009; pp. 9–18. ISBN 978-1-4338-0436-6. [Google Scholar]
- Pattison, E.M.; Kahan, J. The Deliberate Self-Harm Syndrome. Am. J. Psychiatry 1983, 140, 867–872. [Google Scholar] [CrossRef]
- Muehlenkamp, J.J.; Claes, L.; Havertape, L.; Plener, P.L. International Prevalence of Adolescent Non-Suicidal Self-Injury and Deliberate Self-Harm. Child Adolesc. Psychiatry Ment. Health 2012, 6, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swannell, S.V.; Martin, G.E.; Page, A.; Hasking, P.; St John, N.J. Prevalence of Nonsuicidal Self-Injury in Nonclinical Samples: Systematic Review, Meta-Analysis and Meta-Regression. Suicide Life Threat. Behav. 2014, 44, 273–303. [Google Scholar] [CrossRef]
- Gillies, D.; Christou, M.A.; Dixon, A.C.; Featherston, O.J.; Rapti, I.; Garcia-Anguita, A.; Villasis-Keever, M.; Reebye, P.; Christou, E.; Al Kabir, N.; et al. Prevalence and Characteristics of Self-Harm in Adolescents: Meta-Analyses of Community-Based Studies 1990–2015. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 733–741. [Google Scholar] [CrossRef]
- Evans, E.; Hawton, K.; Rodham, K. In What Ways Are Adolescents Who Engage in Self-harm or Experience Thoughts of Self-harm Different in Terms of Help-seeking, Communication and Coping Strategies? J. Adolesc. 2005, 28, 573–587. [Google Scholar] [CrossRef]
- Cerutti, R.; Manca, M.; Presaghi, F.; Gratz, K.L. Prevalence and Clinical Correlates of Deliberate Self-Harm among a Community Sample of Italian Adolescents. J. Adolesc. 2011, 34, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Uh, S.; Dalmaijer, E.S.; Siugzdaite, R.; Ford, T.J.; Astle, D.E. Two Pathways to Self-Harm in Adolescence. J. Am. Acad. Child Adolesc. Psychiatry 2021, 60, 1491–1500. [Google Scholar] [CrossRef]
- Hetrick, S.E.; Subasinghe, A.; Anglin, K.; Hart, L.; Morgan, A.; Robinson, J. Understanding the Needs of Young People Who Engage in Self-Harm: A Qualitative Investigation. Front. Psychol. 2020, 10, 2916. [Google Scholar] [CrossRef]
- Russo, J.E.; Dhruve, D.M.; Oliveros, A.D. Role of developmental timing of childhood adversity in nonsuicidal self-injury persistence or desistance. Res. Child Adolesc. Psychopathol. 2023, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K. Self-Injury. Annu. Rev. Clin. Psychol. 2010, 6, 339–363. [Google Scholar] [CrossRef]
- Meszaros, G.; Horvath, L.O.; Balazs, J. Self-Injury and Externalizing Pathology: A Systematic Literature Review. BMC Psychiatry 2017, 17, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossouw, T.I.; Fonagy, P. Mentalization-Based Treatment for Self-Harm in Adolescents: A Randomized Controlled Trial. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 1304–1313.e3. [Google Scholar] [CrossRef] [PubMed]
- Woodley, S.; Hodge, S.; Jones, K.; Holding, A. How Individuals Who Self-Harm Manage Their Own Risk-’I Cope Because I Self-Harm, and I Can Cope with My Self-Harm’. Psychol. Rep. 2020, 124, 1998–2017. [Google Scholar] [CrossRef]
- Xin, M.; Yang, X.; Liu, K.; Naz Boke, B.; Bastien, L. Impact of Negative Life Events and Social Support on Nonsuicidal Self-Injury Among Chinese Middle School Students. Am. J. Mens. Health 2020, 14, 155798832093712. [Google Scholar] [CrossRef]
- Mucci, M.; Lenzi, F.; D’Acunto, G.M.; Gazzillo, M.; Accorinti, I.; Boldrini, S.; Distefano, G.; Falcone, F.; Fossati, B.; Giurdanella Annina, R.; et al. How COVID-19 Phases Have Impacted Psychiatric Risk: A Retrospective Study in an Emergency Care Unit for Adolescents. Children 2022, 9, 1921. [Google Scholar] [CrossRef] [PubMed]
- Beghi, M.; Ferrari, S.; Biondi, L.; Brandolini, R.; Corsini, C.; De Paoli, G.; Sant’Angelo, R.P.; Fraticelli, C.; Casolaro, I.; Zinchuk, M.; et al. Mid-term psychiatric consequences of the covid-19 pandemic: A 4 months observational study on emergency room admissions for psychiatric evaluation after the (first) lockdown period in Italy. Soc. Psychiatry Psychiatr. Epidemiol. Int. J. Res. Soc. Genet. Epidemiol. Ment. Health Serv. 2022, 57, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Vrouva, I.; Fonagy, P.; Fearon, P.R.M.; Roussow, T. The Risk-Taking and Self-Harm Inventory for Adolescents: Development and Psychometric Evaluation. Psychol. Assess. 2010, 22, 852–865. [Google Scholar] [CrossRef] [Green Version]
- Favazza, A.R. Bodies under Siege: Self-Mutilation and Body Modification in Culture and Psychiatry, 2nd ed.; Johns Hopkins University Press: Baltimore, MD, USA, 1996; ISBN 978-0-8018-5299-2. [Google Scholar]
- Steinberg, L. A Social Neuroscience Perspective on Adolescent Risk-Taking. Dev. Rev. 2008, 28, 78–106. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, L. Risk Taking in Adolescence: What Changes, and Why? Ann. New York Acad. Sci. 2004, 1021, 51–58. [Google Scholar] [CrossRef]
- Xavier, A.; Cunha, M.; Pinto-Gouveia, J. Validation of the Risk-Taking and Self-Harm Inventory for Adolescents in a Portuguese Community Sample. Meas. Eval. Couns. Dev. 2019, 52, 1–14. [Google Scholar] [CrossRef]
- Gratz, K.L. Measurement of Deliberate Self-Harm: Preliminary Data on the Deliberate Self-Harm Inventory. J. Psychopathol. Behav. Assess. 2001, 23, 253. [Google Scholar] [CrossRef]
- Monti, M.R.; D’Agostino, A. Il Deliberate Self-Harm Inventory (DSHI): Validazione linguistico-culturale della versione Italiana. Psichiatr. E Psicoter. 2010, 29, 47–53. [Google Scholar]
- Prinstein, M.J.; Nock, M.K.; Simon, V.; Aikins, J.W.; Cheah, C.S.L.; Spirito, A. Longitudinal Trajectories and Predictors of Adolescent Suicidal Ideation and Attempts Following Inpatient Hospitalization. J. Consult. Clin. Psychol. 2008, 76, 92–103. [Google Scholar] [CrossRef] [Green Version]
- Giletta, M.; Scholte, R.H.J.; Engels, R.C.M.E.; Ciairano, S.; Prinstein, M.J. Adolescent Non-Suicidal Self-Injury: A Cross-National Study of Community Samples from Italy, the Netherlands and the United States. Psychiatry Res. 2012, 197, 66–72. [Google Scholar] [CrossRef] [Green Version]
- Ougrin, D.; Wong, B.H.-C.; Vaezinejad, M.; Plener, P.L.; Mehdi, T.; Romaniuk, L.; Barrett, E.; Hussain, H.; Lloyd, A.; Tolmac, J.; et al. Pandemic-Related Emergency Psychiatric Presentations for Self-Harm of Children and Adolescents in 10 Countries (PREP-Kids): A Retrospective International Cohort Study. Eur. Child. Adolesc. Psychiatry 2021. [Google Scholar] [CrossRef]
- Wright, A.J. Clinical Applications of European Adolescent Assessment Research. J. Personal. Assess. 2020, 102, 440–442. [Google Scholar] [CrossRef]
- Robillard, C.L.; Turner, B.J.; Ames, M.E.; Craig, S.G. Deliberate Self-Harm in Adolescents during COVID-19: The Roles of Pandemic-Related Stress, Emotion Regulation Difficulties, and Social Distancing. Psychiatry Res. 2021, 304, 114152. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, A.; Bracaglia, E.; Cavalli, G.; Valle, A. Comportamenti a Rischio e Autolesivi in Adolescenza. II Questionario RTSHIA Di Vrouva, Fonagy, Fearon, Roussow; Franco Angeli: Milan, Italy, 2013. [Google Scholar]
- Gratz, K.L.; Roemer, L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Sighinolfi, C.; Pala, A.N.; Chiri, L.R.; Marchetti, I.; Sica, C. Difficulties in Emotion Regulation Scale (DERS): Traduzione e Adattamento Italiano. [Difficulties in Emotion Regulation Scale (DERS): The Italian Translation and Adaptation]. Psicoter. Cogn. E Comport. 2010, 16, 141–170. [Google Scholar]
- Sica, C.; Rocco Chiri, L.; Favilli, R.; Marchetti, I. Questionario per La Valutazione Della Psicopatología in Adolescenza; Erickson: Trento, Italy, 2011. [Google Scholar]
- Comrey, A.L.; Lee, H.B. A First Course in Factor Analysis, 2nd ed.; Psychology Press: New York, NY, USA, 2013; ISBN 978-1-315-82750-6. [Google Scholar]
- Lundh, L.-G.; Karim, J.; Quilisch, E. Deliberate Self-Harm in 15-Year-Old Adolescents: A Pilot Study with a Modified Version of the Deliberate Self-Harm Inventory. Scand J. Psychol. 2007, 48, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Horn, J.L. A Rationale and Test for the Number of Factors in Factor Analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Westen, D.; Lohr, N.; Sils, K.R.; Gold, L.; Kerber, K. Object Relations and Social Cognition in Borderlines, Major Depressives, and Normals: A Thematic Apperception Test Analysis. Psychol. Assess. A J. Consult. Clin. Psychol. 1990, 2, 355–364. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.; Babin, J.A.; Andeerson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Prentice Hall: Hoboken, NJ, USA, 2010. [Google Scholar]
- Bentler, P.M. Comparative Fit Indexes in Structural Models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Thompson, B.; Wang, L. Effects of Sample Size, Estimation Methods, and Model Specification on Structural Equation Modeling Fit Indexes. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 56–83. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. In Testing Structural Equation Models; Sage: Newbury Park, CA, USA, 1993; pp. 136–162. [Google Scholar]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]
- Aggarwal, S.; Patton, G.; Reavley, N.; Sreenivasan, S.A.; Berk, M. Youth Self-Harm in Low- and Middle-Income Countries: Systematic Review of the Risk and Protective Factors. Int. J. Soc. Psychiatry 2017, 63, 359–375. [Google Scholar] [CrossRef]
- Vrouva, I.; Midgley, N. Minding the Child: Mentalization-Based Interventions with Children, Young People and their Families; Routledge: London, UK, 2012. [Google Scholar]
- Stagaki, M.; Nolte, T.; Feigenbaum, J.; King-Casas, B.; Lohrenz, T.; Fonagy, P.; Montague, P.R. The Mediating Role of Attachment and Mentalising in the Relationship between Childhood Maltreatment, Self-Harm and Suicidality. Child Abus. Negl. 2022, 128, 105576. [Google Scholar] [CrossRef]
- Fonagy, P.; Campbell, C. Attachment Theory and Mentalization. In The Routledge Handbook of Psychoanalysis in the Social Sciences and Humanities; Routledge: London, UK, 2016; ISBN 978-1-315-65082-1. [Google Scholar]
- Valle, A.; Massaro, D.; Rinaldi, T.; Castelli, I.; Lombardi, E.; Bracaglia, E.A.; Intra, F.S.; Marchetti, A. Attachment Representation, Mentalization and Cognitive Emotion Regulation Strategies at School. Ric. Di Psicol. 2019, 42, 83–102. [Google Scholar] [CrossRef]
- Valle, A.; Rinaldi, T.; Greco, A.; Pianta, R.C.; Castelli, I.; Marchetti, A. Mentalization and Attachment in Educational Relationships in Primary School. Ric. Di Psicol. 2022, 45, 1–23. [Google Scholar] [CrossRef]
- Chung, T. Adolescent substance use: Symptoms and course. In Comprehensive Addictive Behaviors and Disorders, Volume 1: Principles of Addiction; Elsevier Academic Press: San Diego, CA, USA, 2013; pp. 97–106, Chapter xv; 941, ISBN 978-0-12-398336-7. [Google Scholar]
- Martínez-Ferrer, B.; Stattin, H. A Mutual Hostility Explanation for the Co-Occurrence of Delinquency and Depressive Mood in Adolescence. J. Abnorm. Child Psychol. 2017, 45, 1399–1412. [Google Scholar] [CrossRef] [PubMed]
- Latina, D.; Stattin, H. Adolescents Who Self-Harm: The Patterns in Their Interpersonal and Psychosocial Difficulties. J. Res Adolesc 2018, 28, 824–838. [Google Scholar] [CrossRef] [PubMed]
- Naz, A.; Naureen, A.; Kiran, T.; Husain, M.O.; Minhas, A.; Razzaque, B.; Tofique, S.; Husain, N.; Furber, C.; Chaudhry, N. Exploring Lived Experiences of Adolescents Presenting with Self-Harm and Their Views about Suicide Prevention Strategies: A Qualitative Approach. Int. J. Environ. Res. Public Health 2021, 18, 4694. [Google Scholar] [CrossRef] [PubMed]
- De Luca, L.; Giletta, M.; Nocentini, A.; Menesini, E. Non-Suicidal Self-Injury in Adolescence: The Role of Pre-Existing Vulnerabilities and COVID-19-Related Stress. J. Youth Adolesc. 2022, 51, 2383–2395. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| RTSHIA Item | Factor 1 SELF-HARM | Factor 2 RISK-TAKING |
|---|---|---|
| Item 1 | 0.658 | |
| Item 2 | 0.531 | |
| Item 3 | 0.785 | |
| Item 4 | 0.447 | |
| Item 5 | 0.525 | |
| Item 6 | 0.534 | |
| Item 7 | 0.843 | |
| Item 8 | 0.827 | |
| Item 9 | 0.732 | |
| Item 10 | 0.920 | |
| Item 11 | 0.847 | |
| Item 12 | 0.876 | |
| Item 13 | 0.834 | |
| Item 14 | 0.903 | |
| Item 15 | 0.884 | |
| Item 16 | 0.930 | |
| Item 17 | 0.856 | |
| Item 18 | 0.715 | |
| Item 19 | 0.821 | |
| Item 20 | 0.863 | |
| Item 21 | 0.592 | |
| Item 22 | 0.872 | |
| Item 23 | 0.839 | |
| Item 24 | 0.870 | |
| Item 25 | 0.856 | |
| Item 26 | 0.916 | |
| Item 27 | 0.897 |
| Mean | Standard deviation | Skewness | Kurtosis | |
|---|---|---|---|---|
| Item 1 | 1.30 | 1.097 | 0.650 | −0.310 |
| Item 2 | 0.45 | 0.620 | 1.551 | 3.939 |
| Item 3 | 0.99 | 0.935 | 0.890 | 0.389 |
| Item 4 | 0.67 | 0.894 | 1.575 | 2.631 |
| Item 5 | 0.52 | 0.746 | 2.202 | 7.686 |
| Item 6 | 0.67 | 0.854 | 1.931 | 5.640 |
| Item 7 | 0.90 | 0.916 | 1.042 | 0.907 |
| Item 8 | 0.77 | 0.926 | 1.439 | 2.202 |
| Item 9 | 1.31 | 1.150 | 0.776 | −0.133 |
| Item 10 | 0.49 | 0.738 | 1.940 | 5.216 |
| Item 11 | 0.41 | 0.586 | 1.362 | 2.219 |
| Item 12 | 0.47 | 0.670 | 1.758 | 4.500 |
| Item 13 | 0.49 | 0.698 | 1.478 | 2.313 |
| Item 14 | 0.53 | 0.766 | 1.978 | 5.718 |
| Item 15 | 0.49 | 0.693 | 1.687 | 3.707 |
| Item 16 | 0.40 | 0.586 | 1.882 | 7.350 |
| Item 17 | 0.47 | 0.710 | 2.129 | 7.278 |
| Item 18 | 0.47 | 0.684 | 1.718 | 4.064 |
| Item 19 | 0.63 | 0.838 | 1.639 | 3.214 |
| Item 20 | 0.40 | 0.550 | 1.099 | 1.153 |
| Item 21 | 0.70 | 0.886 | 1.431 | 2.152 |
| Item 22 | 0.60 | 0.838 | 1.926 | 4.905 |
| Item 23 | 0.39 | 0.522 | 0.857 | −0.076 |
| Item 24 | 0.58 | 0.834 | 1.780 | 3.579 |
| Item 25 | 0.59 | 0.855 | 1.839 | 4.054 |
| Item 26 | 0.39 | 0.553 | 1.344 | 3.025 |
| Item 27 | 0.38 | 0.530 | 1.200 | 1.882 |
| RMSEA 90% CI | ||||
|---|---|---|---|---|
| CFI | SRMR | RMSEA | Lower | Upper |
| 0.898 | 0.053 | 0.096 | 0.092 | 0.099 |
| RMSEA 90% CI | ||||
|---|---|---|---|---|
| CFI | SRMR | RMSEA | Lower | Upper |
| 0.930 | 0.050 | 0.081 | 0.077 | 0.085 |
| Index | Value |
|---|---|
| Comparative Fit Index (CFI) | 0.911 |
| Root mean square error of approximation (RMSEA) | 0.094 |
| Standardized root mean square residual (SRMR) | 0.050 |
| Index | Value |
|---|---|
| Comparative Fit Index (CFI) | 0.891 |
| Root mean square error of approximation (RMSEA) | 0.073 |
| Standardized root mean square residual (SRMR) | 0.076 |
| Self-harm Pearson Correlation | Risk-taking Pearson Correlation | |
|---|---|---|
| Q-PAD body dissatisfaction | 0.220 ** | −0.040 |
| Q-PAD anxiety | 0.334 ** | 0.093 |
| Q-PAD depression | 0.226 ** | 0.110 |
| Q-PAD substance abuse | 0.059 | 0.511 ** |
| Q-PAD interpersonal conflicts | 0.329 ** | 0.157 * |
| Q-PAD family problems | 0.291 ** | 0.217 ** |
| Q-PAD future uncertainty | 0.110 | −0.023 |
| Q-PAD psychosocial risk | 0.286 ** | 0.440 ** |
| Q-PAD self-esteem and well-being | −0.283 ** | −0.304 |
| DERS non-acceptance | −0.069 | −0.144 ** |
| DERS goals | 0.151 ** | 0.084 |
| DERS impulse | 0.254 ** | 0.068 |
| DERS awareness | 0.284 ** | 0.260 ** |
| DERS strategies | 0.161 ** | 0.039 |
| DERS clarity | 0.079 | −0.047 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valle, A.; Cavalli, G.; Miraglia, L.; Bracaglia, E.A.; Fonagy, P.; Di Dio, C.; Marchetti, A. The Risk-Taking and Self-Harm Inventory for Adolescents: Validation of the Italian Version (RTSHIA-I). Behav. Sci. 2023, 13, 321. https://doi.org/10.3390/bs13040321
Valle A, Cavalli G, Miraglia L, Bracaglia EA, Fonagy P, Di Dio C, Marchetti A. The Risk-Taking and Self-Harm Inventory for Adolescents: Validation of the Italian Version (RTSHIA-I). Behavioral Sciences. 2023; 13(4):321. https://doi.org/10.3390/bs13040321
Chicago/Turabian StyleValle, Annalisa, Giulia Cavalli, Laura Miraglia, Edoardo Alfredo Bracaglia, Peter Fonagy, Cinzia Di Dio, and Antonella Marchetti. 2023. "The Risk-Taking and Self-Harm Inventory for Adolescents: Validation of the Italian Version (RTSHIA-I)" Behavioral Sciences 13, no. 4: 321. https://doi.org/10.3390/bs13040321